
Cytomorphometric Analysis of Inflammation Dynamics in the Periodontium Following the Use of Fixed Dental Prostheses

 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Results
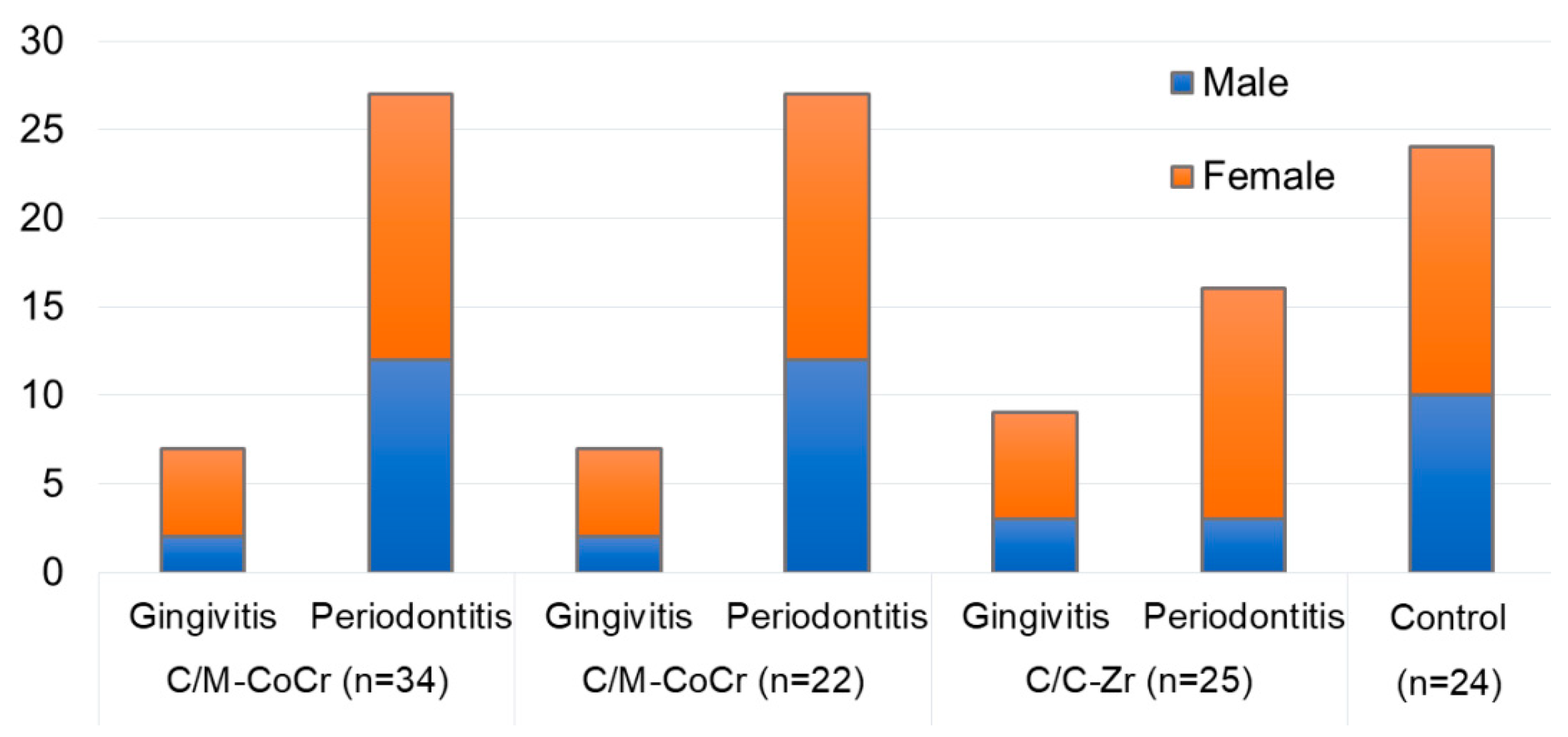
2.1. Study Subjects (Gingivitis, Periodontitis, and Healthy Subjects)
2.2. Oral Epithelial Cells and Connective Tissue Cells Analysis
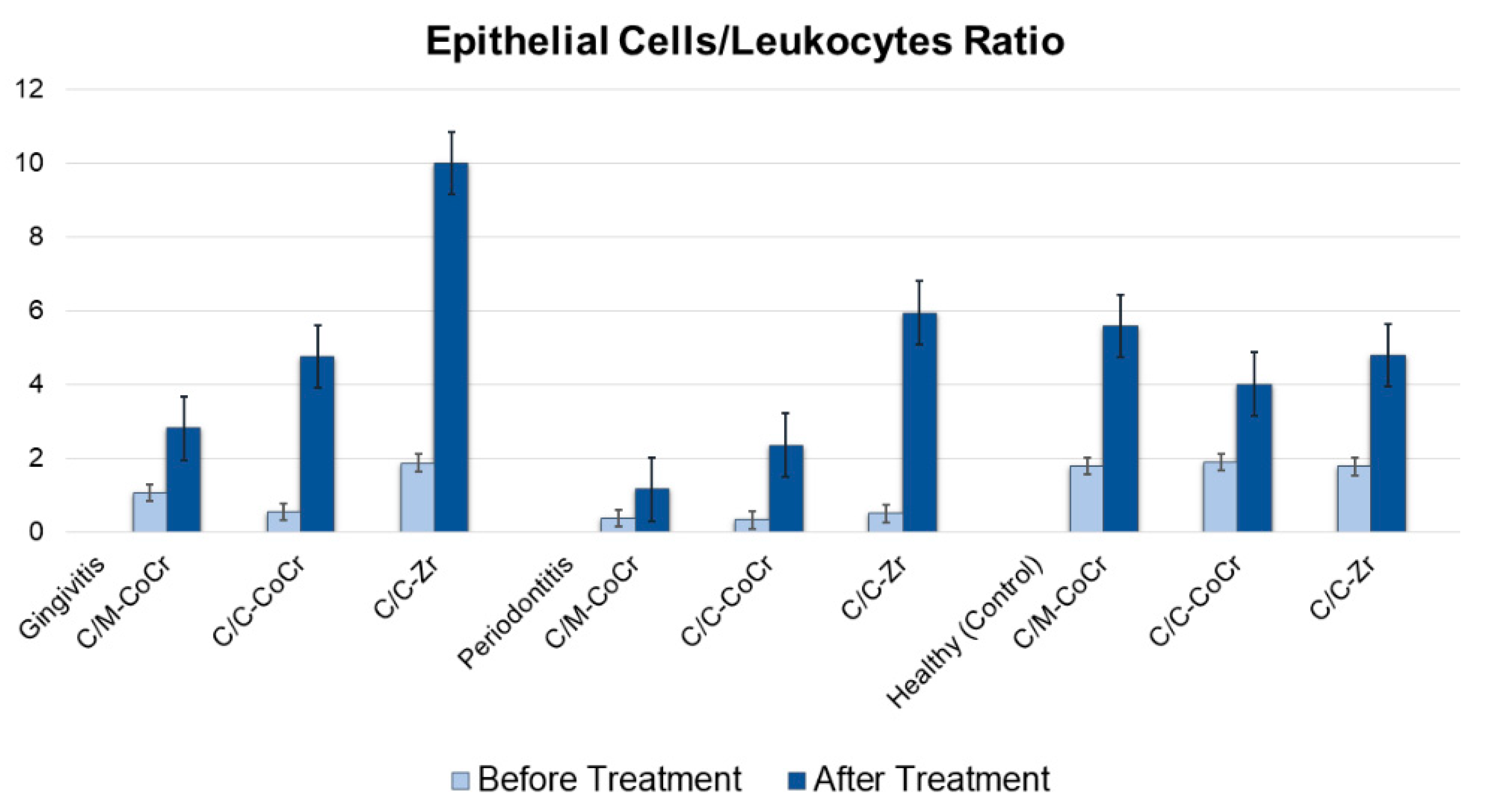
2.3. Epithelium/Leukocyte Index
3. Discussion
4. Materials and Methods
4.1. Ethics Approval and Consent to Participate
4.2. Patients Inclusion and Exclusion Criteria
4.3. Prosthetic Fabrication and Treatment Groups
4.4. Study Groups
4.5. Cytological Sampling and Analyses
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kinane, D.F.; Lappin, D.F. Immune processes in periodontal disease: A review. Ann. Periodontol. 2002, 7, 62–71. [Google Scholar] [CrossRef]
- Manrikyan, M.E. The Dental Morbidity Assessment of the Population of the Republic of Armenia, with the Record of Medical and Social Aspects and Effectiveness of Primary Prevention Programs. Ph.D. Thesis, Yerevan State Medical University, Yerevan, Armenia, 2014. [Google Scholar]
- Chen, M.; Wang, D.W.; Wu, L.P.; Zhu, S.L.; Li, Y.H. Oral health-related quality of life in patients with fixed appliances. Zhonghua Kou Qiang Yi Xue Za Zhi 2009, 44, 416–420. [Google Scholar] [PubMed]
- Kois, J.C.; Vakay, R.T. Relationship of the periodontium to Impression procedures. J. Compend. Contin. Educ. Dent. 2000, 21, 684–692. [Google Scholar]
- Kornman, K.S.; Van Dyke, T.E. Bringing light to the heat: “Inflammation and periodontal diseases: A reappraisal”. J. Periodontol. 2008, 8, 1313–1326. [Google Scholar] [CrossRef]
- Van Dyke, T.E.; Serhan, C.N. Resolution of inflammation: A new paradigm for the of pathogenesis periodontal disease. J. Dent. Res. 2003, 82, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Vita, J.A. Endothelial function. Circulation 2011, 124, 906–912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hou, G.L.; Hou, L.T.; Weisgold, A. Survival rate of teeth with periodontally hopeless prognosis after therapies with intentional replantation and perioprosthetic procedures–A study of case series for 5–12 years. Clin. Exp. Dent. Res. 2016, 2, 85–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hujoel, P.P.; White, B.A.; Garcia, R.T.; Lisgarten, M.A. The dentogingival epitelial surface area revisited. J. Periodontal. Res. 2001, 36, 148–155. [Google Scholar] [CrossRef]
- Taubman, M.A.; Kawai, T.; Han, X. The new concept of periodontal disease pathogenesis requires new and novel therapeutic strategies. J. Clin. Periodontol. 2007, 34, 367–369. [Google Scholar] [CrossRef]
- Cappeli, D.P.; Mobley, C.C. Prevention in Clinical Oral Health; Mosby Elsevier: Louis, MO, USA, 2008; pp. 18–25. [Google Scholar]
- Kornman, K.S. The “innovator’s dilemma” for periodontists. J. Periodontol. 2010, 5, 646–649. [Google Scholar] [CrossRef]
- Abduo, J.; Lyons, K.M. Interdisciplinary interface between fixed prosthodontics and periodontics. Periodontology 2000 2000, 74, 40–62. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, P.V.; Higginbottom, F.L.; Wilson, T.G. Periodontal considerations in restorative and implant therapy. Periodontology 2000 2001, 25, 100–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haroon, R. How does fixed prosthodontics interface with periodontology? J. Res. Dent. 2015, 3, 96. [Google Scholar]
- Kois, J.C. The restorative-periodontal interface: Biological parameters. Periodontology 2000 1996, 11, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Al-Sinaidi, A.; Preethanath, R.S. The effect of fixed partial dentures on periodontal status of abutment teeth. Saudi J. Dent. Res. 2014, 5, 104–108. [Google Scholar] [CrossRef] [Green Version]
- Cekici, A.; Kantarci, A.; Hasturk, H.; Van Dyke, T.E. Inflammatory and immune pathways in the pathogenesis of periodontal disease. Periodontology 2000 2014, 64, 57–80. [Google Scholar] [CrossRef] [Green Version]
- Gupta, G. GCF as a periodontal diagnostic indicator- II: Inflammatory mediators, host-response modifiers and chair side diagnostic aids. J. Med. Life 2013, 6, 7–13. [Google Scholar] [PubMed]
- Hasiuk, P.; Hasiuk, N.; Kindiy, D.; Ivanchyshyn, V.; Kalashnikov, D.; Zubchenko, S. Characteristics of cellular composition of periodontal pockets. Interv. Med. Appl. Sci. 2016, 8, 172–177. [Google Scholar] [CrossRef]
- Kantarci, A.; Oyaizu, K.; Van Dyke, T.E. Neutrophil-mediated tissue injury in periodontal disease pathogenesis: Findings from localized aggressive periodontitis. J. Periodontol. 2003, 74, 66–75. [Google Scholar] [CrossRef]
- Rizo-Gorrita, M.; Luna-Oliva, I.; Serrera-Figallo, M.Á.; Gutiérrez-Pérez, J.L.; Torres-Lagares, D. Comparison of Cytomorphometry and Early Cell Response of Human Gingival Fibroblast (HGFs) between Zirconium and New Zirconia-Reinforced Lithium Silicate Ceramics (ZLS). Int. J. Mol. Sci. 2018, 19, 2718. [Google Scholar] [CrossRef] [Green Version]
- Bretz, W.A.; Weyant, R.J.; Corby, P.M.; Ren, D.; Weissfeld, L.; Kritchevsky, S.B.; Harris, T.; Kurella, M.; Satterfield, S.; Visser, M.; et al. Systemic inflammatory markers, periodontal diseases, and periodontal infections in an elderly population. J. Am. Geriatr. Soc. 2005, 53, 1532–1537. [Google Scholar] [CrossRef] [PubMed]
- Nair, S.; Faizuddin, M.; Dharmapalan, J. Role of autoimmune responses in periodontal disease. Autoim. Dis. 2014, 2014, 596824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Dyke, T.E.; Kornman, K.S. Inflammation and factors that may regulate inflammatory response. Periodontology 2008, 79, 1503–1507. [Google Scholar] [CrossRef] [PubMed]
- Andrews, T.; Sullivan, K.E. Infections in Patients with Inherited Defects in Phagocytic Function. Clin. Microbiol. Rev. 2003, 16, 597–621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosshardt, D.D.; Lang, N.P. The junctional epithelium: From health to disease. J. Dent. Res. 2005, 84, 9–20. [Google Scholar] [CrossRef]
- Delima, A.J.; Van Duke, T.E. Origin and function of the cellular components in gingival crevice fluid. Periodontology 2000 2003, 31, 55–76. [Google Scholar] [CrossRef] [PubMed]
- Bykov, V.L. Human Gingival Immunocompetent Cells in the Norm and in Inflammatory Periodontal Diseases. Arkh. Patol. 2005, 67, 51–55. [Google Scholar]
- Biselli, R.; Ferlini, C.; Di Murro, C.; Paolantonio, M.; Fattorossi, A. Flow cytometric approach to human polymorphonuclear leukocyte activation induced by gingival crevicular fluid in periodontal disease. Inflammation 1995, 19, 479–487. [Google Scholar] [CrossRef]
- Gupta, G. Gingival crevicular fluid as a periodontal diagnostic indicator—I: Host derived enzymes and tissue breakdown products. J. Med. Life 2012, 5, 390–397. [Google Scholar] [PubMed]
- Ebersole, J.L. Humoral immune responses in gingival crevice fluid: Local and systemic implications. Periodontology 2000 2003, 31, 135–166. [Google Scholar] [CrossRef]
- Castro Cecilia, E.; Koss Myriam, A.; López María, E. Cytological analysis of the periodontal pocket in patients with aggressive periodontitis and chronic periodontitis. Contemp. Clin. Dent. 2014, 5, 495–500. [Google Scholar]
- Armitage, G.C. Analysis of gingival crevice fluid and risk of progression of periodontitis. Periodontology 2000 2004, 34, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Shin, H.; Zhang, Y.; Jagannathan, M.; Hasturk, H.; Kantarci, A.; Liu, H.; Van Dyke, T.E.; Ganley-Leal, L.M.; Nikolajczyk, B.S. B cells from periodontal disease patients express surface Toll-like receptor 4. J. Leukoc. Biol. 2009, 85, 648–655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sigusch, B.; Eick, S.; Pfister, W. Altered chemotactie behavior of crevicular PMNs in different forms of periodontitis. J. Glin. Periodontol. 2001, 28, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Moimaz, S.A.S.; Saliba, N.A.; Saliba, O.; Zina, L.G.; Bolonhez, M.R.C. Association between dental prosthesis and periodontal disease in a rural Brazilian community. Braz. J. Oral Sci. 2006, 5, 1226–1231. [Google Scholar]
- Rokaya, D.; Mahat, Y.; Sapkota, B.; Basnyat, S.K. Full Coverage Crowns and Resin-bonded Bridge Combination for Missing Mandibular Anterior Teeth. Kathmandu Univ. Med. J. 2018, 16, 97–99. [Google Scholar]
- World Health Organization. Oral Health Surveys-Basic Methods, 5th ed.; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- Carneiro, L.G.; Nouh, H.; Salih, E. Quantitative gingival crevicular fluid proteome in health and periodontal disease using stable isotope chemistries and mass spectrometry. J. Clin. Periodontol. 2014, 41, 733–747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ballambettu, S.P.; Pradeep, A.R.; Purushottam, M.; Sen, S. Higher interleukin-33 levels in aggressive periodontitis cases. J. Indian Soc. Periodontol. 2019, 23, 424–429. [Google Scholar]
- Thakur, M.; Guttikonda, V.R. Modified ultrafast Papanicolaou staining technique: A comparative study. J. Citol. 2017, 34, 149–153. [Google Scholar] [CrossRef]
- Krafts, K.P.; Pambuccian, S.E. Romanowsky staining in cytopathology: History, advantages and limitations. Biotech. Histochem. 2011, 86, 82–93. [Google Scholar] [CrossRef]
Sample Availability: Samples used in this study are available from the authors. |



{kind=link}
{kind=link}
| Subgroup | Cells Measurements | Groups | p Value | |
|---|---|---|---|---|
| Before Prostheses (Mean ± SD) | After Prostheses (Mean ± SD) | |||
| Gingivitis Group (n = 23) | ||||
| Epithelial cells | 11.14 ± 3.4 | 14 ± 2.2 | 0.002 * |
| PMNs | 10.57 ± 4.7 | 5 ± 1.9 | 0.005 * | |
| Epithelial cells | 9 ± 2.6 | 16.89 ± 1.8 | <0.0001 * |
| PMNs | 16.56 ± 11.4 | 3.56 ± 1.6 | 0.006 * | |
| Epithelial cells | 11.71 ± 4.2 | 18.57 ± 3.2 | <0.0001 * |
| PMNs | 6.29 ± 3.2 | 1.86 ± 0.04 | <0.0001 * | |
| Periodontitis Group (n = 58) | ||||
| Epithelial cells | 8.48 ± 3.03 | 11.67 ± 2.7 | <0.0001 * |
| PMNs | 23.33 ± 10.9 | 10.07 ± 3.4 | <0.0001 * | |
| Epithelial cells | 7.25 ± 2.8 | 14.12 ± 2.7 | <0.0001 * |
| PMNs | 22.63 ± 11.7 | 6.0 ± 2.2 | <0.0001 * | |
| Epithelial cells | 9.13 ± 2.9 | 14.67 ± 3.02 | <0.0001 * |
| PMNs | 18.27 ± 6.2 | 2.47 ± 0.9 | <0.0001 * | |
| Control Group (n = 24) | ||||
| Epithelial cells | 13.67 ± 1.52 | 18.67 ± 3.05 | <0.0001 * |
| PMNs | 7.67 ± 2.51 | 3.33 ± 1.88 | <0.0001 * | |
| Epithelial cells | 16.12 ± 4.67 | 16.75 ± 4.23 | 0.006 * |
| PMNs | 8.50 ± 2.04 | 4 ± 2.97 | 0.04 * | |
| Epithelial cells | 11.08 ± 2.39 | 14.77 ± 2.92 | <0.0001 * |
| PMNs | 6.23 ± 2.5 | 3.08 ± 1.09 | 0.006 * | |
| Group | Cells | Multiple Comparisons | ||
|---|---|---|---|---|
| C/M-CoCr vs. C/C-CoCr | C/M-CoCr vs. C/C-Zr | C/C-CoCr vs. C/C-Zr | ||
| Before Treatment | ||||
| Gingivitis | Epithelial cells | 0.098 | 0.84 | 0.026 * |
| PMNs | 0.020 * | 0.126 | <0.0001 * | |
| Periodontitis | Epithelial cells | 0.062 | 0.453 | 0.0018 * |
| PMNs | 0.923 | 0.017 * | 0.049 * | |
| Healthy Subjects | Epithelial cells | 0.023 * | 0.015 * | <0.0001 * |
| PMNs | 0.438 | 0.094 | 0.003 * | |
| After Treatment | ||||
| Gingivitis | Epithelial cells | 0.0005 * | <0.0001 * | 0.062 |
| PMNs | 0.0032 * | <0.0001 * | 0.004 * | |
| Periodontitis | Epithelial cells | <0.0001 * | <0.0001 * | 0.544 |
| PMNs | <0.0001 * | <0.0001 * | <0.0001 * | |
| Healthy | Epithelial cells | 0.138 | 0.0006 * | 0.122 |
| PMNs | 0.532 | 0.9058 | 0.297 | |
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
| Score | Sign |
|---|---|
| Score 0 | no signs of disease |
| Score 1 | gingival bleeding after gentle probing |
| Score 2 | presence of supra- or subgingival calculus or other plaque retentive factors |
| Score 3 | 4- or 5-mm periodontal pockets |
| Score 4 | 6-mm or deeper periodontal pockets |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heboyan, A.; Syed, A.U.Y.; Rokaya, D.; Cooper, P.R.; Manrikyan, M.; Markaryan, M. Cytomorphometric Analysis of Inflammation Dynamics in the Periodontium Following the Use of Fixed Dental Prostheses. Molecules 2020, 25, 4650. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules25204650
Heboyan A, Syed AUY, Rokaya D, Cooper PR, Manrikyan M, Markaryan M. Cytomorphometric Analysis of Inflammation Dynamics in the Periodontium Following the Use of Fixed Dental Prostheses. Molecules. 2020; 25(20):4650. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules25204650
Chicago/Turabian StyleHeboyan, Artak, Azeem Ul Yaqin Syed, Dinesh Rokaya, Paul R. Cooper, Mikael Manrikyan, and Marina Markaryan. 2020. "Cytomorphometric Analysis of Inflammation Dynamics in the Periodontium Following the Use of Fixed Dental Prostheses" Molecules 25, no. 20: 4650. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules25204650