1. Introduction
Schizophrenia is one of the most severe mental disorders, which affects around 1% of the population [
1]. In periods of acute psychosis, therapeutic strategies focus on managing delusions, hallucinations, and formal thought and behavior disorders. In a stable state, the main therapeutic challenge is reduction of severity of negative (autistic behavior, flat affect, reduced social activities), affective (depressed mood, anxiety), and cognitive symptoms (attention deficits, impairment of working memory, and other executive functions). Dorsolateral prefrontal cortex (DLPFC) and hippocampus are specific brain regions essential for cognition and emotions [
2,
3,
4,
5]. Dysfunction of these regions is associated with presence of negative and cognitive symptoms. White matter (WM) within the frontal lobe consists of axons of cells that make up for the cortex, neurites projecting to the prefrontal cortex, and fibers connecting the DLPFC with the hippocampus [
6].
Therapy with antidepressants (AD) is one of the most widely used methods for augmentation of antipsychotic treatment (AP). It aims to alleviate affective, negative, and to a lesser extent cognitive symptoms [
7]. One meta-analysis demonstrated that significant efficacy of AD is observed particularly in patients with chronic phase of the disease [
8], whereas conclusions of other studies are ambiguous [
9,
10]. Although it was believed that AD treatment may increase the risk of psychotic exacerbation, new data confirms that AD do not cause such complications [
11].
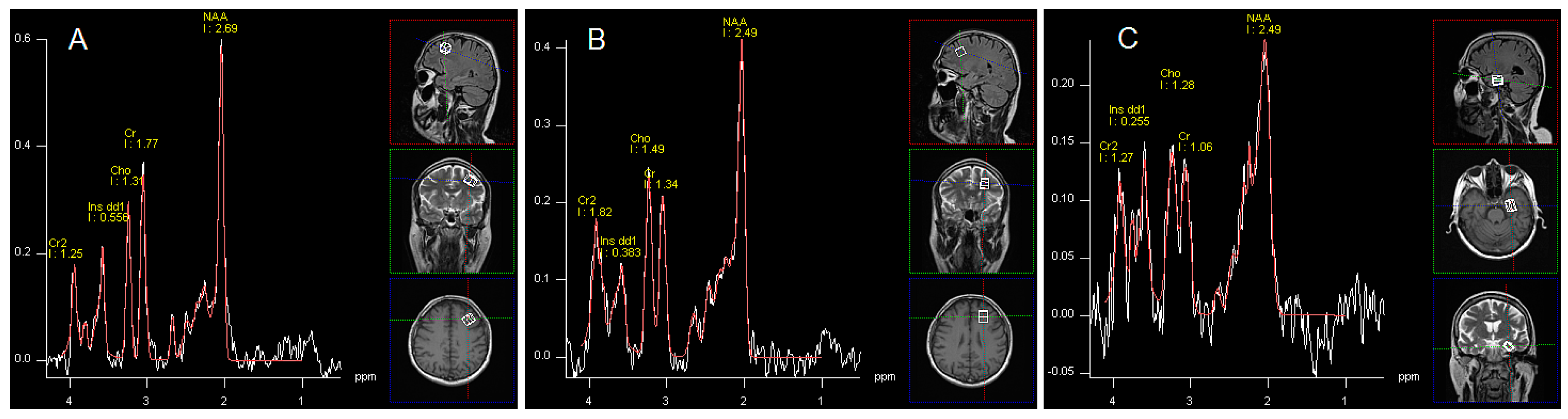
Proton magnetic resonance spectroscopy enables
in vivo assessment of brain metabolic parameters, including changes associated with drug administration. However,
1H-NMR studies in schizophrenia did not allow drawing definite conclusions about changes in metabolic parameters depending on the examined area of the brain, particular symptoms, and phase of the disease or treatment strategy. Most studies in schizophrenia showed a decrease in the concentrations of
N-acetylaspartate (NAA) in gray matter, which is a ubiquitous brain metabolite, considered a reliable marker of viability and integrity of the brain tissue [
12]. According to Brugger, Steen, and Kraguljac NAA concentration in the frontal cortex was similar in patients with the first episode of schizophrenia and individuals in a chronic phase of the disease [
13,
14,
15]. Moreover it also did not depend on the duration of untreated psychosis (DUP) [
16]. Concentrations of NAA and glutamatergic parameters may correlate with severity of the negative and cognitive symptoms [
17,
18,
19,
20,
21,
22,
23,
24]. There was a negative correlation between symptom severity and NAA concentrations in the prefrontal cortex, thalamus, and in the anterior cingulate [
25,
26,
27,
28]. Most studies, however, failed to demonstrate the relationship between concentrations of metabolites and exacerbation of clinical symptoms [
29,
30,
31,
32,
33,
34,
35] or differences in NAA and Glu levels between patients with schizophrenia and healthy controls [
36].
Findings in unmedicated patients with schizophrenia are also ambiguous. Kraguljac
et al. found increased hippocampal Glx/Cr in treatment-naive patients but no alterations in NAA/Cr [
37]. In study of Kegeles
et al. elevated Glx levels in the medial prefrontal cortex were found [
21]. Similar findings in dorsal caudate are also available [
38]. Wood
et al. noted no differences in NAA or Glx levels among similar patients when compared with healthy controls [
39], while Tibbo
et al. found no differences in glutamate levels between first-episode patients and a control group in the prefrontal region [
40].
As far as the effect of medications is concerned, it was proved that AP affect concentrations of brain metabolites [
33,
41,
42,
43]. However, due to increasing number of patients with schizophrenia receiving AD (from 15% of patients in the 1990s to 40% in the last decade [
44]) there is a need for evaluation of their influence. Effects of AD were already demonstrated in patients with major depressive disorder (MDD), who presented increased NAA/Cr ratios values in the left medial prefrontal cortex after successful treatment with selective serotonin transporter inhibitors (SSRIs) or serotonin and norepinephrine inhibitors (SNRI) compared to the pre-treatment values [
45]. Moreover, in patients with major depression Block
et al. described an association between treatment response to SSRI and tricyclic antidepressants and increase in NAA and Cho concentrations in the hippocampus, irrespective of the disease severity. Furthermore, it was revealed that low baseline NAA and Cho levels were predictors of the positive effects of the treatment [
46].
We aim to compare 1H-NMR spectroscopic parameters (NAA, Glx, mI, Cho and Cr) in these regions of the dominant hemisphere that are crucial for pathogenesis of schizophrenia: the left DLPFC, WM of the left frontal lobe and in the left hippocampus between two groups of right-handed patients in the chronic phase of the illness with and without AD therapy. We hypothesize that there are differences in brain metabolic parameters between the two groups—with and without AD.
2. Results
There were no significant differences in patients’ clinical status and the results of PANSS (total score and subscales) and CDSS scales between both groups (
Table 1 and
Table 2). The only significant difference among the main analyzed parameters was the lower mean dose of AP administered in a group treated with AP+AD in comparison to patients receiving only AP. Antidepressive treatment is described in
Table 3.
Table 1.
Characteristics of groups.
Table 1.
Characteristics of groups.
| Features | AP+AD Group | AP Group | p Value |
|---|
| (n = 25) | (n = 25) |
|---|
| Gender | Female | 10 | Female | 0.5449 |
| Male | 15 | Male |
| Age (years) | 35.00 | 39.79 | 0.151 |
| Mean number of hospitalizations | 4 | 5 | 0.24 |
| Mean duration of the illness (years) | 12.1 | 13.7 | 0.1495 |
| Mean timespan of education per patient (years) | 14.7 | 13.8 | 0.5449 |
| Antipsychotic treatment (DDD) | 1.57 | 2.22 | 0.0195 |
| Current smokers | 11 | 9 | 0.5635 |
Table 2.
Results of Positive and Negative Syndrome Scale (PANSS) and Calgary scales in each group.
Table 2.
Results of Positive and Negative Syndrome Scale (PANSS) and Calgary scales in each group.
| Scales | AP+AD Group | AP Group | p Value |
|---|
| Mean | SD | Mean | SD |
|---|
| PANSS P | 9.6 | 3.0 | 10.7 | 3.0 | 0.091635 |
| PANSS N | 25.0 | 4.6 | 26.4 | 5.3 | 0.462515 |
| PANSS G | 35.1 | 7.8 | 34.8 | 7.8 | 0.970098 |
| PANSS Total | 69.6 | 13.1 | 71.9 | 13.2 | 0.333484 |
| Calgary | 3.4 | 3.0 | 3.8 | 2.8 | 0.553671 |
Table 3.
Description of antidepressive therapy.
Table 3.
Description of antidepressive therapy.
| Type of Medication | Number of Patients | Mean Dose (mg) | Range (mg) |
|---|
| Sertraline | 11 | 84.1 | 25–200 |
| Citalopram | 7 | 25.7 | 10–60 |
| Fluvoxamine | 2 | 75 | 50–100 |
| Venlafaxine | 2 | 225 | 225 |
| Fluoxetine | 2 | 15 | 10–20 |
| Clomipramine | 1 | 150 | 150 |
| Escitalopram | 1 | 10 | 10 |
Comparisons of spectroscopic data between both groups are presented in
Table 4 (left DLPFC),
Table 5 (left frontal WM), and
Table 6 (left hippocampus).
Table 4.
Comparison of substance concentration ratios in left DLPFC.
Table 4.
Comparison of substance concentration ratios in left DLPFC.
| Parameter | AP+AD Group | AP Group | p Value |
|---|
| Mean | SD | Mean | SD |
|---|
| NAA/Cr | 1.91 | 0.31 | 1.55 | 0.66 | 0.03651 |
| Cho/Cr | 0.68 | 0.24 | 0.76 | 0.35 | ns |
| mI/Cr | 0.26 | 0.11 | 0.28 | 0.13 | ns |
| Glx/Cr | 1.46 | 0.52 | 0.83 | 0.40 | ns |
| NAA/Cho | 2.19 | 0.61 | 1.48 | 0.72 | 0.01114 |
| mI/Cho | 0.38 | 0.15 | 0.48 | 0.57 | ns |
| Glx/Cho | 1.12 | 0.11 | 0.80 | 0.47 | ns |
In group AP+AD both NAA/Cr and NAA/Cho ratios (by 23.2% and 48%, respectively) were significantly higher (p < 0.05).
Table 5.
Comparison of substance concentration ratios in left frontal WM.
Table 5.
Comparison of substance concentration ratios in left frontal WM.
| Parameter | AP+AD Group | AP Group | p Value |
|---|
| Mean | SD | Mean | SD |
|---|
| NAA/Cr | 1.79 | 2.16 | 1.62 | 0.96 | ns |
| Cho/Cr | 1.24 | 1.06 | 1.01 | 0.53 | ns |
| mI/Cr | 0.42 | 0.27 | 0.26 | 0.19 | 0.04291 |
| Glx/Cr | 0.83 | 0.26 | 0.69 | 0.27 | ns |
| NAA/Cho | 2.42 | 0.89 | 2.17 | 0.60 | ns |
| mI/Cho | 0.34 | 0.24 | 0.26 | 0.24 | ns |
| Glx/Cho | 0.73 | 0.25 | 0.81 | 0.24 | ns |
A typical glial parameter (mI/Cr) was significantly higher (by 61.5%) in the WM in AP+AD group.
Table 6.
Comparison of substance concentration ratios in left hippocampus.
Table 6.
Comparison of substance concentration ratios in left hippocampus.
| Parameter | AP+AD Group | AP Group | p Value |
|---|
| Mean | SD | Mean | SD |
|---|
| NAA/Cr | 3.21 | 2.31 | 2.66 | 2.17 | ns |
| Cho/Cr | 0.97 | 0.72 | 1.45 | 0.88 | ns |
| mI/Cr | 0.74 | 0.72 | 0.62 | 0.85 | ns |
| Glx/Cr | 0.99 | 0.37 | 1.42 | 0.63 | 0.04232 |
| NAA/Cho | 3.48 | 4.10 | 1.70 | 0.94 | ns |
| mI/Cho | 2.46 | 5.48 | 0.44 | 0.68 | ns |
| Glx/Cho | 1.00 | 0.39 | 1.84 | 0.69 | 0.01703 |
In the left hippocampus both parameters associated with the glutamatergic transmission were significantly lower in the group treated with AP+AD than in patients receiving only AP (by 30.3% in Glx/Cr and by 45.6% in Glx/Cho ratio).
Age and smoking status may also influence metabolite concentrations [
47,
48,
49]. Thus, both factors, together with group affiliation, were defined as independent variables in multiple stepwise regression analysis. In this analysis technique only independent variables that influence a dependent variable are included into the model. In
Table 7 there are presented variables that were included in the model for each metabolite concentration ratio in particular brain regions. For brain metabolites not presented in the table the regression analysis did not include any variable into the model.
Table 7.
Multiple stepwise regression analysis of the determinants of substance concentration ratios in left DLPFC, frontal WM and hippocampus.
Table 7.
Multiple stepwise regression analysis of the determinants of substance concentration ratios in left DLPFC, frontal WM and hippocampus.
| Brain Region | Concentration Ratio | Predictor | β-Coefficient (±SD) | Corrected R2 of the Model | p Value |
|---|
| DLPFC | NAA/Cr | AD | 0.3650 (0.2135) | 0.05354 | 0.0967 |
| Cho/Cr | Age | 0.0089 (0.0052) | 0.05587 | 0.0950 |
| Smoking | −0.1189 (0.1050) | 0.2661 |
| Glx/Cr | AD | 0.6290 (0.3549) | 0.26304 | 0.1365 |
| NAA/Cho | AD | 0.7744 (0.3095) | 0.1696 | 0.0177 * |
| Age | −0.0204 (0.0142) | 0.1595 |
| Glx/Cho | Age | 0.0229 (0.0170) | 0.1207 | 0.2347 |
| White Matter | NAA/Cr | AD | 0.5053 (0.1645) | 0.2966 | 0.0063 * |
| mI/Cr | AD | 0.1506 (0.0796) | 0.0705 | 0.0674 |
| Glx/Cr | AD | 0.1282 (0.1235) | 0.0396 | 0.3129 |
| Age | 0.0056 (0.0051) | 0.2795 |
| Smoking | 0.1756 (0.1311) | 0.1972 |
| NAA/Cho | AD | 0.33926 (0.2874) | 0.0479 | 0.2463 |
| smoking | −0.43080 (0.2765) | 0.1288 |
| mI/Cho | AD | 0.1002 (0.0795) | 0.02825 | 0.2156 |
| Smoking | −0.0949 (0.0758) | 0.2192 |
| Hippocampus | Cho/Cr | AD | −0.6074 (0.3218) | 0.0960 | 0.0718 |
| Smoking | −0.3529 (0.3169) | 0.2769 |
| Glx/Cr | Age | −0.0219 (0.0103) | 0.1666 | 0.0478 * |
| Smoking | 0.3640 (0.2354) | 0.1394 |
| NAA/Cho | AD | 8.7339 (4.8314) | 0.0980 | 0.0822 |
| Age | 0.2934 (0.2223) | 0.1985 |
| mI/Cho | AD | 2.492 (1.3188) | 0.1604 | 0.0709 |
| Age | 0.1294 (0.0633) | 0.0519 |
| Glx/Cho | AD | 0.8307 (0.2958) | 0.3646 | 0.0170 * |
3. Discussion
This is the first study comparing spectroscopic parameters in two groups of patients with schizophrenia differing by the addition of AD to AP treatment. In discussion, we will focus on relevant results depending on the region where these changes were observed.
3.1. NAA and DLPFC
N-Acetylaspartate is one of the most common amino acids in the human brain. The role of the NAA in the brain is uncertain, but it is probably engaged in the metabolism of other amino acids (glutamate) and fluid balance [
12]. It is specifically synthesized and present in high concentrations in neuronal mitochondria, but not in glia. Moreover, its level is closely associated with neuronal glucose metabolism [
50]. Thus, NAA is considered as a marker of neuronal viability and integrity [
12]. A higher NAA/Cr and NAA/Cho ratio observed in DLPFC in the AP+AD patients suggests that overall neuronal activity in this area was increased when compared to the AP group. As we previously mentioned, the role of the decreased activity of DLPFC in development of negative and cognitive symptoms is well established [
51,
52]. We suspect possible positive influence of AD on DLPFC metabolism and clinical improvement in context of our findings, even if efficacy of AD in treating negative and cognitive symptoms is still uncertain [
11,
53]. Methodological characteristics of our study (one time point assessment) does not allow provision of an unambiguous answer, whether AD improved mentioned symptoms. An increase of NAA concentration can be an effect of the antipsychotic drugs [
33]. A definitive conclusion should be formulated carefully in this case, but the absence of other statistically significant variables indicates that the use of lower doses of AP may be associated with the use of AD.
In regression analysis we confirmed that administration of AD has the biggest influence on changes in NAA/Cr and NAA/Cho ratios. Although, age was included to the model for NAA/Cho it had small β-coefficient (−0.0204).
3.2. Glx and Hippocampus
It is postulated that in schizophrenia, glutamatergic system hyperactivity results from an impaired control of GABAergic interneurons and disturbed interactions with dopaminergic system [
54].
A decrease in Glx/Cho and Glx/Cr ratios in the experimental group may indicate a positive effect of AD in the management of schizophrenia, because an increase of glutamatergic transmission parameters in hippocampal formation was previously observed in schizophrenia [
18,
37,
55,
56]. It was speculated that a psychotic process originates from the impaired glutamatergic transmission within the dentate gyrus in the hippocampus complex, which in consequence, leads to the hyperglutamatergic state within the CA1, CA3 fields and the subiculum of the hippocampus [
57,
58]. Functional changes in CA3 neurons may cause increased neuronal excitation, inadequate plasticity changes, such as disturbances of a long-term potentiation process (LTP) in aforementioned subfield [
57,
59].
Having the source in the dysfunctional inhibitory processes, which in schizophrenia results from hypofunction of NMDA receptors on GABAergic interneurons [
60], an increased glutamatergic stimulation in the hippocampus is considered one of the key causes of attention deficit and cognitive dysfunction [
57]. Cognitive function decline (assessed with the Wisconsin Card Sorting Test) was correlated with increased glutamate concentrations in the hippocampus in patients with schizophrenia, but not in healthy controls [
60].
Insufficient control of the excitatory glutamatergic system may be also responsible for the development of hallucinations, delusions, and formal thought disorders typical for the acute psychotic states [
54]. These inhibitory control dysfunctions may be expressed in gamma rhythms (25–100 Hz) changes [
61,
62], coherent neuronal oscillation disturbances (rate below 0.1 Hz) [
63] which both might resemble increased information redundancy.
Our results indicate that in AP+AD group pathological hyperactivity within the hippocampus is reduced. It is the first evidence that unfavourable increase of the glutamate concentration within the hippocampus in schizophrenia is slighter in AP+AD group than in AP group.
According to the regression analysis, AD administration had significant effect only on Glx/Cho ratio, but not on Glx/Cr, which was more dependent on age and smoking status. On the other hand, the model for Glx/Cr explained only 16.7% of its variation and 36.5% for Glx/Cho. Thus, AD seems to have significant influence on hippocampus metabolism.
3.3. mI and WM
Myo-inositol—a precursor in the phosphatidylinositol signalling system is also a widely accepted glial marker in spectroscopic studies [
64]. Generally, in neurodegenerative processes, increased mI levels have been found to co-occur with reduced NAA [
65]. In these cases increased mI concentration is probably associated with neuroinflammation, neuronal damage, and glial proliferation [
46]. Interestingly, current and previous depressive episodes in patients with schizophrenia or schizoaffective disorder may be related to higher levels of mI comparing to patient with schizophrenia without depressive episode [
66]. In this study, the duration of the disease and its severity were comparable between both groups. Thus, it can be assumed that there were no significant differences in the intensity of glial proliferation due to the illness and that the observed differences were probably related to the treatment.
We suspect that increased mI/Cr ratio in the group treated with antidepressants may indicate higher activity of glial cells, associated with overall improvement of the brain metabolism, observed in other brain area or mI tendency to increase in patients with affective features having AD treatment as in study of Chiapelli
et al. [
66]. Although AD were included in the model for mI/Cr ratio this variable was not significant (0.0674). Surprisingly, AD were significant determinants of NAA/Cr ratio explaining almost 30% of its variance. This influence might be missed in initial comparison due to masking effect of age and/or smoking status.
3.4. Doses of AP
Difference in the mean doses of the antipsychotic drug, significantly lower in AP+AD patients, requires a commentary. Our data is insufficient to draw convincing conclusions, but this may indicate that to achieve similar parameters of the mental state using AD and AP, reduced doses of AP are needed.


 ,
, 
{kind=link}
