
Gingival Crevicular Fluid (GCF): A Diagnostic Tool for the Detection of Periodontal Health and Diseases


 , ,
, , 
 and
and 
Abstract
:1. Introduction
2. Gingival Crevicular Fluid
2.1. Formation of GCF
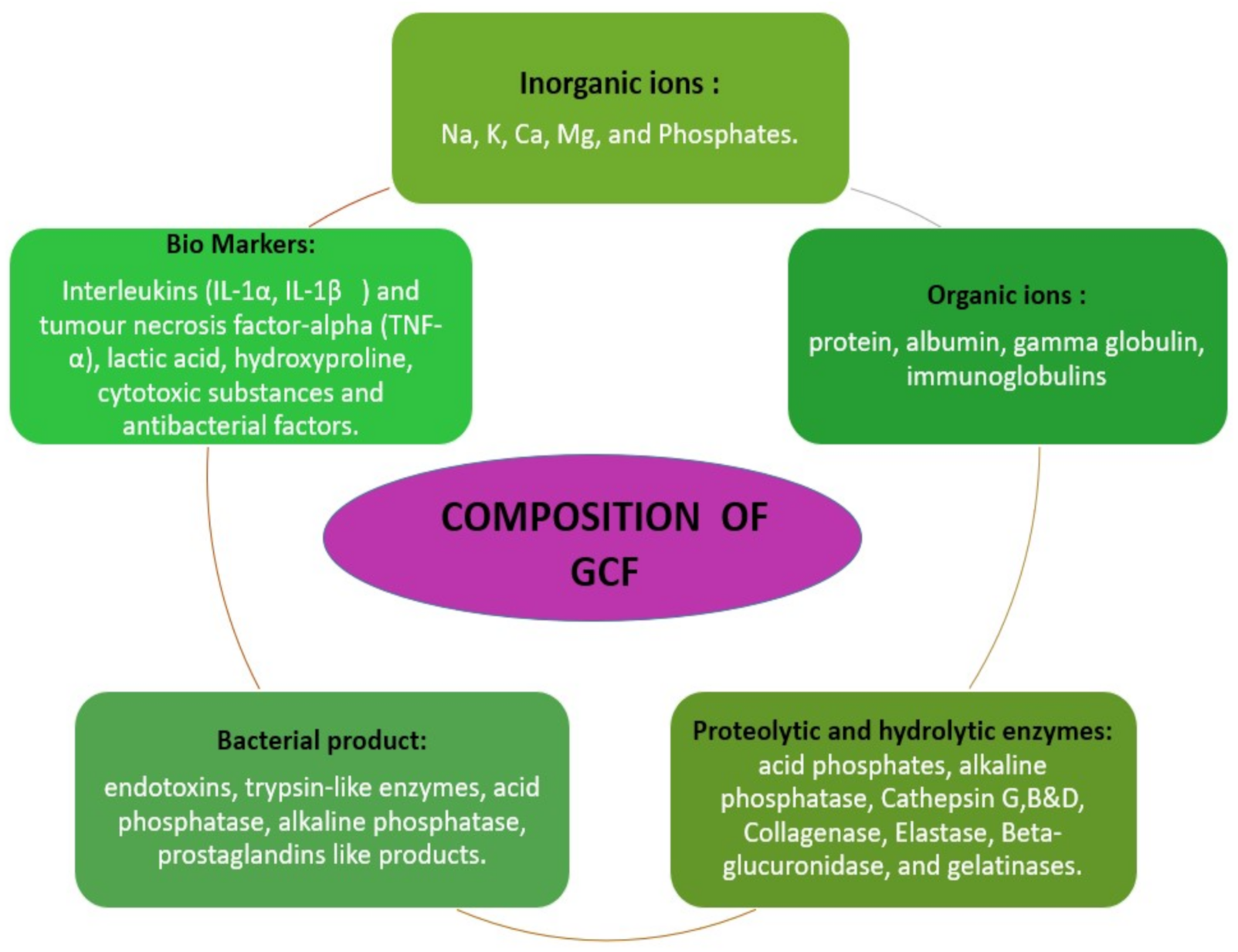
2.2. Constituents of GCF Aliquot
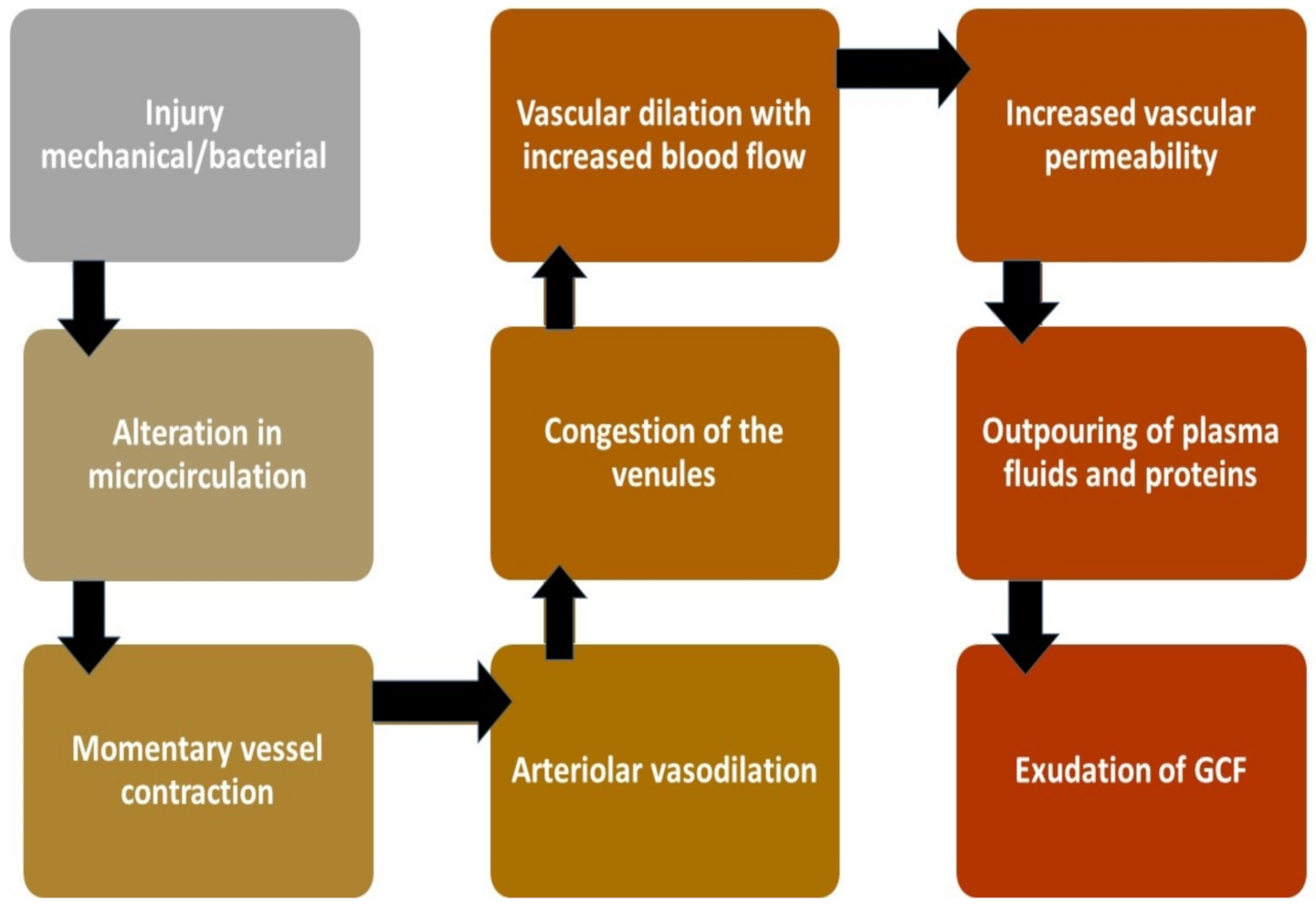
2.3. Mechanism of Production
2.4. Circadian Rhythm of GCF
2.5. Collection of GCF
2.6. Conventional Diagnostic Measure Versus GCF
2.7. GCF as a Biomarker
3. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Goodson, J.M.; Tanner, A.C.R.; Haffajee, A.D.; Sornberger, G.C.; Socransky, S.S. Patterns of progression and regression of advanced destructive periodontal disease. J. Clin. Periodontol. 1982, 9, 472–481. [Google Scholar] [CrossRef] [PubMed]
- Albandar, J.M. Periodontal diseases in North America. Periodontology 2000 2002, 29, 31–69. [Google Scholar] [CrossRef] [PubMed]
- Tonetti, M.S.; Jepsen, S.; Jin, L.; Otomo-Corgel, J. Impact of the global burden of periodontal diseases on health, nutrition and wellbeing of mankind: A call for global action. J. Clin. Periodontol. 2017, 44, 456–462. [Google Scholar] [CrossRef] [Green Version]
- Darveau, R.P. Periodontitis: A polymicrobial disruption of host homeostasis. Nat. Rev. Microbiol. 2010, 8, 481–490. [Google Scholar] [CrossRef] [PubMed]
- Ebersole, J.L. Humoral immune responses in gingival crevice fluid: Local and systemic implications. Periodontology 2000 2003, 31, 135–166. [Google Scholar] [CrossRef]
- Zhou, J.; Yao, Y.; Jiao, K.; Zhang, J.; Zheng, X.; Wu, F.; Hu, X.; Li, J.; Yu, Z.; Zhang, G.; et al. Relationship between Gingival Crevicular Fluid Microbiota and Cytokine Profile in Periodontal Host Homeostasis. Front. Microbiol. 2017, 8, 2144. [Google Scholar] [CrossRef]
- Pei, J.; Li, F.; Xie, Y.; Liu, J.; Yu, T.; Feng, X. Microbial and metabolomic analysis of gingival crevicular fluid in general chronic periodontitis patients: Lessons for a predictive, preventive, and personalized medical approach. EPMA J. 2020, 11, 197–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khurshid, Z.; Mali, M.; Naseem, M.; Najeeb, S.; Zafar, M.S. Human Gingival Crevicular Fluids (GCF) Proteomics: An Overview. Dent. J. 2017, 5, 12. [Google Scholar] [CrossRef]
- Griffiths, G.S. Formation, collection and significance of gingival crevice fluid. Periodontology 2000 2003, 31, 32–42. [Google Scholar] [CrossRef]
- Brill, N.; Krasse, B.O. The Passage of Tissue Fluid into the Clinically Healthy Gingival Pocket. Acta Odontol. Scand. 1958, 16, 233–245. [Google Scholar] [CrossRef]
- Armitage, G.C. The complete periodontal examination. Periodontology 2000 2004, 34, 22–33. [Google Scholar] [CrossRef] [PubMed]
- Oswal, S.; Dwarakanath, C. Relevance of gingival crevice fluid components in assessment of periodontal disease—A critical analysis. J. Indian Soc. Periodontol. 2010, 14, 282–286. [Google Scholar] [CrossRef]
- Günday, S.; Topcu, A.O.; Ercan, E.; Yamalik, N. Analysis of Daytime Variations in Gingival Crevicular Fluid: A Circadian Periodicity? J. Periodontol. 2014, 85, e47–e56. [Google Scholar] [CrossRef] [PubMed]
- Winer, R.A.; O’Donnell, L.J.; Chauncey, H.H.; McNamara, T.F. Enzyme Activity in Periodontal Disease. J. Periodontol. 1970, 41, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Arias-Bujanda, N.; Regueira-Iglesias, A.; Alonso-Sampedro, M.; González-Peteiro, M.M.; Mira, A.; Balsa-Castro, C.; Tomás, I. Cytokine thresholds in gingival crevicular fluid with potential diagnosis of chronic periodontitis differentiating by smoking status. Sci. Rep. 2018, 8, 1–12. [Google Scholar]
- Skapski, H.; Lehner, T. A crevicular washing method for investigating immune components of crevicular fluid in man. J. Periodontal Res. 1976, 11, 19–24. [Google Scholar] [CrossRef]
- Shrivastava, D.; Srivastava, K.C.; Dayakara, J.K.; Sghaireen, M.G.; Gudipaneni, R.K.; Al-Johani, K.; Baig, M.N.; Khurshid, Z. BactericidalActivity of Crevicular Polymorphonuclear Neutrophils in Chronic Periodontitis Patients and Healthy Subjects under the Influence of Areca Nut Extract: An In Vitro Study. Appl. Sci. 2020, 10, 5008. [Google Scholar] [CrossRef]
- Ghallab, N.A. Diagnostic potential and future directions of biomarkers in gingival crevicular fluid and saliva of periodontal diseases: Review of the current evidence. Arch. Oral Biol. 2018, 87, 115–124. [Google Scholar] [CrossRef]
- Gul, S.S.; Griffiths, G.S.; Stafford, G.P.; Al-Zubidi, M.I.; Rawlinson, A.; Douglas, C.W. Investigation of a novel predictive biomarker profile for the outcome of periodontal treatment. J. Periodontol. 2017, 88, 1135–1144. [Google Scholar] [CrossRef]
- Nimbulkar, G.; Garacha, V.; Shetty, V.; Bhor, K.; Srivastava, K.C.; Shrivastava, D.; Sghaireen, M.G. Microbiological and clinical evaluation of Neem gel and Chlorhexidine gel on dental plaque and gingivitis in 20–30 years old adults: A randomized parallel-armed, double-blinded controlled trial. J. Pharm. Bioallied Sci. 2020, 12 (Suppl. 1), S345–S351. [Google Scholar] [CrossRef]
- Larsson, L. Current Concepts of Epigenetics and Its Role in Periodontitis. Curr. Oral Health Rep. 2017, 4, 286–293. [Google Scholar] [CrossRef] [Green Version]
- Qasim, S.S.B.; Al-Otaibi, D.; Al-Jasser, R.; Gul, S.S.; Zafar, M.S. An Evidence-Based Update on the Molecular Mechanisms Underlying Periodontal Diseases. Int. J. Mol. Sci. 2020, 21, 3829. [Google Scholar] [CrossRef]
- Nomura, Y.; Okada, A.; Kakuta, E.; Gunji, T.; Kajiura, S.; Hanada, N. A new screening method for periodontitis: An alternative to the community periodontal index. BMC Oral Health 2016, 16, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Lindhe, J.; Haffajee, A.D.; Socransky, S.S. Progression of periodontal disease in adult subjects in the absence of periodontal therapy. J. Clin. Periodontol. 1983, 10, 433–442. [Google Scholar] [CrossRef]
- Buduneli, N. Biomarkers in periodontal health and disease: Rationale, benefits, and future directions. In Biomarkers in Periodontal Health and Disease: Rationale, Benefits, and Future Directions; Springer: Cham, Switzerland, 2019; Volume 90. [Google Scholar]
- Subrahmanyam, M.V.; Sangeetha, M. Gingival crevicular fluid a marker of the periodontal disease activity. Indian J. Clin. Biochem. 2003, 18, 5–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Alencar Silva, F.G.; Gomes, S.C. Validation of an alternative absorbent paper for collecting gingival crevicular fluid/Validação de um papel absorvente para coleta de Fluido Crevicular Gengival. Periodontia 2009, 19, 85–90. [Google Scholar]
- Konopka, Ł.; Pietrzak, A.; Brzezińska-Błaszczyk, E. Effect of scaling and root planing on interleukin-1β, interleukin-8 and MMP-8 levels in gingival crevicular fluid from chronic periodontitis patients. J. Periodontal Res. 2012, 47, 681–688. [Google Scholar] [CrossRef]
- Majeed, Z.N.; Philip, K.; Alabsi, A.M.; Pushparajan, S.; Swaminathan, D. Identification of Gingival Crevicular Fluid Sampling, Analytical Methods, and Oral Biomarkers for the Diagnosis and Monitoring of Periodontal Diseases: A Systematic Review. Dis. Markers 2016, 2016, 1804727. [Google Scholar]
- Graves, D. Cytokines that Promote Periodontal Tissue Destruction. J. Periodontol. 2008, 79, 1585–1591. [Google Scholar] [CrossRef] [Green Version]
- Offenbacher, S.; Barros, S.P.; Singer, R.E.; Moss, K.; Williams, R.C.; Beck, J.D. Periodontal disease at the biofilm-gingival interface. J. Periodontol. 2007, 78, 1911–1925. [Google Scholar] [CrossRef] [PubMed]
- Júnior, A.A.B.; Pallos, D.; Cortelli, J.R.; Saraceni, C.H.C.; Queiroz, C.S. Evaluation of organic and inorganic compounds in the saliva of patients with chronic periodontal disease. Rev. Odonto Ciência 2010, 25, 234–238. [Google Scholar] [CrossRef]
- Wong, D.T. Salivary diagnostics powered by nanotechnologies, proteomics and genomics. J. Am. Dent. Assoc. 2006, 137, 313–321. [Google Scholar] [CrossRef] [Green Version]
- Oringer, R.J.; Howell, T.H.; Nevins, M.L.; Reasner, D.S.; Davis, G.H.; Sekler, J.; Fiorellini, J.P. Relationship Between Crevicular Aspartate Aminotransferase Levels and Periodontal Disease Progression. J. Periodontol. 2001, 72, 17–24. [Google Scholar] [CrossRef]
- Eley, B.M.; Cox, S.W. The relationship between gingival crevicular fluid cathepsin B activity and periodontal attachment loss in chronic periodontitis patients: A 2-year longitudinal study. J. Periodontal Res. 1996, 31, 381–392. [Google Scholar] [CrossRef]
- Ahmad, P.; Arshad, A.I.; Bella, E.D.; Khurshid, Z.; Stoddart, M. Systemic Manifestations of the Periodontal Disease: A Bibliometric Review. Molecules 2020, 25, 4508. [Google Scholar] [CrossRef]
- Fassbender, W.J.; Steinhauer, B.; Stracke, H.; Schumm-Draeger, P.-M.; Usadel, K.-H. Validation of a new automated immunoassay for measurement of intact osteocalcin. Clin. Lab. 2002, 48, 31–38. [Google Scholar] [PubMed]
- Khiste, S.V.; Ranganath, V.; Nichani, A.S.; Rajani, V. Critical analysis of biomarkers in the current periodontal practice. J. Indian Soc. Periodontol. 2011, 15, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Bowers, M.R.; Fisher, L.W.; Termine, J.D.; Somerman, M.J. Connective tissue-associated proteins in crevicular fluid: Potential markers for periodontal diseases. J. Periodontol. 1989, 60, 448–451. [Google Scholar] [CrossRef] [PubMed]
- Airila-Månsson, S.; Söder, B.; Kari, K.; Meurman, J.H. Influence of Combinations of Bacteria on the Levels of Prostaglandin E2, Interleukin-1β, and Granulocyte Elastase in Gingival Crevicular Fluid and on the Severity of Periodontal Disease. J. Periodontol. 2006, 77, 1025–1031. [Google Scholar] [CrossRef] [PubMed]
- Huynh, Q.N.; Wang, S.; Tafolla, E.; Gansky, S.A.; Kapila, S.; Armitage, G.C.; Kapila, Y.L. Specific Fibronectin Fragments as Markers of Periodontal Disease Status. J. Periodontol. 2002, 73, 1101–1110. [Google Scholar] [CrossRef]
- Aral, C.A.; Ölçer, S.N.; Aral, K.; Kapila, Y. Oxidative stress, neutrophil elastase and IGFBP7 levels in patients with oropharyngeal cancer and chronic periodontitis. Oral Dis. 2020, 26, 1393–1401. [Google Scholar] [CrossRef]
- Sophia, K.; Suresh, S.; Sudhakar, U.; Cader, S.A., Jr.; Vardhini, V.M.; Arunachalam, T.L.; Jean, S.C. Comparative Evaluation of Serum and Gingival Crevicular Fluid Periostin Levels in Periodontal Health and Disease: A Biochemical Study. Cureus 2020, 12, e7218. [Google Scholar] [CrossRef] [Green Version]
- Kumar, P.A.; Kripal, K.; Chandrasekaran, K.; Bhavanam, S.R. Estimation of YKL-40 Levels in Serum and Gingival Crevicular Fluid in Chronic Periodontitis and Type 2 Diabetes Patients among South Indian Population: A Clinical Study. Contemporary Clin. Dent. 2019, 10, 304–310. [Google Scholar]
- Hashimura, S.; Kido, J.; Matsuda, R.; Yokota, M.; Matsui, H.; Inoue-Fujiwara, M.; Inagaki, Y.; Hidaka, M.; Tanaka, T.; Tsutsumi, T.; et al. A low level of lysophosphatidic acid in human gingival crevicular fluid from patients with periodontitis due to high soluble lysophospholipase activity: Its potential protective role on alveolar bone loss by periodontitis. Biochim. Biophys. Acta Mol. Cell Biol. Lipids 2020, 1865, 158698. [Google Scholar] [CrossRef]
- Pereira, A.G.; Costa, L.C.M.; Soldati, K.R.; De Abreu, M.H.N.G.; Costa, F.O.; Zandim-Barcelos, D.L.; Cota, L.O.M. Gingival Crevicular Fluid Levels of Human Beta-defensin 2 and 3 in Healthy and Diseased Sites of Individuals with and without Periodontitis. J. Int. Acad. Periodontol. 2020, 22, 90–99. [Google Scholar]
- Zorina, O.A.; Amkhadova, M.A.; Abaev, Z.M.; Khamukova, A.A.; Demidova, A.A. Hypoxia-dependent transcriptional control of activity of destructive inflammatory and malignant periodontium changes. Stomatologiia 2020, 99, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Kinney, J.S.; Morelli, T.; Oh, M.; Braun, T.M.; Ramseier, C.A.; Sugai, J.V.; Giannobile, W.V. Crevicular fluid biomarkers and periodontal disease progression. J. Clin. Periodontol. 2014, 41, 113–120. [Google Scholar] [CrossRef] [Green Version]
- Takai, H.; Furuse, N.; Ogata, Y. Anti-heat shock protein 70 levels in gingival crevicular fluid of Japanese patients with chronic periodontitis. J. Oral Sci. 2020, 62, 281–284. [Google Scholar] [CrossRef]
- Najeeb, S.; Zafar, M.S.; Khurshid, Z.; Zohaib, S.; Almas, K. The Role of Nutrition in Periodontal Health: An Update. Nutrients 2016, 8, 530. [Google Scholar] [CrossRef] [PubMed]
- Garlet, G.P. Critical reviews in oral biology & medicine: Destructive and protective roles of cytokines in periodontitis: A re-appraisal from host defense and tissue destruction viewpoints. J. Dent. Res. 2010, 89, 1349–1363. [Google Scholar] [PubMed]
- Barros, S.P.; Williams, R.C.; Offenbacher, S.; Morelli, T. Gingival crevicular fluid as a source of biomarkers for periodontitis. Periodontology 2000 2016, 70, 53–64. [Google Scholar] [CrossRef]
- Kaur, G.; Mohindra, K.; Singla, S. Autoimmunity—Basics and link with periodontal disease. Autoimmun. Rev. 2017, 16, 64–71. [Google Scholar] [CrossRef]
- Bostanci, N.; Bao, K.; Greenwood, D.; Silbereisen, A.; Belibasakis, G.N. Periodontal disease: From the lenses of light microscopy to the specs of proteomics and next-generation sequencing. In Advances in Clinical Chemistry; Elsevier: London, UK, 2019; pp. 263–290. [Google Scholar]
- Khurshid, Z.; Warsi, I.; Moin, S.F.; Slowey, P.D.; Latif, M.; Zohaib, S.; Zafar, M.S. Biochemical analysis of oral fluids for disease detection. In Advances in Clinical Chemistry; Elsevier: London, UK, 2021; pp. 205–253. [Google Scholar]
- Armitage, G.C.; Svanberc, G.K.; Loe, H. Microscopic evaluation of clinical measurements of connective tissue attachment levels. J. Clin. Periodontol. 1977, 4, 173–190. [Google Scholar] [CrossRef] [Green Version]
- Heft, M.W.; Perelmuter, S.H.; Cooper, B.Y.; Magnusson, I.; Clark, W.B. Relationship between gingival inflammation and painfulness of periodontal probing. J. Clin. Periodontol. 1991, 18, 213–215. [Google Scholar] [CrossRef]
- Lang, N.P.; Adler, R.; Joss, A.; Nyman, S. Absence of bleeding on probing an indicator of periodontal stability. J. Clin. Periodontol. 1990, 17, 714–721. [Google Scholar] [CrossRef] [PubMed]
- Rüdin, H.J.; Overdiek, H.F.; Rateitschak, K.H. Correlation between sulcus fluid rate and clinical and histological inflammation of the marginal gingiva. Helv. Odontol. Acta 1970, 14, 21–26. [Google Scholar] [PubMed]
- Ito, H.; Numabe, Y.; Hashimoto, S.; Sekino, S.; Murakashi, E.; Ishiguro, H.; Sasaki, D.; Yaegashi, T.; Takai, H.; Mezawa, M.; et al. Correlation between Gingival Crevicular Fluid Hemoglobin Content and Periodontal Clinical Parameters. J. Periodontol. 2016, 87, 1314–1319. [Google Scholar] [CrossRef] [PubMed]
- Hong, I.; Pae, H.-C.; Song, Y.W.; Cha, J.-K.; Lee, J.-S.; Paik, J.-W.; Choi, S.-H. Oral Fluid Biomarkers for Diagnosing Gingivitis in Human: A Cross-Sectional Study. J. Clin. Med. 2020, 9, 1720. [Google Scholar] [CrossRef] [PubMed]
- Chaudhari, A.U.; Byakod, G.N.; Waghmare, P.F.; Karhadkar, V.M. Correlation of Levels of Interleukin-1β in Gingival Crevicular Fluid to the Clinical Parameters of Chronic Periodontitis. J. Contemp. Dent. Pr. 2011, 12, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Becerik, S.; Öztürk, V.Ö.; Atmaca, H.; Atilla, G.; Emingil, G. Gingival Crevicular Fluid and Plasma Acute-Phase Cytokine Levels in Different Periodontal Diseases. J. Periodontol. 2012, 83, 1304–1313. [Google Scholar] [CrossRef]
- Bıyıkoğlu, B.; Buduneli, N.; Kardeşler, L.; Aksu, K.; Pitkala, M.; Sorsa, T. Gingival Crevicular Fluid MMP-8 and −13 and TIMP-1 Levels in Patients with Rheumatoid Arthritis and Inflammatory Periodontal Disease. J. Periodontol. 2009, 80, 1307–1314. [Google Scholar] [CrossRef] [PubMed]
- Fujita, Y.; Ito, H.; Sekino, S.; Numabe, Y. Correlations between pentraxin 3 or cytokine levels in gingival crevicular fluid and clinical parameters of chronic periodontitis. Odontology 2012, 100, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Wassall, R.R.; Preshaw, P.M. Clinical and technical considerations in the analysis of gingival crevicular fluid. Periodontology 2000 2016, 70, 65–79. [Google Scholar] [CrossRef] [PubMed]
- Türkoğlu, O.; Becerik, S.; Tervahartiala, T.; Sorsa, T.; Atilla, G.; Emingil, G. The effect of adjunctive chlorhexidine mouthrinse on GCF MMP-8 and TIMP-1 levels in gingivitis: A randomized placebo-controlled study. BMC Oral Health 2014, 14, 55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marcaccini, A.M.; Meschiari, C.A.; Zuardi, L.R.; de Sousa, T.S.; Taba, M., Jr.; Teofilo, J.M.; Jacob-Ferreira, A.L.B.; Tanus-Santos, J.E.; Novaes, A.B., Jr.; Gerlach, R.F. Gingival crevicular fluid levels of MMP-8, MMP-9, TIMP-2, and MPO decrease after periodontal therapy. J. Clin. Periodontol. 2010, 37, 180–190. [Google Scholar] [CrossRef]
- Pourabbas, R.; Kashefimehr, A.; Rahmanpour, N.; Babaloo, Z.; Kishen, A.; Tenenbaum, H.C.; Azarpazhooh, A. Effects of Photodynamic Therapy on Clinical and Gingival Crevicular Fluid Inflammatory Biomarkers in Chronic Periodontitis: A Split-Mouth Randomized Clinical Trial. J. Periodontol. 2014, 85, 1222–1229. [Google Scholar] [CrossRef]
- Rai, B.; Kaur, J.; Jain, R.; Anand, S.C. Levels of gingival crevicular metalloproteinases-8 and -9 in periodontitis. Saudi Dent. J. 2010, 22, 129–131. [Google Scholar] [CrossRef] [Green Version]
- Rai, B.; Kharb, S.; Jain, R.; Anand, S.C. Biomarkers of periodontitis in oral fluids. J. Oral Sci. 2008, 50, 53–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reinhardt, R.A.; Stoner, J.A.; Golub, L.M.; Lee, H.-M.; Nummikoski, P.V.; Sorsa, T.; Payne, J.B. Association of Gingival Crevicular Fluid Biomarkers During Periodontal Maintenance with Subsequent Progressive Periodontitis. J. Periodontol. 2010, 81, 251–259. [Google Scholar] [CrossRef]
- Sorsa, T.; Hernández, M.; Leppilahti, J.; Munjal, S.; Netuschil, L.; Mäntylä, P. Detection of gingival crevicular fluid MMP-8 levels with different laboratory and chair-side methods. Oral Dis. 2010, 16, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Silva, N.; Dutzan, N.; Hernández, M.; Dezerega, A.; Rivera, O.; Aguillón, J.C.; Aravena, O.; Lastres, P.; Pozo, P.; Vernal, R.; et al. Characterization of progressive periodontal lesions in chronic periodontitis patients: Levels of chemokines, cytokines, matrix metalloproteinase-13, periodontal pathogens and inflammatory cells. J. Clin. Periodontol. 2008, 35, 206–214. [Google Scholar] [CrossRef]
- Bozkurt, F.Y.; Ay, Z.Y.; Sütçü, R.; Delibas, N.; Demirel, R. Gingival Crevicular Fluid Leptin Levels in Periodontitis Patients with Long-Term and Heavy Smoking. J. Periodontol. 2006, 77, 634–640. [Google Scholar] [CrossRef] [PubMed]
- Mah, J.; Prasad, N. Dentine phosphoproteins in gingival crevicular fluid during root resorption. Eur. J. Orthod. 2004, 26, 25–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fadel, H.T.; Pliaki, A.; Gronowitz, E.; Mårild, S.; Ramberg, P.; Dahlén, G.; Yucel-Lindberg, T.; Heijl, L.; Birkhed, D. Clinical and biological indicators of dental caries and periodontal disease in adolescents with or without obesity. Clin. Oral Investig. 2014, 18, 359–368. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.; Su, J.; Zou, D.; Mariano, Z. The concentrations of IL-8 and IL-6 in gingival crevicular fluid during nickel–chromium alloy porcelain crown restoration. J. Mater. Sci. Mater. Med. 2013, 24, 1717–1722. [Google Scholar] [CrossRef]
- Tiwari, I.; Mannava, P.; Shetty, S.; Singh, A.; Shrivastava, L.; Verma, S. Clinical and Microbiological Evaluation of Marginal Gingiva Around Direct Composite Veneers. J. Int. Oral Health 2016, 8, 367. [Google Scholar]
- Hamid, H.; Khurshid, Z.; Adanir, N.; Zafar, M.S.; Zohaib, S. COVID-19 Pandemic and Role of Human Saliva as a Testing Biofluid in Point-of-Care Technology. Eur. J. Dent. 2020, 14, S123–S129. [Google Scholar] [CrossRef]
- Sanikop, S.; Patil, S.; Agrawal, P. Gingival crevicular fluid alkaline phosphatase as a potential diagnostic marker of periodontal disease. J. Indian Soc. Periodontol. 2012, 16, 513–518. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study Title | Year of Study | Sample | Biomarkers | Objective | Outcome | References |
|---|---|---|---|---|---|---|
| Correlation of levels of interleukin 1β in gingival crevicular fluid to the clinical parameters of chronic periodontitis. | 2011 | GCF | IL-1β | Correlate IL-1β levels with the clinical parameters of the periodontal disease progression. | IL-1β seems to be a strong correlation between periodontal tissue destruction and IL-1β. Furthermore, IL-1β level could also differentiate between active and inactive periodontal lesions. | [62] |
| Gingival crevicular fluid and plasma acute phase cytokine levels in different periodontal diseases. | 2012 | GCF | IL1-β | To investigate gingival crevicular fluid (GCF) and plasma acute-phase cytokines, interleukin-1b (IL-1b), interleukin-6 (IL-6), interleukin11 (IL-11), oncostatin M (OSM), and leukemia inhibitory factor (LIF) levels in patients with different periodontal diseases. | Chronic periodontitis (CP) and generalized aggressive periodontitis (GAgP) groups had significantly higher GCF IL-1b, IL-6, and IL-11 levels when compared with the healthy group. | [63] |
| Gingival crevicular fluid MMP-8 and -13 and TIMP-1 Levels in patients with rheumatoid arthritis and inflammatory periodontal disease. | 2009 | GCF | MMP-13 MMP-8 | To compare GCF levels of matrix metalloproteinase (MMP)-8 and -13 and tissue inhibitor of MMP (TIMP)-1 in patients with rheumatoid arthritis (RA) and systemically healthy counterparts with inflammatory periodontal disease. | The total amounts of MMP-8 were lower in the healthy control group than in RA-gingivitis, RA-periodontitis, and healthy/periodontitis groups. Patients with RA and gingivitis or periodontitis exhibited levels of MMP-8 and -13 and TIMP-1 that were similar to systemically healthy counterparts. | [64] |
| Correlations between pentraxin 3 or cytokine levels in gingival crevicular fluid and clinical parameters of chronic periodontitis. | 2012 | GCF | IL-1β | To determine the levels of IL-1β, IL-6, IL-8, TNF-α, IL-10 and PTX3 in GCF from diseased and healthy sites in patients with chronic periodontitis. | The mean level of PTX3 in diseased sites was approximately 10 times higher than in healthy sites. Additionally, the mean levels of IL-1β, IL-6, IL-8, IL-10 and TNF-α were significantly higher in diseased sites as compared to healthy sites. | [65] |
| Crevicular fluid biomarkers and periodontal disease progression. | 2014 | GCF, Saliva | MMP-8, MMP-9, Osteoprotegerin, C-reactive Protein and IL-1β. | Assess the ability of a panel of GCF biomarkers as predictors of periodontal disease progression (PDP). | Except for GCF C-reactive protein, all biomarkers were significantly higher in the PDP group compared to stable patients. | [66] |
| The effect of adjunctive chlorhexidine mouth rinse on GCF MMP-8 and TIMP-1 levels in gingivitis: a randomized placebo-controlled study. | 2014 | GCF | TIMP-1 | To evaluate the effect of adjunctive chlorhexidine (CHX) mouth rinse on GCF MMP-8 and TIMP-1 levels in plaque-associated gingivitis. | CHX usage had no significant effects on the GCF MMP-8 and TIMP-1 levels in plaque-associated gingivitis. However, daily plaque control increased GCF TIMP-1 levels regardless of CHX usage. | [67] |
| Gingival crevicular fluid levels of MMP-8, MMP-9, TIMP-2, and MPO decrease after periodontal therapy. | 2010 | GCF | MMP-8, MMP-9, TIMP-2, and MPO | Comparing the levels of MMP-8, TIMP-1 and TIMP-2, Myeloperoxidase (MPO), and MMP-9 in the GCF of CP patients and controls at baseline and 3 months after non-surgical therapy. | Higher levels of MMP-8, TIMP-2, MPO, and 87 kDa MMP-9 were found in the GCF of patients compared with controls, and these markers decreased 3 months after periodontal therapy. | [68] |
| Effects of photodynamic therapy on clinical and gingival crevicular fluid inflammatory biomarkers in chronic periodontitis: A split-mouth randomized clinical trial. | 2014 | GCF | Interleukin-1b, tumor necrosis factor (TNF)-a, and MMP-8 and -9 | Compare the clinical parameters and cytokine profiles in the gingival crevicular fluid of patients with moderate-to-severe chronic periodontitis who have been treated using scaling and root planing (SRP) alone or SRP + photodynamic therapy (PDT). | It was concluded that the addition of PDT (using a 638-nm laser and toluidine blue) to SRP did not provide any additional improvements in the clinical or biologic parameters of periodontitis. | [69] |
| Levels of gingival crevicular metalloproteinases-8 and -9 in periodontitis. | 2010 | GCF | MMP-8 and MMP-9 | To determine the levels of GCF MMP-8 and -9 in patients with periodontitis and healthy controls. | Crevicular MMP-8 and -9 may serve as biomarkers of periodontal disease and aid in early detection of periodontitis. | [70] |
| Biomarkers of periodontitis in oral fluids. | 2008 | GCF, saliva | MMP-8, MMP-9, and MMP-2 | Compare levels of MMP-2, MMP-9 in GCF and MMP-8 in saliva sample from healthy subjects and patients with gingivitis and periodontitis. | Elevated MMP-8 levels in periodontitis and gingivitis subjects compared to controls, similarly increased MMP-9 levels in GCF of both groups than healthy group. Whereas, MMP-2 was lower in both groups compared to the healthy group. | [71] |
| Association of gingival crevicular fluid biomarkers during periodontal maintenance with subsequent progressive periodontitis. | 2010 | GCF | MMP-8, IL-1β, SDD, ICTP (Carboxyterminaltelopeptide cross-link fragment of type I collagen) | Correlate GCF biomarkers of inflammation and bone resorption with subsequent periodontal attachment and bone loss in a longitudinal trial of a matrix metalloproteinase (MMP)-inhibitor. | Elevated GCF biomarkers of inflammation and bone resorption from a small number of moderate/deep sites hold promise in identifying patients vulnerable to progressive periodontitis, and SDD may modify that risk. | [72] |
| Detection of gingival crevicular fluid MMP-8 levels with different laboratory and chair-side methods. | 2010 | GCF | MMP-8 | To compare four methods for GCF MMP-8 detection; IFMA, dentoAnalyzer, MMP-8 dipstick test, Amersham ELISA kit. | Investigated levels of GCF MMP-8 with two different chair-side and two laboratory methods. IFMA, dentoAnalyzer and MMP-8 specific chair-side dip-stick test results were well in line. | [73] |
| Characterization of progressive periodontal lesions in chronic periodontitis patients: levels of chemokines, cytokines, matrix metalloproteinase-13, periodontal pathogens and inflammatory cell. | 2008 | GCF | IL-1β, RANK-L, MCP-1, TNF-α, MMP-13, periodontal pathogen | To determine the levels of chemokine, cytokine, MMP-13, periodontal pathogen, and inflammatory cells in periodontal sites by active periodontal connective destruction. | Higher RANK-L, IL-1β and MMP-13 activity levels observed in active site. | [74] |
| Gingival crevicular fluid leptin levels in periodontitis patients with long term and heavy smoking. | 2006 | GCF | Leptin levels | Assess the levels of leptin in patients with chronic periodontitis via GCF. | High GCF levels of leptin in healthy sites in periodontitis patients suggesting a protective role of Leptin in periodontal disease. | [75] |
| Dentin phosphoprotein in gingival crevicular fluid during root resorption. | 2004 | GCF | Dentine phosphoprotein (DPP) | External apical root resorption measurement using dentine phosphoprotein during orthodontic treatment. | DPP is most abundant in GCF of an exfoliating tooth, the lesser amount is found in apical root resorption in teeth associated with orthodontic treatment. | [76] |
| Clinical and biological indicators of dental caries and periodontal disease in adolescents with or without obesity. | 2014 | GCF samples, Unstimulated and paraffin stimulated whole saliva samples. | SIgAlevels, BMI | This study aimed to assess clinical, microbiological and inflammatory parameters as indicators for caries and periodontal disease. | No significant differences in any of the measured inflammatory markers in GCF were observed between the two groups. | [77] |
| The concentrations of IL-8 and IL-6 in gingival crevicular fluid during nickel-chromium alloy porcelain crown restoration. | 2013 | GCF sample | IL-8 and IL-6 | Explored gum irritation and cytotoxicity caused by nickel-chromium (Ni-Cr) alloy porcelain by IL-8, IL-6 and GCF volumes at different time point’ speri-crown restoration. | IL-8 and IL-6 during nickel-chromium alloy porcelain crown restoration relates to cytotoxicity induced by Ni–Cr alloy. Thus, should be used with caution in clinical practice, especially in the female population. | [78] |
| Clinical and microbiological evaluation of marginal gingiva around direct composite veneers. | 2016 | GCF sample | Clinical and microbiological markers | To evaluate clinically and microbiologically the gingival margins around direct composite veneers. | The volumetric analysis of GCF at the baseline showed lower mean GCF compared to post-veneer placement after 8 weeks, which was statically significant. Microbiologically, no statistically significant difference was seen at the baseline and 8 weeks after veneers placement. Therefore, direct composite veneers can be used as a treatment modality for mild to moderate fluorosis cases. | [79] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bibi, T.; Khurshid, Z.; Rehman, A.; Imran, E.; Srivastava, K.C.; Shrivastava, D. Gingival Crevicular Fluid (GCF): A Diagnostic Tool for the Detection of Periodontal Health and Diseases. Molecules 2021, 26, 1208. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules26051208
Bibi T, Khurshid Z, Rehman A, Imran E, Srivastava KC, Shrivastava D. Gingival Crevicular Fluid (GCF): A Diagnostic Tool for the Detection of Periodontal Health and Diseases. Molecules. 2021; 26(5):1208. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules26051208
Chicago/Turabian StyleBibi, Tauqeer, Zohaib Khurshid, Ambreen Rehman, Eisha Imran, Kumar Chandan Srivastava, and Deepti Shrivastava. 2021. "Gingival Crevicular Fluid (GCF): A Diagnostic Tool for the Detection of Periodontal Health and Diseases" Molecules 26, no. 5: 1208. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules26051208