
Atypical Antipsychotics in the Treatment of Acute Bipolar Depression with Mixed Features: A Systematic Review and Exploratory Meta-Analysis of Placebo-Controlled Clinical Trials


 ,
,  ,
,
Abstract
:1. Introduction
2. Results
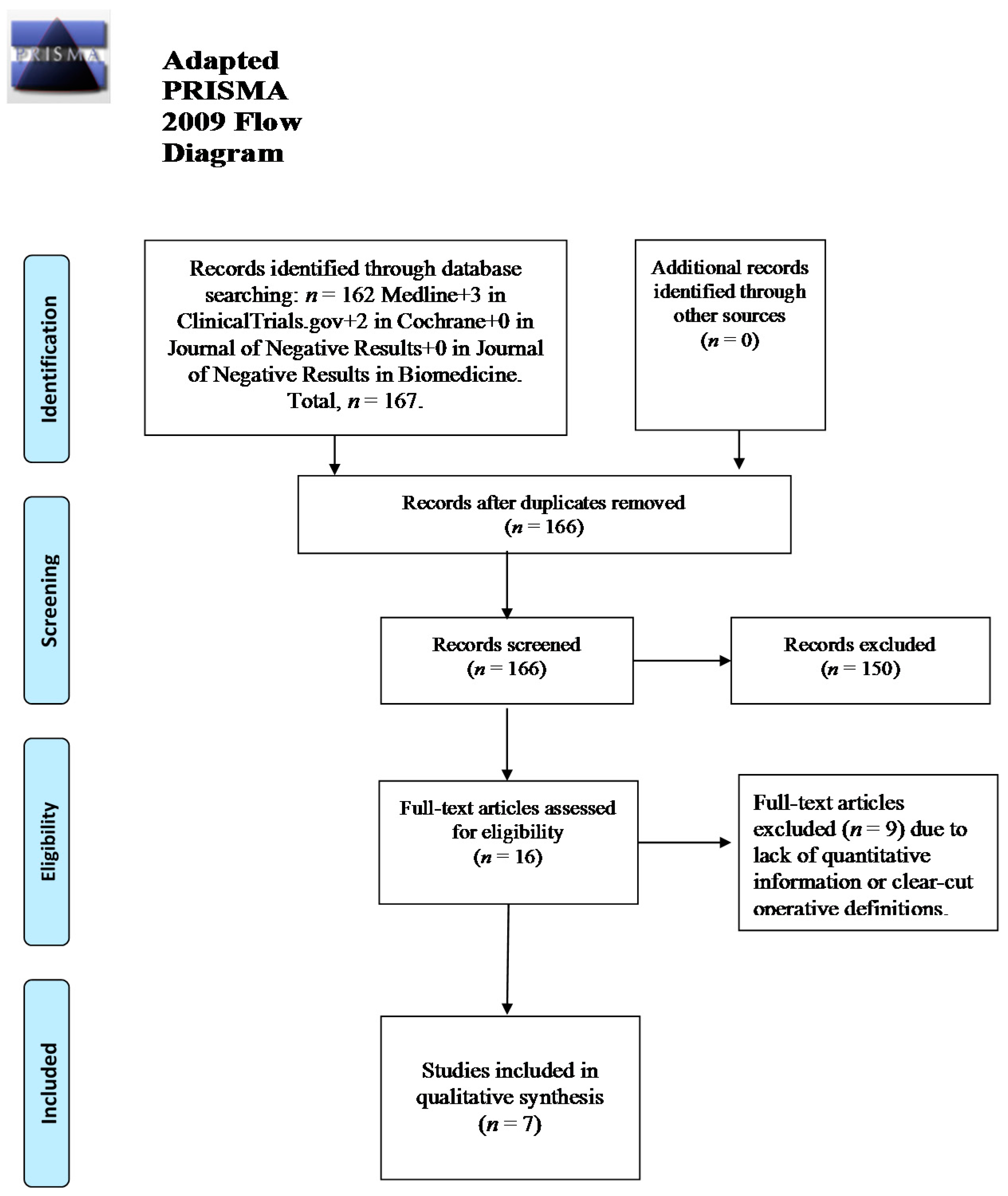
2.1. Included Studies

| Study | SGA | Mean Baseline/Study Endpoint Dose (Range) in mg | Duration of the Study | SGA Group | Placebo Group | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| MADRS Baseline | MADRS Endpoint | YMRS Baseline | YMRS Endpoint | MADRS Baseline | MADRS Endpoint | YMRS Baseline | YMRS Endpoint | ||||
| * Patkar A. et al.; 2012 [33] | Ziprasidone | 40/129.7 (80–160) | 6-week | 23.4 ± 6.5 | 12.0 ± 10.9 | 8.4 ± 6.1 | 4.7 ± 5.2 | 25.1 ± 7.9 | 19.12 ± 9.3 | 8.8 ± 6.2 | 6.5 ± 5.1 |
| & | |||||||||||
| * Pae C.U. et al., 2012 [34] | |||||||||||
| Sherwood B. et al., 2014 [30] | Quetiapine | 50/600 (50–600) | 12-week | 18.6 ± 7.0 | Undisclosed (not an outcome measure) | 13.9 ± 6.7 | Undisclosed (not an outcome measure) | 25 ± 9.2 | Undisclosed (not an outcome measure) | 13.6 ± 8.2 | Undisclosed (not an outcome measure) |
| * Tohen M. et al., 2014 [14] | Olanzapine | 5/20 (5–20) | 6-week | 31.4 ± 6.0 | 26.14 ± 4.0 | 4.61 ± 2.8 | 2.55 ± 1.8 | 30.53 ± 6.2 | 28.5 ± 4.2 | 4.94 ± 1.36 | 4.62 ± 2.5 |
| & | |||||||||||
| * Benazzi F. et al., 2009 [32] | |||||||||||
| McIntyre R.S. et al., 2015 [29] | Lurasidone | 20/20–60 (mean endpoint dose = 31.8) (20–60) | 6-week | 31.2 ± 5.2 | 15.5 ± 3.4 | 5.9 ± 2.2 | 3.5 ± 2.9 | 31.2 ± 5.3 | 20.3 ± 2.1 | 6.2 ± 2.6 | 3.9 ± 1.3 |
| & | |||||||||||
| 20/80–120 (mean endpoint dose = 82) (80–120) | |||||||||||
| Berk M. et al., 2015 [31] | Asenapine arm | 20/10-20 (10–20) | 3-week | 24.64 ± 3.73 | 13.89 ± 3.7 | 27.52 ± 4.79 | 10.94 ± 2.4 | 26.23 ± 4.86 | 21.04 ± 3.1 | 27.19 ± 4.79 | 16.92 ± 2.6 |
| Olanzapine arm | 15 (5–20) | 3-week | 25.03 ± 4.33 | 16.58 ± 3.32 | 28.36 ± 6.49 | Undisclosed | |||||

2.2. Efficacy
2.3. Meta-Analysis
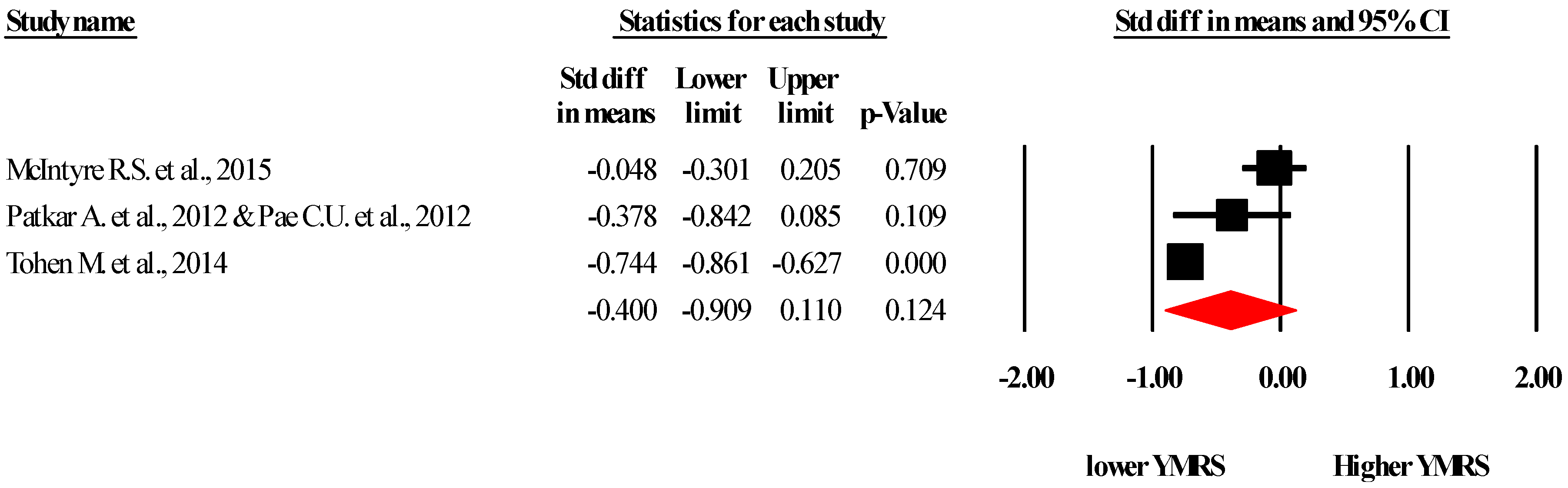
2.3.1. Young Mania Rating Scale (YMRS)

{kind=link}
{kind=link}
{kind=link}
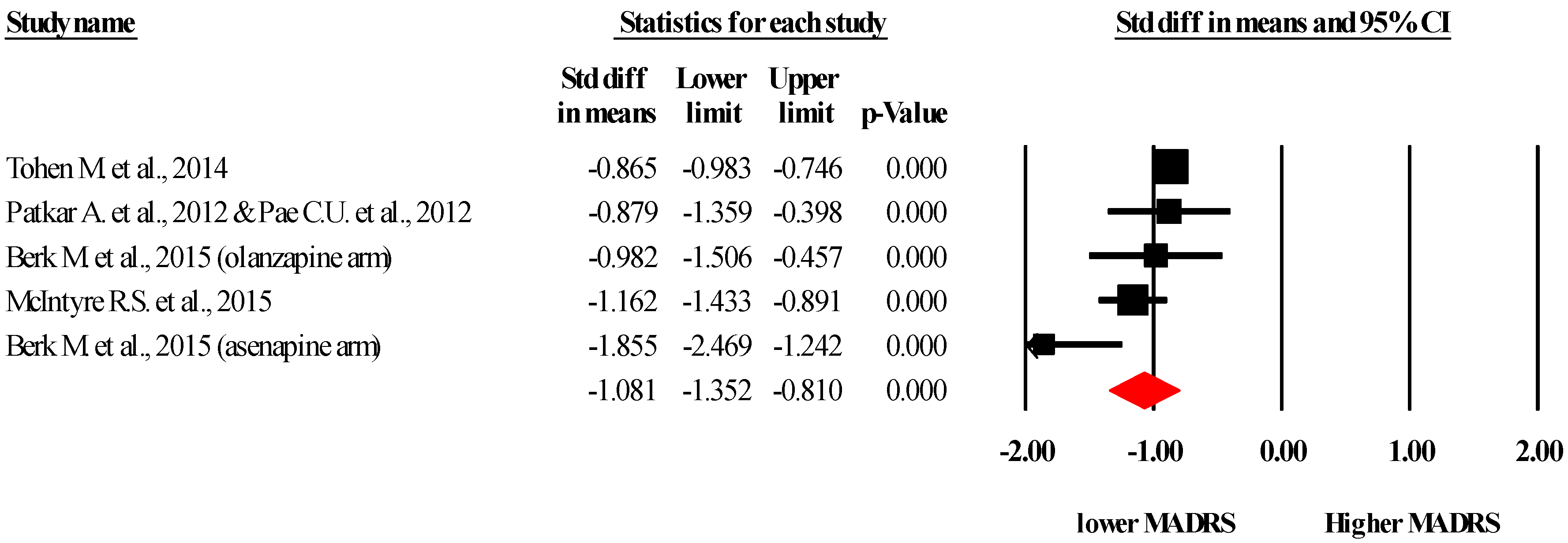
2.3.2. Montgomery–Åsberg Depression Rating Scale (MADRS)

3. Discussion
3.1. Main Results and Implication for the Clinical Practice
3.2. Limitations of the Study
4. Materials and Methods
4.1. Data Source and Methods of Search
4.2. Data Analysis
4.3. Essential Description of the Main Rating Scales and Their Scoring:
Author Contributions
Conflicts of Interest
Abbreviations
| BD | Bipolar Disorder; either Type-I (BD-I) or Type-II (BD-II) |
| CI | Confidence Interval |
| DSM | Diagnostic and Statistical Manual for Mental Disorder |
| DSM-IV | DSM, Fourth Edition |
| DSM-5 | DSM, Fifth Edition |
| HAM-D | |
| Jadad (scale) | a rating scale developed by Dr. Jadad (2007) |
| MADRS | Montgomery–Åsberg Depression Rating Scale [37] |
| MDD | Major Depressive Disorder |
| MDE | Major Depressive Episode |
| MEDLINE | Medical Literature Analysis and Retrieval System Online (U.S. National Library of Medicine’s life science database) |
| MFs | Mixed Feature(s) (of the DSM-5) |
| MOOSE | Meta-analysis Of Observational Studies in Epidemiology [guidelines] |
| MRS | Mania Rating Scale (see also “YMRS”—Authored by Young R.C. et al., 1978) [38] |
| NCO | Newcastle Ottawa Scale |
| NOS | Not Otherwise Specified (referred to the DSM-IV. Note: the DSM-5 essentially replaced “NOS” with two categories, either “other specified disorder” or “unspecified disorder”; a new category, namely “NEC”—“not elsewhere classified” was also introduced by the DSM-5 [62]) |
| O.R. | Odd ratio |
| RCT | Randomized Controlled Trial |
| S.D. | Standard Deviation |
| SGA | Second Generation Antipsychotic |
| SMD | Standardized Mean Difference |
| YMRS | Young Mania Rating Scale [38] |
References
- Hayes, J.; Prah, P.; Nazareth, I.; King, M.; Walters, K.; Petersen, I.; Osborn, D. Prescribing trends in bipolar disorder: Cohort study in the United Kingdom THIN primary care database 1995–2009. PLoS ONE 2011, 6, e28725. [Google Scholar] [CrossRef] [PubMed]
- Kendall, T. The rise and fall of the atypical antipsychotics. Br. J. Psychiatry 2011, 199, 266–268. [Google Scholar] [CrossRef] [PubMed]
- Hooshmand, F.; Miller, S.; Dore, J.; Wang, P.W.; Hill, S.J.; Portillo, N.; Ketter, T.A. Trends in pharmacotherapy in patients referred to a bipolar specialty clinic, 2000–2011. J. Affect. Disord. 2014, 155, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Medici, C.R.; Videbech, P.; Gustafsson, L.N.; Munk-Jorgensen, P. Mortality and secular trend in the incidence of bipolar disorder. J. Affect. Disord. 2015, 183, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Bauer, M.; Glenn, T.; Alda, M.; Sagduyu, K.; Marsh, W.; Grof, P.; Munoz, R.; Severus, E.; Ritter, P.; Whybrow, P.C. Drug treatment patterns in bipolar disorder: Analysis of long-term self-reported data. Int. J. Bipolar Disord. 2013, 1. [Google Scholar] [CrossRef] [PubMed]
- Carlborg, A.; Ferntoft, L.; Thuresson, M.; Bodegard, J. Population study of disease burden, management, and treatment of bipolar disorder in Sweden: A retrospective observational registry study. Bipolar Disord. 2015, 17, 76–85. [Google Scholar] [CrossRef] [PubMed]
- Stubbs, B.; Vancampfort, D.; Solmi, M.; Veronese, N.; Fornaro, M. How common is bipolar disorder in general primary care attendees? A systematic review and meta-analysis investigating prevalence determined according to structured clinical assessments. Aust. N. Z. J. Psychiatry 2016. [Google Scholar] [CrossRef] [PubMed]
- Berk, M.; Dodd, S.; Malhi, G.S. “Bipolar missed states”: The diagnosis and clinical salience of bipolar mixed states. Aust. N. Z. J. Psychiatry 2005, 39, 215–221. [Google Scholar] [PubMed]
- American Psychiatric Association (APA). Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Association: Washington, DC, USA, 1994; pp. 143–147. [Google Scholar]
- Goldberg, J.F.; Perlis, R.H.; Bowden, C.L.; Thase, M.E.; Miklowitz, D.J.; Marangell, L.B.; Calabrese, J.R.; Nierenberg, A.A.; Sachs, G.S. Manic symptoms during depressive episodes in 1380 patients with bipolar disorder: Findings from the STEP-BD. Am. J. Psychiatry 2009, 166, 173–181. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association (APA). Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- McIntyre, R.S.; Soczynska, J.K.; Cha, D.S.; Woldeyohannes, H.O.; Dale, R.S.; Alsuwaidan, M.T.; Gallaugher, L.A.; Mansur, R.B.; Muzina, D.J.; Carvalho, A.; et al. The prevalence and illness characteristics of DSM-5-defined ‘mixed feature specifier’ in adults with major depressive disorder and bipolar disorder: Results from the International Mood Disorders Collaborative Project. J. Affect. Disord. 2014, 172C, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Perugi, G.; Angst, J.; Azorin, J.M.; Bowden, C.L.; Mosolov, S.; Reis, J.; Vieta, E.; Young, A.H.; Group, B.R.-I.-M.S. Mixed features in patients with a major depressive episode: The BRIDGE-II-MIX study. J. Clin. Psychiatry 2015, 76, e351–e358. [Google Scholar] [CrossRef] [PubMed]
- Tohen, M.; Kanba, S.; McIntyre, R.S.; Fujikoshi, S.; Katagiri, H. Efficacy of olanzapine monotherapy in the treatment of bipolar depression with mixed features. J. Affect. Disord. 2014, 164, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, J.F. Mixed depression: A farewell to differential diagnosis? J. Clin. Psychiatry 2015, 76, e378–e380. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Mansur, R.; McIntyre, R.S. Mixed specifier for bipolar mania and depression: Highlights of DSM-5 changes and implications for diagnosis and treatment in primary care. Prim Care Companion CNS Disord. 2014, 16. [Google Scholar] [CrossRef] [PubMed]
- Prieto, M.L.; Ozerdem, A.; Quiroz, D.; Altinbas, K.; Aydemir, O.; Yalin, N.; Feeder, S.E.; Geske, J.R.; Frye, M.A. Exploratory factor analysis of mixed depression utilizing a modified version of Hypomania Checklist 32 (mHCL-32). Bipolar Disord. 2013, 15, 114. [Google Scholar]
- Koukopoulos, A.; Sani, G.; Ghaemi, S.N. Mixed features of depression: Why DSM-5 is wrong (and so was DSM-IV). Br. J. Psychiatry 2013, 203, 3–5. [Google Scholar] [CrossRef] [PubMed]
- Sani, G.; Vöhringer, P.A.; Napoletano, F.; Holtzman, N.S.; Dalley, S.; Girardi, P.; Ghaemi, S.N.; Koukopoulos, A. Koukopoulos’ diagnostic criteria for mixed depression: A validation study. J. Affect. Disord. 2014, 164, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Judd, L.L.; Schettler, P.J.; Akiskal, H.; Coryell, W.; Fawcett, J.; Fiedorowicz, J.G.; Solomon, D.A.; Keller, M.B. Prevalence and clinical significance of subsyndromal manic symptoms, including irritability and psychomotor agitation, during bipolar major depressive episodes. J. Affect. Disord. 2012, 138, 440–448. [Google Scholar] [CrossRef] [PubMed]
- Benazzi, F. Bipolar disorder—Focus on bipolar II disorder and mixed depression. Lancet 2007, 369, 935–945. [Google Scholar] [CrossRef]
- Benazzi, F. A tetrachoric factor analysis validation of mixed depression. Prog. Neuropsychopharmacol. Biol. Psychiatry 2008, 32, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Swann, A.C. Activated depression: Mixed bipolar disorder or agitated unipolar depression? Curr. Psychiatry Rep. 2013, 15. [Google Scholar] [CrossRef] [PubMed]
- Takeshima, M.; Oka, T. DSM-5-defined ‘mixed features’ and Benazzi’s mixed depression: Which is practically useful to discriminate bipolar disorder from unipolar depression in patients with depression? Psychiatry Clin. Neurosci. 2015, 69, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Malhi, G.S.; Fritz, K.; Allwang, C.; Burston, N.; Cocks, C.; Harper, M.; Kearney, B.; Klug, P.; Meagher, L.; Mimnagh, J.; et al. Agitation for recognition by DSM-5 mixed features specifier signals fatigue? Aust. N. Z. J. Psychiatry 2015, 49, 499–501. [Google Scholar] [CrossRef] [PubMed]
- Ghaemi, S.N. All mixed up: On the absence of diagnostic guidelines for mixed states in the ISBD Diagnostic Guidelines Task Force Report. Bipolar Disord. 2008, 10 Pt 2, 129–130. [Google Scholar] [CrossRef] [PubMed]
- Fornaro, M.; Aguglia, E.; Dell'Osso, L.; Perugi, G. Could the underestimation of bipolarity obstruct the search for novel antidepressant drugs? Expert Opin. Pharmacother. 2011, 12, 2817–2831. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, J.F.; Freeman, M.P.; Balon, R.; Citrome, L.; Thase, M.E.; Kane, J.M.; Fava, M. The American society of clinical psychopharmacology survey of psychopharmacologists’ practice patterns for the treatment of mood disorders. Depress Anxiety 2015, 32, 605–613. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, R.S.; Cucchiaro, J.; Pikalov, A.; Kroger, H.; Loebel, A. Lurasidone in the treatment of bipolar depression with mixed (subsyndromal hypomanic) features: Post hoc analysis of a randomized placebo-controlled trial. J. Clin. Psychiatry 2015, 76, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Sherwood Brown, E.; Davila, D.; Nakamura, A.; Carmody, T.J.; Rush, A.J.; Lo, A.; Holmes, T.; Adinoff, B.; Caetano, R.; Swann, A.C.; et al. A randomized, double-blind, placebo-controlled trial of quetiapine in patients with bipolar disorder, mixed or depressed phase, and alcohol dependence. Alcohol. Clin. Exp. Res. 2014, 38, 2113–2118. [Google Scholar] [CrossRef] [PubMed]
- Berk, M.; Tiller, J.W.; Zhao, J.; Yatham, L.N.; Malhi, G.S.; Weiller, E. Effects of asenapine in bipolar I patients meeting proxy criteria for moderate-to-severe mixed major depressive episodes: A post hoc analysis. J. Clin. Psychiatry 2015, 76, 728–734. [Google Scholar] [CrossRef] [PubMed]
- Benazzi, F.; Berk, M.; Frye, M.A.; Wang, W.; Barraco, A.; Tohen, M. Olanzapine/fluoxetine combination for the treatment of mixed depression in bipolar I disorder: A post hoc analysis. J. Clin. Psychiatry 2009, 70, 1424–1431. [Google Scholar] [CrossRef] [PubMed]
- Patkar, A.; Gilmer, W.; Pae, C.U.; Vohringer, P.A.; Ziffra, M.; Pirok, E.; Mulligan, M.; Filkowski, M.M.; Whitham, E.A.; Holtzman, N.S.; et al. A 6 week randomized double-blind placebo-controlled trial of ziprasidone for the acute depressive mixed state. PLoS ONE 2012, 7, e34757. [Google Scholar] [CrossRef] [PubMed]
- Pae, C.U.; Patkar, A.A.; Gilmer, W.; Holtzman, N.; Thommi, S.B.; Ghaemi, S.N. Predictors of response to ziprasidone: Results from a 6-week randomized double-blind, placebo-controlled trial for acute depressive mixed state. Pharmacopsychiatry 2012, 45, 152–155. [Google Scholar] [CrossRef] [PubMed]
- Clark, H.D.; Wells, G.A.; Huët, C.; McAlister, F.A.; Salmi, L.R.; Fergusson, D.; Laupacis, A. Assessing the quality of randomized trials: Reliability of the Jadad scale. Controll. Clin. Trials 1999, 20, 448–452. [Google Scholar] [CrossRef]
- Wells, G.; Shea, B.; O’connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2000. [Google Scholar]
- Montgomery, S.A.; Asberg, M. A new depression scale designed to be sensitive to change. Br. J. Psychiatry 1979, 134, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Young, R.; Biggs, J.; Ziegler, V.; Meyer, D. A rating scale for mania: Reliability, validity and sensitivity. Br. J. Psychiatry 1978, 133, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Dunn, R.T.; Stan, V.A.; Chriki, L.S.; Filkowski, M.M.; Ghaemi, S.N. A prospective, open-label study of Aripiprazole mono- and adjunctive treatment in acute bipolar depression. J. Affect. Disord. 2008, 110, 70–74. [Google Scholar] [CrossRef] [PubMed]
- Malhi, G.S.; Fritz, K.; Allwang, C.; Burston, N.; Cocks, C.; Devlin, J.; Harper, M.; Hoadley, B.; Kearney, B.; Klug, P. Are manic symptoms that ‘dip’ into depression the essence of mixed features? J. Affect. Disord. 2016, 192, 104–108. [Google Scholar] [CrossRef] [PubMed]
- De Berardis, D.; Marini, S.; Carano, A.; Lang, A.P.; Cavuto, M.; Piersanti, M.; Fornaro, M.; Perna, G.; Valchera, A.; Mazza, M.; et al. Efficacy and safety of long acting injectable atypical antipsychotics: A review. Curr. Clin. Pharmacol. 2013, 8, 256–264. [Google Scholar] [CrossRef] [PubMed]
- Fornaro, M.; de Berardis, D.; Iasevoli, F.; Pistorio, M.L.; D'Angelo, E.; Mungo, S.; Martino, M.; Ventriglio, A.; Cattaneo, C.I.; Favaretto, E.; et al. Corrigendum to ‘Treatment adherence towards prescribed medications in bipolar-II acute depressed patients: Relationship with cyclothymic temperament and ‘therapeutic sensation seeking’ in response towards subjective intolerance to pain’ [J. Affect. Disord. 151 (2) (November 2013), 596–604]. J. Affect. Disord. 2014, 170C. [Google Scholar] [CrossRef]
- Fornaro, M.; De Berardis, D.; Koshy, A.N.; Perna, G.; Valchera, A.; Vancampfort, D.; Stubbs, B. Prevalence and clinical features associated with bipolar disorder polypharmacy: A systematic review. Neuropsychiatr. Dis. Treat. 2016, in press. [Google Scholar]
- Perugi, G.; Fornaro, M. Bipolar disorder treatment guidelines and their limits in every day clinical practice. G. Ital. Psicopatol. 2011, 17, 261–264. [Google Scholar]
- Fornaro, M.; Giosuè, P. Current nosology of treatment resistant depression: A controversy resistant to revision. Clin. Pract. Epidemiol. Ment. Health 2010, 6, 20–24. [Google Scholar] [CrossRef] [PubMed]
- Marneros, A.; Goodwin, F. Bipolar Disorders: Mixed States, Rapid Cycling and Atypical Forms; Cambridge University Press: Cambridge, UK, 2005. [Google Scholar]
- Maj, M. “Mixed” depression: Drawbacks of DSM-5 (and other) polythetic diagnostic criteria. J. Clin. Psychiatry 2015, 76, e381–e382. [Google Scholar] [CrossRef] [PubMed]
- Koukopoulos, A.; Sani, G. DSM-5 criteria for depression with mixed features: A farewell to mixed depression. Acta Psychiatr. Scand. 2014, 129, 4–16. [Google Scholar] [CrossRef] [PubMed]
- Suppes, T.; Silva, R.; Cucchiaro, J.; Mao, Y.; Targum, S.; Streicher, C.; Pikalov, A.; Loebel, A. Lurasidone for the Treatment of Major Depressive Disorder With Mixed Features: A Randomized, Double-Blind, Placebo-Controlled Study. Am. J. Psychiatry 2015. [Google Scholar] [CrossRef] [PubMed]
- Fornaro, M.; Martino, M.; De Pasquale, C.; Moussaoui, D. The argument of antidepressant drugs in the treatment of bipolar depression: Mixed evidence or mixed states? Expert Opin. Pharmacother. 2012, 13, 2037–2051. [Google Scholar] [CrossRef] [PubMed]
- Roberts, R.J.; Lohano, K.K.; El-Mallakh, R.S. Antipsychotics as antidepressants. Asia Pac. Psychiatry 2015. [Google Scholar] [CrossRef] [PubMed]
- Davey, J.; Turner, R.M.; Clarke, M.J.; Higgins, J.P. Characteristics of meta-analyses and their component studies in the Cochrane Database of Systematic Reviews: A cross-sectional, descriptive analysis. BMC Med. Res. Methodol. 2011, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kicinski, M.; Springate, D.A.; Kontopantelis, E. Publication bias in meta-analyses from the Cochrane Database of Systematic Reviews. Stat. Med. 2015, 34, 2781–2793. [Google Scholar] [CrossRef] [PubMed]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Qi, X.; Yang, M.; Ren, W.; Jia, J.; Wang, J.; Han, G.; Fan, D. Find duplicates among the PubMed, EMBASE, and Cochrane Library Databases in systematic review. PLoS ONE 2013, 8, e71838. [Google Scholar]
- Reuters, T. Endnote X7; Thomson Reuters: Philadelphia, PA, USA, 2013. [Google Scholar]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Carmody, T.J.; Rush, A.J.; Bernstein, I.; Warden, D.; Brannan, S.; Burnham, D.; Woo, A.; Trivedi, M.H. The Montgomery Asberg and the Hamilton ratings of depression: A comparison of measures. Eur. Neuropsychopharmacol. 2006, 16, 601–611. [Google Scholar] [CrossRef] [PubMed]
- Borenstein, M.; Hedges, L.; Higgins, J.; Rothstein, H. Comprehensive Meta-Analysis Version 3; Biostat: Englewood, NJ, USA, 2005; p. 104. [Google Scholar]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, S.; Tweedie, R. A Non-Parametric ‘Trim and Fill’ Method of Assessing Publication Bias in Meta-Analysis; University of Colorado Health Sciences Center: Denver, FL, USA, 1998. [Google Scholar]
- Roth, L.S. The DSM-V: Simplify, clarify. Psychiatry 2005, 2, 12–13. [Google Scholar] [PubMed]
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fornaro, M.; Stubbs, B.; De Berardis, D.; Perna, G.; Valchera, A.; Veronese, N.; Solmi, M.; Ganança, L. Atypical Antipsychotics in the Treatment of Acute Bipolar Depression with Mixed Features: A Systematic Review and Exploratory Meta-Analysis of Placebo-Controlled Clinical Trials. Int. J. Mol. Sci. 2016, 17, 241. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17020241
Fornaro M, Stubbs B, De Berardis D, Perna G, Valchera A, Veronese N, Solmi M, Ganança L. Atypical Antipsychotics in the Treatment of Acute Bipolar Depression with Mixed Features: A Systematic Review and Exploratory Meta-Analysis of Placebo-Controlled Clinical Trials. International Journal of Molecular Sciences. 2016; 17(2):241. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17020241
Chicago/Turabian StyleFornaro, Michele, Brendon Stubbs, Domenico De Berardis, Giampaolo Perna, Alessandro Valchera, Nicola Veronese, Marco Solmi, and Licínia Ganança. 2016. "Atypical Antipsychotics in the Treatment of Acute Bipolar Depression with Mixed Features: A Systematic Review and Exploratory Meta-Analysis of Placebo-Controlled Clinical Trials" International Journal of Molecular Sciences 17, no. 2: 241. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17020241