An Ethnopharmacological Study of Medicinal Plants in New South Wales

{kind=link}
{kind=link}
Abstract
:Introduction
Discussion
Development of best practices
Ethnobotanical study
Ethnopharmacological study
Extraction and isolation
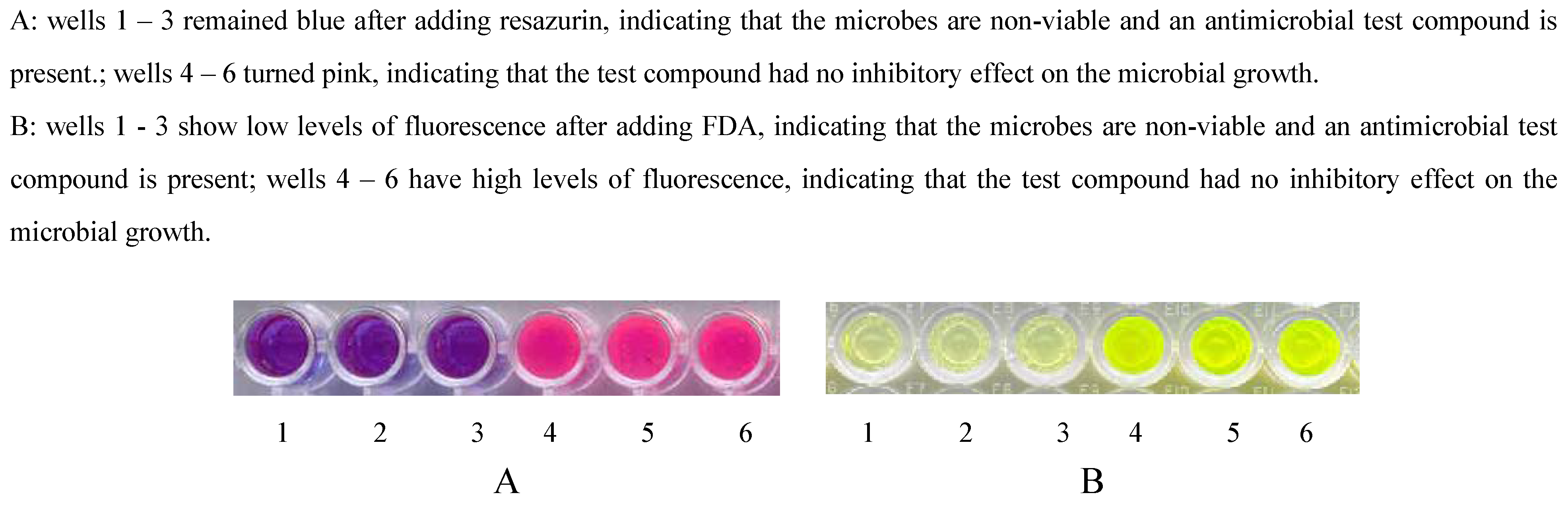
Antimicrobial assays


Neurological assays

Anti-inflammatory assays

Conclusions
Acknowledgements
References
- Aboriginal Communities of the Northern Territory of Australia. Traditional Bush Medicines: An Aboriginal Pharmacopoeia; Greenhouse Publications: Richmond, 1988; pp. 8–10. [Google Scholar]
- Smith, N.M. Ethnobotanical Field Notes from the Northern Territory. J. Adelaide Bot. Gard. 1991, 14, 1–65. [Google Scholar]
- World Health Organisation. Traditional Medicine Strategy 2002-2005; WHO: Geneva, 2002. see http://www.who.int/medicines/library/trm/trm_strat_eng.pdf. Last accessed 26/11/2004.
- Davis, E.W. Ethnobotany: An Old Practice, A New Discipline. Schultes, R.E., von Reis, S., Eds.; In Ethnobotany: Evolution of a Discipline; Chapman & Hall / Dioscorides Press: London, 1995; pp. 40–49. [Google Scholar]
- Reid, E.J.; Betts, T.J. Records of Western Australian Plants Used by Aboriginals as Medicinal Agents. Planta Med. 1979, 36, 164–173. [Google Scholar] [CrossRef] [PubMed]
- Gott, B. NSWUSE-Database of NSW Plants Utilised by Aborigines; Lodged at the Australian Institute of Aboriginal and Torres Strait Islander Studies (AIATSIS) Library; 1996. [Google Scholar]
- National Health and Medical Research Council. Values and Ethics: Guidelines for Ethical Conduct in Aboriginal and Torres Strait Islander Health Research; Commonwealth of Australia: Canberra, 2003; see: http://www.nhmrc.gov.au/publications/pdf/e52.pdf; Last accessed 13/04/2005.
- United Nations Environment Program. Traditional Knowledge and the Convention on Biological Diversity; Secretariat to the Convention on Biological Diversity: Montreal, 1993. [Google Scholar]
- Tuxill, J.; Nabhan, G.P. People, Plants and Protected Areas: a guide to in situ management. UNESCO / Earthscan: London, 2001. [Google Scholar]
- Farnsworth, N.R. Ethnopharmacology and drug development. Prance, G.T., Chadwick, D.J., Marsh, J., Eds.; In Ethnobotany and the search for new drugs; Ciba Foundation Symposium 185; Wiley: New York, 1994; pp. 42–51. [Google Scholar]
- Latz, P. quoted in Lassak, E.V.; McCarthy, T. In Australian Medicinal Plants; New Holland Publishers: Sydney, 2001; p. 14. [Google Scholar]
- Fabricant, D.S.; Farnsworth, N.R. The Value of Plants Used in Traditional Medicine for Drug Discovery. Environ. Health Persp. 2001, 109 (suppl. 1), 69–75. [Google Scholar] [CrossRef]
- Balick, M.J.; Cox, P.A. Plants, People, and Culture: The Science of Ethnobotany; Scientific American Library: New York, 1997; pp. 56–57. [Google Scholar]
- World Health Organisation. Fact sheet No. 194; WHO: Geneva Revised January 2002 see http://www.who.int/mediacentre/factsheets/fs194/en/print.html. Last accessed 26/11/2004.
- World Health Organisation. Fact sheet No. 265; WHO: Geneva, December 2001. see http://www.who.int/mediacentre/factsheets/fs265/en/print.html. Last accessed 26/11/2004.
- Antuono, P.; Beyer, J. The Burden of Dementia: A Medical and Research Perspective. Theor. Med. 1999, 20, 3–13. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. Australia's Health 2000; AIHW: Canberra, 2000; pp. 97–102. [Google Scholar]
- Houghton, P.J.; Raman, A. Laboratory Handbook for the Fractionation of Natural Extracts; Chapman & Hall: London, 1998. [Google Scholar]
- Straton, C.W.; Cooksey, R.C. Susceptibility Tests: Special Tests. Balows, A., Ed.; In Manual of Clinical Microbiology; American Society for Microbiology: Washington, 1991; pp. 1153–1165. [Google Scholar]
- Barry, A.L.; Thorsnberry, C. Susceptibility Tests: Diffusion Test Procedures. Balows, A., Ed.; In Manual of Clinical Microbiology; American Society for Microbiology: Washington, 1991; pp. 1117–1125. [Google Scholar]
- O'Brien, J.; Wilson, I.; Orton, T.; Pognan, F. Investigation of the Alamar Blue (resazurin) fluorescent dye for the assessment of mammalian cell cytotoxicity. Eur. J. Biochem. 2000, 267, 5421–5426. [Google Scholar] [CrossRef] [PubMed]
- Mann, C.M.; Markham, J.L. A new method for determining the minimum inhibitory concentration of essential oils. J. Appl. Microbiol. 1998, 84, 538–544. [Google Scholar] [CrossRef] [PubMed]
- Wanandy, S.; Brouwer, N.; Liu, Q.; Mahon, A.; Cork, S.; Karuso, P.; Vemulpad, S.; Jamie, J. Optimisation of the fluorescein diacetate antibacterial assay. J. Microbiol. Methods. 2005, 60, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Chand, S.; Lusunzi, I.; Veal, D.A.; Williams, L.R.; Karuso, P. Rapid Screening of the Antimicrobial Activity of Extracts and Natural Products. J. Antibiot. 1994, 47, 1295–1304. [Google Scholar] [CrossRef] [PubMed]
- Brunius, G. Technical Aspects of the Use of 3’,6’-Diacetyl Fluorescein for Vital Fluorescent Staining of Bacteria. Curr. Microbiol. 1980, 4, 321–323. [Google Scholar] [CrossRef]
- Chebib, M.; Johnston, G.A.R. GABA-Activated Ligand Gated Ion Channels: Medicinal Chemistry and Molecular Biology. J. Med. Chem. 2000, 43, 1427–1447. [Google Scholar] [CrossRef] [PubMed]
- Schnizler, K.; Küster, M.; Methfessel, C.; Fejtl, M. The Roboocyte: Automated cDNA/mRNA Injection and Subsequent TEVC Recording on Xenopus Oocytes in 96-Well Microtiter Plates. Receptor. Channel. 2003, 9, 41–48. [Google Scholar] [CrossRef]
- Voet, D.; Voet, J.G. Biochemistry; Wiley: New York, 1995; pp. 704–710. [Google Scholar]
- Dubois, R.N.; Abramson, S.B.; Crofford, L.; Gupta, R.A.; Simon, L.S.; van de Putte, L.B.A.; Lipsky, P.E. Cyclooygenase in biology and disease. FASEB J. 1998, 12, 1063–1073. [Google Scholar]
- Chandrasekharan, N.V.; Dai, H.; Roos, K.L.T.; Evanson, N.K.; Tomsik, J.; Elton, T.S.; Simmons, D.L. COX-3, a cyclooxygenase-1 variant inhibited by acetaminophen and other analgesic/antipyretic dugs: Cloning, structure, and expression. Proc. Natl. Acad. Sci. 2002, 99, 13926–13931. [Google Scholar] [CrossRef] [PubMed]
- Bertolini, A.; Ottani, A.; Sandrini, M. Selective COX-2 Inhibitors and Dual Acting Anti- inflammatory Drugs: Critical Remarks. Curr. Med. Chem. 2002, 9, 1033–1043. [Google Scholar] [CrossRef]
- Wu, K.K. Biochemical Pharmacology of Nonsteroidal Anti-Inflammatory Drugs. Biochem. Pharmacol. 1998, 55, 543–547. [Google Scholar] [PubMed]
- Topol, E.J. Arthritis Medicines and Cardiovascular Events – “House of Coxibs”. J. Am. Med. Assoc. 2005, 293, 366–368. [Google Scholar] [CrossRef] [PubMed]
- Cayman Chemical, COX Inhibitor Screening Assay, Catalog No. 560131. Ann Arbor, MI 48108, USA.
- Cayman Chemical, Lipoxygenase Inhibitor Screening Assay Kit, Catalog No. 760700. Ann Arbor, MI 48108, USA
© 2005 by MDPI (http:www.mdpi.org). Reproduction is permitted for noncommercial purposes.
Share and Cite
Brouwer, N.; Liu, Q.; Harrington, D.; Kohen, J.; Vemulpad, S.; Jamie, J.; Randall, M.; Randall, D. An Ethnopharmacological Study of Medicinal Plants in New South Wales. Molecules 2005, 10, 1252-1262. https://0-doi-org.brum.beds.ac.uk/10.3390/10101252
Brouwer N, Liu Q, Harrington D, Kohen J, Vemulpad S, Jamie J, Randall M, Randall D. An Ethnopharmacological Study of Medicinal Plants in New South Wales. Molecules. 2005; 10(10):1252-1262. https://0-doi-org.brum.beds.ac.uk/10.3390/10101252
Chicago/Turabian StyleBrouwer, N., Q. Liu, D. Harrington, J. Kohen, S. Vemulpad, J. Jamie, M. Randall, and D. Randall. 2005. "An Ethnopharmacological Study of Medicinal Plants in New South Wales" Molecules 10, no. 10: 1252-1262. https://0-doi-org.brum.beds.ac.uk/10.3390/10101252