2.2. Comparison of the Number or Fraction of Distinct Immune Cells in Patients with AIS/TIA, CCD, and HV
The numbers or fractions of immune cell subsets in patients with AIS/TIA and CCD and in HV are shown in
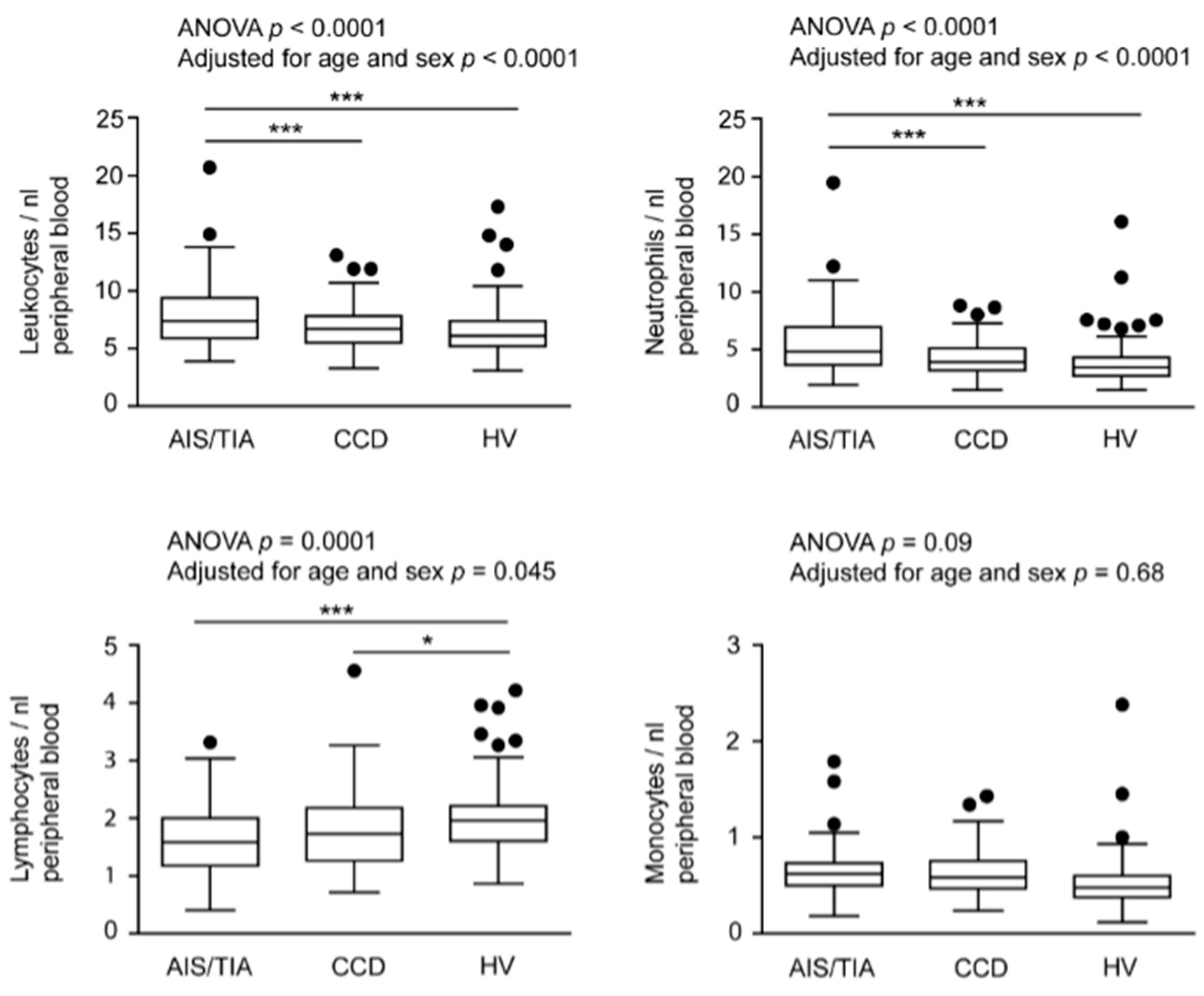
Figure 1 for comparison. For the primary analyses of data (without adjustment for confounders, but also adjusted for age and sex), we found significantly higher numbers of leukocytes and neutrophils in patients with AIS/TIA (leukocytes, 7.9 ± 2.7/nL; neutrophils, 5.4 ± 2.6/nL) compared with patients with CCD (leukocytes, 6.8 ± 1.8/nL,
p < 0.001; neutrophils, 4.2 ± 1.4/nL,
p < 0.001) and HV (leukocytes, 6.5 ± 2.2/nL,
p < 0.001; neutrophils, 3.8 ± 1.9/nL,
p < 0.001). In contrast, lymphocytes were higher in HV (2.0 ± 0.6/nL) compared with patients with CCD 1.8 ± 0.6/nL,
p < 0.05) and those with AIS/TIA (1.6 ± 0.6/nL,
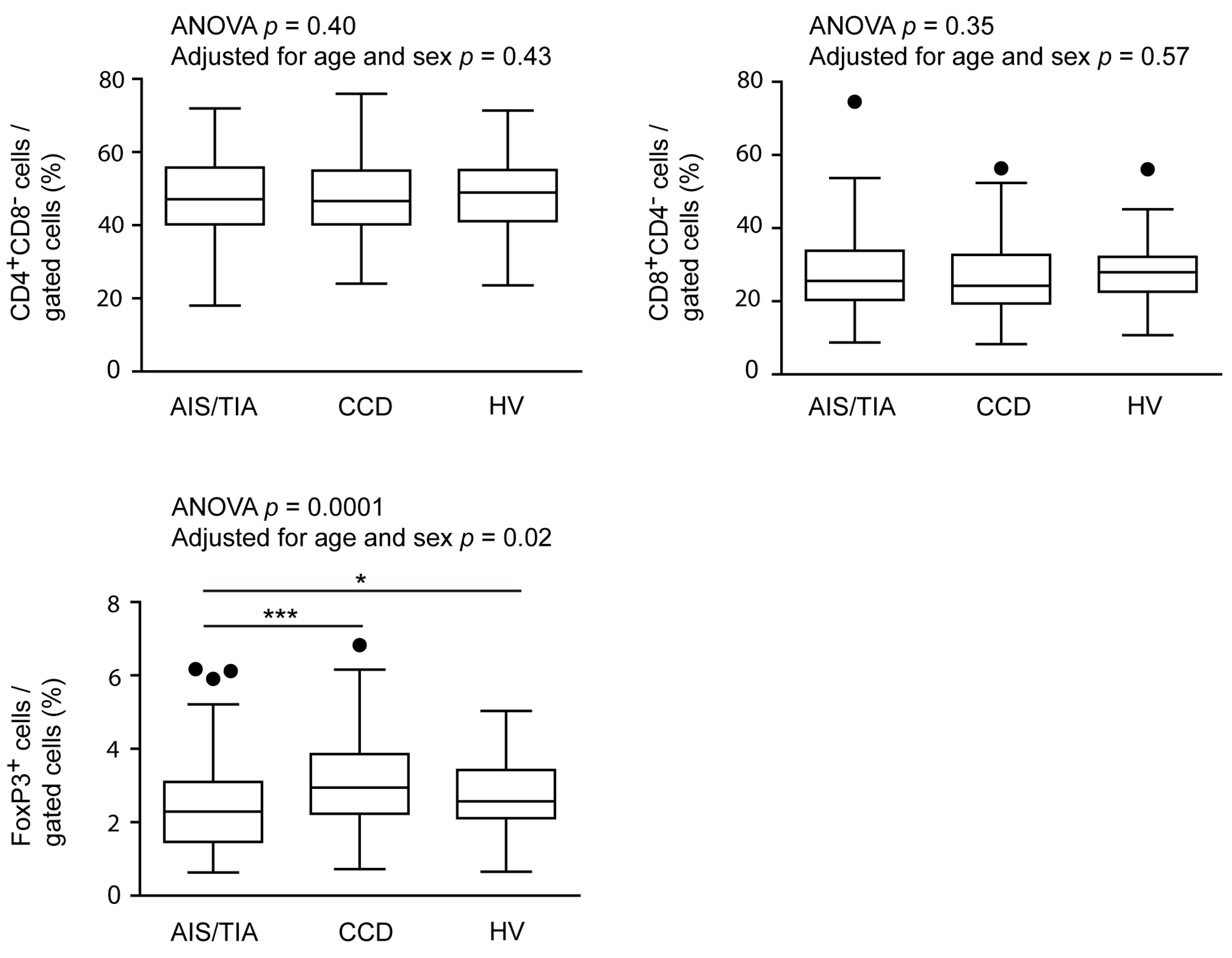
p < 0.001). Also FoxP3
+ regulatory T cells (T
reg), a subset of lymphocytes, were decreased in patients with AIS/TIA (2.4% ± 1.2%) compared with patients with CCD (3.1% ± 1.2%,
p < 0.001) and HV (2.8% ± 1.0%,
p < 0.05). There was no difference in the number of monocytes as well as the fraction of CD4
+CD8
− or CD8
+CD4
− T cells between the groups.
Figure 1.
Numbers or fractions of important immune cell subsets in acute ischemic stroke (AIS)/transitory ischemic attack (TIA), chronic cerebrovascular disease (CCD), and healthy volunteers (HV). The number of leukocytes, neutrophils, lymphocytes, monocytes, CD4+CD8−, CD8+CD4−, and FoxP3 regulatory T cells (Treg) are depicted in box-and-whisker plots indicating the first and third quartiles as well as the 1.5 interquartile range (IQR, Tukey plot). Outliers that lie outside the 1.5 IQR are represented by single dots. The numbers of leukocytes, neutrophils, lymphocytes and FoxP3+ Treg differed significantly between the three groups, as determined by analysis of variance with Bonferroni post hoc test, *** p < 0.001, * p < 0.05.
Figure 1.
Numbers or fractions of important immune cell subsets in acute ischemic stroke (AIS)/transitory ischemic attack (TIA), chronic cerebrovascular disease (CCD), and healthy volunteers (HV). The number of leukocytes, neutrophils, lymphocytes, monocytes, CD4+CD8−, CD8+CD4−, and FoxP3 regulatory T cells (Treg) are depicted in box-and-whisker plots indicating the first and third quartiles as well as the 1.5 interquartile range (IQR, Tukey plot). Outliers that lie outside the 1.5 IQR are represented by single dots. The numbers of leukocytes, neutrophils, lymphocytes and FoxP3+ Treg differed significantly between the three groups, as determined by analysis of variance with Bonferroni post hoc test, *** p < 0.001, * p < 0.05.
2.3. Relationship between the Number or Fraction of Immune Cell Subsets and Key Demographic and Clinical Parameters in Patients with Acute Cerebrovascular Disease
Results from univariate analysis of the association between the number or fraction of immune cells subsets and key demographic and clinical characteristics are summarized in
Table 2 and
Table 3. Leukocyte (
p < 0.001) and neutrophil numbers (
p < 0.001) as well as the fraction of FoxP3
+ T
reg (
p = 0.02) were higher in patients with AIS compared with patients with TIA. In contrast, the number of monocytes was lower in patients with AIS than in patients with TIA (
p = 0.02). Older patients showed a lower quantity of lymphocytes (
p = 0.02) and a smaller fraction of CD4
+CD8
− T cells (
p = 0.03). Severity of stroke at admission was associated with different immune cell subsets (NIHSS: leukocytes,
p = 0.05, neutrophils,
p = 0.007, CD4
+CD8
− cells,
p = 0.004; Barthel Index: leukocytes,
p = 0.01, neutrophils,
p = 0.001). Again, leukocytes (
p = 0.01) and neutrophils (
p = 0.003) were associated with thrombolysis. Interestingly, sex and pretreatment with platelet inhibitors did not influence the number or fraction of immune cell subsets.
Table 2.
Predictors of the absolute number or fraction of immune cells in patients with acute ischemic stroke/transient ischemic attack (univariate analysis; leukocytes, lymphocytes, neutrophils, monocytes).
Table 2.
Predictors of the absolute number or fraction of immune cells in patients with acute ischemic stroke/transient ischemic attack (univariate analysis; leukocytes, lymphocytes, neutrophils, monocytes).
| Immune Cell Subset | Leukocytes/nL (Mean ± SD) | p Value | Lymphocytes/nL (Mean ± SD) | p Value | Neutrophils/nL (Mean ± SD) | p Value | Monocytes/nL (Mean ± SD) | p Value |
|---|
| Sex |
| Male | 7.9 ± 2.7 | - | 1.7 ± 0.5 | - | 5.4 ± 2.5 | - | 0.7 ± 0.3 | - |
| Female | 7.9 ± 2.6 | 0.76 | 1.6 ± 0.7 | 0.24 | 5.5 ± 2.7 | 0.60 | 0.6 ± 0.2 | 0.80 |
| Age, years |
| <55 | 8.0 ± 3.2 | - | 2.0 ± 0.6 | - | 5.1 ± 3.1 | - | 0.6 ± 0.4 | - |
| 55–64 | 8.0 ± 2.2 | - | 1.7 ± 0.5 | - | 5.5 ± 1.9 | - | 0.6 ± 0.2 | - |
| 65–74 | 7.6 ± 2.2 | - | 1.7 ± 0.7 | - | 5.2 ± 1.9 | - | 0.7 ± 0.3 | - |
| 75–84 | 7.5 ± 2.3 | - | 1.5 ± 0.5 | - | 5.3 ± 2.3 | - | 0.6 ± 0.2 | - |
| >84 | 9.0 ± 4.5 | 0.85 | 1.3 ± 0.6 | 0.02 | 6.9 ± 4.7 | 0.63 | 0.6 ± 0.2 | 0.71 |
| Disease modality |
| AIS | 8.6 ± 2.9 | - | 1.7 ± 0.6 | - | 6.2 ± 2.8 | - | 0.6 ± 0.2 | - |
| TIA | 6.9 ± 1.9 | <0.001 | 1.6 ± 0.6 | 0.36 | 4.4 ± 1.8 | <0.001 | 0.7 ± 0.3 | 0.02 |
| Modified TOAST criteria |
| Cardioembolism | 8.0 ± 2.9 | - | 1.6 ± 0.6 | - | 5.6 ± 2.9 | - | 0.6 ± 0.2 | - |
| Large-artery atherosclerosis | 7.1 ± 2.0 | - | 1.8 ± 0.4 | - | 4.6 ± 1.9 | - | 0.6 ± 0.1 | - |
| Small-vessel occlusion | 7.8 ± 2.1 | - | 1.8 ± 0.5 | - | 5.0 ± 1.9 | - | 0.7 ± 0.2 | - |
| Other determined or undetermined etiology | 7.7 ± 2.3 | 0.94 | 1.5 ± 0.6 | 0.32 | 5.4 ± 2.2 | 0.91 | 0.6 ± 0.2 | 0.80 |
| Duration between symptom onset and blood withdrawal, h |
| <5 | 7.7 ± 2.2 | - | 1.6 ± 0.6 | - | 5.4 ± 2.2 | - | 0.6 ± 0.2 | - |
| 5–12 | 7.5 ± 2.4 | - | 1.7 ± 0.6 | - | 5.0 ± 2.2 | - | 0.6 ± 0.2 | - |
| 12–24 | 8.4 ± 2.3 | 0.14 | 1.3 ± 0.4 | 0.63 | 6.3 ± 2.5 | 0.05 | 0.7 ± 0.1 | 0.80 |
| National Institutes of Health Stroke Scale |
| 0–4 | 7.4 ± 2.2 | - | 1.7 ± 0.6 | - | 4.8 ± 2.0 | - | 0.6 ± 0.2 | - |
| 5–9 | 8.5 ± 2.8 | - | 1.5 ± 0.4 | - | 6.2 ± 2.6 | - | 0.7 ± 0.3 | - |
| 10–15 | 8.8 ± 3.1 | - | 1.7 ± 0.7 | - | 6.3 ± 2.9 | - | 0.7 ± 0.3 | - |
| >15 | 9.6 ± 4.1 | 0.05 | 1.2 ± 0.4 | 0.06 | 7.7 ± 4.4 | 0.007 | 0.6 ± 0.1 | 0.88 |
| Barthel Index |
| 0–30 | 9.7 ± 4.4 | - | 1.2 ± 0.6 | - | 7.7 ± 4.7 | - | 0.6 ± 0.2 | - |
| 35–70 | 8.5 ± 2.7 | - | 1.6 ± 0.5 | - | 6.1 ± 2.6 | - | 0.7 ± 0.3 | - |
| >70 | 6.9 ± 1.7 | 0.01 | 1.8 ± 0.6 | 0.048 | 4.3 ± 1.5 | 0.001 | 0.6 ± 0.2 | 0.13 |
| Thrombolysis |
| Yes | 8.6 ± 2.2 | - | 1.6 ± 0.4 | - | 6.2 ± 2.3 | - | 0.7 ± 0.3 | - |
| No | 7.6 ± 2.8 | 0.01 | 1.7 ± 0.7 | 0.99 | 5.1 ± 2.7 | 0.003 | 0.6 ± 0.2 | 0.38 |
| Platelet inhibitor before blood withdrawal |
| Yes | 8.0 ± 2.9 | - | 1.7 ± 0.6 | - | 5.6 ± 2.9 | - | 0.6 ± 0.2 | - |
| No | 7.6 ± 2.2 | 0.60 | 1.6 ± 0.6 | 0.42 | 5.2 ± 2.0 | 0.83 | 0.7 ± 0.3 | 0.81 |
Table 3.
Predictors of the absolute number or fraction of immune cells in patients with acute ischemic stroke/transient ischemic attack (univariate analysis; (CD4+CD8− T cells, CD8+CD4− T cells, FoxP3 Treg).
Table 3.
Predictors of the absolute number or fraction of immune cells in patients with acute ischemic stroke/transient ischemic attack (univariate analysis; (CD4+CD8− T cells, CD8+CD4− T cells, FoxP3 Treg).
| Immune Cell Subset | CD4+CD8− Cells/Gated Cells (%) (Mean ± SD) | p Value | CD8+CD4− Cells/Gated Cells (%) (Mean ± SD) | p Value | FoxP3+ Cells/Gated Cells (%) (Mean ± SD) | p Value |
|---|
| Sex |
| Male | 46.3 ± 11.3 | - | 29.9 ± 11.6 | - | 2.4 ± 1.1 | - |
| Female | 47.7 ± 11.8 | 0.51 | 25.8 ± 9.8 | 0.04 | 2.4 ± 1.4 | 0.36 |
| Age, years |
| <55 | 50.1 ± 9.8 | - | 24.9 ± 9.7 | - | 2.8 ± 1.3 | - |
| 55–64 | 49.2 ± 11.2 | - | 28.5 ± 12.2 | - | 2.3 ± 1.2 | - |
| 65–74 | 50.1 ± 10.1 | - | 26.7 ± 9.9 | - | 2.4 ± 1.2 | - |
| 75–84 | 41.6 ± 11.8 | - | 31.8 ± 11.0 | - | 2.4 ± 1.3 | - |
| >84 | 42.5 ± 12.9 | 0.03 | 24.9 ± 11.7 | 0.22 | 2.2 ± 1.1 | 0.81 |
| Disease modality |
| AIS | 49.2 ± 10.4 | - | 26.0 ± 9.6 | - | 2.7 ± 1.2 | - |
| TIA | 45.3 ± 12.1 | 0.09 | 29.4 ± 11.7 | 0.24 | 2.2 ± 1.2 | 0.02 |
| Modified TOAST criteria |
| Cardioembolism | 46.0 ± 12.1 | - | 29.3 ± 11.0 | - | 2.4 ± 1.3 | - |
| Large-artery atherosclerosis | 55.0 ± 12.2 | - | 21.2 ± 6.7 | - | 3.3 ± 1.3 | - |
| Small-vessel occlusion | 51.1 ± 7.2 | - | 24.8 ± 8.7 | - | 2.7 ± 1.2 | - |
| Other determined or undetermined etiology | 46.4 ± 11.2 | 0.27 | 27.0 ± 12.0 | 0.35 | 2.1 ± 1.0 | 0.23 |
| Duration between symptom onset and blood withdrawal, h |
| <5 | 49.4 ± 8.5 | - | 26.4 ± 8.7 | - | 2.4 ± 1.0 | - |
| 5–12 | 47.2 ± 11.4 | - | 27.7 ± 10.1 | - | 2.5 ± 1.3 | - |
| 12–24 | 49.8 ± 13.8 | 0.86 | 18.9 ± 2.1 | 0.47 | 2.7 ± 0.2 | 0.59 |
| National Institutes of Health Stroke Scale |
| 0–4 | 48.5 ± 10.6 | - | 26.6 ± 9.5 | - | 2.5 ± 1.1 | - |
| 5–9 | 48.7 ± 10.6 | - | 28.6 ± 10.4 | - | 2.7 ± 1.4 | - |
| 10–15 | 47.5 ± 11.2 | - | 29.1 ± 7.1 | - | 2.3 ± 1.3 | - |
| >15 | 32.2 ± 11.7 | 0.004 | 35.2 ± 20.1 | 0.66 | 1.4 ± 0.9 | 0.03 |
| Barthel Index |
| 0–30 | 43.7 ± 12.0 | - | 23.8 ± 5.2 | - | 2.0 ± 1.3 | - |
| 35–70 | 45.6 ± 10.0 | - | 28.0 ± 11.3 | - | 2.4 ± 1.2 | - |
| >70 | 50.3 ± 9.3 | 0.16 | 25.7 ± 8.4 | 0.58 | 2.7 ± 1.3 | 0.37 |
| Thrombolysis |
| Yes | 45.4 ± 10.5 | - | 27.7 ± 13.3 | - | 2.3 ± 1.4 | - |
| No | 47.6 ± 11.9 | 0.32 | 28.1 ± 10.0 | 0.39 | 2.4 ± 1.1 | 0.31 |
| Platelet inhibitor before blood withdrawal |
| Yes | 45.6 ± 11.5 | - | 28.4 ± 10.8 | - | 2.4 ± 1.2 | - |
| No | 49.3 ± 11.2 | 0.11 | 27.3 ± 11.5 | 0.49 | 2.4 ± 1.2 | 0.97 |
Multivariate analysis (adjusted for age and sex) (
Table 4,
Table 5,
Table 6 and
Table 7) identified disease modality (AIS
vs. TIA) as an independent predictor of leukocyte (
p = 0.006), neutrophil (
p = 0.005), and monocyte count (
p = 0.04). Sex was only associated with the fraction of CD8
+CD4
− T cells (
p = 0.03). Age only accounted for CD4
+CD8
− T cell regulation (
p = 0.012). NIHSS scores were independent predictors of the CD4
+CD8
− as well as the CD8
+CD4
− fractions (
p = 0.02 and 0.03, respectively). We found no independent predictor of FoxP3 T
reg. In addition, none of the measured variables (leukocytes,
p = 0.48; neutrophils,
p = 0.54; lymphocytes,
p = 0.81; monocytes,
p = 0.81; CD4
+CD8
− T cells,
p = 0.65; CD8
+CD4
− T cells,
p = 0.65; FoxP3 T
reg,
p = 0.95) were influenced by the time of blood withdrawal (Days 0, 1, and 3; data not shown).
Table 4.
Predictors of absolute numbers of leukocytes and lymphocytes in patients with acute ischemic stroke/transient ischemic attack (multivariate analysis).
Table 4.
Predictors of absolute numbers of leukocytes and lymphocytes in patients with acute ischemic stroke/transient ischemic attack (multivariate analysis).
| Immune Cell Subset | Leukocytes | Lymphocytes |
|---|
| Coefficient | 95% CI | p Value | Coefficient | 95% CI | p Value |
|---|
| Sex | Male | Reference | - | - | Reference | - | - |
| Female | −0.4 ± 0.9 | −1.1 to 1.0 | 0.93 | 0.0 ± 0.1 | −0.2 to 0.3 | 0.71 |
| Age, years | - | - | 0.74 | - | - | 0.003 |
| <55 | Reference | - | - | Reference | - | - |
| 55–64 | −0.5 ± 0.9 | −2.2 to 1.3 | - | −0.3 ± 0.2 | −0.7 to 0.1 | - |
| 65–74 | −0.4 ± 0.8 | −2.0 to 1.3 | - | −0.4 ± 0.2 | −0.7 to 0.0 | - |
| 75–84 | −0.7 ± 0.9 | −2.4 to 1.0 | - | −0.5 ± 0.2 | −0.9 to −0.1 | - |
| >84 | 0.5 ± 1.1 | −1.7 to 2.6 | - | −0.6 ± 0.2 | −1.1 to −0.2 | - |
| Disease modality (TIA vs. AIS) | 1.5 ± 0.5 | 0.4 to 2.6 | 0.006 | −0.1 ± 0.1 | −0.3 to 0.2 | 0.66 |
| National Institutes of Health Stroke Scale | - | - | 0.11 | - | - | 0.052 |
| 0–4 | Reference | - | - | Reference | - | - |
| 5–9 | 0.8 ± 0.8 | −0.7 to 2.3 | - | −0.3 ± 0.2 | −0.6 to 0.1 | - |
| 10–15 | 0.8 ± 0.9 | −0.9 to 2.6 | - | −0.1 ± 0.2 | −0.5 to 0.3 | - |
| >15 | 1.3 ± 1.0 | −0.8 to 3.3 | - | −0.5 ± 0.2 | −1.0 to −0.1 | - |
| Thrombolysis | 0.1 ± 0.7 | −1.3 to 1.4 | 0.94 | 0.1 ± 0.2 | −0.20 to 0.4 | 0.53 |
| Use of platelet inhibitor before blood taking | 0.5 ± 0.5 | −0.6 to 1.6 | 0.34 | 0.2 ± 0.1 | −0.1 to 0.4 | 0.17 |
Table 5.
Predictors of absolute numbers of neutrophils and monocytes in patients with acute ischemic stroke/transient ischemic attack (multivariate analysis).
Table 5.
Predictors of absolute numbers of neutrophils and monocytes in patients with acute ischemic stroke/transient ischemic attack (multivariate analysis).
| Immune Cell Subset | Neutrophils | Monocytes |
|---|
| Coefficient | 95% CI | p Value | Coefficient | 95% CI | p Value |
|---|
| Sex | Male | Reference | - | - | Reference | - | - |
| Female | −0.0 ± 0.5 | −1.0 to 0.9 | 0.98 | −0.0 ± 0.1 | −0.1 to 0.1 | 0.53 |
| Age, years | - | - | 0.25 | - | - | 0.53 |
| <55 | Reference | - | - | Reference | - | - |
| 55–64 | −0.1 ± 0.8 | −1.8 to 1.5 | - | −0.0 ± 0.1 | −0.2 to 0.1 | - |
| 65–74 | 0.1 ± 0.8 | −1.5 to 1.6 | - | 0.0 ± 0.1 | −0.1 to 0.2 | - |
| 75–84 | −0.1 ± 0.8 | −1.7 to 1.5 | - | −0.0 ± 0.1 | −0.2 to 0.1 | - |
| >84 | 1.2 ± 1.0 | −0.8 to 3.2 | - | −0.1 ± 0.1 | −0.3 to 0.1 | - |
| Disease modality (TIA vs. AIS) | 1.5 ± 0.5 | 0.5 to 2.5 | 0.005 | 0.1 ± 0.1 | 0.0 to 0.2 | 0.04 |
| National Institutes of Health Stroke Scale | - | - | 0.031 | - | - | 0.72 |
| 0–4 | Reference | - | - | Reference | - | - |
| 5–9 | 1.0 ± 0.7 | −0.4 to 2.5 | - | 0.0 ± 0.1 | −0.1 to 0.2 | - |
| 10–15 | 1.0 ± 0.8 | −0.7 to 2.6 | - | 0.0 ± 0.1 | −0.1 to 0.2 | - |
| >15 | 1.8 ± 1.0 | −0.2 to 3.7 | - | 0.0 ± 0.1 | −0.2 to 0.2 | - |
| Thrombolysis | 0.0 ± 0.6 | −1.2 to 1.3 | 0.96 | −0.0 ± 0.1 | −0.1 to 0.1 | 0.88 |
| Use of platelet inhibitor before blood taking | 2.4 ± 1.2 | 0.1 to 4.7 | 0.46 | −0.0 ± 0.1 | −0.1 to 0.1 | 0.58 |
Table 6.
Predictors of fractions of CD4+CD8− and CD8+CD4− T cells in patients with acute ischemic stroke/transient ischemic attack (multivariate analysis).
Table 6.
Predictors of fractions of CD4+CD8− and CD8+CD4− T cells in patients with acute ischemic stroke/transient ischemic attack (multivariate analysis).
| Immune Cell Subset | CD4+CD8− Cells | CD8+CD4− Cells |
|---|
| Coefficient | 95% CI | p Value | Coefficient | 95% CI | p Value |
|---|
| Sex | Male | Reference | - | - | Reference | - | - |
| Female | 2.8 ± 2.1 | −1.3 to 6.9 | 0.18 | −4.7 ± 2.1 | −8.8 to −0.5 | 0.03 |
| Age, years | - | - | 0.012 | - | - | 0.63 |
| <55 | Reference | - | - | Reference | - | - |
| 55–64 | −0.5 ± 3.6 | −7.7 to 6.7 | - | 3.8 ± 3.6 | −3.4 to 11.0 | - |
| 65–74 | −1.5 ± 3.4 | −8.2 to 5.3 | - | 3.4 ± 3.4 | −3.4 to 10.2 | - |
| 75–84 | −8.7 ± 3.5 | −15.7 to −1.6 | - | 6.9 ± 3.6 | −0.2 to 14.0 | - |
| >84 | −5.0 ± 4.4 | −13.7 to 3.7 | - | −0.6 ± 4.4 | −9.3 to 8.2 | - |
| Disease modality (TIA vs. AIS) | −2.7 ± 2.2 | −7.1 to 1.7 | 0.22 | 2.5 ± 2.2 | −1.9 to 6.9 | 0.26 |
| National Institutes of Health Stroke Scale | - | - | 0.02 | - | - | 0.03 |
| 0–4 | Reference | - | - | Reference | - | - |
| 5–9 | 1.5 ± 3.1 | −4.6 to 7.6 | - | 3.3 ± 3.1 | −2.9 to 9.4 | - |
| 10–15 | −0.0 ± 3.8 | −7.5 to 7.5 | - | 2.1 ± 3.8 | −5.5 to 9.7 | - |
| >15 | −12.9 ± 4.2 | −21.2 to −4.7 | - | 11.2 ± 4.2 | 2.8 to 19.5 | - |
| Thrombolysis | −1.1 ± 2.7 | −6.4 to 4.2 | 0.67 | −0.3 ± 2.7 | −8.6 to 2.1 | 0.24 |
| Use of platelet inhibitor before blood taking | −1.9 ± 2.2 | −6.3 to 2.4 | 0.39 | −0.7 ± 2.2 | −5.1 to 3.7 | 0.77 |
Table 7.
Predictors of fraction of FoxP3 Treg in patients with acute ischemic stroke/transient ischemic attack (multivariate analysis).
Table 7.
Predictors of fraction of FoxP3 Treg in patients with acute ischemic stroke/transient ischemic attack (multivariate analysis).
| Immune Cell Subset | FoxP3+ Cells |
|---|
| Coefficient | 95% CI | p Value |
|---|
| Sex | Male | Reference | - | - |
| Female | −0.0 ± 0.2 | −0.5 to 0.5 | 0.95 |
| Age, years | - | - | 0.57 |
| <55 | Reference | - | - |
| 55–64 | −0.3 ± 0.4 | −1.1 to 0.5 | - |
| 65–74 | −0.4 ± 0.4 | −1.2 to 0.4 | - |
| 75–84 | −0.3 ± 0.4 | −1.2 to 0.5 | - |
| >84 | −0.2 ± 0.5 | −1.2 to 0.8 | - |
| Disease modality (TIA vs. AIS) | −0.4 ± 0.3 | −0.9 to 0.2 | 0.16 |
| National Institutes of Health Stroke Scale | - | - | 0.13 |
| 0–4 | Reference | - | - |
| 5–9 | 0.3 ± 0.4 | −0.4 to 0.1 | - |
| 10–15 | −0.1 ± 0.4 | −0.9 to 0.8 | - |
| >15 | −1.0 ± 0.5 | −2.0 to −0.1 | - |
| Thrombolysis | 0.1 ± 0.3 | −0.5 to 0.7 | 0.80 |
| Use of platelet inhibitor before blood taking | 0.1 ± 0.3 | −0.4 to 0.6 | 0.69 |
2.4. Discussion
In this case-control study, we analyzed peripheral immune responses in different cerebrovascular disease settings and showed that the number or fraction of distinct immune cell subsets is differentially regulated between patients with AIS/TIA and CCD, compared with HV. Moreover, within the AIS/TIA group, several clinical (e.g., NIHSS, Barthel index, thrombolysis or not, AIS or TIA) or demographic (age, sex) parameters predicted the number or fraction of immune cells even after adjustment for age and sex.
Most of our findings in patients with AIS/TIA are consistent with the results of previously published studies regarding ischemic stroke [
1,
2,
32,
33,
34,
35]. However, in contrast to other observations [
24,
36], we found no change in the number of monocytes during the observation period until day 3. Of note, a low fraction of CD4
+CD8
− T cells and a high percentage of CD8
+CD4
− T cells were independently associated with high clinical severity of patients with AIS/TIA at admission. This observation can be confirmed by a study showing that subjects with a high fraction of CD8
+ cells often have comorbidities that include insulin resistance and an increased risk of cardiovascular events [
36]. Therefore, despite evidence for reduced cytotoxic function of CD8
+ T cells in AIS [
26], it can be hypothesized that especially CD8
+ cells have detrimental properties in cardiovascular disease. FoxP3 T
reg were associated with clinical severity in univariate analysis but not after adjustment for age and sex.
Very importantly, other diseases of the CNS—such as like aneurysmal subarachnoid hemorrhage [
4] or acute cerebral hemorrhage [
25]—are also associated with changes in peripheral immune cell homeostasis and distribution, showing that peripheral immune cell modulation is an unspecific response to various acute CNS diseases [
7,
8]. Nevertheless, kinetics of immune cell regulation might be different between various CNS diseases. In contrast to our results in ischemic stroke, Shi
et al. [
25] reported an increase in T
reg over time in patients with intracerebral hemorrhage and Sarrafzadeh
et al. [
4] found an increase in CD4
+ and CD8
+ T cells in a subpopulation of patients in the first days after aneurysmal subarachnoid hemorrhage.
Despite clear evidence that inflammatory mechanisms and immune cells play an important part in the pathophysiology of atherosclerosis—including plaque progression and instability [
31,
37]—to the best of our knowledge, this report is the first description of the detailed regulation of immune cell subsets in CCD. The numbers of leukocytes, neutrophils, and lymphocytes in patients with CCD lie between those seen for patients with AIS/TIA and HV, pointing towards a hypothetical sequence of disease from healthy persons to chronic cerebrovascular atherosclerotic lesions (extracranial and/or intracranial) and finally AIS. Very interestingly, FoxP3
+ T
reg were even higher in patients with CCD compared with those with AIS/TIA, suggesting a pathophysiologic role of T
reg in CCD. Atherosclerosis is currently understood as a systemic disease that might also be influenced by pro- and anti-inflammatory cytokines. A recent report suggested that the level of detrimental cytokines could be decreased by physical exercise [
38]. Further studies are needed to better understand the underlying pathophysiology.
As immune cells are not only biomarkers after ischemic stroke, but also potential therapeutic targets [
23], a detailed characterization of their regulation is absolutely necessary for elaborating the best treatment strategy and also for improving the translation of promising preclinical agents into the clinic. We identified several variables that independently predicted the number or fraction of various immune cell subsets (AIS
vs. TIA, age, sex, NIHSS). It seems that the number of immune cells depends on various non-modifiable clinical and demographic variables, making it difficult to develop universal treatment strategies.
There are several limitations to this study that should be considered. First, it should be remembered that the potential for reverse causation as a result of blood withdrawal following a cerebrovascular event cannot be disregarded. Accordingly, the current study describes the magnitude and significance of associations between immune cell subsets and demographic/clinical parameters without attributing causality. Further prospective studies are required to formally elucidate causality. Second, all patients were required to provide informed consent before participating in the study. However, this may have resulted in patients who have suffered a severe stroke and/or aphasia being underrepresented in this study because neurological deficits related to their condition may have prevented them from being capable of providing informed consent. Third, it was not possible to completely rule out a non-vascular origin for symptoms in 42% of the TIA patient population, meaning that the possibility of the aforementioned factors influencing the regulation of immune cell subsets remains.



{kind=link}
{kind=link}

