
The Efficacy of Non-Pharmacological Interventions on Brain-Derived Neurotrophic Factor in Schizophrenia: A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Methods
2.1. Search Strategy and Selection Criteria
2.2. Data Extraction
2.3. Assessment of Risk of Bias
2.4. Data Synthesis
3. Results
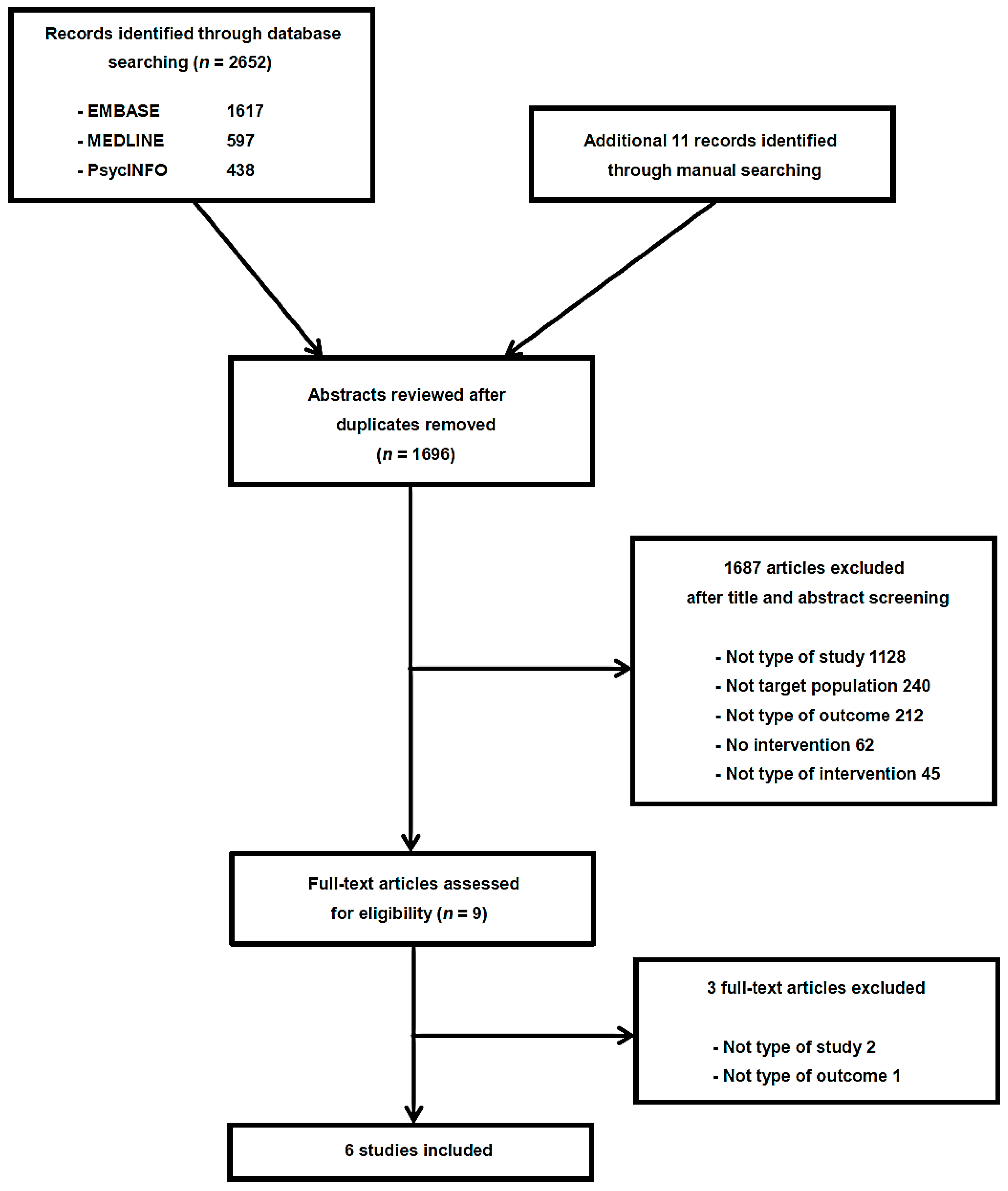
3.1. Included Randomized Controlled Trials (RCTs)
3.2. Risk of Bias
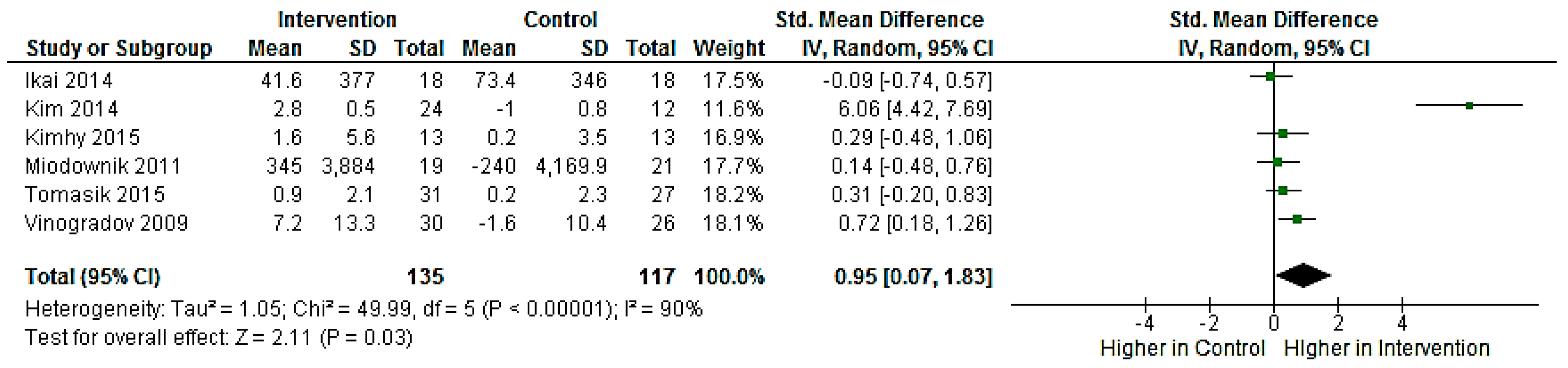
3.3. Meta-Analyses
3.4. Subgroup Analyses
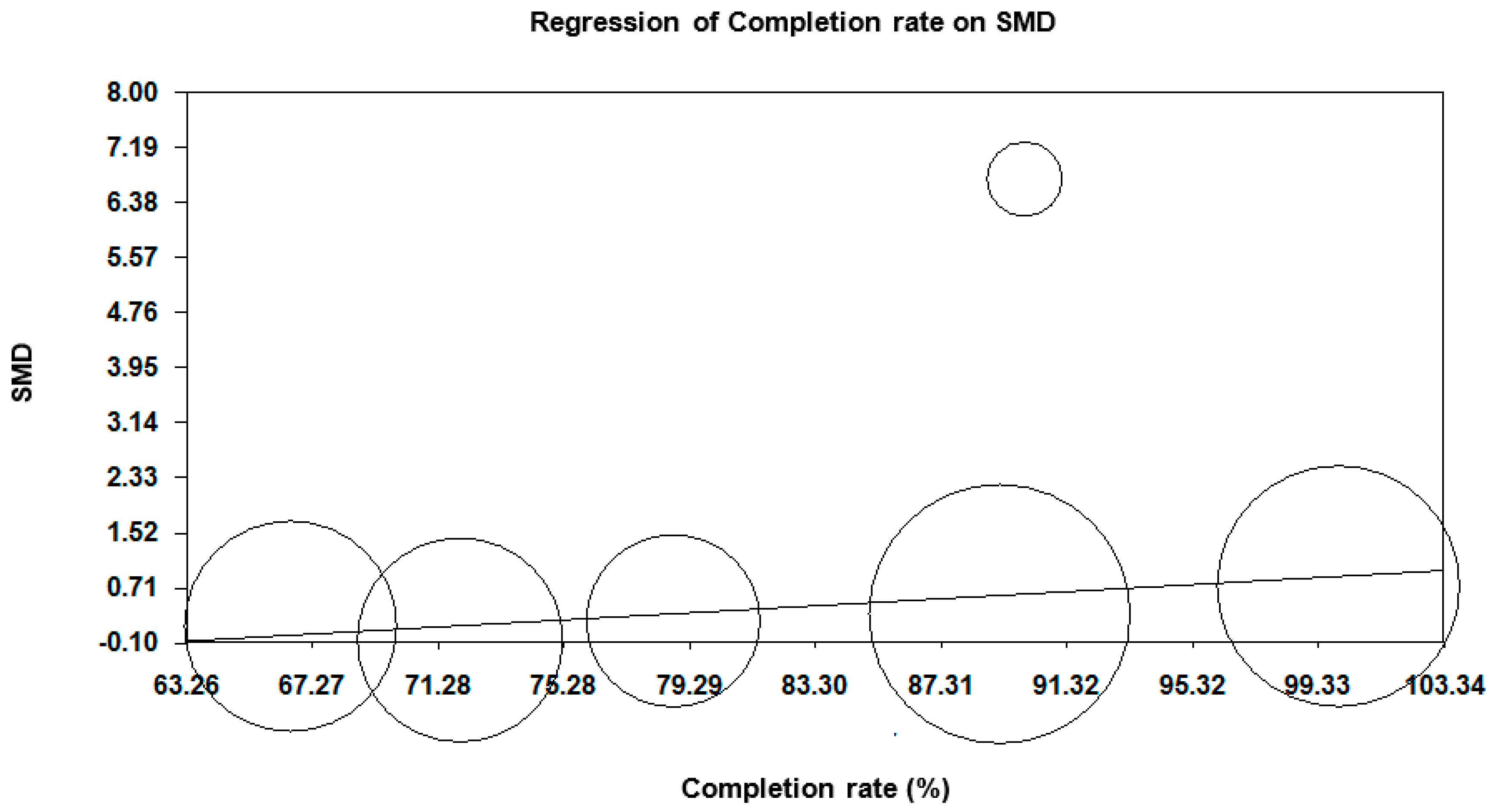
3.5. Meta-Regression Analyses
3.6. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Goff, D.C. Future perspectives on the treatment of cognitive deficits and negative symptoms in schizophrenia. World Psychiatry 2013, 12, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Pawełczyk, T.; Grancow-Grabka, M.; Kotlicka, M.; Trafalska, E.; Pawełczyk, A. A randomized controlled study of the efficacy of six-month supplementation with concentrated fish oil rich in omega-3 polyunsaturated fatty acids in first episode schizophrenia. J. Psychiatr. Res. 2016, 73, 34–44. [Google Scholar] [CrossRef] [PubMed]
- Dean, O.M.; Mancuso, S.G.; Bush, A.I.; Copolov, D.; Do, K.Q.; Cuénod, M.; Conus, P.; Rossell, S.L.; Castle, D.J.; Berk, M. Benefits of adjunctive N-acetylcysteine in a sub-group of clozapine-treated individuals diagnosed with schizophrenia. Psychiatry Res. 2015, 230, 982–983. [Google Scholar] [CrossRef] [PubMed]
- Roffman, J.L.; Lamberti, J.S.; Achtyes, E.; Macklin, E.A.; Galendez, G.C.; Raeke, L.H.; Silverstein, N.J.; Smoller, J.W.; Hill, M.; Goff, D.C. Randomized multicenter investigation of folate plus vitamin B12 supplementation in schizophrenia. JAMA Psychiatry 2013, 70, 481–489. [Google Scholar] [CrossRef] [PubMed]
- López-Navarro, E.; del Canto, C.; Belber, M.; Mayol, A.; Fernández-Alonso, O.; Lluis, J.; Munar, E.; Chadwick, P. Mindfulness improves psychological quality of life in community-based patients with severe mental health problems: A pilot randomized clinical trial. Schizophr. Res. 2015, 168, 530–536. [Google Scholar] [CrossRef] [PubMed]
- Binder, D.K.; Scharfman, H.E. Brain-derived neurotrophic factor. Growth Factors 2004, 22, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeld, R.D.; Zeni, L.; Haniu, M.; Talvenheimo, J.; Radka, S.F.; Bennett, L.; Miller, J.A.; Welcher, A.A. Purification and identification of brainderived neurotrophic factor from human serum. Protein Expr. Purif. 1995, 6, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Harrisberger, F.; Smieskova, R.; Schmidt, A.; Lenz, C.; Walter, A.; Wittfeld, K.; Grabe, H.J.; Lang, U.E.; Fusar-Poli, P.; Borgwardt, S. BDNF Val66Met polymorphism and hippocampal volume in neuropsychiatric disorders: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2015, 55, 107–118. [Google Scholar] [CrossRef] [PubMed]
- Martinotti, G.; Pettorruso, M.; de Berardis, D.; Varasano, P.A.; Pressanti, G.L.; de Remigis, V.; Valchera, A.; Ricci, V.; di Nicola, M.; Janiri, L.; et al. Agomelatine increases BDNF serum levels in depressed patients in correlation with the improvement of depressive symptoms. Int. J. Neuropsychopharmacol. 2016, 19, pyw003. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Li, X.X.; Hu, X.Z. Post-traumatic stress disorder risk and brain-derived neurotrophic factor Val66Met. World J. Psychiatry 2016, 6, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Li, X.; Xin, X.; Kan, P.C.; Yan, Y. MicroRNA-613 regulates the expression of brain-derived neurotrophic factor in Alzheimer’s disease. Biosci. Trends 2016. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, B.S.; Steiner, J.; Berk, M.; Molendijk, M.L.; Gonzalez-Pinto, A.; Turck, C.W.; Nardin, P.; Gonçalves, C.A. Peripheral brain-derived neurotrophic factor in schizophrenia and the role of antipsychotics: Meta-analysis and implications. Mol. Psychiatry 2015, 20, 1108–1119. [Google Scholar] [CrossRef] [PubMed]
- Pillai, A.; Kale, A.; Joshi, S.; Naphade, N.; Raju, M.S.; Nasrallah, H.; Mahadik, S.P. Decreased BDNF levels in CSF of drug-naive first-episode psychotic subjects: Correlation with plasma BDNF and psychopathology. Int. J. Neuropsychopharmacol. 2010, 13, 535–539. [Google Scholar] [CrossRef] [PubMed]
- Kuo, F.C.; Lee, C.H.; Hsieh, C.H.; Kuo, P.; Chen, Y.C.; Hung, Y.J. Lifestyle modification and behavior therapy effectively reduce body weight and increase serum level of brain-derived neurotrophic factor in obese non-diabetic patients with schizophrenia. Psychiatry Res. 2013, 209, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Shiina, A.; Kanahara, N.; Sasaki, T.; Oda, Y.; Hashimoto, T.; Hasegawa, T.; Yoshida, T.; Iyo, M.; Hashimoto, K. An open study of sulforaphane-rich broccoli sprout extract in patients with schizophrenia. Clin. Psychopharmacol. Neurosci. 2015, 13, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0. 2011. Available online: http://handbook.cochrane.org/ (accessed on 9 December 2015).
- Booth, A.; Clarke, M.; Ghersi, D.; Moher, D.; Petticrew, M.; Stewart, L. An international registry of systematic-review protocols. Lancet 2011, 377, 108–109. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gotzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. Cochrane Bias Methods Group; Cochrane Statistical Methods Group: The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Hedges, L.V.; Olkin, I. Statistical Methods for Meta Analysis; Academic Press: Orlando, FL, USA, 1985. [Google Scholar]
- Cooper, H.; Hedges, L. The Handbook of Research Synthesis; Russell Sage Foundation Press: New York, NY, USA, 1994. [Google Scholar]
- Hirschberg, R.; Cohen, A.H.; Kopple, J.D. Effects of keto acid supplements on renal function and histology in azotemic rats fed high-protein diets. Am. J. Nephrol. 1988, 8, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Hedges, L.V.; Vevea, J.L. Fixed-and random-effects models in meta-analysis. Psychol. Methods 1998, 3, 486–504. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Hannah, R. Introduction to Meta-Analysis; John Wiley & Sons Ltd.: Chichester, UK, 2009. [Google Scholar]
- Duval, S.; Tweedie, R. Trim and Fill: A Simple Funnel-Plot-Based Method. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Vevea, J.L.; Woods, C.M. Publication bias in research synthesis: Sensitivity analysis using a priori weight functions. Psychol. Methods 2005, 10, 428–443. [Google Scholar] [CrossRef] [PubMed]
- Cuijpers, P.; van Straten, A.; Andersson, G.; van Oppen, P. Psychotherapy for depression in adults: A meta-analysis of comparative outcome studies. J. Consult. Clin. Psychol. 2008, 76, 909–922. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detect by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Vinogradov, S.; Fisher, M.; Holland, C.; Shelly, W.; Wolkowitz, O.; Mellon, S.H. Is serum brain-derived neurotrophic factor a biomarker for cognitive enhancement in schizophrenia? Biol. Psychiatry 2009, 66, 549–553. [Google Scholar] [CrossRef] [PubMed]
- Kimhy, D.; Vakhrusheva, J.; Bartels, M.N.; Armstrong, H.F.; Ballon, J.S.; Khan, S.; Chang, R.W.; Hansen, M.C.; Ayanruoh, L.; Lister, A.; et al. The impact of aerobic exercise on brain-derived neurotrophic factor and neurocognition in individuals with schizophrenia: A single-blind, randomized clinical trial. Schizophr. Bull. 2015, 41, 859–868. [Google Scholar] [CrossRef] [PubMed]
- Tomasik, J.; Yolken, R.H.; Bahn, S.; Dickerson, F.B. Immunomodulatory effects of probiotic supplementation in schizophrenia patients: A randomized, placebo-controlled trial. Biomark. Insights 2015, 10, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Ikai, S.; Suzuki, T.; Uchida, H.; Saruta, J.; Tsukinoki, K.; Fujii, Y.; Mimura, M. Effects of weekly one-hour Hatha yoga therapy on resilience and stress levels in patients with schizophrenia-spectrum disorders: An eight-week randomized controlled trial. J. Altern. Complement. Med. 2014, 20, 823–830. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Song, B.K.; So, B.; Lee, O.; Song, W.; Kim, Y. Increase of circulating BDNF levels and its relation to improvement of physical fitness following 12 weeks of combined exercise in chronic patients with schizophrenia: A pilot study. Psychiatry Res. 2014, 220, 792–796. [Google Scholar] [CrossRef] [PubMed]
- Miodownik, C.; Maayan, R.; Ratner, Y.; Lerner, V.; Pintov, L.; Mar, M.; Weizman, A.; Ritsner, M.S. Serum levels of brain-derived neurotrophic factor and cortisol to sulfate of dehydroepiandrosterone molar ratio associated with clinical response to L-theanine as augmentation of antipsychotic therapy in schizophrenia and schizoaffective disorder patients. Clin. Neuropharmacol. 2011, 34, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Rey, M.J.; Schulz, P.; Costa, C.; Dick, P.; Tissot, R. Guidelines for the dosage of neuroleptics. I: Chlorpromazine equivalents of orally administered neuroleptics. Int. Clin. Psychopharmacol. 1989, 4, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Inagaki, A.; Inada, T.; Fujii, Y.; Yagi, G.; Yoshio, T.; Nakamura, H.; Yamauchi, T. Equivalent Dose of Psychotropics (in Japanese); Seiwa Shoten: Tokyo, Japan, 1999. [Google Scholar]
- Woods, S.W. Chlorpromazine equivalent doses for the newer atypical antipsychotics. J. Clin. Psychiatry 2003, 64, 663–667. [Google Scholar] [CrossRef] [PubMed]
- Inagaki, A.; Inada, T. Dose equivalence of psychotropic drugs. Part XXI: Dose equivalence of novel antipsychotics: Blonanserin. Jpn. J. Clin. Psychopharmacol. 2008, 11, 887–890. [Google Scholar]
- Pirildar, S.; Gonul, A.S.; Taneli, F.; Akdeniz, F. Low serum levels of brain-derived neurotrophic factor in patients with schizophrenia do not elevate after antipsychotic treatment. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2004, 28, 709–713. [Google Scholar] [CrossRef] [PubMed]
- Hori, H.; Yoshimura, R.; Yamada, Y.; Ikenouchi, A.; Mitoma, M.; Ida, Y.; Nakamura, J. Effects of olanzapine on plasma levels of catecholamine metabolites, cytokines, and brain-derived neurotrophic factor in schizophrenic patients. Int. Clin. Psychopharmacol. 2007, 22, 21–27. [Google Scholar] [PubMed]
- González-Pinto, A.; Mosquera, F.; Palomino, A.; Alberich, S.; Gutiérrez, A.; Haidar, K.; Vega, P.; Barbeito, S.; Ortiz, A.; Matute, C. Increase in brain-derived neurotrophic factor in first episode psychotic patients after treatment with atypical antipsychotics. Int. Clin. Psychopharmacol. 2010, 25, 241–245. [Google Scholar] [CrossRef] [PubMed]
- Rizos, E.N.; Papadopoulou, A.; Laskos, E.; Michalopoulou, P.G.; Kastania, A.; Vasilopoulos, D.; Katsafouros, K.; Lykouras, L. Reduced serum BDNF levels in patients with chronic schizophrenic disorder in relapse, who were treated with typical or atypical antipsychotics. World J. Biol. Psychiatry 2010, 11, 251–255. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.C.; Huang, T.L. Effects of antipsychotics on the serum BDNF levels in schizophrenia. Psychiatry Res. 2011, 189, 327–330. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.H.; Lange, C.; Ricken, R.; Hellweg, R.; Lang, U.E. Reduced brain-derived neurotrophic factor serum concentrations in acute schizophrenic patients increase during antipsychotic treatment. J. Clin. Psychopharmacol. 2011, 31, 334–336. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, R.; Hori, H.; Ikenouchi-Sugita, A.; Umene-Nakano, W.; Katsuki, A.; Hayashi, K.; Atake, K.; Tomita, M.; Nakamura, J. Aripiprazole altered plasma levels of brain-derived neurotrophic factor and catecholamine metabolites in first-episode untreated Japanese schizophrenia patients. Hum. Psychopharmacol. 2012, 27, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Ajami, A.; Hosseini, S.H.; Taghipour, M.; Khalilian, A. Changes in serum levels of brain derived neurotrophic factor and nerve growth factor-beta in schizophrenic patients before and after treatment. Scand. J. Immunol. 2014, 80, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Mizuno, M.; Yamada, K.; Olariu, A.; Nawa, H.; Nabeshima, T. Involvement of brain-derived neurotrophic factor in spatial memory formation and maintenance in a radial maze test in rats. J. Neurosci. 2000, 20, 7116–7121. [Google Scholar] [PubMed]
- Young, D.; Lawlor, P.A.; Leone, P.; Draqunow, M.; During, M.J. Environmental enrichment inhibits spontaneous apoptosis, prevents seizures and is neuroprotective. Nat. Med. 1999, 5, 448–453. [Google Scholar] [PubMed]
- Durany, N.; Michel, T.; Zöchling, R.; Boissl, K.W.; Cruz-Sánchez, F.F.; Riederer, P.; Thome, J. Brain-derived neurotrophic factor and neurotrophin 3 in schizophrenic psychoses. Schizophr. Res. 2001, 52, 79–86. [Google Scholar] [CrossRef]
- Weickert, C.S.; Hyde, T.M.; Lipska, B.K.; Herman, M.M.; Weinberger, D.R.; Kleinman, J.E. Reduced brain-derived neurotrophic factor in prefrontal cortex of patients with schizophrenia. Mol. Psychiatry 2003, 8, 592–610. [Google Scholar] [CrossRef] [PubMed]
- Weickert, C.S.; Ligons, D.L.; Romanczyk, T.; Ungaro, G.; Hyde, T.M.; Herman, M.M.; Weinberger, D.R.; Kleinman, J.E. Reductions in neurotrophin receptor mRNAs in the prefrontal cortex of patients with schizophrenia. Mol. Psychiatry 2005, 10, 637–650. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, T.; Bergen, S.E.; Nguyen, Q.L.; Xu, B.; Monteggia, L.M.; Pierri, J.N.; Sun, Z.; Sampson, A.R.; Lewis, D.A. Relationship of brain-derived neurotrophic factor and its receptor TrkB to altered inhibitory prefrontal circuitry in schizophrenia. J. Neurosci. 2005, 25, 372–383. [Google Scholar] [CrossRef] [PubMed]
- Grillo, R.W.; Ottoni, G.L.; Leke, R.; Souza, D.O.; Portela, L.V.; Lara, D.R. Reduced serum BDNF levels in schizophrenic patients on clozapine or typical antipsychotics. J. Psychiatr. Res. 2007, 41, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Xiu, M.H.; Hui, L.; Dang, Y.F.; Hou, T.D.; Zhang, C.X.; Zheng, Y.L.; Chen, D.C.; Kosten, T.R.; Zhang, X.Y. Decreased serum BDNF levels in chronic institutionalized schizophrenia on long-term treatment with typical and atypical antipsychotics. Prog. Neuropsychopharmacol. Biol. Psychiatry 2009, 33, 1508–1512. [Google Scholar] [CrossRef] [PubMed]
- Buckley, P.F.; Pillai, A.; Evans, D.; Stirewalt, E.; Mahadik, S. Brain derived neurotropic factor in first-episode psychosis. Schizophr. Res. 2007, 91, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Rizos, E.N.; Rontos, I.; Laskos, E.; Arsenis, G.; Michalopoulou, P.G.; Vasilopoulos, D.; Gournellis, R.; Lykouras, L. Investigation of serum BDNF levels in drug-naive patients with schizophrenia. Prog. Neuropsychopharmacol. Biol. Psychiatry 2008, 32, 1308–1311. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.C.; Wang, J.; Wang, B.; Yang, S.C.; Zhang, C.X.; Zheng, Y.L.; Li, Y.L.; Wang, N.; Yang, K.B.; Xiu, M.H.; et al. Decreased levels of serum brain-derived neurotrophic factor in drug-naive first-episode schizophrenia: Relationship to clinical phenotypes. Psychopharmacology 2009, 207, 375–380. [Google Scholar] [CrossRef] [PubMed]
- Jindal, R.D.; Pillai, A.K.; Mahadik, S.P.; Eklund, K.; Montrose, D.M.; Keshavan, M.S. Decreased BDNF in patients with antipsychotic naive first episode schizophrenia. Schizophr. Res. 2010, 119, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Gama, C.S.; Andreazza, A.C.; Kunz, M.; Berk, M.; Belmonte-de-Abreu, P.S.; Kapczinski, F. Serum levels of brain-derived neurotrophic factor in patients with schizophrenia and bipolar disorder. Neurosci. Lett. 2007, 420, 45–48. [Google Scholar] [CrossRef] [PubMed]
- Reis, H.J.; Nicolato, R.; Barbosa, I.G.; Teixeira do Prado, P.H.; Romano-Silva, M.A.; Teixeira, A.L. Increased serum levels of brain-derived neurotrophic factor in chronic institutionalized patients with schizophrenia. Neurosci. Lett. 2008, 439, 157–159. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, E.; Hashimoto, K.; Watanabe, H.; Komatsu, N.; Okamura, N.; Koike, K.; Shinoda, N.; Nakazato, M.; Kumakiri, C.; Okada, S.; et al. Serum brain-derived neurotrophic factor (BDNF) levels in schizophrenia are indistinguishable from controls. Neurosci. Lett. 2003, 351, 111–114. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.L.; Lee, C.T. Associations between serum brain-derived neurotrophic factor levels and clinical phenotypes in schizophrenia patients. J. Psychiatr. Res. 2006, 40, 664–668. [Google Scholar] [CrossRef] [PubMed]
- Karege, F.; Schwald, M.; Cisse, M. Postnatal developmental profile of brain-derived neurotrophic factor in rat brain and platelets. Neurosci. Lett. 2002, 328, 261–264. [Google Scholar] [CrossRef]
- Klein, A.B.; Williamson, R.; Santini, M.A.; Clemmensen, C.; Ettrup, A.; Rios, M.; Knudsen, G.M.; Aznar, S. Blood BDNF concentrations reflect brain-tissue BDNF levels across species. Int. J. Neuropsychopharmacol. 2011, 14, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Neeper, S.A.; Gómez-Pinilla, F.; Choi, J.; Cotman, C. Exercise and brain neurotrophins. Nature 1995, 373, 109. [Google Scholar] [CrossRef] [PubMed]
- Farmer, J.; Zhao, X.; van Praag, H.; Wodtke, K.; Gage, F.H.; Christie, B.R. Effects of voluntary exercise on synaptic plasticity and gene expression in the dentate gyrus of adult male Sprague-Dawley rats in vivo. Neuroscience 2004, 124, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Berchtold, N.C.; Chinn, G.; Chou, M.; Kesslak, J.P.; Cotman, C.W. Exercise primes a molecular memory for brain-derived neurotrophic factor protein induction in the rat hippocampus. Neuroscience 2005, 133, 853–861. [Google Scholar] [CrossRef] [PubMed]
- Duraiswamy, G.; Thirthalli, J.; Nagendra, H.R.; Gangadhar, B.N. Yoga therapy as an add-on treatment in the management of patients with schizophrenia—A randomized controlled trial. Acta Psychiatr. Scand. 2007, 116, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Behere, R.V.; Arasappa, R.; Jagannathan, A.; Varambally, S.; Venkatasubramanian, G.; Thirthalli, J.; Subbakrishna, D.K.; Nagendra, H.R.; Gangadhar, B.N. Effect of yoga therapy on facial emotion recognition deficits, symptoms and functioning in patients with schizophrenia. Acta Psychiatr. Scand. 2011, 123, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Varambally, S.; Gangadhar, B.N.; Thirthalli, J.; Jagannathan, A.; Kumar, S.; Venkatasubramanian, G.; Muralidhar, D.; Subbakrishna, D.K.; Nagendra, H.R. Therapeutic efficacy of add-on yogasana intervention in stabilized outpatient schizophrenia: Randomized controlled comparison with exercise and waitlist. Indian J. Psychiatry 2012, 54, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Chan, S.K.; Lee, E.H.; Chang, W.C.; Tse, M.; Su, W.W.; Sham, P.; Hui, C.L.; Joe, G.; Chan, C.L.; et al. Aerobic exercise and yoga improve neurocognitive function in women with early psychosis. NPJ Schizophr. 2015, 1, 15047. [Google Scholar] [CrossRef] [PubMed]
- Green, M.J.; Matheson, S.L.; Shepherd, A.; Weickert, C.S.; Carr, V.J. Brain-derived neurotrophic factor levels in schizophrenia: A systematic review with meta-analysis. Mol. Psychiatry 2011, 16, 960–972. [Google Scholar] [CrossRef] [PubMed]
- Kenny, P.J.; File, S.E.; Rattray, M. Acute nicotine decreases, and chronic nicotine increases the expression of brain-derived neurotrophic factor mRNA in rat hippocampus. Brain Res. Mol. Brain Res. 2000, 85, 234–238. [Google Scholar] [CrossRef]
- Yeom, M.; Shim, I.; Lee, H.J.; Hahm, D.H. Proteomic analysis of nicotine-associated protein expression in the striatum of repeated nicotine-treated rats. Biochem. Biophys. Res. Commun. 2005, 326, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.S.; Kim, D.J.; Lee, H.; Kim, Y.K. Increased plasma brain-derived neurotrophic factor levels in chronic smokers following unaided smoking cessation. Neurosci. Lett. 2007, 423, 53–57. [Google Scholar] [CrossRef] [PubMed]
- Umene-Nakano, W.; Yoshimura, R.; Yoshii, C.; Hoshuyama, T.; Hayashi, K.; Hori, H.; Katsuki, A.; Ikenouchi-Sugita, A.; Nakmura, J. Varenicline does not increase serum BDNF levels in patients with nicotine dependence. Hum. Psychopharmacol. 2010, 25, 276–279. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| Participants | Schizophrenia and/or related disorders, or these patients and a healthy population; No restrictions were placed on age and the diagnostic procedures | Patients with other disorders, only healthy subjects |
| Interventions | Non-pharmacological interventions (NPIs) with usual antipsychotic treatment were eligible | Only pharmacological interventions |
| Outcome | At least circulating serum or plasma levels of BDNF outcomes | Only other biomarkers |
| Study design | Only randomized controlled trials (RCTs) | |
| Publications | Published as full-text articles in peer-reviewed scientific journals | Published as reviews, case reports, conference abstracts, or letters |
| Study, Country | Intervention | Controls | Population | Mean Age (Years) | Gender (% Male) | Completion Rate (%) | Duration of Illness (Years) | CPZ Equivalent (Mean mg/day) | BMI (kg/m2) | Smoking (%) | Funding |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Kimhy et al., 2015 [32], United States | Aerobic exercise (N = 16) 12 weeks | Treatment as usual (PC) (N = 17) | SZ or related disorders DSM-IV Outpatients | I: 36.6 ± 10.4 PC: 37.2 ± 9.9 | I: 63 PC: 65 | 78.8 | ND | I: 258.9 ± 232.5 PC: 439.7 ± 362.8 | I: 31.6 ± 6.6 PC: 30.8 ± 5.5 | I: 25 PC: 23 | Government |
| Tomasik et al., 2015 [33], United States | Probiotic supplementation (N = 31), 14 weeks | Placebo supplementation (PC) (N = 27) | SZ or SZA DSM-IV Outpatients | I: 44.8 ± 11.2 PC: 48.1 ± 9.4 | I: 71 PC: 59 | 89.2 | ND | ND | ND | ND | Nonprofit organization |
| Ikai et al., 2014 [34], Japan | Hatha yoga (N = 25) 8 weeks | Daycare program (AC) (N = 25) | SZ or related psychotic disorders ICD-10 Outpatients | I: 53.5 ± 9.9 AC: 48.2 ± 12.3 | I: 64 AC: 68 | 72.0 | I: 25.3 ± 9.6 AC: 24.7 ± 11.1 | I: 659.3 ± 386.2 AC: 733.5 ± 432.5 | I: 24.6 ± 6.2 AC: 24.5 ± 3.1 | ND | ND |
| Kim et al., 2014 [35], Korea | Combined exercise (N = 24) 12 weeks | Routine activities (PC) (N = 12) | SZ DSM-IV Inpatients (more than 3 years) | I: 48.7 ± 9.9 PC: 50.7 ± 12.0 | ND | 90.0 | ND | ND | I: 25.0 ± 4.3 PC: 26.5 ± 4.7 | ND | Government |
| Miodownik et al., 2011 [36], Israel | l-theanine supplementation (N = 19) 8 weeks | Placebo supplementation (PC) (N = 21) | SZ or SZA DSM-IV Inpatients and outpatients | I: 35.4 ± 11.1 PC: 32.3 ± 10.2 | I: 90 PC: 67 | 66.6 | I: 12.0 ± 9.8 PC: 9.3 ± 7.3 | I: 500 ± 191 PC: 520 ± 296 | I: 25.4 ± 6.0 PC: 25.6 ± 2.6 | ND | Nonprofit organization |
| Vinogradov et al., 2009 [31], United States | Auditory training (N = 30) 10 weeks | Computer games (AC) (N = 26) Healthy (PC) (N = 16) | SZ DSM-IV Outpatients | I: 42.1 ± 9.4 AC: 46.0 ± 9.0 PC: 44.5 ± 11.7 | I: 73 AC: 77 PC: 62 | 100 | ND | I: 444 ± 477 AC: 515 ± 495 PC: NA | I: 29.0 ± 5.5 AC: 29.5 ± 4.5 PC: 26.9 ± 4.3 | I: 50 AC: 43 PC: 50 | Government |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanada, K.; Zorrilla, I.; Iwata, Y.; Bermúdez-Ampudia, C.; Graff-Guerrero, A.; Martínez-Cengotitabengoa, M.; González-Pinto, A. The Efficacy of Non-Pharmacological Interventions on Brain-Derived Neurotrophic Factor in Schizophrenia: A Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2016, 17, 1766. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17101766
Sanada K, Zorrilla I, Iwata Y, Bermúdez-Ampudia C, Graff-Guerrero A, Martínez-Cengotitabengoa M, González-Pinto A. The Efficacy of Non-Pharmacological Interventions on Brain-Derived Neurotrophic Factor in Schizophrenia: A Systematic Review and Meta-Analysis. International Journal of Molecular Sciences. 2016; 17(10):1766. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17101766
Chicago/Turabian StyleSanada, Kenji, Iñaki Zorrilla, Yusuke Iwata, Cristina Bermúdez-Ampudia, Ariel Graff-Guerrero, Mónica Martínez-Cengotitabengoa, and Ana González-Pinto. 2016. "The Efficacy of Non-Pharmacological Interventions on Brain-Derived Neurotrophic Factor in Schizophrenia: A Systematic Review and Meta-Analysis" International Journal of Molecular Sciences 17, no. 10: 1766. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17101766