
Progress in Targeted Alpha-Particle-Emitting Radiopharmaceuticals as Treatments for Prostate Cancer Patients with Bone Metastases


Abstract
:1. Introduction
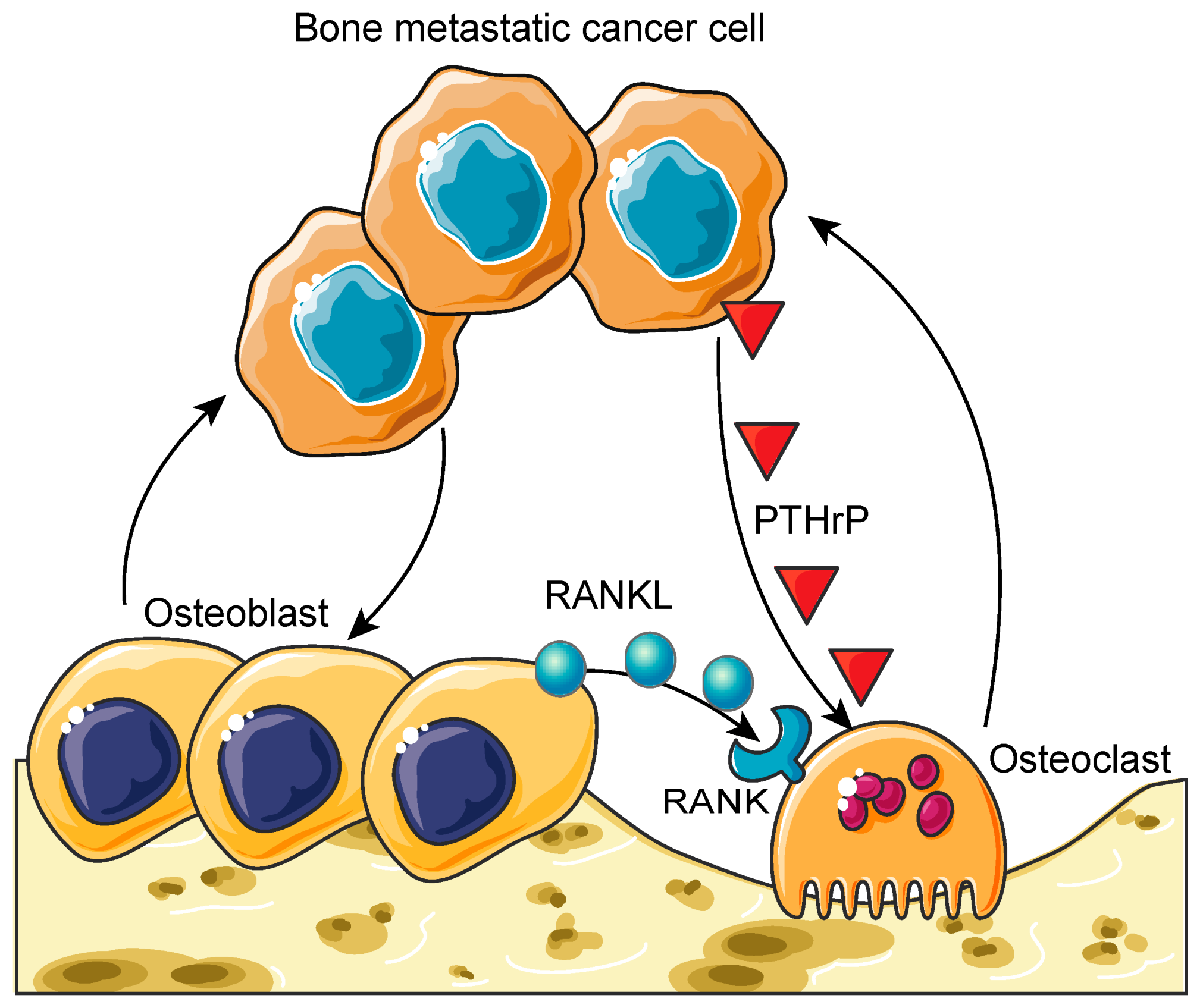
2. The Biology of the Vicious Cycle of Bone Metastases
3. Treatment of Bone Metastases
3.1. Radiopharmaceuticals for Bone Metastases
3.2. Targeted Radiopharmaceuticals for Bone Metastases
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Seyfried, T.N.; Huysentruyt, L.C. On the origin of cancer metastasis. Crit. Rev. Oncog. 2013, 18, 43–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macedo, F.; Ladeira, K.; Pinho, F.; Saraiva, N.; Bonito, N.; Pinto, L.; Goncalves, F. Bone Metastases: An Overview. Oncol. Rev. 2017, 11, 321. [Google Scholar] [PubMed]
- Selvaggi, G.; Scagliotti, G.V. Management of bone metastases in cancer: A review. Crit. Rev. Oncol. Hematol. 2005, 56, 365–378. [Google Scholar] [CrossRef] [PubMed]
- Hagiwara, M.; Delea, T.E.; Chung, K. Healthcare costs associated with skeletal-related events in breast cancer patients with bone metastases. J. Med. Econ. 2014, 17, 223–230. [Google Scholar] [CrossRef]
- Barlev, A.; Song, X.; Ivanov, B.; Setty, V.; Chung, K. Payer costs for inpatient treatment of pathologic fracture, surgery to bone, and spinal cord compression among patients with multiple myeloma or bone metastasis secondary to prostate or breast cancer. J. Manag. Care Pharm. 2010, 16, 693–702. [Google Scholar] [CrossRef] [PubMed]
- Delea, T.; Langer, C.; McKiernan, J.; Liss, M.; Edelsberg, J.; Brandman, J.; Sung, J.; Raut, M.; Oster, G. The cost of treatment of skeletal-related events in patients with bone metastases from lung cancer. Oncology 2004, 67, 390–396. [Google Scholar] [CrossRef]
- Delea, T.; McKiernan, J.; Brandman, J.; Edelsberg, J.; Sung, J.; Raut, M.; Oster, G. Retrospective study of the effect of skeletal complications on total medical care costs in patients with bone metastases of breast cancer seen in typical clinical practice. J. Support. Oncol. 2006, 4, 341–347. [Google Scholar]
- Delea, T.E.; McKiernan, J.; Brandman, J.; Edelsberg, J.; Sung, J.; Raut, M.; Oster, G. Impact of skeletal complications on total medical care costs among patients with bone metastases of lung cancer. J. Thorac. Oncol. 2006, 1, 571–576. [Google Scholar] [CrossRef]
- Lage, M.J.; Barber, B.L.; Harrison, D.J.; Jun, S. The cost of treating skeletal-related events in patients with prostate cancer. Am. J. Manag. Care 2008, 14, 317–322. [Google Scholar]
- Krupski, T.L.; Foley, K.A.; Baser, O.; Long, S.; Macarios, D.; Litwin, M.S. Health care cost associated with prostate cancer, androgen deprivation therapy and bone complications. J. Urol. 2007, 178, 1423–1428. [Google Scholar] [CrossRef]
- Groot, M.T.; Boeken Kruger, C.G.; Pelger, R.C.; Uyl-de Groot, C.A. Costs of prostate cancer, metastatic to the bone, in the Netherlands. Eur. Urol. 2003, 43, 226–232. [Google Scholar] [CrossRef]
- Duran, I.; Garzon, C.; Sanchez, A.; Garcia-Carbonero, I.; Perez-Gracia, J.L.; Segui-Palmer, M.A.; Wei, R.; Restovic, G.; Gasquet, J.A.; Gutierrez, L. Cost analysis of skeletal-related events in Spanish patients with bone metastases from solid tumours. Clin. Transl. Oncol. 2014, 16, 322–329. [Google Scholar] [CrossRef] [Green Version]
- Hechmati, G.; Cure, S.; Gouepo, A.; Hoefeler, H.; Lorusso, V.; Luftner, D.; Duran, I.; Garzon-Rodriguez, C.; Ashcroft, J.; Wei, R.; et al. Cost of skeletal-related events in European patients with solid tumours and bone metastases: Data from a prospective multinational observational study. J. Med. Econ. 2013, 16, 691–700. [Google Scholar] [CrossRef] [PubMed]
- Tangirala, K.; Appukkuttan, S.; Simmons, S. Costs and Healthcare Resource Utilization Associated with Hospital Admissions of Patients with Metastatic or Nonmetastatic Prostate Cancer. Am. Health Drug Benef. 2019, 12, 306–312. [Google Scholar]
- Hadjidakis, D.J.; Androulakis, I.I. Bone remodeling. Ann. N. Y. Acad. Sci. 2006, 1092, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Guise, T.A. The vicious cycle of bone metastases. J. Musculoskelet. Neuronal. Interact. 2002, 2, 570–572. [Google Scholar] [PubMed]
- Stopeck, A.T.; Lipton, A.; Body, J.J.; Steger, G.G.; Tonkin, K.; de Boer, R.H.; Lichinitser, M.; Fujiwara, Y.; Yardley, D.A.; Viniegra, M.; et al. Denosumab compared with zoledronic acid for the treatment of bone metastases in patients with advanced breast cancer: A randomized, double-blind study. J. Clin. Oncol. 2010, 28, 5132–5139. [Google Scholar] [CrossRef] [Green Version]
- Fizazi, K.; Carducci, M.; Smith, M.; Damiao, R.; Brown, J.; Karsh, L.; Milecki, P.; Shore, N.; Rader, M.; Wang, H.; et al. Denosumab versus zoledronic acid for treatment of bone metastases in men with castration-resistant prostate cancer: A randomised, double-blind study. Lancet 2011, 377, 813–822. [Google Scholar] [CrossRef] [Green Version]
- McCain, J. Drugs that offer a survival advantage for men with bone metastases resulting from castration-resistant prostate cancer: New and emerging treatment options. Pharm. Ther. 2014, 39, 130–143. [Google Scholar]
- Nguyen, N.C.; Shah, M.; Appleman, L.J.; Parikh, R.; Mountz, J.M. Radium-223 Therapy for Patients with Metastatic Castrate-Resistant Prostate Cancer: An Update on Literature with Case Presentation. Int. J. Mol. Imaging 2016, 2016, 2568031. [Google Scholar] [CrossRef] [PubMed]
- Vogelzang, N.J.; Coleman, R.E.; Michalski, J.M.; Nilsson, S.; O’Sullivan, J.M.; Parker, C.; Widmark, A.; Thuresson, M.; Xu, L.; Germino, J.; et al. Hematologic Safety of Radium-223 Dichloride: Baseline Prognostic Factors Associated with Myelosuppression in the ALSYMPCA Trial. Clin. Genitourin Cancer 2017, 15, 42–52. [Google Scholar] [CrossRef] [Green Version]
- Wadas, T.J.; Pandya, D.N.; Solingapuram Sai, K.K.; Mintz, A. Molecular targeted alpha-particle therapy for oncologic applications. AJR Am. J. Roentgenol. 2014, 203, 253–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scheinberg, D.A.; McDevitt, M.R. Actinium-225 in targeted alpha-particle therapeutic applications. Curr. RadioPharm. 2011, 4, 306–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamazaki, H.; Nakamura, S.; Suzuki, G.; Yoshida, K.; Yoshioka, Y.; Koizumi, M.; Ogawa, K. Hypofractionated Radiotherapy for Localized Prostate Cancer: A Challenging Accelerated Hypofractionated Radiotherapy. Anticancer Res. 2015, 35, 5167–5177. [Google Scholar] [PubMed]
- Lewis, B.; Chalhoub, E.; Chalouhy, C.; Sartor, O. Radium-223 in Bone-Metastatic Prostate Cancer: Current Data and Future Prospects. Oncology (Williston Park) 2015, 29, 483–488. [Google Scholar] [PubMed]
- de Kruijff, R.M.; Wolterbeek, H.T.; Denkova, A.G. A Critical Review of Alpha Radionuclide Therapy-How to Deal with Recoiling Daughters? Pharmaceuticals (Basel) 2015, 8, 321–336. [Google Scholar] [CrossRef]
- Guerard, F.; Barbet, J.; Chatal, J.F.; Kraeber-Bodere, F.; Cherel, M.; Haddad, F. Which radionuclide, carrier molecule and clinical indication for alpha-immunotherapy? Q. J. Nucl. Med. Mol. Imaging 2015, 59, 161–167. [Google Scholar]
- McGann, S.; Horton, E.R. Radium-223 dichloride: A novel treatment option for castration-resistant prostate cancer patients with symptomatic bone metastases. Ann. Pharmacother. 2015, 49, 469–476. [Google Scholar] [CrossRef]
- Qi, W.X.; Fu, S.; Zhang, Q.; Guo, X.M. Charged particle therapy versus photon therapy for patients with hepatocellular carcinoma: A systematic review and meta-analysis. Radiother. Oncol. 2015, 114, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Buroni, F.E.; Persico, M.G.; Pasi, F.; Lodola, L.; Nano, R.; Aprile, C. Radium-223: Insight and Perspectives in Bone-metastatic Castration-resistant Prostate Cancer. Anticancer Res. 2016, 36, 5719–5730. [Google Scholar] [CrossRef] [Green Version]
- Cordier, D.; Krolicki, L.; Morgenstern, A.; Merlo, A. Targeted Radiolabeled Compounds in Glioma Therapy. Semin. Nucl. Med. 2016, 46, 243–249. [Google Scholar] [CrossRef]
- Ettari, R.; Previti, S.; Bitto, A.; Grasso, S.; Zappala, M. Immunoproteasome-Selective Inhibitors: A Promising Strategy to Treat Hematologic Malignancies, Autoimmune and Inflammatory Diseases. Curr. Med. Chem. 2016, 23, 1217–1238. [Google Scholar] [CrossRef]
- Sgouros, G.; Bodei, L.; McDevitt, M.R.; Nedrow, J.R. Radiopharmaceutical therapy in cancer: Clinical advances and challenges. Nat. Rev. Drug Discov. 2020, 19, 589–608. [Google Scholar] [CrossRef]
- Tafreshi, N.K.; Doligalski, M.L.; Tichacek, C.J.; Pandya, D.N.; Budzevich, M.M.; El-Haddad, G.; Khushalani, N.I.; Moros, E.G.; McLaughlin, M.L.; Wadas, T.J.; et al. Development of Targeted Alpha Particle Therapy for Solid Tumors. Molecules 2019, 24, 4314. [Google Scholar] [CrossRef] [Green Version]
- Schaue, D.; McBride, W.H. Opportunities and challenges of radiotherapy for treating cancer. Nat. Rev. Clin. Oncol. 2015, 12, 527–540. [Google Scholar] [CrossRef]
- Laurenti, E.; Gottgens, B. From haematopoietic stem cells to complex differentiation landscapes. Nature 2018, 553, 418–426. [Google Scholar] [CrossRef]
- Shiozawa, Y.; Taichman, R.S. Getting blood from bone: An emerging understanding of the role that osteoblasts play in regulating hematopoietic stem cells within their niche. Exp. Hematol. 2012, 40, 685–694. [Google Scholar] [CrossRef] [Green Version]
- Galan-Diez, M.; Kousteni, S. The osteoblastic niche in hematopoiesis and hematological myeloid malignancies. Curr. Mol. Biol. Rep. 2017, 3, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Yin, T.; Li, L. The stem cell niches in bone. J. Clin. Investig. 2006, 116, 1195–1201. [Google Scholar] [CrossRef]
- Askmyr, M.; Sims, N.A.; Martin, T.J.; Purton, L.E. What is the true nature of the osteoblastic hematopoietic stem cell niche? Trends Endocrinol. Metab. 2009, 20, 303–309. [Google Scholar] [CrossRef]
- Szade, K.; Gulati, G.S.; Chan, C.K.F.; Kao, K.S.; Miyanishi, M.; Marjon, K.D.; Sinha, R.; George, B.M.; Chen, J.Y.; Weissman, I.L. Where Hematopoietic Stem Cells Live: The Bone Marrow Niche. Antioxid. Redox Signal. 2018, 29, 191–204. [Google Scholar] [CrossRef]
- Pinho, S.; Frenette, P.S. Haematopoietic stem cell activity and interactions with the niche. Nat. Rev. Mol. Cell Biol. 2019, 20, 303–320. [Google Scholar] [CrossRef]
- Jung, Y.; Song, J.; Shiozawa, Y.; Wang, J.; Wang, Z.; Williams, B.; Havens, A.; Schneider, A.; Ge, C.; Franceschi, R.T.; et al. Hematopoietic stem cells regulate mesenchymal stromal cell induction into osteoblasts thereby participating in the formation of the stem cell niche. Stem Cells 2008, 26, 2042–2051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, X.; Wang, Z.; Duan, N.; Zhu, G.; Schwarz, E.M.; Xie, C. Osteoblast-osteoclast interactions. Connect. Tissue Res. 2018, 59, 99–107. [Google Scholar] [CrossRef]
- Sims, N.A.; Martin, T.J. Coupling the activities of bone formation and resorption: A multitude of signals within the basic multicellular unit. Bonekey Rep. 2014, 3, 481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vessella, R.L.; Corey, E. Targeting factors involved in bone remodeling as treatment strategies in prostate cancer bone metastasis. Clin. Cancer Res. 2006, 12, 6285s–6290s. [Google Scholar] [CrossRef] [Green Version]
- Paget, S. The distribution of secondary growths in cancer of the breast. 1889. Cancer Metastasis Rev. 1989, 8, 98–101. [Google Scholar]
- Raubenheimer, E.J.; Noffke, C.E. Pathogenesis of bone metastasis: A review. J. Oral. Pathol. Med. 2006, 35, 129–135. [Google Scholar] [CrossRef]
- Guise, T.A.; Mundy, G.R. Cancer and bone. Endocr. Rev. 1998, 19, 18–54. [Google Scholar]
- Chantrain, C.F.; Feron, O.; Marbaix, E.; DeClerck, Y.A. Bone marrow microenvironment and tumor progression. Cancer Microenviron. 2008, 1, 23–35. [Google Scholar] [CrossRef] [Green Version]
- Cook, L.M.; Shay, G.; Araujo, A.; Lynch, C.C. Integrating new discoveries into the “vicious cycle” paradigm of prostate to bone metastases. Cancer Metastasis Rev. 2014, 33, 511–525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiozawa, Y.; Pedersen, E.A.; Havens, A.M.; Jung, Y.; Mishra, A.; Joseph, J.; Kim, J.K.; Patel, L.R.; Ying, C.; Ziegler, A.M.; et al. Human prostate cancer metastases target the hematopoietic stem cell niche to establish footholds in mouse bone marrow. J. Clin. Investig. 2011, 121, 1298–1312. [Google Scholar] [CrossRef] [Green Version]
- Shiozawa, Y.; Berry, J.E.; Eber, M.R.; Jung, Y.; Yumoto, K.; Cackowski, F.C.; Yoon, H.J.; Parsana, P.; Mehra, R.; Wang, J.; et al. The marrow niche controls the cancer stem cell phenotype of disseminated prostate cancer. Oncotarget 2016, 7, 41217–41232. [Google Scholar] [CrossRef] [Green Version]
- Hage, W.D.; Aboulafia, A.J.; Aboulafia, D.M. Incidence, location, and diagnostic evaluation of metastatic bone disease. Orthop. Clin. N. Am. 2000, 31, 515–528. [Google Scholar] [CrossRef]
- Mundy, G.R. Metastasis to bone: Causes, consequences and therapeutic opportunities. Nat. Rev. Cancer 2002, 2, 584–593. [Google Scholar] [CrossRef]
- Taube, T.; Elomaa, I.; Blomqvist, C.; Beneton, M.N.; Kanis, J.A. Histomorphometric evidence for osteoclast-mediated bone resorption in metastatic breast cancer. Bone 1994, 15, 161–166. [Google Scholar] [CrossRef]
- Martin, T.J. Osteoblast-derived PTHrP is a physiological regulator of bone formation. J. Clin. Investig. 2005, 115, 2322–2324. [Google Scholar] [CrossRef] [Green Version]
- Iwamura, M.; di Sant’Agnese, P.A.; Wu, G.; Benning, C.M.; Cockett, A.T.; Deftos, L.J.; Abrahamsson, P.A. Immunohistochemical localization of parathyroid hormone-related protein in human prostate cancer. Cancer Res. 1993, 53, 1724–1726. [Google Scholar] [PubMed]
- Weilbaecher, K.N.; Guise, T.A.; McCauley, L.K. Cancer to bone: A fatal attraction. Nat. Rev. Cancer 2011, 11, 411–425. [Google Scholar] [CrossRef]
- Keller, E.T.; Brown, J. Prostate cancer bone metastases promote both osteolytic and osteoblastic activity. J. Cell Biochem. 2004, 91, 718–729. [Google Scholar] [CrossRef] [Green Version]
- Ganguly, S.S.; Li, X.; Miranti, C.K. The host microenvironment influences prostate cancer invasion, systemic spread, bone colonization, and osteoblastic metastasis. Front. Oncol. 2014, 4, 364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kohli, S.S.; Kohli, V.S. Role of RANKL-RANK/osteoprotegerin molecular complex in bone remodeling and its immunopathologic implications. Indian J. Endocrinol. Metab. 2011, 15, 175–181. [Google Scholar] [CrossRef]
- Pinski, J.; Dorff, T.B. Prostate cancer metastases to bone: Pathophysiology, pain management, and the promise of targeted therapy. Eur. J. Cancer 2005, 41, 932–940. [Google Scholar] [CrossRef]
- Lipton, A. Management of bone metastases in breast cancer. Curr. Treat. Options Oncol. 2005, 6, 161–171. [Google Scholar] [CrossRef]
- Woolf, D.K.; Padhani, A.R.; Makris, A. Assessing response to treatment of bone metastases from breast cancer: What should be the standard of care? Ann. Oncol. 2015, 26, 1048–1057. [Google Scholar] [CrossRef]
- Parker, C.; Nilsson, S.; Heinrich, D.; Helle, S.I.; O’Sullivan, J.M.; Fossa, S.D.; Chodacki, A.; Wiechno, P.; Logue, J.; Seke, M.; et al. Alpha emitter radium-223 and survival in metastatic prostate cancer. N. Engl. J. Med. 2013, 369, 213–223. [Google Scholar] [CrossRef] [Green Version]
- Badrising, S.K.; van der Noort, V.; Hamberg, P.; Coenen, J.L.; Aarts, M.J.; van Oort, I.M.; van den Eertwegh, A.J.; Los, M.; van den Berg, H.P.; Gelderblom, H.; et al. Enzalutamide as a Fourth- or Fifth-Line Treatment Option for Metastatic Castration-Resistant Prostate Cancer. Oncology 2016, 91, 267–273. [Google Scholar] [CrossRef]
- Vignani, F.; Bertaglia, V.; Buttigliero, C.; Tucci, M.; Scagliotti, G.V.; Di Maio, M. Skeletal metastases and impact of anticancer and bone-targeted agents in patients with castration-resistant prostate cancer. Cancer Treat. Rev. 2016, 44, 61–73. [Google Scholar] [CrossRef]
- Abou, D.S.; Ulmert, D.; Doucet, M.; Hobbs, R.F.; Riddle, R.C.; Thorek, D.L. Whole-Body and Microenvironmental Localization of Radium-223 in Naive and Mouse Models of Prostate Cancer Metastasis. J. Natl Cancer Inst. 2016, 108, djv380. [Google Scholar] [CrossRef] [Green Version]
- Laird, B.J.; Walley, J.; Murray, G.D.; Clausen, E.; Colvin, L.A.; Fallon, M.T. Characterization of cancer-induced bone pain: An exploratory study. Support. Care Cancer 2011, 19, 1393–1401. [Google Scholar] [CrossRef]
- De Felice, F.; Piccioli, A.; Musio, D.; Tombolini, V. The role of radiation therapy in bone metastases management. Oncotarget 2017, 8, 25691–25699. [Google Scholar] [CrossRef] [Green Version]
- Kassis, A.I.; Adelstein, S.J. Radiobiologic principles in radionuclide therapy. J. Nucl. Med. 2005, 46 (Suppl. 1), 4S–12S. [Google Scholar] [PubMed]
- Cole, A. Absorption of 20-eV to 50,000-eV electron beams in air and plastic. Radiat. Res. 1969, 38, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Kassis, A.I.; Adelstein, S.J.; Haydock, C.; Sastry, K.S.; McElvany, K.D.; Welch, M.J. Lethality of Auger electrons from the decay of bromine-77 in the DNA of mammalian cells. Radiat. Res. 1982, 90, 362–373. [Google Scholar] [CrossRef]
- Kassis, A.I.; Sastry, K.S.; Adelstein, S.J. Kinetics of uptake, retention, and radiotoxicity of 125IUdR in mammalian cells: Implications of localized energy deposition by Auger processes. Radiat. Res. 1987, 109, 78–89. [Google Scholar] [CrossRef]
- Walicka, M.A.; Vaidyanathan, G.; Zalutsky, M.R.; Adelstein, S.J.; Kassis, A.I. Survival and DNA damage in Chinese hamster V79 cells exposed to alpha particles emitted by DNA-incorporated astatine-211. Radiat. Res. 1998, 150, 263–268. [Google Scholar] [CrossRef]
- Goddu, S.M.; Howell, R.W.; Rao, D.V. Cellular dosimetry: Absorbed fractions for monoenergetic electron and alpha particle sources and S-values for radionuclides uniformly distributed in different cell compartments. J. Nucl. Med. 1994, 35, 303–316. [Google Scholar] [PubMed]
- Choi, J.Y. Treatment of Bone Metastasis with Bone-Targeting Radiopharmaceuticals. Nucl. Med. Mol. Imaging 2018, 52, 200–207. [Google Scholar] [CrossRef]
- Paes, F.M.; Serafini, A.N. Systemic metabolic radiopharmaceutical therapy in the treatment of metastatic bone pain. Semin Nucl. Med. 2010, 40, 89–104. [Google Scholar] [CrossRef]
- Lepareur, N.; Lacoeuille, F.; Bouvry, C.; Hindre, F.; Garcion, E.; Cherel, M.; Noiret, N.; Garin, E.; Knapp, F.F.R., Jr. Rhenium-188 Labeled Radiopharmaceuticals: Current Clinical Applications in Oncology and Promising Perspectives. Front. Med. (Lausanne) 2019, 6, 132. [Google Scholar] [CrossRef] [Green Version]
- Alavi, M.; Omidvari, S.; Mehdizadeh, A.; Jalilian, A.R.; Bahrami-Samani, A. Metastatic Bone Pain Palliation using (177)Lu-Ethylenediaminetetramethylene Phosphonic Acid. World J. Nucl. Med. 2015, 14, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Friedell, H.L.; Storaasli, J.P. The use of radioactive phosphorus in the treatment of carcinoma of the breast with widespread metastases to bone. Am. J. Roentgenol. Radium Ther. 1950, 64, 559–575. [Google Scholar] [PubMed]
- Maxfield, J.R., Jr.; Maxfield, J.G.; Maxfield, W.S. The use of radioactive phosphorus and testosterone in metastatic bone lesions from breast and prostate. South. Med. J. 1958, 51, 320–327. [Google Scholar] [CrossRef]
- Miller, A.D. Radiophosphorous (P32) treatment in carcinoma of the breast and prostate: Report of 39 cases. J. Am. Osteopath Assoc. 1974, 74, 217–222. [Google Scholar] [PubMed]
- Cheung, A.; Driedger, A.A. Evaluation of radioactive phosphorus in the palliation of metastatic bone lesions from carcinoma of the breast and prostate. Radiology 1980, 134, 209–212. [Google Scholar] [CrossRef]
- Silberstein, E.B. The treatment of painful osseous metastases with phosphorus-32-labeled phosphates. Semin. Oncol. 1993, 20 (Suppl. 2), 10–21. [Google Scholar]
- Nair, N. Relative efficacy of 32P and 89Sr in palliation in skeletal metastases. J. Nucl. Med. 1999, 40, 256–261. [Google Scholar]
- Blake, G.M.; Zivanovic, M.A.; McEwan, A.J.; Ackery, D.M. Sr-89 therapy: Strontium kinetics in disseminated carcinoma of the prostate. Eur. J. Nucl. Med. 1986, 12, 447–454. [Google Scholar] [CrossRef]
- Finlay, I.G.; Mason, M.D.; Shelley, M. Radioisotopes for the palliation of metastatic bone cancer: A systematic review. Lancet Oncol. 2005, 6, 392–400. [Google Scholar] [CrossRef]
- Silberstein, E.B.; Williams, C. Strontium-89 therapy for the pain of osseous metastases. J. Nucl. Med. 1985, 26, 345–348. [Google Scholar] [PubMed]
- Robinson, R.G.; Preston, D.F.; Spicer, J.A.; Baxter, K.G. Radionuclide therapy of intractable bone pain: Emphasis on strontium-89. Semin. Nucl. Med. 1992, 22, 28–32. [Google Scholar] [CrossRef]
- Mertens, W.C.; Stitt, L.; Porter, A.T. Strontium 89 therapy and relief of pain in patients with prostatic carcinoma metastatic to bone: A dose response relationship? Am. J. Clin. Oncol. 1993, 16, 238–242. [Google Scholar] [CrossRef]
- Maxon, H.R., 3rd; Schroder, L.E.; Thomas, S.R.; Hertzberg, V.S.; Deutsch, E.A.; Scher, H.I.; Samaratunga, R.C.; Libson, K.F.; Williams, C.C.; Moulton, J.S.; et al. Re-186(Sn) HEDP for treatment of painful osseous metastases: Initial clinical experience in 20 patients with hormone-resistant prostate cancer. Radiology 1990, 176, 155–159. [Google Scholar] [CrossRef]
- Giannakenas, C.; Kalofonos, H.P.; Apostolopoulos, D.J.; Zarakovitis, J.; Kosmas, C.; Vassilakos, P.J. Preliminary results of the use of Re-186-HEDP for palliation of pain in patients with metastatic bone disease. Am. J. Clin. Oncol. 2000, 23, 83–88. [Google Scholar] [CrossRef]
- Kolesnikov-Gauthier, H.; Carpentier, P.; Depreux, P.; Vennin, P.; Caty, A.; Sulman, C. Evaluation of toxicity and efficacy of 186Re-hydroxyethylidene diphosphonate in patients with painful bone metastases of prostate or breast cancer. J. Nucl. Med. 2000, 41, 1689–1694. [Google Scholar]
- Sciuto, R.; Tofani, A.; Festa, A.; Giannarelli, D.; Pasqualoni, R.; Maini, C.L. Short- and long-term effects of 186Re-1,1-hydroxyethylidene diphosphonate in the treatment of painful bone metastases. J. Nucl. Med. 2000, 41, 647–654. [Google Scholar]
- Quirijnen, J.M.; Han, S.H.; Zonnenberg, B.A.; de Klerk, J.M.; van het Schip, A.D.; van Dijk, A.; ten Kroode, H.F.; Blijham, G.H.; van Rijk, P.P. Efficacy of rhenium-186-etidronate in prostate cancer patients with metastatic bone pain. J. Nucl. Med. 1996, 37, 1511–1515. [Google Scholar]
- Maxon, H.R., 3rd; Schroder, L.E.; Hertzberg, V.S.; Thomas, S.R.; Englaro, E.E.; Samaratunga, R.; Smith, H.; Moulton, J.S.; Williams, C.C.; Ehrhardt, G.J.; et al. Rhenium-186(Sn)HEDP for treatment of painful osseous metastases: Results of a double-blind crossover comparison with placebo. J. Nucl. Med. 1991, 32, 1877–1881. [Google Scholar]
- Han, S.H.; de Klerk, J.M.; Tan, S.; van het Schip, A.D.; Derksen, B.H.; van Dijk, A.; Kruitwagen, C.L.; Blijham, G.H.; van Rijk, P.P.; Zonnenberg, B.A. The PLACORHEN study: A double-blind, placebo-controlled, randomized radionuclide study with (186)Re-etidronate in hormone-resistant prostate cancer patients with painful bone metastases. Placebo Controlled Rhenium Study. J. Nucl. Med. 2002, 43, 1150–1156. [Google Scholar]
- Liepe, K. (188)Re-HEDP therapy in the therapy of painful bone metastases. World J. Nucl. Med. 2018, 17, 133–138. [Google Scholar] [CrossRef]
- Liepe, K.; Kotzerke, J. A comparative study of 188Re-HEDP, 186Re-HEDP, 153Sm-EDTMP and 89Sr in the treatment of painful skeletal metastases. Nucl. Med. Commun. 2007, 28, 623–630. [Google Scholar] [CrossRef]
- Resche, I.; Chatal, J.F.; Pecking, A.; Ell, P.; Duchesne, G.; Rubens, R.; Fogelman, I.; Houston, S.; Fauser, A.; Fischer, M.; et al. A dose-controlled study of 153Sm-ethylenediaminetetramethylenephosphonate (EDTMP) in the treatment of patients with painful bone metastases. Eur. J. Cancer 1997, 33, 1583–1591. [Google Scholar] [CrossRef]
- Tian, J.H.; Zhang, J.M.; Hou, Q.T.; Oyang, Q.H.; Wang, J.M.; Luan, Z.S.; Chuan, L.; He, Y.J. Multicentre trial on the efficacy and toxicity of single-dose samarium-153-ethylene diamine tetramethylene phosphonate as a palliative treatment for painful skeletal metastases in China. Eur. J. Nucl. Med. 1999, 26, 2–7. [Google Scholar] [CrossRef] [PubMed]
- Yadav, M.P.; Ballal, S.; Sahoo, R.K.; Dwivedi, S.N.; Bal, C. Radioligand Therapy With (177)Lu-PSMA for Metastatic Castration-Resistant Prostate Cancer: A Systematic Review and Meta-Analysis. AJR Am. J. Roentgenol. 2019, 213, 275–285. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, S.; Das, T.; Banerjee, S.; Balogh, L.; Chaudhari, P.R.; Sarma, H.D.; Polyak, A.; Mathe, D.; Venkatesh, M.; Janoki, G.; et al. 177Lu-EDTMP: A viable bone pain palliative in skeletal metastasis. Cancer Biother. Radio Pharm. 2008, 23, 202–213. [Google Scholar] [CrossRef] [PubMed]
- Mathe, D.; Balogh, L.; Polyak, A.; Kiraly, R.; Marian, T.; Pawlak, D.; Zaknun, J.J.; Pillai, M.R.; Janoki, G.A. Multispecies animal investigation on biodistribution, pharmacokinetics and toxicity of 177Lu-EDTMP, a potential bone pain palliation agent. Nucl. Med. Biol. 2010, 37, 215–226. [Google Scholar] [CrossRef]
- Agarwal, K.K.; Singla, S.; Arora, G.; Bal, C. (177)Lu-EDTMP for palliation of pain from bone metastases in patients with prostate and breast cancer: A phase II study. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, S.; Das, T.; Sarma, H.D.; Venkatesh, M.; Banerjee, S. Comparative studies of 177Lu-EDTMP and 177Lu-DOTMP as potential agents for palliative radiotherapy of bone metastasis. Appl. Radiat. Isot. 2008, 66, 1196–1205. [Google Scholar] [CrossRef]
- Das, T.; Shinto, A.; Karuppuswamy Kamaleshwaran, K.; Banerjee, S. Theranostic Treatment of Metastatic Bone Pain with 177Lu-DOTMP. Clin. Nucl. Med. 2016, 41, 966–967. [Google Scholar] [CrossRef]
- Bahrami-Samani, A.; Anvari, A.; Jalilian, A.R.; Shirvani-Arani, S.; Yousefnia, H.; Aghamiri, M.R.; Ghannadi-Maragheh, M. Production, Quality Control and Pharmacokinetic Studies of (177)Lu-EDTMP for Human Bone Pain Palliation Therapy Trials. Iran. J. Pharm. Res. 2012, 11, 137–144. [Google Scholar]
- Yousefnia, H.; Zolghadri, S.; Jalilian, A.R. Absorbed dose assessment of (177)Lu-zoledronate and (177)Lu-EDTMP for human based on biodistribution data in rats. J. Med. Phys. 2015, 40, 102–108. [Google Scholar] [PubMed]
- Yadav, M.P.; Ballal, S.; Meckel, M.; Roesch, F.; Bal, C. [(177)Lu]Lu-DOTA-ZOL bone pain palliation in patients with skeletal metastases from various cancers: Efficacy and safety results. EJNMMI Res. 2020, 10, 130. [Google Scholar] [CrossRef] [PubMed]
- Wissing, M.D.; van Leeuwen, F.W.; van der Pluijm, G.; Gelderblom, H. Radium-223 chloride: Extending life in prostate cancer patients by treating bone metastases. Clin. Cancer Res. 2013, 19, 5822–5827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kassis, A.I. Therapeutic radionuclides: Biophysical and radiobiologic principles. Semin Nucl. Med. 2008, 38, 358–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baidoo, K.E.; Yong, K.; Brechbiel, M.W. Molecular pathways: Targeted alpha-particle radiation therapy. Clin. Cancer Res. 2013, 19, 530–537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sgouros, G.; Hobbs, R.F.; Song, H. Modelling and dosimetry for alpha-particle therapy. Curr. Radio Pharm. 2011, 4, 261–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, H.; Hobbs, R.F.; Vajravelu, R.; Huso, D.L.; Esaias, C.; Apostolidis, C.; Morgenstern, A.; Sgouros, G. Radioimmunotherapy of breast cancer metastases with alpha-particle emitter 225Ac: Comparing efficacy with 213Bi and 90Y. Cancer Res. 2009, 69, 8941–8948. [Google Scholar] [CrossRef] [Green Version]
- Saad, F.; Carles, J.; Gillessen, S.; Heidenreich, A.; Heinrich, D.; Gratt, J.; Levy, J.; Miller, K.; Nilsson, S.; Petrenciuc, O.; et al. Radium-223 and concomitant therapies in patients with metastatic castration-resistant prostate cancer: An international, early access, open-label, single-arm phase 3b trial. Lancet Oncol. 2016, 17, 1306–1316. [Google Scholar] [CrossRef]
- Delgado Bolton, R.C.; Giammarile, F. Bone radionuclide therapy and increased survival with radium-223 is the way to go for nuclear medicine: The offer that oncologists cannot refuse. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 822–823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gravis, G. Systemic treatment for metastatic prostate cancer. Asian J. Urol. 2019, 6, 162–168. [Google Scholar] [CrossRef]
- Smith, M.; Parker, C.; Saad, F.; Miller, K.; Tombal, B.; Ng, Q.S.; Boegemann, M.; Matveev, V.; Piulats, J.M.; Zucca, L.E.; et al. Addition of radium-223 to abiraterone acetate and prednisone or prednisolone in patients with castration-resistant prostate cancer and bone metastases (ERA 223): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019, 20, 408–419. [Google Scholar] [CrossRef]
- Chang, S.S. Overview of prostate-specific membrane antigen. Rev. Urol. 2004, 6 (Suppl. 10), S13–S18. [Google Scholar] [PubMed]
- Hupe, M.C.; Philippi, C.; Roth, D.; Kumpers, C.; Ribbat-Idel, J.; Becker, F.; Joerg, V.; Duensing, S.; Lubczyk, V.H.; Kirfel, J.; et al. Expression of Prostate-Specific Membrane Antigen (PSMA) on Biopsies Is an Independent Risk Stratifier of Prostate Cancer Patients at Time of Initial Diagnosis. Front. Oncol. 2018, 8, 623. [Google Scholar] [CrossRef]
- Sun, M.; Niaz, M.O.; Nelson, A.; Skafida, M.; Niaz, M.J. Review of 177Lu-PSMA-617 in Patients with Metastatic Castration-Resistant Prostate Cancer. Cureus 2020, 12, e8921. [Google Scholar] [CrossRef]
- Hofman, M.S.; Violet, J.; Hicks, R.J.; Ferdinandus, J.; Thang, S.P.; Akhurst, T.; Iravani, A.; Kong, G.; Ravi Kumar, A.; Murphy, D.G.; et al. [(177)Lu]-PSMA-617 radionuclide treatment in patients with metastatic castration-resistant prostate cancer (LuPSMA trial): A single-centre, single-arm, phase 2 study. Lancet Oncol. 2018, 19, 825–833. [Google Scholar] [CrossRef]
- Rahbar, K.; Bodei, L.; Morris, M.J. Is the Vision of Radioligand Therapy for Prostate Cancer Becoming a Reality? An Overview of the Phase III VISION Trial and Its Importance for the Future of Theranostics. J. Nucl. Med. 2019, 60, 1504–1506. [Google Scholar] [CrossRef] [Green Version]
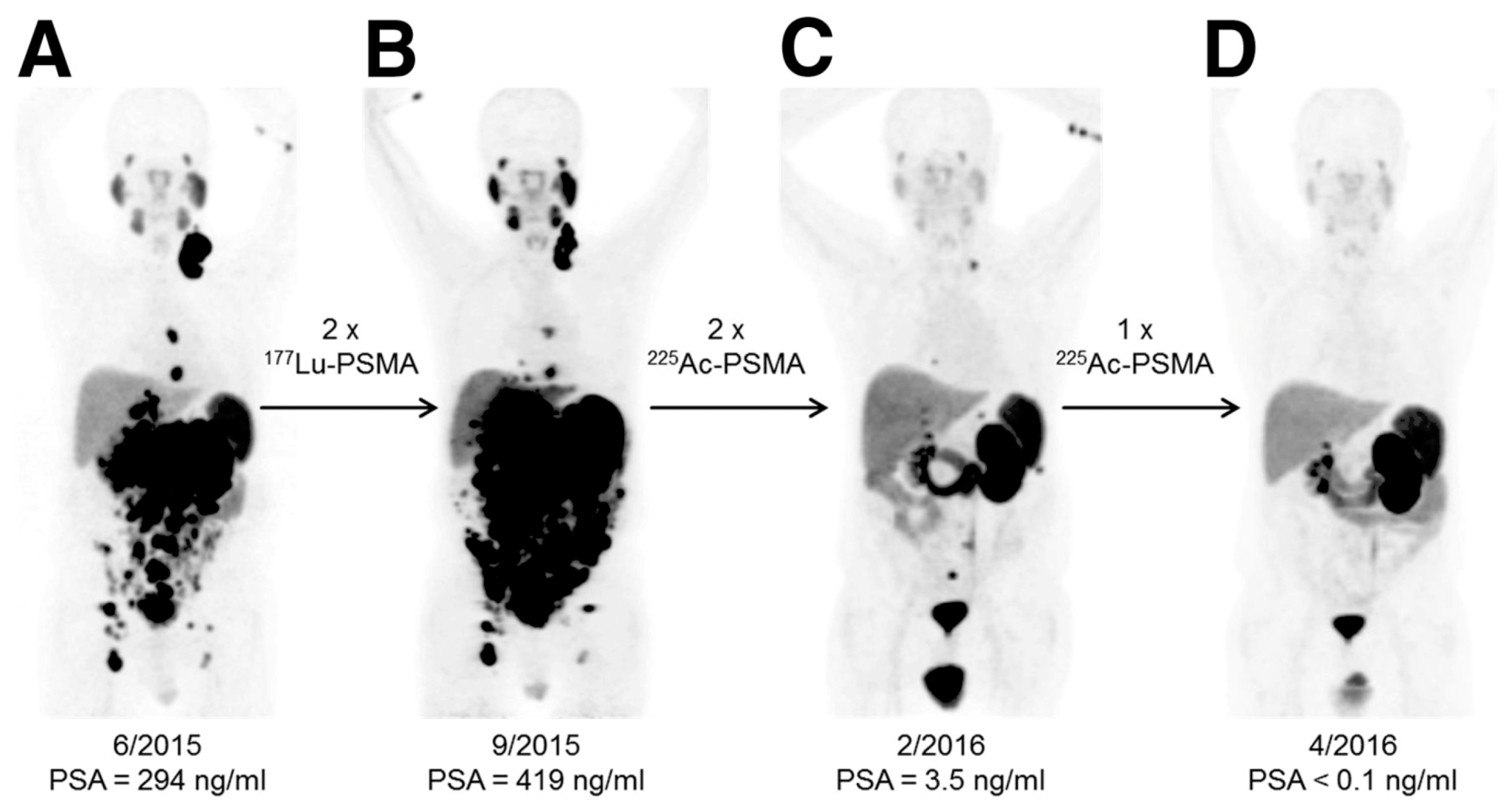
- Kratochwil, C.; Bruchertseifer, F.; Giesel, F.L.; Weis, M.; Verburg, F.A.; Mottaghy, F.; Kopka, K.; Apostolidis, C.; Haberkorn, U.; Morgenstern, A. 225Ac-PSMA-617 for PSMA-Targeted alpha-Radiation Therapy of Metastatic Castration-Resistant Prostate Cancer. J. Nucl. Med. 2016, 57, 1941–1944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yadav, M.P.; Ballal, S.; Sahoo, R.K.; Tripathi, M.; Seth, A.; Bal, C. Efficacy and safety of (225)Ac-PSMA-617 targeted alpha therapy in metastatic castration-resistant Prostate Cancer patients. Theranostics 2020, 10, 9364–9377. [Google Scholar] [CrossRef] [PubMed]
- Kratochwil, C.; Haberkorn, U.; Giesel, F.L. (225)Ac-PSMA-617 for Therapy of Prostate Cancer. Semin. Nucl. Med. 2020, 50, 133–140. [Google Scholar] [CrossRef]
- Deblonde, G.J.; Abergel, R.J. Active actinium. Nat. Chem. 2016, 8, 1084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vasiliev, A.; Severin, A.; Lapshina, E.; Chernykh, E.; Ermolaev, S.; Kalmykov, S. Hydroxylapatite particles as carriers for 223Ra. J. Radioanal. Nuclear Chem. 2016, 311, 1503–1509. [Google Scholar] [CrossRef]
- McDevitt, M.R.; Ma, D.; Simon, J.; Frank, R.K.; Scheinberg, D.A. Design and synthesis of 225Ac radioimmunopharmaceuticals. Appl. Radiat. Isot. 2002, 57, 841–847. [Google Scholar] [CrossRef]
- Sofou, S.; Kappel, B.J.; Jaggi, J.S.; McDevitt, M.R.; Scheinberg, D.A.; Sgouros, G. Enhanced retention of the alpha-particle-emitting daughters of Actinium-225 by liposome carriers. Bioconjug. Chem. 2007, 18, 2061–2067. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antczak, C.; Jaggi, J.S.; LeFave, C.V.; Curcio, M.J.; McDevitt, M.R.; Scheinberg, D.A. Influence of the linker on the biodistribution and catabolism of actinium-225 self-immolative tumor-targeted isotope generators. Bioconjug. Chem. 2006, 17, 1551–1560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borchardt, P.E.; Yuan, R.R.; Miederer, M.; McDevitt, M.R.; Scheinberg, D.A. Targeted actinium-225 in vivo generators for therapy of ovarian cancer. Cancer Res. 2003, 63, 5084–5090. [Google Scholar]
- Davis, I.A.; Glowienka, K.A.; Boll, R.A.; Deal, K.A.; Brechbiel, M.W.; Stabin, M.; Bochsler, P.N.; Mirzadeh, S.; Kennel, S.J. Comparison of 225actinium chelates: Tissue distribution and radiotoxicity. Nucl. Med. Biol. 1999, 26, 581–589. [Google Scholar] [CrossRef]
- Deal, K.A.; Davis, I.A.; Mirzadeh, S.; Kennel, S.J.; Brechbiel, M.W. Improved in vivo stability of actinium-225 macrocyclic complexes. J. Med. Chem. 1999, 42, 2988–2992. [Google Scholar] [CrossRef] [PubMed]
- Sathekge, M.; Bruchertseifer, F.; Knoesen, O.; Reyneke, F.; Lawal, I.; Lengana, T.; Davis, C.; Mahapane, J.; Corbett, C.; Vorster, M.; et al. (225)Ac-PSMA-617 in chemotherapy-naive patients with advanced prostate cancer: A pilot study. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 129–138. [Google Scholar] [CrossRef] [Green Version]
- Paganelli, G.; Sarnelli, A.; Severi, S.; Sansovini, M.; Belli, M.L.; Monti, M.; Foca, F.; Celli, M.; Nicolini, S.; Tardelli, E.; et al. Dosimetry and safety of (177)Lu PSMA-617 along with polyglutamate parotid gland protector: Preliminary results in metastatic castration-resistant prostate cancer patients. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 3008–3017. [Google Scholar] [CrossRef]
- Langbein, T.; Chausse, G.; Baum, R.P. Salivary Gland Toxicity of PSMA Radioligand Therapy: Relevance and Preventive Strategies. J. Nucl. Med. 2018, 59, 1172–1173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rathke, H.; Bruchertseifer, F.; Kratochwil, C.; Keller, H.; Giesel, F.L.; Apostolidis, C.; Haberkorn, U.; Morgenstern, A. First patient exceeding 5-year complete remission after (225)Ac-PSMA-TAT. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 311–312. [Google Scholar] [CrossRef] [PubMed]
- Kratochwil, C.; Giesel, F.L.; Heussel, C.P.; Kazdal, D.; Endris, V.; Nientiedt, C.; Bruchertseifer, F.; Kippenberger, M.; Rathke, H.; Leichsenring, J.; et al. Patients Resistant Against PSMA-Targeting alpha-Radiation Therapy Often Harbor Mutations in DNA Damage-Repair-Associated Genes. J. Nucl. Med. 2020, 61, 683–688. [Google Scholar] [CrossRef]
- McDevitt, M.R.; Barendswaard, E.; Ma, D.; Lai, L.; Curcio, M.J.; Sgouros, G.; Ballangrud, A.M.; Yang, W.H.; Finn, R.D.; Pellegrini, V.; et al. An alpha-particle emitting antibody ([213Bi]J591) for radioimmunotherapy of prostate cancer. Cancer Res. 2000, 60, 6095–6100. [Google Scholar]
- Ballangrud, A.M.; Yang, W.H.; Charlton, D.E.; McDevitt, M.R.; Hamacher, K.A.; Panageas, K.S.; Ma, D.; Bander, N.H.; Scheinberg, D.A.; Sgouros, G. Response of LNCaP spheroids after treatment with an alpha-particle emitter (213Bi)-labeled anti-prostate-specific membrane antigen antibody (J591). Cancer Res. 2001, 61, 2008–2014. [Google Scholar] [PubMed]
- Li, Y.; Tian, Z.; Rizvi, S.M.; Bander, N.H.; Allen, B.J. In vitro and preclinical targeted alpha therapy of human prostate cancer with Bi-213 labeled J591 antibody against the prostate specific membrane antigen. Prostate Cancer Prostatic Dis. 2002, 5, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Nonnekens, J.; Chatalic, K.L.; Molkenboer-Kuenen, J.D.; Beerens, C.E.; Bruchertseifer, F.; Morgenstern, A.; Veldhoven-Zweistra, J.; Schottelius, M.; Wester, H.J.; van Gent, D.C.; et al. (213)Bi-Labeled Prostate-Specific Membrane Antigen-Targeting Agents Induce DNA Double-Strand Breaks in Prostate Cancer Xenografts. Cancer Biother. Radio Pharm. 2017, 32, 67–73. [Google Scholar]
- Kiess, A.P.; Minn, I.; Vaidyanathan, G.; Hobbs, R.F.; Josefsson, A.; Shen, C.; Brummet, M.; Chen, Y.; Choi, J.; Koumarianou, E.; et al. (2S)-2-(3-(1-Carboxy-5-(4-211At-Astatobenzamido)Pentyl)Ureido)-Pentanedioic Acid for PSMA-Targeted alpha-Particle Radiopharmaceutical Therapy. J. Nucl. Med. 2016, 57, 1569–1575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khreish, F.; Ebert, N.; Ries, M.; Maus, S.; Rosar, F.; Bohnenberger, H.; Stemler, T.; Saar, M.; Bartholoma, M.; Ezziddin, S. (225)Ac-PSMA-617/(177)Lu-PSMA-617 tandem therapy of metastatic castration-resistant prostate cancer: Pilot experience. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 721–728. [Google Scholar] [CrossRef] [PubMed]
- Hammer, S.; Hagemann, U.B.; Zitzmann-Kolbe, S.; Larsen, A.; Ellingsen, C.; Geraudie, S.; Grant, D.; Indrevoll, B.; Smeets, R.; von Ahsen, O.; et al. Preclinical Efficacy of a PSMA-Targeted Thorium-227 Conjugate (PSMA-TTC), a Targeted Alpha Therapy for Prostate Cancer. Clin. Cancer Res. 2020, 26, 1985–1996. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Decay | Particle | Maximum Particle Range (mm) | Maximum Particle Energy (MeV) | Linear Energy Transfer (kEV/µm) |
|---|---|---|---|---|
| Electron capture internal conversion | Non-energetic electrons | 0.0005 | 0.001 | 26 |
| Beta minus particle | Energetic electrons | 12 | 2.3 | 0.2 |
| Alpha particle | Helium nuclei | 0.1 | 9 | 80 |
| Agent | Conjugator | Development Phase | Refs. |
|---|---|---|---|
| 213Bi-J591 | PSMA-targeting murine monoclonal antibody, J591 | Preclinical study | [143,144,145] |
| 213Bi-PSMA I&T | PSMA-targeting (3S,7S)-29,32-dibenzyl-5,13,20,28,31,34-hexaoxo-37-(4,7,10-tris(carboxymethyl)-1,4,7,10-tetraazacyclododecan-1-yl)-4,6,12,21,27,30,33-heptaazaheptatriacontane-1,3,7,26,37-pentacarboxylic acid (DOTAGA-FFK(Sub-KuE)), PSMA I&T | Preclinical study | [146] |
| 213Bi-JVZ-008 | PSMA-targeting nanobody, JVZ-008 | Preclinical study | [146] |
| 211At-6 | PSMA-targeting (2S)-2-(3-(1-carboxy-5-(4-211At-astatobenzamido)pentyl)ureido)-pentanedioic acid, compound 6 | Preclinical study | [147] |
| 225Ac-PSMA-617 | PSMA-targeting small molecule, PSMA-617 | Clinical study | [127,138,141,148] |
| 227Th-PSMA-TTC | PSMA-targeting fully human antibody, BAY 2315158 | Clinical trial (phase I: NCT03724747) | [149] |
| 225Ac-J591 | PSMA-targeting murine monoclonal antibody, J591 | Clinical trial (phase I: NCT03276572) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patel, C.M.; Wadas, T.J.; Shiozawa, Y. Progress in Targeted Alpha-Particle-Emitting Radiopharmaceuticals as Treatments for Prostate Cancer Patients with Bone Metastases. Molecules 2021, 26, 2162. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules26082162
Patel CM, Wadas TJ, Shiozawa Y. Progress in Targeted Alpha-Particle-Emitting Radiopharmaceuticals as Treatments for Prostate Cancer Patients with Bone Metastases. Molecules. 2021; 26(8):2162. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules26082162
Chicago/Turabian StylePatel, Chirayu M., Thaddeus J. Wadas, and Yusuke Shiozawa. 2021. "Progress in Targeted Alpha-Particle-Emitting Radiopharmaceuticals as Treatments for Prostate Cancer Patients with Bone Metastases" Molecules 26, no. 8: 2162. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules26082162