Oxidative Stress in Complex Regional Pain Syndrome (CRPS): No Systemically Elevated Levels of Malondialdehyde, F2-Isoprostanes and 8OHdG in a Selected Sample of Patients

Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
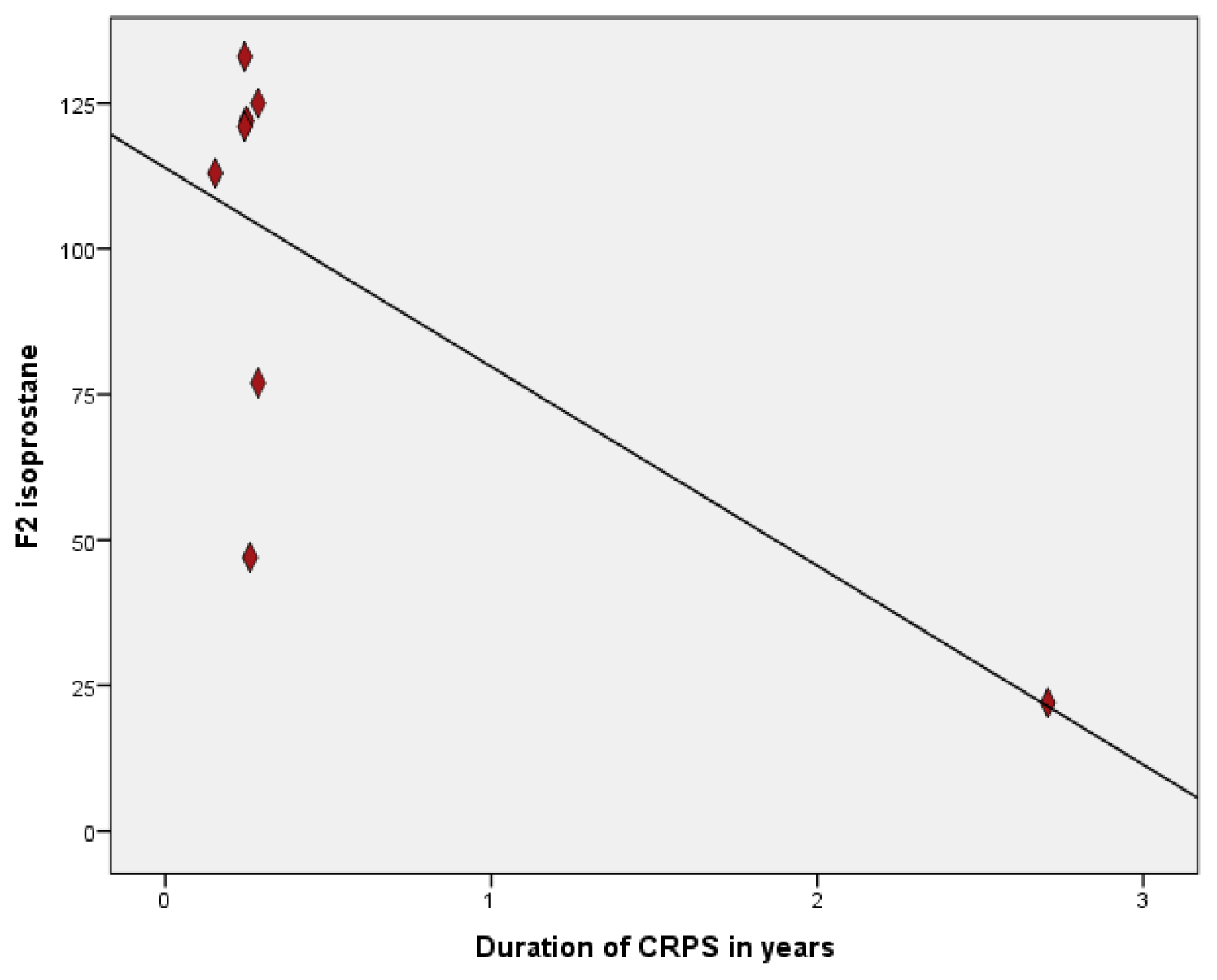
2.2. Oxidative Stress Markers
3. Discussion
4. Methods
4.1. Patients and Healthy Volunteers
4.2. Measurement of Plasma Malondialdehyde
4.3. Measurement F2-Isoprostanes in Plasma
4.4. Measurement F2-Isoprostanes in Urine
4.5. Measurement of 8-Hydroxy-2-Deoxyguanosine in Plasma
4.6. Measurement of 8-Hydroxy-2-Deoxyguanosine in Urine
4.7. Statistics
5. Conclusions
Acknowledgements
Conflict of Interest
References
- Bruehl, S.; Harden, R.N.; Galer, B.S.; Saltz, S.; Backonja, M.; Stanton-Hicks, M. Complex regional pain syndrome: Are there distinct subtypes and sequential stages of the syndrome? Pain 2002, 95, 119–124. [Google Scholar]
- Harden, R.N.; Bruehl, S.; Galer, B.S.; Saltz, S.; Bertram, M.; Backonja, M.; Gayles, R.; Rudin, N.; Bhugra, M.K.; Stanton-Hicks, M. Complex regional pain syndrome: Are the IASP diagnostic criteria valid and sufficiently comprehensive? Pain 1999, 83, 211–219. [Google Scholar]
- Alexander, G.M.; van Rijn, M.A.; van Hilten, J.J.; Perreault, M.J.; Schwartzman, R.J. Changes in cerebrospinal fluid levels of pro-inflammatory cytokines in CRPS. Pain 2005, 11, 213–219. [Google Scholar]
- Birklein, F.; Schmelz, M. Neuropeptides, neurogenic inflammation and complex regional pain syndrome (CRPS). Neurosci. Lett. 2008, 199–202. [Google Scholar]
- Eisenberg, E.; Shtahl, S.; Geller, R.; Reznick, A.Z.; Sharf, O.; Ravbinovich, M.; Erenreich, A.; Nagler, R.M. Serum and salivary oxidative analysis in complex regional pain syndrome. Pain 2008, 138, 226–232. [Google Scholar]
- Schinkel, C.; Scherens, A.; Koller, M.; Roellecke, G.; Muhr, G.; Maier, C. Systemic inflammatory mediators in post-traumatic complex regional pain syndrome (CRPS I)— Longitudinal investigations and differences to control groups. Eur. J. Med. Res 2009, 14, 130–135. [Google Scholar]
- Goris, R.J.; Dongen, L.M.; Winters, H.A. Are toxic oxygen radicals involved in the pathogenesis of reflex sympathetic dystrophy? Free Radic. Res. Commun 1987, 3, 13–18. [Google Scholar]
- Perez, R.S.; Zollinger, P.E.; Dijkstra, P.U.; Thomassen-Hilgersom, I.L.; Zuurmond, W.W.; Rosenbrand, K.C.; Geertzen, J.H. Evidence based guidelines for complex regional pain syndrome type 1. BMC Neurol. 2010, 10. [Google Scholar] [CrossRef]
- Zuurmond, W.W.; Langendijk, P.N.; Bezemer, P.D.; Brink, H.E.; de Lange, J.J.; van Loenen, A.C. Treatment of acute reflex sympathetic dystrophy with DMSO 50% in a fatty cream. Acta Anaesthesiol. Scand 1996, 40, 364–367. [Google Scholar]
- Zollinger, P.E.; Tuinebreijer, W.E.; Breederveld, R.S.; Kreis, R.W. Can vitamin C prevent complex regional pain syndrome in patients with wrist fractures? A randomized, controlled, multicenter dose-response study. J. Bone Joint Surg. Am 2007, 89, 1424–1431. [Google Scholar]
- Montuschi, P.; Barnes, P.J.; Roberts, L.J. Isoprostanes: Markers and mediators of oxidative stress. FASEB J 2004, 18, 1791–1800. [Google Scholar]
- Carlstrom, M.; Persson, A.E.; Larsson, E.; Hezel, M.; Scheffer, P.G.; Teerlink, T.; Weitzberg, E.; Lundberg, J.O. Dietary nitrate attenuates oxidative stress, prevents cardiac and renal injuries, and reduces blood pressure in salt-induced hypertension. Cardiovasc. Res 2011, 89, 574–585. [Google Scholar]
- Del, R.D.; Stewart, A.J.; Pellegrini, N. A review of recent studies on malondialdehyde as toxic molecule and biological marker of oxidative stress. Nutr. Metab. Cardiovasc. Dis 2005, 15, 316–328. [Google Scholar]
- Liu, W.; Morrow, J.D.; Yin, H. Quantification of F2-isoprostanes as a reliable index of oxidative stress in vivo using gas chromatography-mass spectrometry (GC-MS) method. Free Radic. Biol. Med 2009, 47, 1101–1107. [Google Scholar]
- Morrow, J.D. Quantification of isoprostanes as indices of oxidant stress and the risk of atherosclerosis in humans. Arterioscler. Thromb. Vasc. Biol 2005, 25, 279–286. [Google Scholar]
- Pratico, D.; Rokach, J.; Lawson, J.; FitzGerald, G.A. F2-isoprostanes as indices of lipid peroxidation in inflammatory diseases. Chem. Phys. Lipids 2004, 128, 165–171. [Google Scholar]
- Sauvain, J.J.; Setyan, A.; Wild, P.; Tacchini, P.; Lagger, G.; Storti, F.; Deslarzes, S.; Guillemin, M.; Rossi, M.J.; Riediker, M. Biomarkers of oxidative stress and its association with the urinary reducing capacity in bus maintenance workers. J. Occup. Med. Toxicol. 2011, 6. [Google Scholar] [CrossRef]
- Tasset, I.; Aguera, E.; Sanchez-Lopez, F.; Feijoo, M.; Giraldo, A.I.; Cruz, A.H.; Gascon, F.; Tunez, I. Peripheral oxidative stress in relapsing-remitting multiple sclerosis. Clin. Biochem 2012, 45, 440–444. [Google Scholar]
- Perez, R.S.; Zuurmond, W.W.; Bezemer, P.D.; Kuik, D.J.; van Loenen, A.C.; de Lange, J.J.; Zuidhof, A.J. The treatment of complex regional pain syndrome type I with free radical scavengers: A randomized controlled study. Pain 2003, 10, 297–307. [Google Scholar]
- Birklein, F. Diagnostik und therapie komplexer regionaler schmerzsyndrome (CRPS). Leitlin. Diagn. Ther. Neurol 2008, 4, 640–652. [Google Scholar]
- Mos, M.; de Bruijn, A.G.; Huygen, F.J.; Dieleman, J.P.; Stricker, B.H.; Sturkenboom, M.C. The incidence of complex regional pain syndrome: A population-based study. Pain 2007, 129, 12–20. [Google Scholar]
- Schinkel, C.; Gaertner, A.; Zaspel, J.; Zedler, S.; Faist, E.; Schuermann, M. Inflammatory mediators are altered in the acute phase of posttraumatic complex regional pain syndrome. Clin. J. Pain 2006, 22, 235–239. [Google Scholar]
- Coderre, T.J.; Bennett, G.J. A hypothesis for the cause of complex regional pain syndrome-type I (reflex sympathetic dystrophy): Pain due to deep-tissue microvascular pathology. Pain Med 2010, 11, 1224–1238. [Google Scholar]
- Heijmans-Antonissen, C.; Wesseldijk, F.; Munnikes, R.J.; Huygen, F.J.; van der Meijden, P.; Hop, W.C.; Hooijkaas, H.; Zijlstra, F.J. Multiplex bead array assay for detection of 25 soluble cytokines in blister fluid of patients with complex regional pain syndrome type 1. Mediators Inflamm 2006, 2006, 283–298. [Google Scholar]
- Huygen, F.J.; De Bruijn, A.G.; De Bruin, M.T.; Groeneweg, J.G.; Klein, J.; Zijlstra, F.J. Evidence for local inflammation in complex regional pain syndrome type 1. Mediators Inflamm 2002, 11, 47–51. [Google Scholar]
- Huygen, F.J.; Ramdhani, N.; van Toorenenbergen, A.; Klein, J.; Zijlstra, F.J. Mast cells are involved in inflammatory reactions during complex regional pain syndrome type 1. Immunol. Lett 2004, 91, 147–154. [Google Scholar]
- Heerschap, A.; den Hollander, J.A.; Reynen, H.; Goris, R.J. Metabolic changes in reflex sympathetic dystrophy: A 31P NMR spectroscopy study. Muscle Nerve 1993, 16, 367–373. [Google Scholar]
- Birklein, F.; Weber, M.; Neundorfer, B. Increased skin lactate in complex regional pain syndrome: Evidence for tissue hypoxia? Neurology 2000, 55, 1213–1215. [Google Scholar]
- Beek, W.J.; Remarque, E.J.; Westendorp, R.G.; van Hilten, J.J. Innate cytokine profile in patients with complex regional pain syndrome is normal. Pain 2001, 91, 259–261. [Google Scholar]
- Proudfoot, J.; Barden, A.; Mori, T.A.; Burke, V.; Croft, K.D.; Beilin, L.J.; Puddey, I.B. Measurement of urinary F(2)-isoprostanes as markers of in vivo lipid peroxidation-A comparison of enzyme immunoassay with gas chromatography/mass spectrometry. Anal. Biochem 1999, 272, 209–215. [Google Scholar]
- Wesseldijk, F.; Huygen, F.J.; Heijmans-Antonissen, C.; Niehof, S.P.; Zijlstra, F.J. Tumor necrosis factor-alpha and interleukin-6 are not correlated with the characteristics of complex regional pain syndrome type 1 in 66 patients. Eur. J. Pain 2007, 12, 716–721. [Google Scholar]
- van de Kerkhof, J.; Schalkwijk, C.G.; Konings, C.J.; Cheriex, E.C.; van der Sande, F.M.; Scheffer, P.G.; ter Wee, P.M.; Leunissen, K.M.; Kooman, J.P. Nepsilon-(carboxymethyl)lysine, Nepsilon-(carboxyethyl)lysine and vascular cell adhesion molecule-1 (VCAM-1) in relation to peritoneal glucose prescription and residual renal function; a study in peritoneal dialysis patients. Nephrol. Dial. Transplant 2004, 19, 910–916. [Google Scholar]
- Roest, M.; Voorbij, H.A.; van der Schouw, Y.T.; Peeters, P.H.; Teerlink, T.; Scheffer, P.G. High levels of urinary F2-isoprostanes predict cardiovascular mortality in postmenopausal women. J. Clin. Lipidol 2008, 2, 298–303. [Google Scholar]
- Nguy, L.; Nilsson, H.; Lundgren, J.; Johansson, M.E.; Teerlink, T.; Scheffer, P.G.; Guron, G. Vascular function in rats with adenine-induced chronic renal failure. Am. J. Physiol. Regul. Integr. Comp. Physiol 2012, 302, R1426–R1435. [Google Scholar]


{kind=link}
| CRPS-1 patients | Healthy volunteers | p-value | ||
|---|---|---|---|---|
| n = 9 | n = 9 | |||
| Age * | 50.1 (17.0) | 49.3 (16.8) | 0.92 | |
| Duration CRPS (months) ** | 3.0 (2.0–3.5) | - | - | |
| Affected extremity | - | - | - | |
| upper/lower | 5/4 | |||
| Temperature affected extremity (warm/cold/no difference) | 4/3/2 | - | - | |
| Swelling (yes/no) | 4/5 | - | - | |
| Reduced range of motion (yes/no) | 9/0 | - | - | |
| Pain score * | Pain yes/no mean over 1 week during movement | 9/0 5.3 (2.3) 6.2 (3.3) | - | - |
| Impairment levels sum score * (ISS) | 26.1 (11.1) | - | - | |
| CRPS Severity Score * (CSS) | 10.3 (2.6) | - | - | |
| Plasma | - | - | - | |
| MDA* (μmol/L) | 5.2 (0.9) | 5.4 (0.5) | 0.66 | |
| F2 isoprostanes * (pg/mL) | 83.9 (18.7) | 80.5 (12.3) | 0.65 | |
| 8OhdG * (pmol/L) | 92.6 (25.5) | 86.9 (19.0) | 0.60 | |
| Urine | n = 8 | n = 9 | - | |
| F2 isoprostanes ** (ng/mmol) | 117 (54.5–124.3) | 85.0 (55.5–110.0) | 0.61 | |
| 8OHdG* (nmol/mmol) | 1.4 (0.7) | 1.4 (0.5) | 0.85 | |
© 2013 by the authors; licensee MDPI, Basel, Switzerland This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Fischer, S.G.L.; Perez, R.S.G.M.; Nouta, J.; Zuurmond, W.W.A.; Scheffer, P.G. Oxidative Stress in Complex Regional Pain Syndrome (CRPS): No Systemically Elevated Levels of Malondialdehyde, F2-Isoprostanes and 8OHdG in a Selected Sample of Patients. Int. J. Mol. Sci. 2013, 14, 7784-7794. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms14047784
Fischer SGL, Perez RSGM, Nouta J, Zuurmond WWA, Scheffer PG. Oxidative Stress in Complex Regional Pain Syndrome (CRPS): No Systemically Elevated Levels of Malondialdehyde, F2-Isoprostanes and 8OHdG in a Selected Sample of Patients. International Journal of Molecular Sciences. 2013; 14(4):7784-7794. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms14047784
Chicago/Turabian StyleFischer, Sigrid G. L., Roberto S. G. M. Perez, Jan Nouta, Wouter W. A. Zuurmond, and Peter G. Scheffer. 2013. "Oxidative Stress in Complex Regional Pain Syndrome (CRPS): No Systemically Elevated Levels of Malondialdehyde, F2-Isoprostanes and 8OHdG in a Selected Sample of Patients" International Journal of Molecular Sciences 14, no. 4: 7784-7794. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms14047784