
Serotonergic Neurotransmission System Modulator, Vortioxetine, and Dopaminergic D2/D3 Receptor Agonist, Ropinirole, Attenuate Fibromyalgia-Like Symptoms in Mice


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
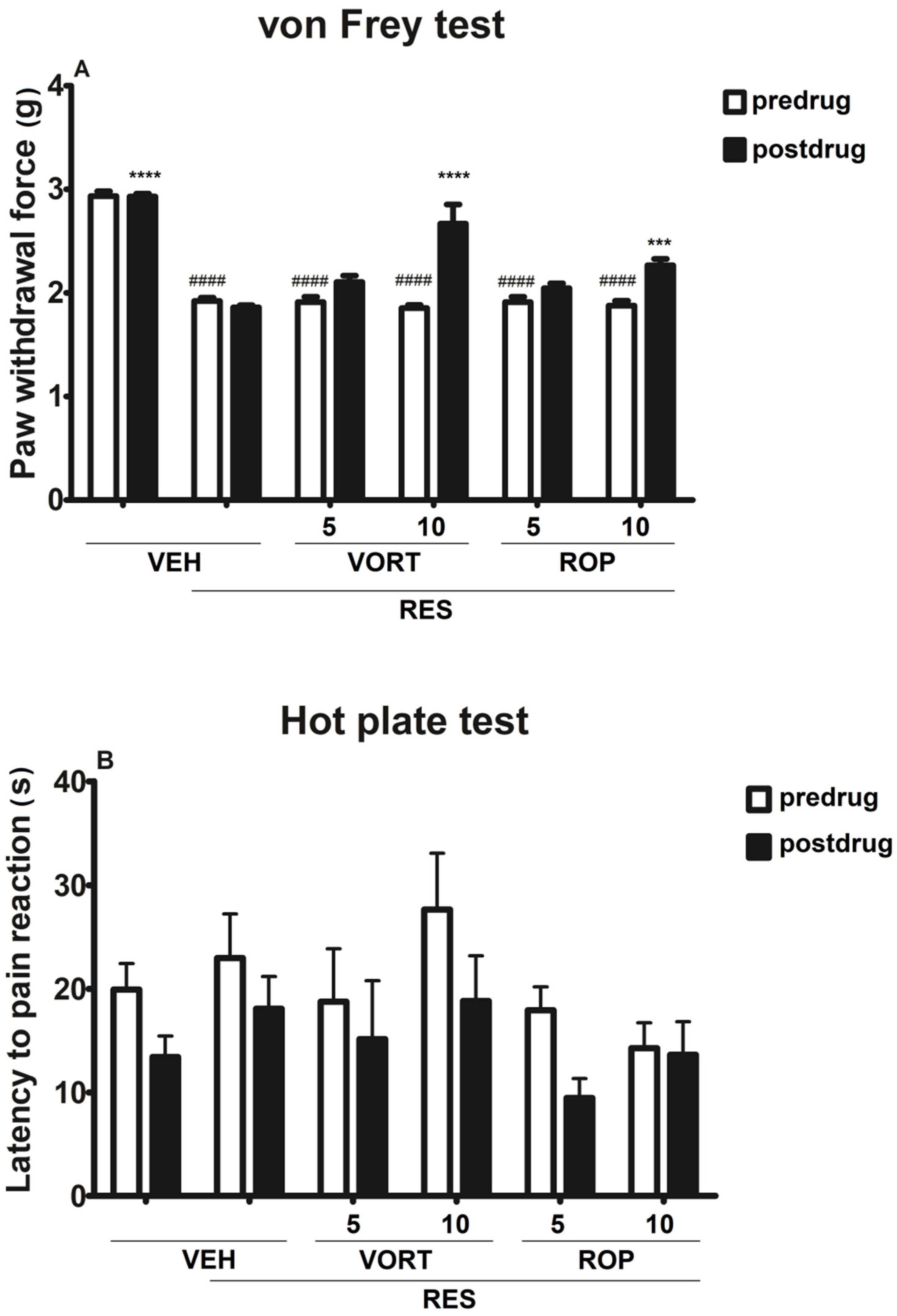
2.1. Effect on Tactile Allodynia (Von Frey Test)
2.2. Effect on Heat Hyperalgesia (Hot Plate Test)
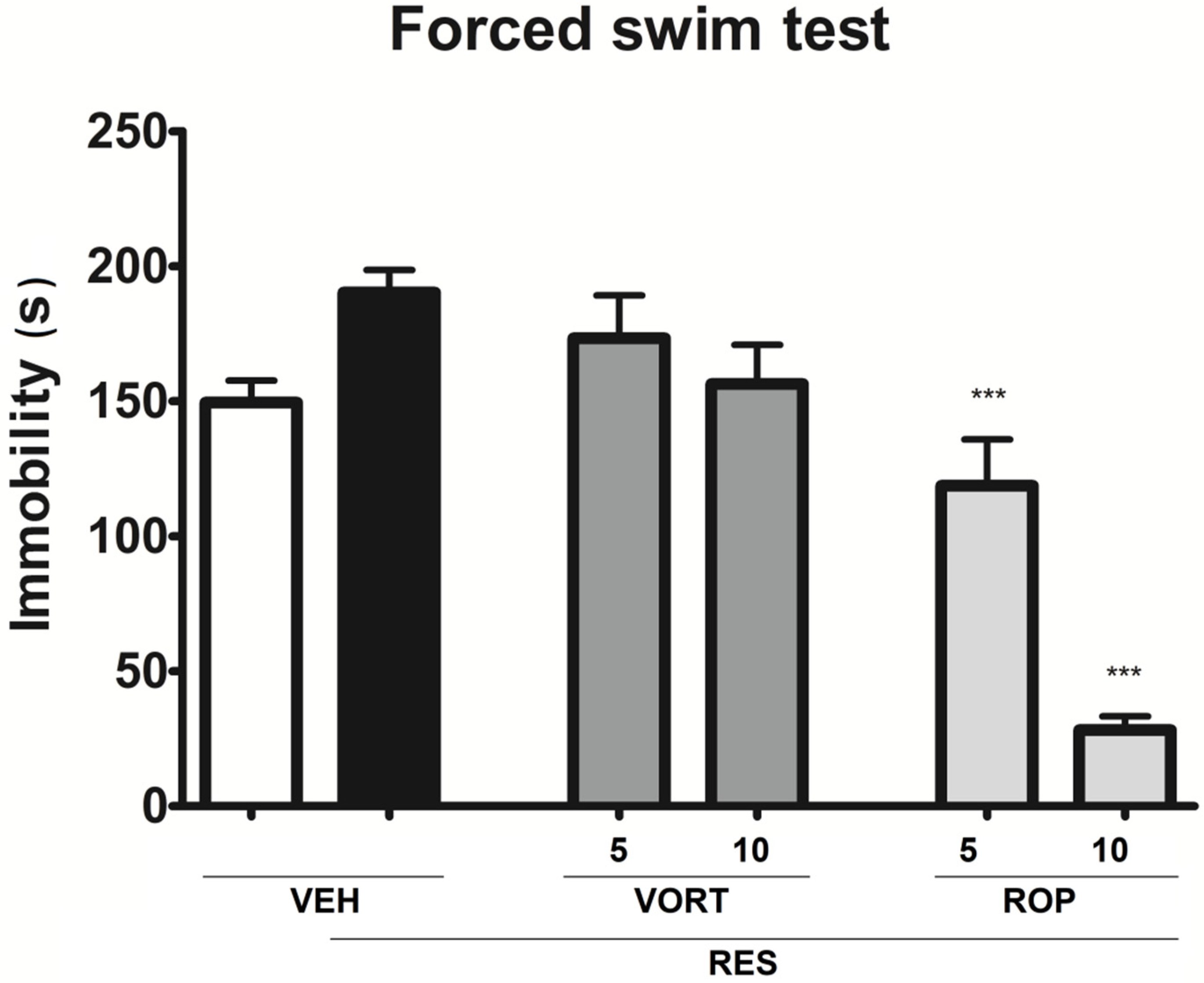
2.3. Effect on Depressive-Like Symptoms (Forced Swim Test; FST)
2.4. Effect on Anxiety-Like Symptoms (Four-Plate Test; FPT)
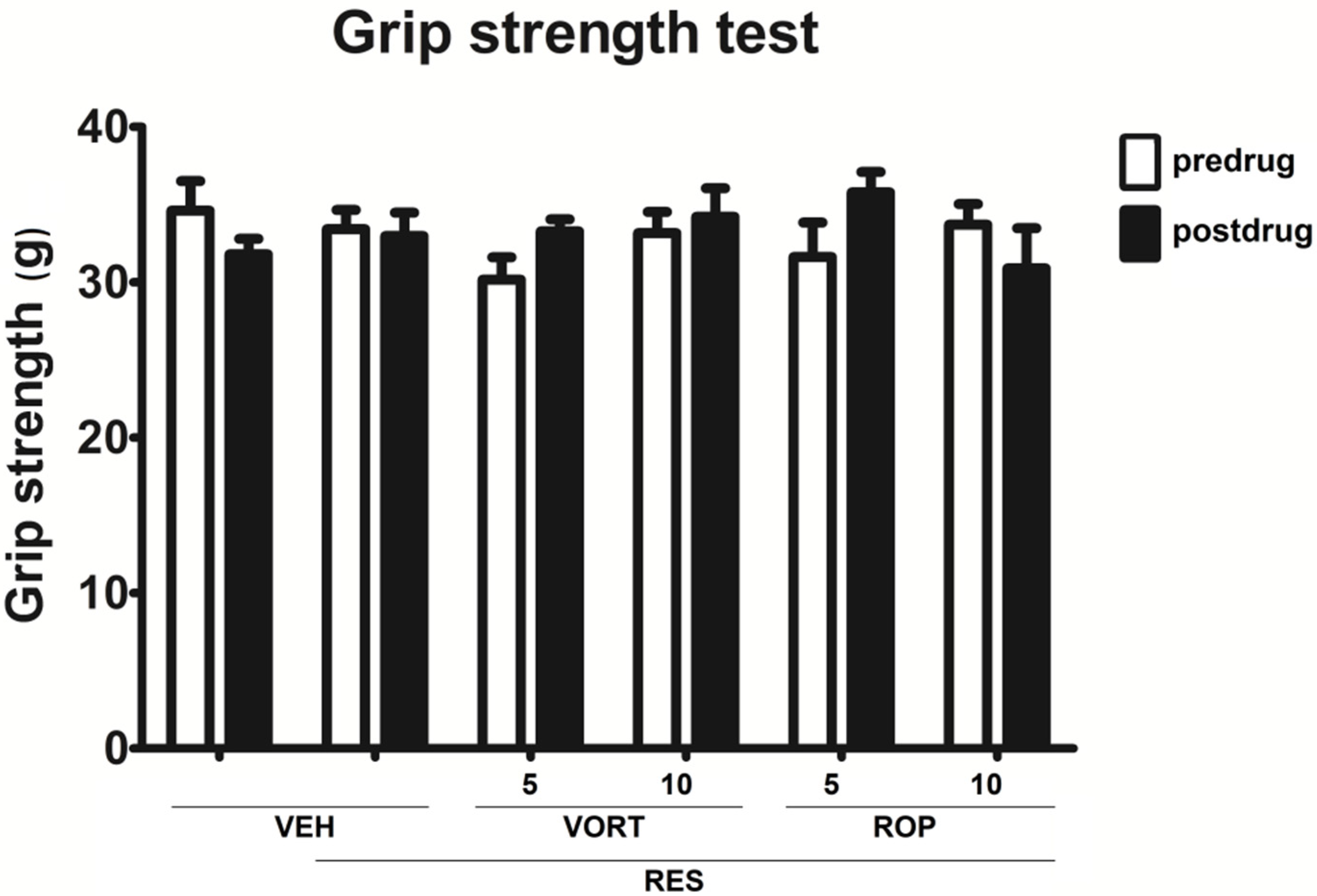
2.5. Effect on Muscle Strength (Grip Strength Test)
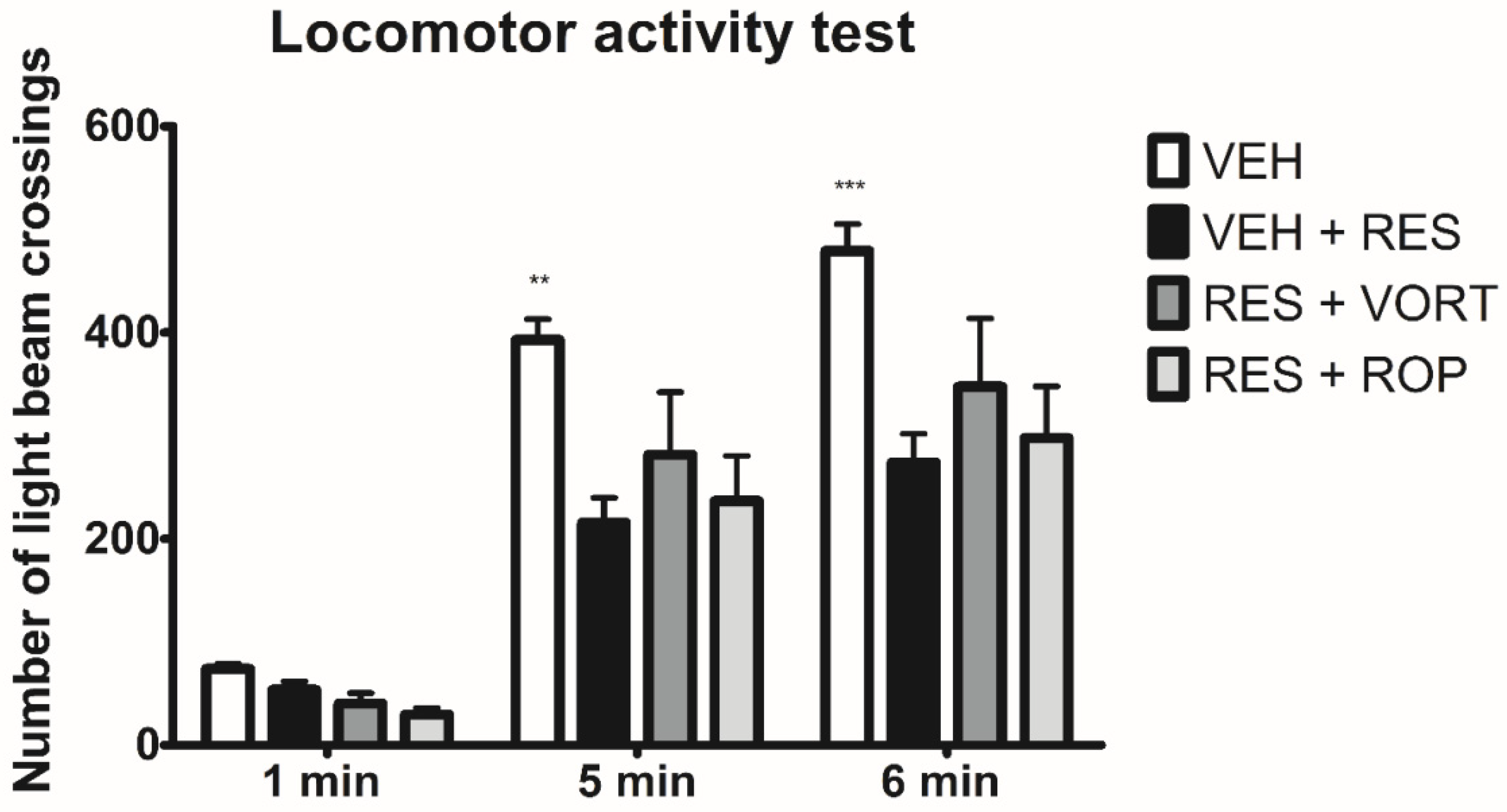
2.6. Effect on Locomotor Activity
3. Discussion
4. Materials and Methods
4.1. Animals and Housing Conditions
4.2. Chemicals
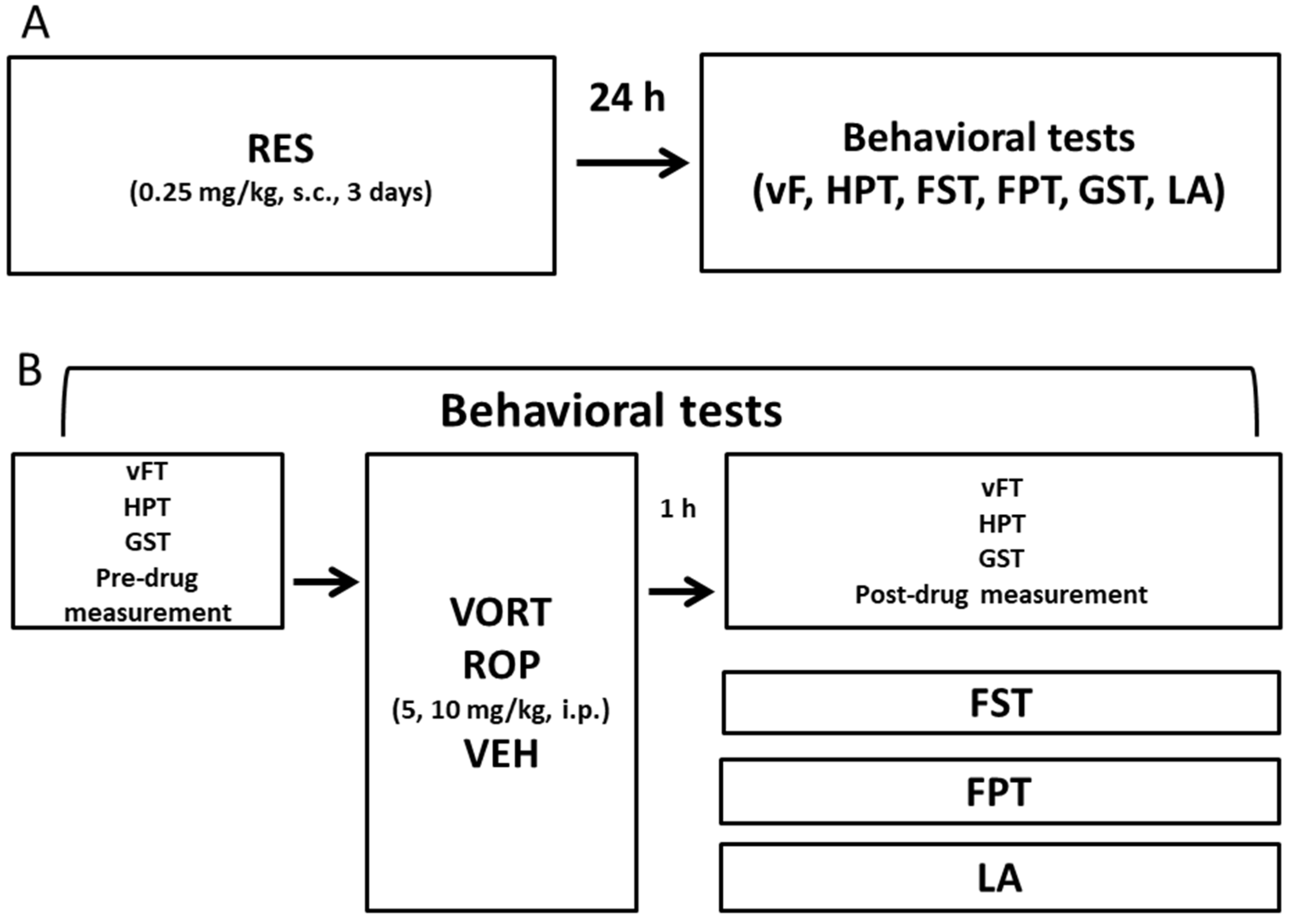
4.3. Induction of FM-Like Model in Mice
4.4. Behavioral Tests
4.4.1. Effect on Pain Threshold
Influence on Tactile Allodynia (Von Frey Test)
Influence on Thermal Hyperalgesia (Hot Plate Test)
4.4.2. Assessment of Antidepressant-Like Activity (Forced Swim Test, FST)
4.4.3. Assessment of Anxiolytic-Like Activity (Four-Plate Test, FPT)
4.4.4. Assessment of the Effect on Muscle Strength (Grip-Strength Test)
4.4.5. Assessment of the Effect on Locomotor Activity
4.5. Data Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Sample Availability
Abbreviations
| FM | Fibromyalgia |
| HTR3 | Serotonergic 5-HT3 receptor gene |
| HPT | Hot plate test |
| FST | Forced swim test |
| FPT | Four-plate test |
| GST | Grip strength test |
| LA | Locomotor activity test |
| SERT | Serotonin transporter |
| RES | Reserpine |
| ROP | Ropinirole |
| VEH | Vehicle |
| vFT | Von Frey test |
| VORT | Vortioxetine |
References
- Sallinen, M.; Kukkurainen, M.L.; Peltokallio, L.; Mikkelsson, M. “I’m tired of being tired”—Fatigue as experienced by women with fibromyalgia. Adv. Physiother. 2011, 13, 11–17. [Google Scholar] [CrossRef]
- Hadlandsmyth, K.; Dailey, D.L.; Rakel, B.A.; Zimmerman, M.B.; Vance, C.G.T.; Merriwether, E.N.; Chimenti, R.L.; Geasland, K.M.; Crofford, L.J.; Sluka, K.A. Somatic symptom presentations in women with fibromyalgia are differentially associated with elevated depression and anxiety. J. Health Psychol. 2017, 25, 819–829. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef] [Green Version]
- Aguilera, M.; Paz, C.; Compañ, V.; Medina, J.C.; Feixas, G. Cognitive rigidity in patients with depression and fibromyalgia. Int. J. Clin. Health Psychol. 2019, 9, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Häuser, W.; Jung, E.; Erbslöh-Möller, B.; Gesmann, M.; Kühn-Becker, H.; Petermann, F.; Langhorst, J.; Thoma, R.; Weiss, T.; Wolfe, F.; et al. The German fibromyalgia consumer reports—A cross-sectional survey. BMC Musculoskelet. Disord. 2012, 13, 74. [Google Scholar] [CrossRef] [Green Version]
- Bennett, R.M.; Jones, J.; Turk, D.C.; Russell, I.J.; Matallana, L. An internet survey of 2596 people with fibromyalgia. BMC Musculoskelet. Disord. 2007, 8, 27. [Google Scholar] [CrossRef]
- Ablin, J.; Fitzcharles, M.A.; Buskila, D.; Shir, Y.; Sommer, C.; Häuser, W. Treatment of fibromyalgia syndrome: Recommendations of recent evidence-based interdisciplinary guidelines with special emphasis on complementary and alternative therapies. Evid. Based Complement. Altern. Med. 2013, 2013. [Google Scholar] [CrossRef] [Green Version]
- Available online: https://www.rheumatology.org/I-Am-A/Patient-Caregiver/Diseases-Conditions/Fibromyalgia (accessed on 24 February 2020).
- Marques, A.P.; Santo, A.S.D.E.; Berssaneti, A.A.; Matsutani, L.A.; Yuan, S.L.K. Prevalence of fibromyalgia: Literature review update. Rev. Bras. Reumatol. 2017, 57, 356–363. [Google Scholar] [CrossRef]
- Smith, S.B.; Maixner, D.W.; Fillingim, R.B.; Slade, G.; Gracely, R.H.; Ambrose, K.; Zaykin, D.V.; Hyde, C.; John, S.; Tan, K.; et al. Large candidate gene association study reveals genetic risk factors and therapeutic targets for fibromyalgia. Arthritis Rheum. 2012, 64, 584–593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruiz-Pérez, I.; Plazaola-Castaño, J.; Cáliz-Cáliz, R.; Rodríguez-Calvo, I.; García-Sánchez, A.; Ferrer-González, M.Á.; Guzmán-Ubeda, M.; del Río-Lozano, M.; López-Chicheri García, I. Risk factors for fibromyalgia: The role of violence against women. Clin. Rheumatol. 2009, 28, 777–786. [Google Scholar] [CrossRef] [PubMed]
- Bradley, L.A. Pathophysiology of Fibromyalgia. Am. J. Med. 2009, 122 (Suppl. 12), S22–S30. [Google Scholar] [CrossRef] [Green Version]
- Goldenberg, D.L. Fibromyalgia Syndrome a Decade Later: What Have We Learned? Arch. Intern. Med. 1999, 159, 777–785. [Google Scholar] [CrossRef] [Green Version]
- Gran, J.T. The epidemiology of chronic generalized musculoskeletal pain. Best Pract. Res. Clin. Rheumatol. 2003, 17, 547–561. [Google Scholar] [CrossRef]
- Ledermann, K.; Hasler, G.; Jenewein, J.; Sprott, H.; Schnyder, U.; Martin-Soelch, C. 5′UTR polymorphism in the serotonergic receptor HTR3A gene is differently associated with striatal Dopamine D2/D3 receptor availability in the right putamen in Fibromyalgia patients and healthy controls-Preliminary evidence. Synapse 2020, 74, e22147. [Google Scholar] [CrossRef]
- Van Houdenhove, B.; Egle, U.; Luyten, P. The role of life stress in fibromyalgia. Curr. Rheumatol. Rep. 2005, 7, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Desmeules, J.A.; Cedraschi, C.; Rapiti, E.; Baumgartner, E.; Finckh, A.; Cohen, P.; Dayer, P.; Vischer, T.L. Neurophysiologic evidence for a central sensitization in patients with fibromyalgia. Arthritis Rheum. 2003, 48, 1420–1429. [Google Scholar] [CrossRef] [PubMed]
- Fitzcharles, M.A.; Boulos, P. Inaccuracy in the diagnosis of fibromyalgia syndrome: Analysis of referrals. Rheumatology 2003, 42, 263–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mease, P. Fibromyalgia syndrome: Review of clinical presentation, pathogenesis, outcome measures, and treatment. J. Rheumatol. Suppl. 2005, 75, 6–21. [Google Scholar]
- Senba, E.; Kami, K. A new aspect of chronic pain as a lifestyle-related disease. Neurobiol. Pain 2017, 1, 6–15. [Google Scholar] [CrossRef] [PubMed]
- Häuser, W. Fibromyalgiesyndrom Basiswissen, Diagnostik und Therapie [Fibromyalgia syndrome: Basic knowledge, diagnosis and treatment]. Med. Monatsschr. Pharm. 2016, 39, 504–511. [Google Scholar]
- Olivier, B. Serotonin: A never-ending story. Eur. J. Pharmacol. 2015, 753, 2–18. [Google Scholar] [CrossRef] [Green Version]
- Štrac, D.Š.; Pivac, N.; Mück-Šeler, D. The serotonergic system and cognitive function. Transl. Neurosci. 2016, 7, 35–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lian, Y.N.; Wang, Y.; Zhang, Y.; Yang, C.X. Duloxetine for pain in fibromyalgia in adults: A systematic review and a meta-analysis. Int. J. Neurosci. 2020, 130, 71–82. [Google Scholar] [CrossRef] [PubMed]
- Welsch, P.; Üçeyler, N.; Klose, P.; Walitt, B.; Häuser, W. Serotonin and noradrenaline reuptake inhibitors (SNRIs) for fibromyalgia. Cochrane Database Syst. Rev. 2018, 2, CD010292. [Google Scholar] [CrossRef] [Green Version]
- Shelton, R.C. Serotonin and Norepinephrine Reuptake Inhibitors. Handb. Exp. Pharmacol. 2019, 250, 145–180. [Google Scholar] [CrossRef]
- Lawson, K. Tricyclic antidepressants and fibromyalgia: What is the mechanism of action? Expert Opin. Investig. Drugs 2002, 11, 1437–1445. [Google Scholar] [CrossRef] [PubMed]
- Häuser, W.; Urrútia, G.; Tort, S.; Uçeyler, N.; Walitt, B. Serotonin and noradrenaline reuptake inhibitors (SNRIs) for fibromyalgia syndrome. Cochrane Database Syst. Rev. 2013, CD010292. [Google Scholar] [CrossRef]
- Walitt, B.; Urrútia, G.; Nishishinya, M.B.; Cantrell, S.E.; Häuser, W. Selective serotonin reuptake inhibitors for fibromyalgia syndrome. Cochrane Database Syst. Rev. 2015, 2015, CD011735. [Google Scholar] [CrossRef]
- Gonda, X.; Sharma, S.R.; Tarazi, F.I. Vortioxetine: A novel antidepressant for the treatment of major depressive disorder. Expert Opin. Drug Discov. 2019, 14, 81–89. [Google Scholar] [CrossRef]
- Okano, H.; Yasuda, D.; Fujimori, K.; Morimoto, S.; Takahashi, S. Ropinirole, a New ALS Drug Candidate Developed Using iPSCs. Trends Pharmacol. Sci. 2020, 41, 99–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albrecht, D.S.; MacKie, P.J.; Kareken, D.A.; Hutchins, G.D.; Chumin, E.J.; Christian, B.T.; Yoder, K.K. Differential dopamine function in fibromyalgia. Brain Imaging Behav. 2016, 10, 829–839. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Borreguero, D.; Silber, M.H.; Winkelman, J.W.; Högl, B.; Bainbridge, J.; Buchfuhrer, M.; Hadjigeorgiou, G.; Inoue, Y.; Manconi, M.; Oertel, W.; et al. Guidelines for the first-line treatment of restless legs syndrome/Willis-Ekbom disease, prevention and treatment of dopaminergic augmentation: A combined task force of the IRLSSG, EURLSSG, and the RLS-foundation. Sleep Med. 2016, 1, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellis, J.M.; Fell, M.J. Current approaches to the treatment of Parkinson’s Disease. Bioorg. Med. Chem. Lett. 2017, 27, 4247–4255. [Google Scholar] [CrossRef] [PubMed]
- Holman, A.J. Ropinirole, open preliminary observations of a dopamine agonist for refractory fibromyalgia. J. Clin. Rheumatol. 2003, 9, 277–279. [Google Scholar] [CrossRef]
- Nagakura, Y.; Oe, T.; Aoki, T.; Matsuoka, N. Biogenic amine depletion causes chronic muscular pain and tactile allodynia accompanied by depression: A putative animal model of fibromyalgia. Pain 2009, 146, 26–33. [Google Scholar] [CrossRef]
- Micov, A.M.; Tomić, M.A.; Todorović, M.B.; Vuković, M.J.; Pecikoza, U.B.; Jasnic, N.I.; Djordjevic, J.D.; Stepanović-Petrović, R.M. Vortioxetine reduces pain hypersensitivity and associated depression-like behavior in mice with oxaliplatin-induced neuropathy. Prog. Neuropsychopharmacol. Biol. Psychiatry 2020, 103, 109975. [Google Scholar] [CrossRef]
- Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2008/020658s018s020s021lbl.pdf (accessed on 1 April 2021).
- Turner, P.V.; Brabb, T.; Pekow, C.; Vasbinder, M.A. Administration of substances to laboratory animals: Routes of administration and factors to consider. J. Am. Assoc. Lab. Anim. Sci. 2011, 50, 600–613. [Google Scholar] [PubMed]
- Sumpton, J.E.; Moulin, D.E. Fibromyalgia. Handb. Clin. Neurol. 2014, 119, 513–527. [Google Scholar] [CrossRef] [PubMed]
- Stahl, S.M. Fibromyalgia-pathways and neurotransmitters. Hum. Psychopharmacol. 2009, 24 (Suppl. 1), S11–S17. [Google Scholar] [CrossRef] [PubMed]
- Paredes, S.; Cantillo, S.; Candido, K.D.; Knezevic, N.N. An Association of Serotonin with Pain Disorders and Its Modulation by Estrogens. Int. J. Mol. Sci. 2019, 20, 5729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maffei, M.E. Fibromyalgia: Recent Advances in Diagnosis, Classification, Pharmacotherapy and Alternative Remedies. Int. J. Mol. Sci. 2020, 21, 7877. [Google Scholar] [CrossRef]
- Wood, P.B.; Glabus, M.F.; Simpson, R.; Patterson, J.C., 2nd. Changes in gray matter density in fibromyalgia: Correlation with dopamine metabolism. J. Pain 2009, 10, 609–618. [Google Scholar] [CrossRef]
- Wood, P.B.; Patterson, J.C., 2nd; Sunderland, J.J.; Tainter, K.H.; Glabus, M.F.; Lilien, D.L. Reduced presynaptic dopamine activity in fibromyalgia syndrome demonstrated with positron emission tomography: A pilot study. J. Pain 2007, 8, 51–58. [Google Scholar] [CrossRef]
- Sung, S.; Vijiaratnam, N.; Chan, D.W.C.; Farrell, M.; Evans, A.H. Pain sensitivity in Parkinson’s disease: Systematic review and meta-analysis. Park. Relat. Disord. 2018, 48, 17–27. [Google Scholar] [CrossRef]
- Valek, L.; Auburger, G.; Tegeder, I. Sensory neuropathy and nociception in rodent models of Parkinson’s disease. DMM Dis. Model. Mech. 2019, 12, dmm039396. [Google Scholar] [CrossRef] [Green Version]
- Wawrzczak-Bargieła, A.; Ziółkowska, B.; Piotrowska, A.; Starnowska-Sokół, J.; Rojewska, E.; Mika, J.; Przewłocka, B.; Przewłocki, R. Neuropathic Pain Dysregulates Gene Expression of the Forebrain Opioid and Dopamine Systems. Neurotox. Res. 2020, 37, 800–814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wood, P.B.; Schweinhardt, P.; Jaeger, E.; Dagher, A.; Hakyemez, H.; Rabiner, E.A.; Bushnell, M.C.; Chizh, B.A. Fibromyalgia patients show an abnormal dopamine response to pain. Eur. J. Neurosci. 2007, 25, 3576–3582. [Google Scholar] [CrossRef] [PubMed]
- Wood, P.B. Role of central dopamine in pain and analgesia. Expert Rev. Neurother. 2008, 8, 781–797. [Google Scholar] [CrossRef]
- Kashyap, P.; Kalaiselvan, V.; Kumar, R.; Kumar, S. Ajmalicine and Reserpine: Indole Alkaloids as Multi-Target Directed Ligands towards Factors Implicated in Alzheimer’s Disease. Molecules 2020, 25, 1609. [Google Scholar] [CrossRef] [Green Version]
- Li, L.M.; Shi, S.D.; Liu, Y.; Zou, Q. Bioactivity-Guided Isolation and Identification of New and Immunosuppressive Monoterpenoid Indole Alkaloids from Rauvolfia yunnanensis Tsiang. Molecules 2019, 24, 4574. [Google Scholar] [CrossRef] [Green Version]
- Celano, C.M.; Freudenreich, O.; Fernandez-Robles, C.; Stern, T.A.; Caro, M.A.; Huffman, J.C. Depressogenic effects of medications: A review. Dialogues Clin. Neurosci. 2011, 13, 109–125. [Google Scholar] [CrossRef]
- Sulser, F.; Brodie, B.B. Is reserpine tranquilization linked to change in brain serotonin or brain norepinephrine? Science 1960, 131, 1440–1441. [Google Scholar] [CrossRef]
- Klein, C.P.; Sperotto, N.D.; Maciel, I.S.; Leite, C.E.; Souza, A.H.; Campos, M.M. Effects of D-series resolvins on behavioral and neurochemical changes in a fibromyalgia-like model in mice. Neuropharmacology 2014, 86, 57–66. [Google Scholar] [CrossRef]
- Leão, A.H.; Sarmento-Silva, A.J.; Santos, J.R.; Ribeiro, A.M.; Silva, R.H. Molecular, Neurochemical, and Behavioral Hallmarks of Reserpine as a Model for Parkinson’s Disease: New Perspectives to a Long-Standing Model. Brain Pathol. 2015, 25, 377–390. [Google Scholar] [CrossRef] [Green Version]
- De Souza, A.H.; Da Costa Lopes, A.M.; Castro, C.J.; Pereira, E.M.R.; Klein, C.P.; Da Silva, C.A.; Da Silva, J.F.; Ferreira, J.; Gomez, M.V. The effects of Phα1β, a spider toxin, calcium channel blocker, in a mouse fibromyalgia model. Toxicon 2014, 81, 37–42. [Google Scholar] [CrossRef]
- Bisong, S.A.; Brown, R.; Osim, E.E. Comparative effects of Rauwolfia vomitoria and chlorpromazine on locomotor behaviour and anxiety in mice. J. Ethnopharmacol. 2010, 132, 334–339. [Google Scholar] [CrossRef]
- Hernandez-Leon, A.; Fernández-Guasti, A.; Martínez, A.; Pellicer, F.; González-Trujano, M.E. Sleep architecture is altered in the reserpine-induced fibromyalgia model in ovariectomized rats. Behav. Brain Res. 2019, 364, 383–392. [Google Scholar] [CrossRef]
- Fischer, S.P.M.; Brusco, I.; Brum, E.S.; Fialho, M.F.P.; Camponogara, C.; Scussel, R.; Machado-de-Ávila, R.A.; Trevisan, G.; Oliveira, S.M. Involvement of TRPV1 and the efficacy of α-spinasterol on experimental fibromyalgia symptoms in mice. Neurochem. Int. 2020, 134, 104673. [Google Scholar] [CrossRef]
- Kaur, A.; Singh, L.; Singh, N.; Bhatti, M.S.; Bhatti, R. Ameliorative effect of imperatorin in chemically induced fibromyalgia: Role of NMDA/NFkB mediated downstream signaling. Biochem. Pharmacol. 2019, 166, 56–69. [Google Scholar] [CrossRef]
- Leal, P.C.; Lins, L.C.; de Gois, A.M.; Marchioro, M.; Santos, J.R. Commentary: Evaluation of Models of Parkinson’s Disease. Front. Neurosci. 2016, 10, 283. [Google Scholar] [CrossRef] [PubMed]
- Fukuzaki, K.; Kamenosono, T.; Nagata, R. Effects of ropinirole on various parkinsonian models in mice, rats, and cynomolgus monkeys. Pharmacol. Biochem. Behav. 2000, 65, 503–508. [Google Scholar] [CrossRef]
- Duty, S.; Jenner, P. Animal models of Parkinson’s disease: A source of novel treatments and clues to the cause of the disease. Br. J. Pharmacol. 2011, 164, 1357–1391. [Google Scholar] [CrossRef] [Green Version]
- Ikram, H.; Haleem, D.J. Repeated treatment with a low dose of reserpine as a progressive model of Parkinson’s dementia. Pak. J. Pharm. Sci. 2019, 32, 555–562. [Google Scholar]
- Leventhal, L.J. Management of Fibromyalgia. Ann. Intern. Med. 1999, 131, 850. [Google Scholar] [CrossRef] [PubMed]
- Oe, T.; Tsukamoto, M.; Nagakura, Y. Reserpine causes biphasic nociceptive sensitivity alteration in conjunction with brain biogenic amine tones in rats. Neuroscience 2010, 169, 1860–1871. [Google Scholar] [CrossRef] [PubMed]
- Sarwer-Foner, G.J.; Ogle, W. Psychosis and enhanced anxiety produced by reserpine and chlorpromazine. Can. Med. Assoc. J. 1956, 74, 526–532. [Google Scholar]
- Zuena, A.R.; Maftei, D.; Alemà, G.S.; Dal Moro, F.; Lattanzi, R.; Casolini, P.; Nicoletti, F. Multimodal antidepressant vortioxetine causes analgesia in a mouse model of chronic neuropathic pain. Mol. Pain 2018, 14, 1744806918808987. [Google Scholar] [CrossRef] [Green Version]
- Adamo, D.; Pecoraro, G.; Aria, M.; Favia, G.; Mignogna, M.D. Vortioxetine in the Treatment of Mood Disorders Associated with Burning Mouth Syndrome: Results of an Open-Label, Flexible-Dose Pilot Study. Pain Med. 2020, 21, 185–194. [Google Scholar] [CrossRef]
- Adamo, D.; Pecoraro, G.; Coppola, N.; Calabria, E.; Aria, M.; Mignogna, M. Vortioxetine versus other antidepressants in the treatment of burning mouth syndrome: An open-label randomized trial. Oral Dis. 2020. [Google Scholar] [CrossRef]
- Tang, D.L.; Luan, Y.W.; Zhou, C.Y.; Xiao, C. D2 receptor activation relieves pain hypersensitivity by inhibiting superficial dorsal horn neurons in parkinsonian mice. Acta Pharmacol. Sin. 2021, 42, 189–198. [Google Scholar] [CrossRef]
- van Reij, R.R.I.; Joosten, E.A.J.; van den Hoogen, N.J. Dopaminergic neurotransmission and genetic variation in chronification of post-surgical pain. Br. J. Anaesth. 2019, 123, 853–864. [Google Scholar] [CrossRef]
- Holman, A.J. Treatment of fibromyalgia: A changing of the guard. Womens Health 2005, 1, 409–420. [Google Scholar] [CrossRef] [Green Version]
- Okifuji, A.; Gao, J.; Bokat, C.; Hare, B.D. Management of fibromyalgia syndrome in 2016. Pain Manag. 2016, 6, 383–400. [Google Scholar] [CrossRef] [Green Version]
- Ross, J.W.; Ashford, A. The effect of reserpine and alpha-methyldopa on the analgesic action of morphine in the mouse. J. Pharm. Pharmacol. 1967, 19, 709–713. [Google Scholar] [CrossRef]
- Barber, B.A.; Kohl, K.L.; Kassam-Adams, N.; Gold, J.I. Acute stress, depression, and anxiety symptoms among English and Spanish speaking children with recent trauma exposure. J. Clin. Psychol. Med. Settings 2014, 21, 66–71. [Google Scholar] [CrossRef]
- Ottman, A.A.; Warner, C.B.; Brown, J.N. The role of mirtazapine in patients with fibromyalgia: A systematic review. Rheumatol. Int. 2018, 38, 2217–2224. [Google Scholar] [CrossRef]
- Arnold, L.M. Duloxetine and other antidepressants in the treatment of patients with fibromyalgia. Pain Med. 2007, 8 (Suppl. 2), S63–S74. [Google Scholar] [CrossRef]
- Kara, N.Z.; Stukalin, Y.; Einat, H. Revisiting the validity of the mouse forced swim test: Systematic review and meta-analysis of the effects of prototypic antidepressants. Neurosci. Biobehav Rev. 2018, 84, 1–11. [Google Scholar] [CrossRef]
- Commons, K.G.; Cholanians, A.B.; Babb, J.A.; Ehlinger, D.G. The Rodent Forced Swim Test Measures Stress-Coping Strategy, Not Depression-like Behavior. ACS Chem. Neurosci. 2017, 8, 955–960. [Google Scholar] [CrossRef] [Green Version]
- Cryan, J.; Markou, A.; Lucki, I. Assessing antidepressant activity in rodents: Recent developments and future needs. Trends Pharmacol. Sci. 2002, 23, 238–245. [Google Scholar] [CrossRef]
- Dhir, A.; Kulkarni, S.K. Involvement of dopamine (DA)/serotonin (5-HT)/sigma (sigma) receptor modulation in mediating the antidepressant action of ropinirole hydrochloride, a D2/D3 dopamine receptor agonist. Brain Res. Bull. 2007, 74, 58–65. [Google Scholar] [CrossRef]
- Mavrikaki, M.; Schintu, N.; Nomikos, G.G.; Panagis, G.; Svenningsson, P. Ropinirole regulates emotionality and neuronal activity markers in the limbic forebrain. Int. J. Neuropsychopharmacol. 2014, 17, 1981–1993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benes, H.; Mattern, W.; Peglau, I.; Dreykluft, T.; Bergmann, L.; Hansen, C.; Kohnen, R.; Banik, N.; Schoen, S.W.; Hornyak, M. Ropinirole improves depressive symptoms and restless legs syndrome severity in RLS patients: A multicentre, randomized, placebo-controlled study. J. Neurol. 2011, 258, 1046–1054. [Google Scholar] [CrossRef] [PubMed]
- Rénéric, J.P.; Lucki, I. Antidepressant behavioral effects by dual inhibition of monoamine reuptake in the rat forced swimming test. Psychopharmacology 1998, 136, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Ghorpade, S.; Tripathi, R.; Sonawane, D.; Manjrekar, N. Evaluation of antidepressant activity of ropinirole coadministered with fluoxetine in acute and chronic behavioral models of depression in rats. J. Basic Clin. Physiol. Pharmacol. 2011, 22, 109–114. [Google Scholar] [CrossRef]
- Bourin, M. Animal models for screening anxiolytic-like drugs: A perspective. Dialogues Clin. Neurosci. 2015, 17, 295–303. [Google Scholar] [CrossRef]
- Sowa-Kućma, M.; Pańczyszyn-Trzewik, P.; Misztak, P.; Jaeschke, R.R.; Sendek, K.; Styczeń, K.; Datka, W.; Koperny, M. Vortioxetine: A review of the pharmacology and clinical profile of the novel antidepressant. Pharmacol. Rep. 2017, 69, 595–601. [Google Scholar] [CrossRef] [PubMed]
- Christensen, M.C.; Loft, H.; Florea, I.; McIntyre, R.S. Efficacy of vortioxetine in working patients with generalized anxiety disorder. CNS Spectr. 2019, 24, 249–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pae, C.U.; Wang, S.M.; Han, C.; Lee, S.J.; Patkar, A.A.; Masand, P.S.; Serretti, A. Vortioxetine, a multimodal antidepressant for generalized anxiety disorder: A systematic review and meta-analysis. J. Psychiatr. Res. 2015, 64, 88–98. [Google Scholar] [CrossRef]
- Guilloux, J.P.; Mendez-David, I.; Pehrson, A.; Guiard, B.P.; Repérant, C.; Orvoën, S.; Gardier, A.M.; Hen, R.; Ebert, B.; Miller, S.; et al. Antidepressant and anxiolytic potential of the multimodal antidepressant vortioxetine (Lu AA21004) assessed by behavioural and neurogenesis outcomes in mice. Neuropharmacology 2013, 73, 147–159. [Google Scholar] [CrossRef] [Green Version]
- Available online: https://www.mayoclinic.org/drugs-supplements/ropinirole-oral-route/side-effects/drg-20066810?p=1 (accessed on 1 March 2021).
- Available online: https://parkinsonsnewstoday.com/forums/forums/topic/ropinirole-cause-of-shortness-of-breath-anxiety-like-symptoms-between-med-dose/ (accessed on 1 March 2021).
- Rogers, D.C.; Costall, B.; Domeney, A.M.; Gerrard, P.A.; Greener, M.; Kelly, M.E.; Hagan, J.J.; Hunter, A.J. Anxiolytic profile of ropinirole in the rat, mouse and common marmoset. Psychopharmacology 2000, 151, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Peciña, M.; Sikora, M.; Avery, E.T.; Heffernan, J.; Peciña, S.; Mickey, B.J.; Zubieta, J.K. Striatal dopamine D2/3 receptor-mediated neurotransmission in major depression: Implications for anhedonia, anxiety and treatment response. Eur. Neuropsychopharmacol. 2017, 27, 977–986. [Google Scholar] [CrossRef]
- Simon, P.; Panissaud, C.; Costentin, J. Anxiogenic-like effects induced by stimulation of dopamine receptors. Pharmacol. Biochem. Behav. 1993, 45, 685–690. [Google Scholar] [CrossRef]
- Jiang, L.X.; Huang, G.D.; Su, F.; Wang, H.; Zhang, C.; Yu, X. Vortioxetine administration attenuates cognitive and synaptic deficits in 5×FAD mice. Psychopharmacology 2020, 237, 1233–1243. [Google Scholar] [CrossRef] [PubMed]
- Witt, N.A.; Lee, B.; Ghent, K.; Zhang, W.Q.; Pehrson, A.L.; Sánchez, C.; Gould, G.G. Vortioxetine Reduces Marble Burying but Only Transiently Enhances Social Interaction Preference in Adult Male BTBR T+Itpr3tf/J Mice. ACS Chem. Neurosci. 2019, 10, 4319–4327. [Google Scholar] [CrossRef]
- Sałat, K.; Gawlik, K.; Witalis, J.; Pawlica-Gosiewska, D.; Filipek, B.; Solnica, B.; Więckowski, K.; Malawska, B. Evaluation of antinociceptive and antioxidant properties of 3-[4-(3-trifluoromethyl-phenyl)-piperazin-1-yl]-dihydrofuran-2-one in mice. Naunyn. Schmiedebergs Arch. Pharmacol. 2013, 386, 493–505. [Google Scholar] [CrossRef] [Green Version]
- Porsolt, R.D.; Bertin, A.; Jalfre, M. Behavioral despair in mice: A primary screening test for antidepressants. Arch. Int. Pharmacodyn. Ther. 1977, 229, 327–336. [Google Scholar]
- Sałat, K.; Siwek, A.; Starowicz, G.; Librowski, T.; Nowak, G.; Drabik, U.; Gajdosz, R.; Popik, P. Antidepressant-like effects of ketamine, norketamine and dehydronorketamine in forced swim test: Role of activity at NMDA receptor. Neuropharmacology 2015, 99, 301–307. [Google Scholar] [CrossRef]
- Bourin, M.; Masse, F.; Dailly, E.; Hascoët, M. Anxiolytic-like effect of milnacipran in the four-plate test in mice: Mechanism of action. Pharmacol. Biochem. Behav. 2005, 81, 645–656. [Google Scholar] [CrossRef]
- Montilla-García, Á.; Tejada, M.Á.; Perazzoli, G.; Entrena, J.M.; Portillo-Salido, E.; Fernández-Segura, E.; Cañizares, F.J.; Cobos, E.J. Grip strength in mice with joint inflammation: A rheumatology function test sensitive to pain and analgesia. Neuropharmacology 2017, 125, 231–242. [Google Scholar] [CrossRef]
- DeSantana, J.M.; da Cruz, K.M.; Sluka, K.A. Animal models of fibromyalgia. Arthritis Res. Ther. 2013, 15, 222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blasco-Serra, A.; Escrihuela-Vidal, F.; González-Soler, E.M.; Martínez-Expósito, F.; Blasco-Ausina, M.C.; Martínez-Bellver, S.; Cervera-Ferri, A.; Teruel-Martí, V.; Valverde-Navarro, A.A. Depressive-like symptoms in a reserpine-induced model of fibromyalgia in rats. Physiol. Behav. 2015, 151, 456–462. [Google Scholar] [CrossRef] [PubMed]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sałat, K.; Furgała-Wojas, A. Serotonergic Neurotransmission System Modulator, Vortioxetine, and Dopaminergic D2/D3 Receptor Agonist, Ropinirole, Attenuate Fibromyalgia-Like Symptoms in Mice. Molecules 2021, 26, 2398. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules26082398
Sałat K, Furgała-Wojas A. Serotonergic Neurotransmission System Modulator, Vortioxetine, and Dopaminergic D2/D3 Receptor Agonist, Ropinirole, Attenuate Fibromyalgia-Like Symptoms in Mice. Molecules. 2021; 26(8):2398. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules26082398
Chicago/Turabian StyleSałat, Kinga, and Anna Furgała-Wojas. 2021. "Serotonergic Neurotransmission System Modulator, Vortioxetine, and Dopaminergic D2/D3 Receptor Agonist, Ropinirole, Attenuate Fibromyalgia-Like Symptoms in Mice" Molecules 26, no. 8: 2398. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules26082398