
Platelet-Rich Plasma-Loaded Poly(d,l-lactide)-Poly(ethylene glycol)-Poly(d,l-lactide) Hydrogel Dressing Promotes Full-Thickness Skin Wound Healing in a Rodent Model


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
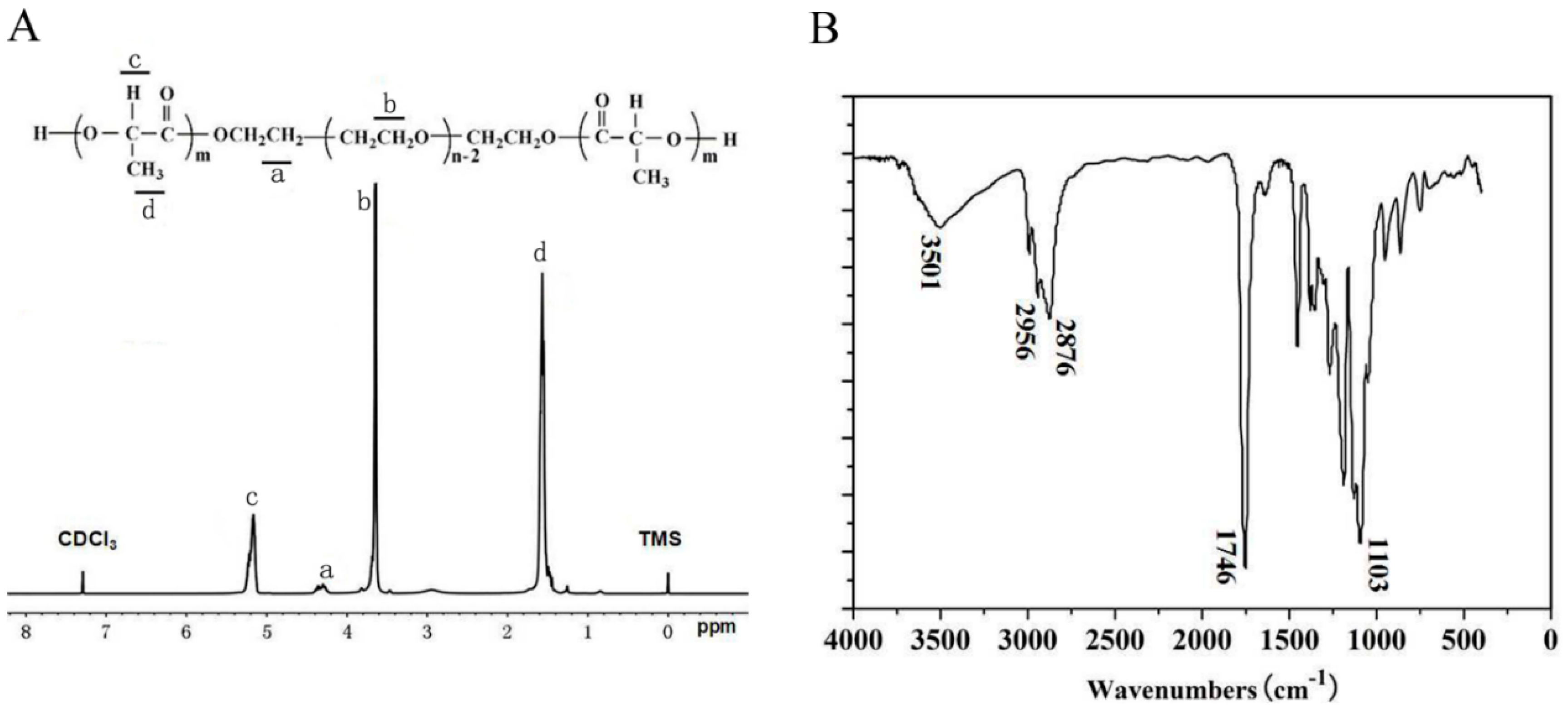
2.1. Characterization of Poly(d,l-lactide)-Poly(ethylene glycol)-Poly(d,l-lactide) (PLEL) Triblock Copolymers
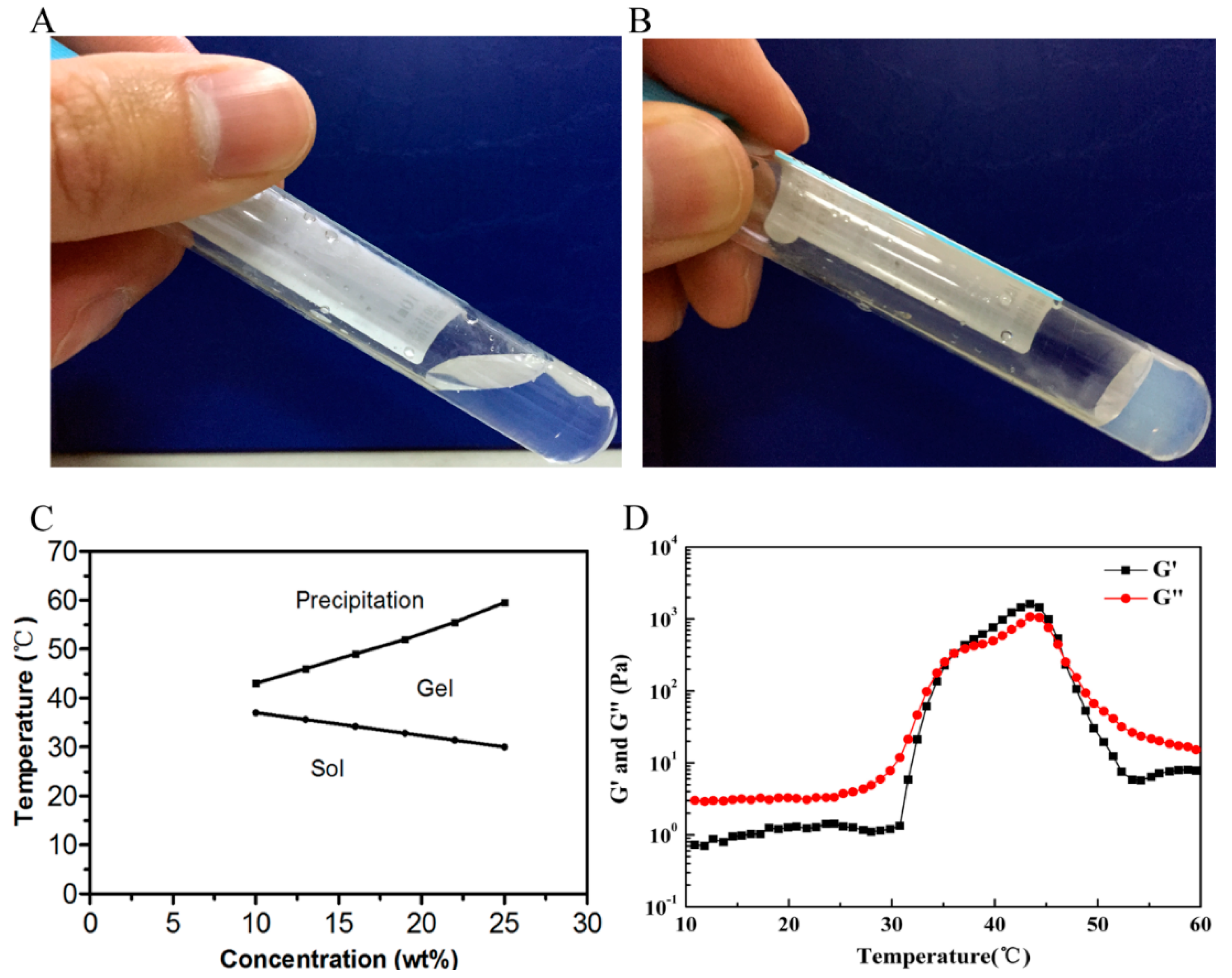
2.2. Temperature-Dependent Sol–Gel-Precipitation Transition Behavior of PLEL Hydrogel
2.3. Cytotoxicity Evaluation of PLEL Hydrogel and Its Extract
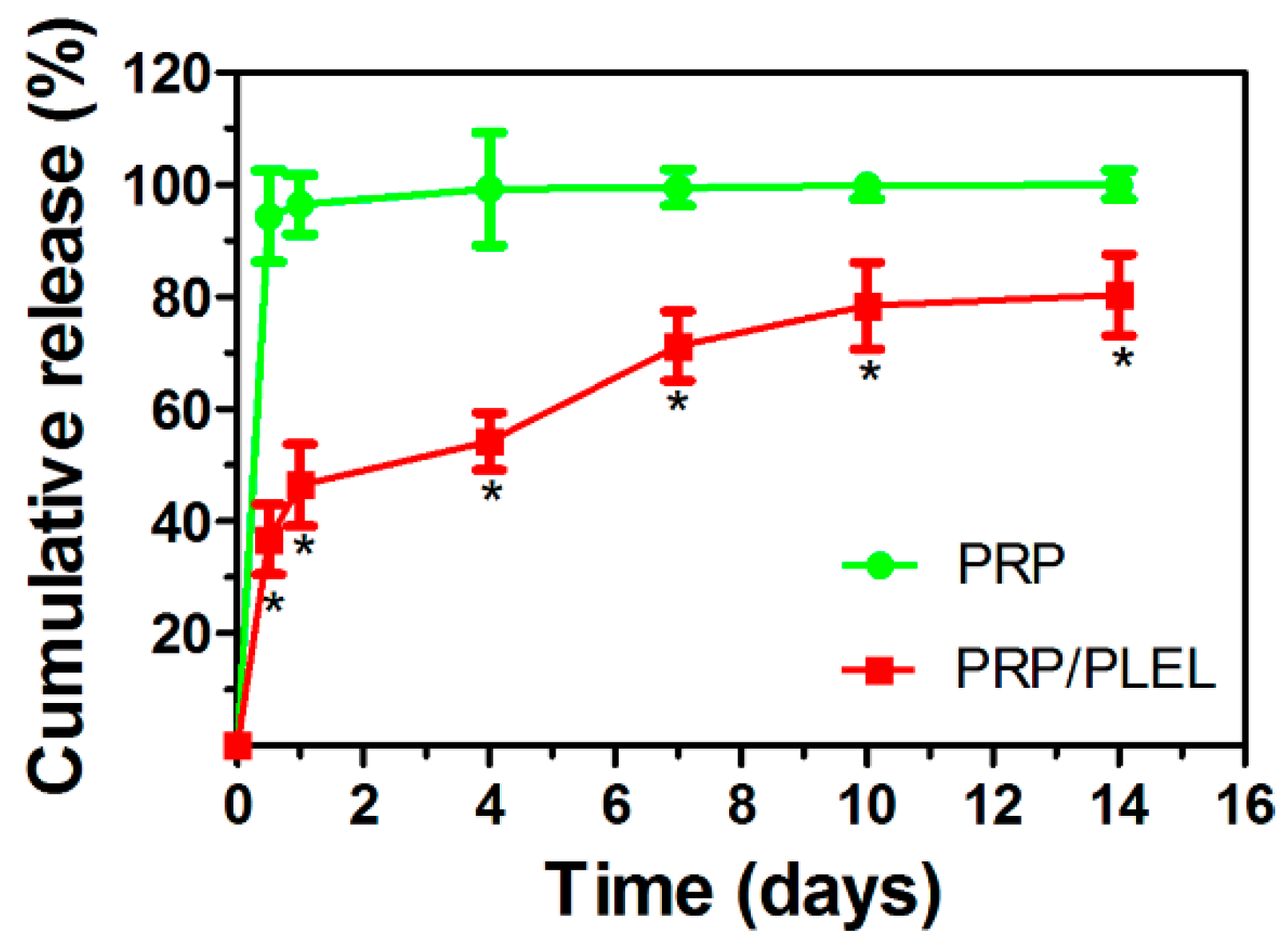
2.4. Release Kinetics of Platelet-Derived Growth Factor (PDGF)-BB from Platelet-Rich Plasma (PRP) with and without Delivery Vehicle
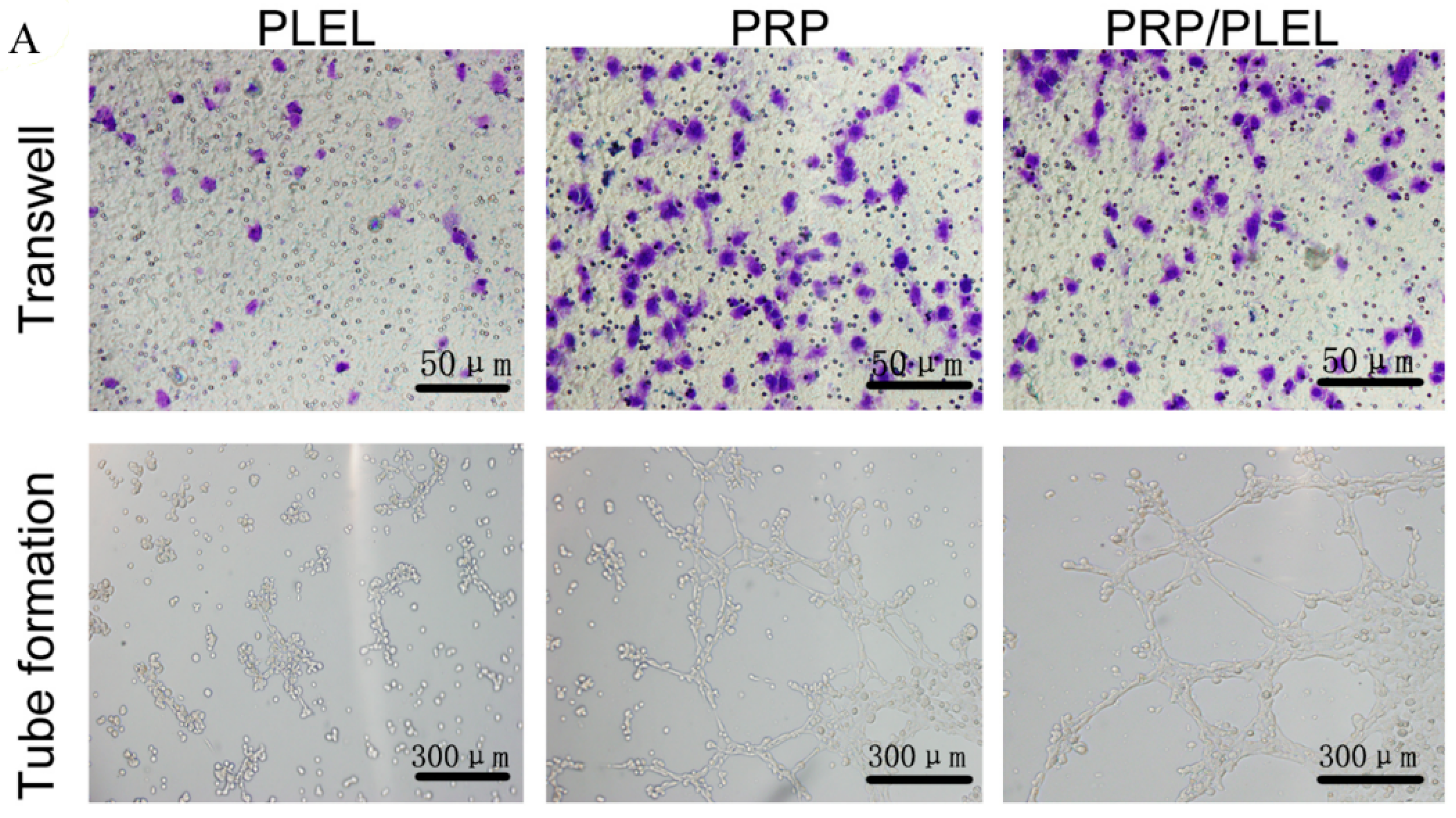
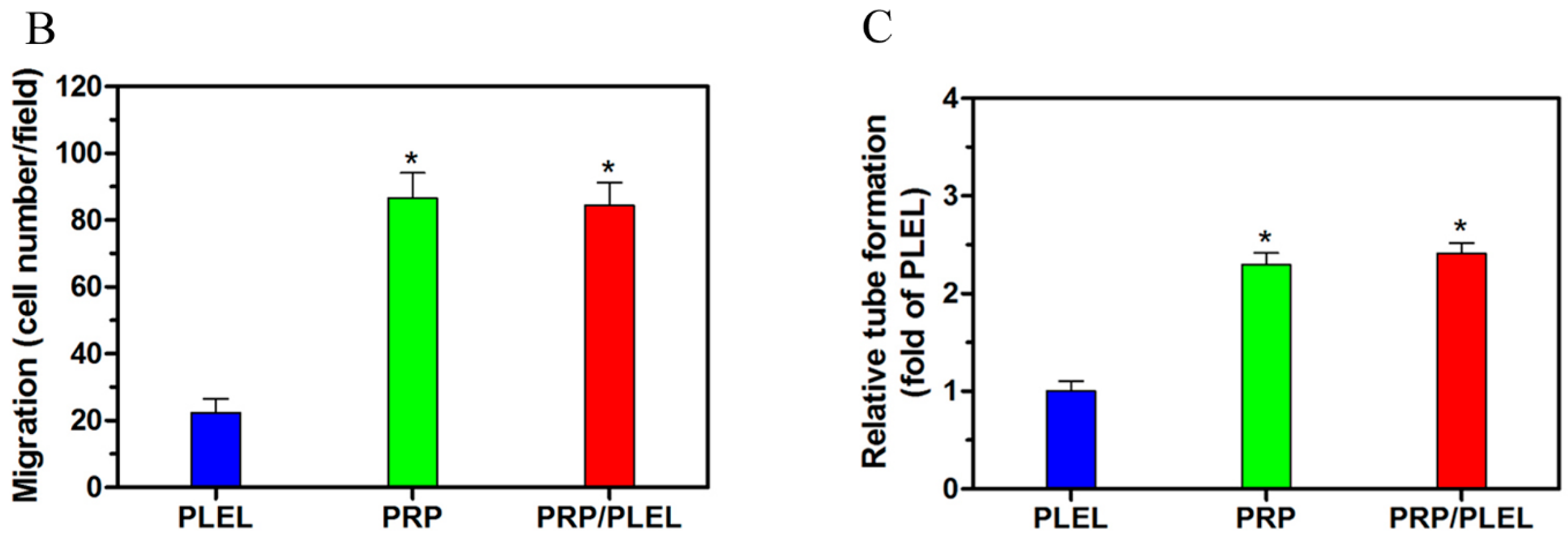
2.5. Platelet-Rich Plasma (PRP)/PLEL Promotes Migration and Tube Formation of EaHy926
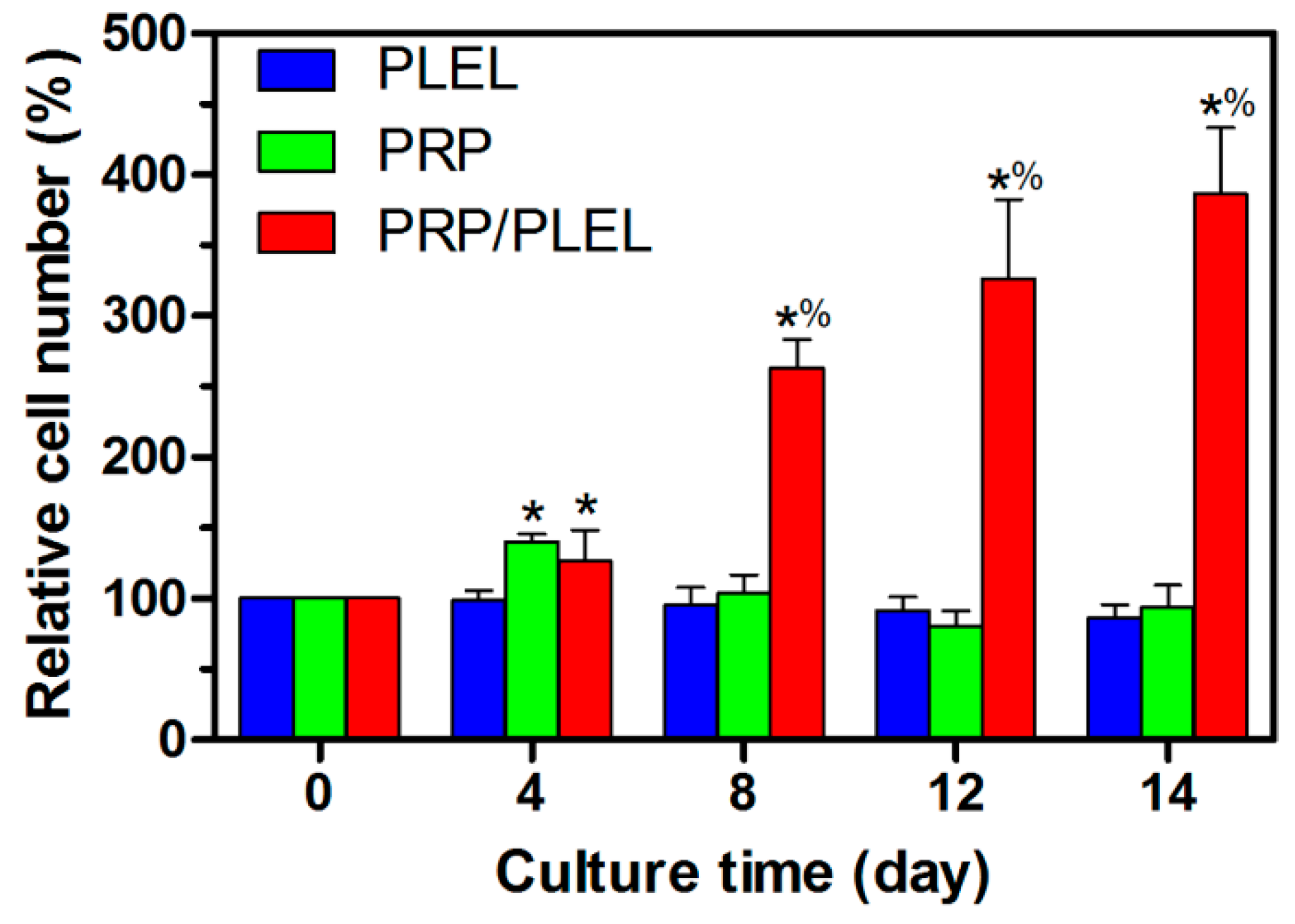
2.6. Bioactivity of Growth Factors (GFs) Released from PRP and PRP/PLEL
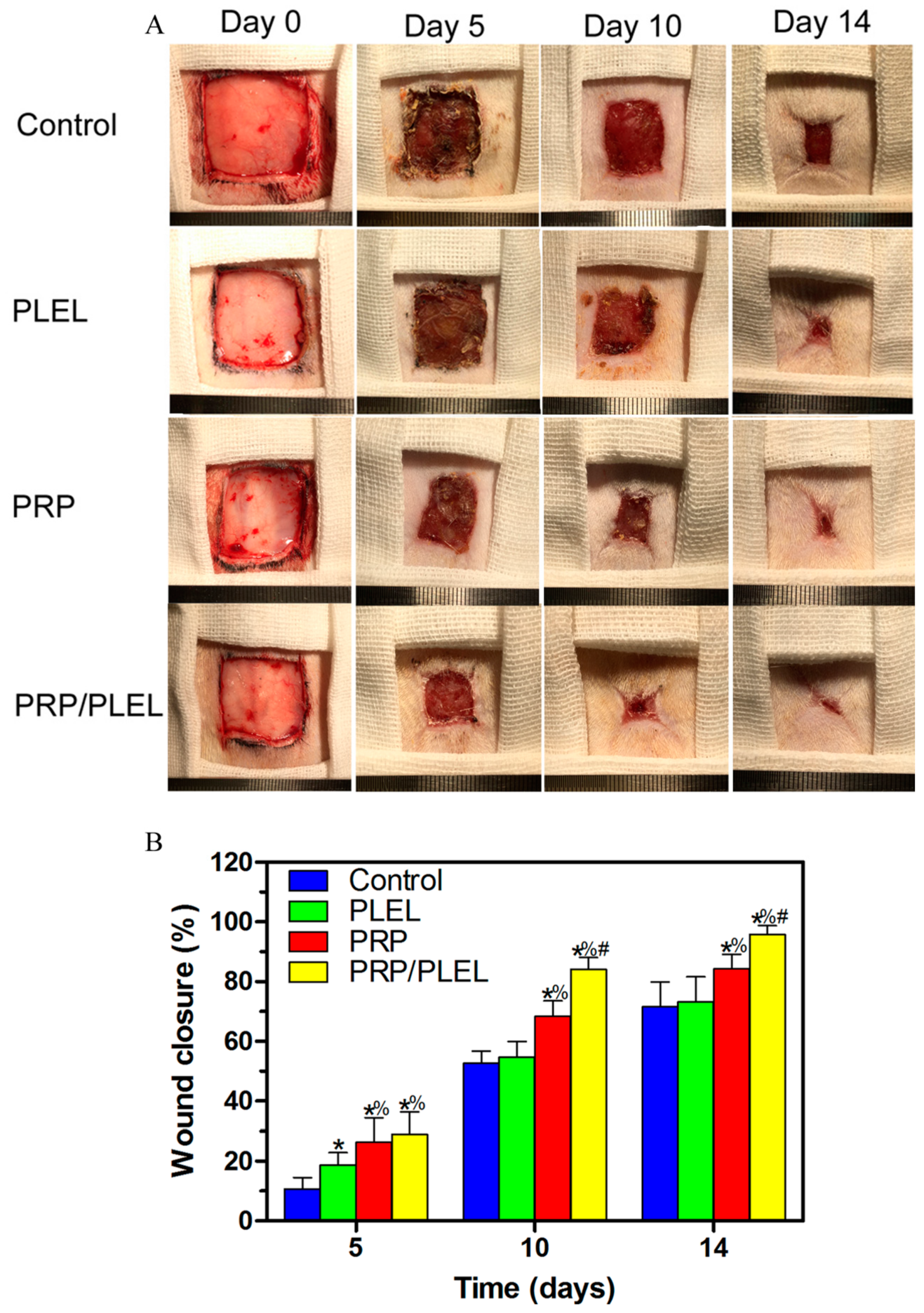
2.7. Gross Observation of Skin Wounds and Wound Closure Calculation
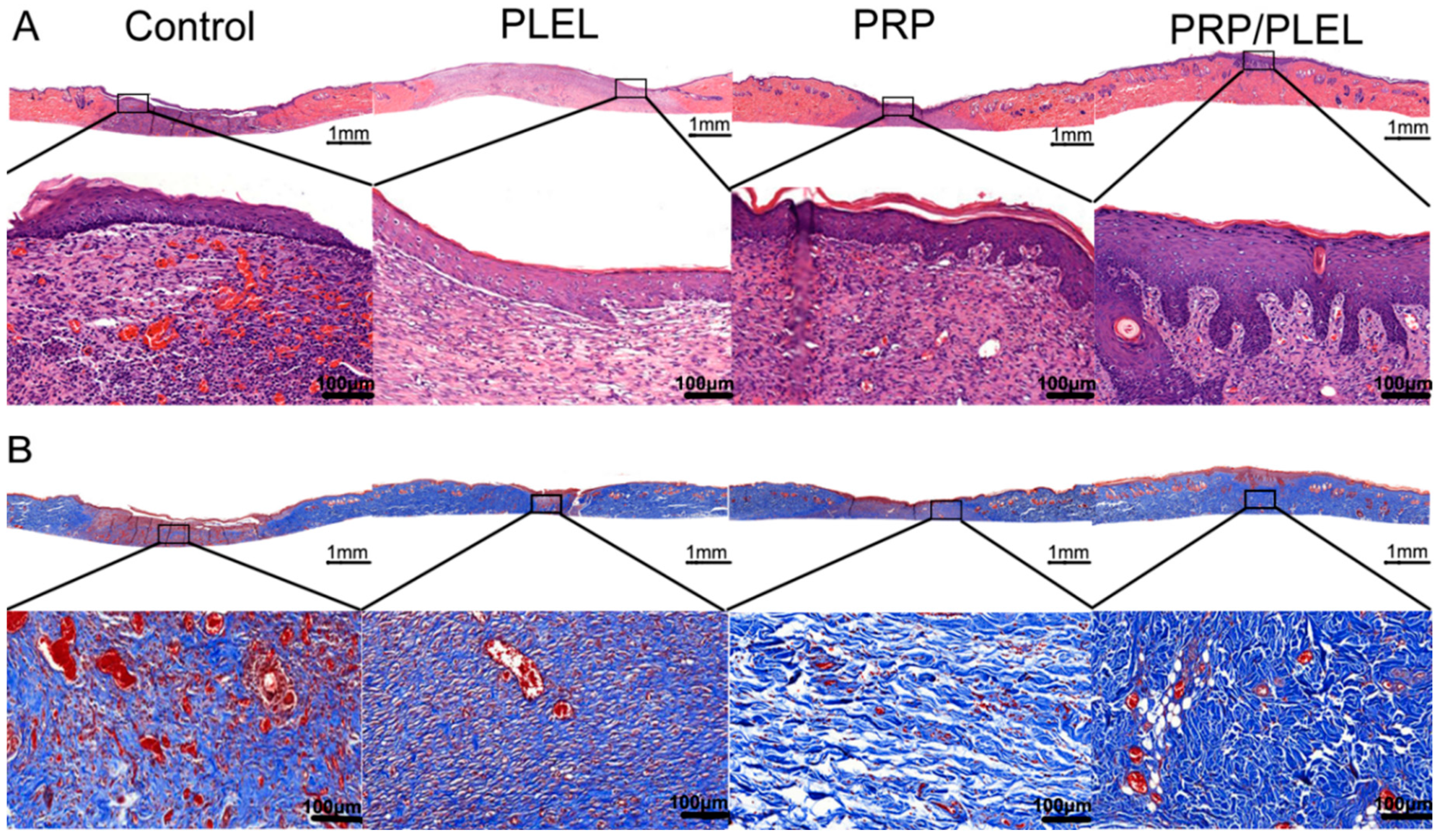
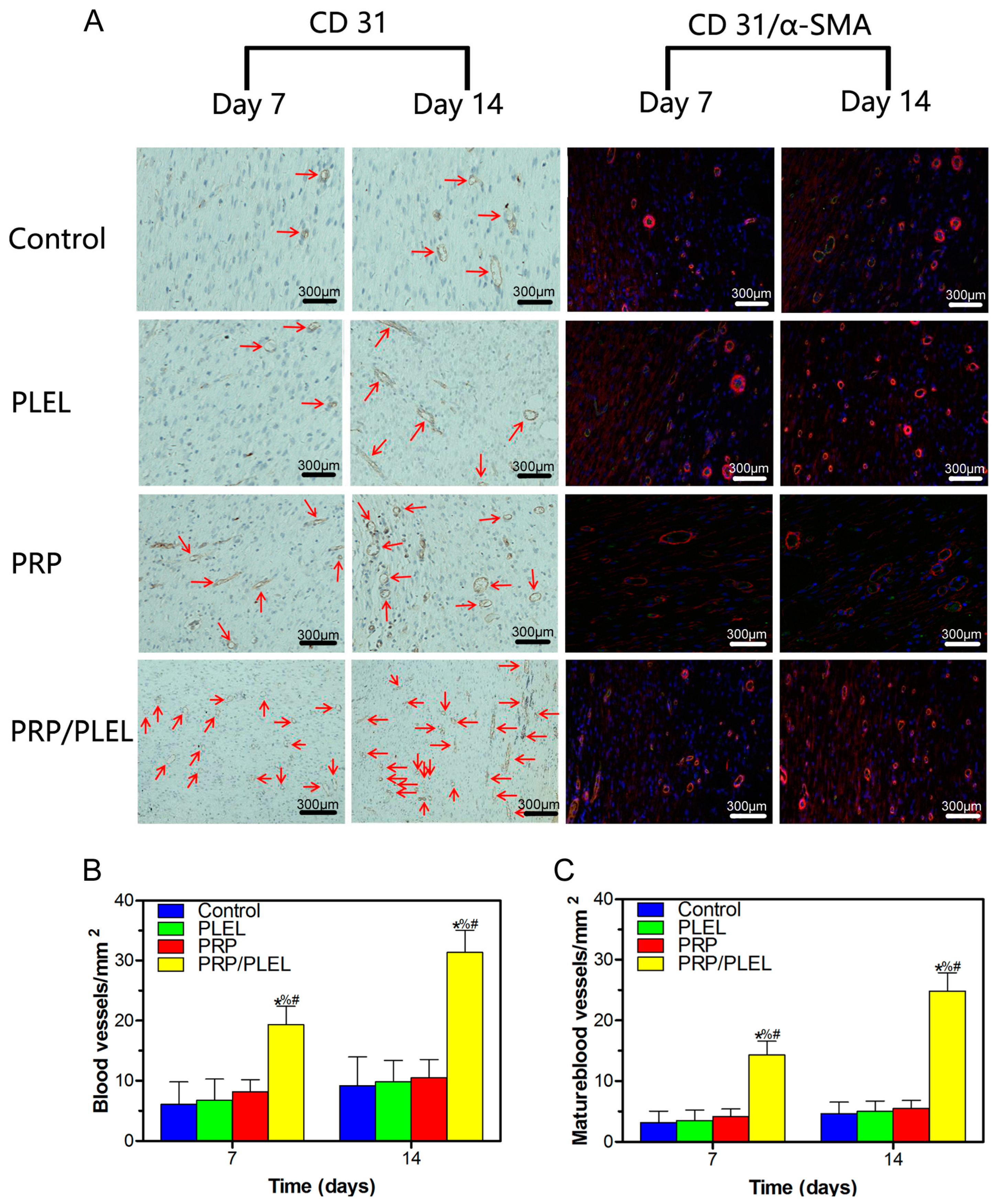
2.8. Histologic, Immunohistochemical and Immunofluorescent Evalution
3. Discussion
4. Materials and Methods
4.1. Materials
4.2. Synthesis, Characterization of PLEL Triblock Copolymers
4.3. Sol–Gel–Precipitation Phase Transition Behavior Study of PLEL Hydrogel
4.4. In Vitro Cytotoxicity Tests
4.5. PRP and PRP/PLEL Composite Preparation
4.6. Release Kinetics of PDGF-BB from PRP and PRP/PLEL
4.7. EaHy926 Migration and Tube-Formation Assays
4.8. Cell Proliferation Analysis
4.9. Skin Wound Treatment
4.10. Wound Analysis
4.11. Assessment of Reepithelialization, Collagen Deposition and Angiogenesis
4.12. Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Balasubramani, M.; Kumar, T.R.; Babu, M. Skin substitutes: A review. Burns 2001, 27, 534–544. [Google Scholar] [CrossRef]
- Singer, A.J.; Clark, R.A. Cutaneous wound healing. N. Engl. J. Med. 1999, 341, 738–746. [Google Scholar] [PubMed]
- Hrabchak, C.; Flynn, L.; Woodhouse, K.A. Biological skin substitutes for wound cover and closure. Expert Rev. Med. Devices 2006, 3, 373–385. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Gao, C.; Mao, Z.; Zhou, J.; Shen, J.; Hu, X.; Han, C. Collagen/chitosan porous scaffolds with improved biostability for skin tissue engineering. Biomaterials 2003, 24, 4833–4841. [Google Scholar] [CrossRef]
- Metcalfe, A.D.; Ferguson, M.W. Bioengineering skin using mechanisms of regeneration and repair. Biomaterials 2007, 28, 5100–5113. [Google Scholar] [CrossRef] [PubMed]
- Barrientos, S.; Stojadinovic, O.; Golinko, M.S.; Brem, H.; Tomic-Canic, M. Growth factors and cytokines in wound healing. Wound Repair Regen. 2008, 16, 585–601. [Google Scholar] [CrossRef] [PubMed]
- Khoshbin, A.; Leroux, T.; Wasserstein, D.; Marks, P.; Theodoropoulos, J.; Ogilvie-Harris, D.; Chahal, J. The efficacy of platelet-rich plasma in the treatment of symptomatic knee osteoarthritis: A systematic review with quantitative synthesis. Arthroscopy 2013, 29, 2037–2048. [Google Scholar] [CrossRef] [PubMed]
- Ishida, K.; Kuroda, R.; Miwa, M.; Tabata, Y.; Hokugo, A.; Kawamoto, T.; Kurosaka, M. The regenerative effects of platelet-rich plasma on meniscal cells in vitro and its in vivo application with biodegradable gelatin hydrogel. Tissue Eng. 2007, 13, 1103–1112. [Google Scholar] [CrossRef] [PubMed]
- Hee, H.T.; Majd, M.E.; Holt, R.T.; Myers, L. Do autologous growth factors enhance transforaminal lumbar interbody fusion? Eur. Spine J. 2003, 12, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Stellos, K.; Gawaz, M. Platelet interaction with progenitor cells: Potential implications for regenerative medicine. Thromb. Haemost. 2007, 98, 922. [Google Scholar] [CrossRef] [PubMed]
- Bennett, N.T.; Schultz, G.S. Growth factors and wound healing: Part II. Role in normal and chronic wound healing. Am. J. Surg. 1993, 166, 74–81. [Google Scholar] [CrossRef]
- Slater, M.; Patava, J.; Kingham, K.; Mason, R.S. Involvement of platelets in stimulating osteogenic activity. J. Orthop. Res. 1995, 13, 655–663. [Google Scholar] [CrossRef] [PubMed]
- Thawani, J.P.; Wang, A.C.; Than, K.D.; Lin, C.Y.; La Marca, F.; Park, P. Bone morphogenetic proteins and cancer: Review of the literature. Neurosurgery 2010, 66, 233–246. [Google Scholar] [CrossRef] [PubMed]
- Bir, S.C.; Esaki, J.; Marui, A.; Yamahara, K.; Tsubota, H.; Ikeda, T.; Sakata, R. Angiogenic properties of sustained release platelet-rich plasma: characterization in vitro and in the ischemic hind limb of the mouse. J. Vasc. Surg. 2009, 50, 870–879. [Google Scholar] [CrossRef] [PubMed]
- La, W.G.; Yang, H.S. Heparin-conjugated poly (lactic-co-glycolic acid) nanospheres enhance large-wound healing by delivering growth factors in platelet-rich plasma. Artif. Organs. 2015, 39, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Gong, C.Y.; Shi, S.; Dong, P.W.; Yang, B.; Qi, X.R.; Guo, G.; Qian, Z.Y. Biodegradable in situ gel-forming controlled drug delivery system based on thermosensitive PCL–PEG–PCL hydrogel: Part 1—synthesis, characterization, and acute toxicity evaluation. J. Pharm. Sci. 2009, 98, 4684–4694. [Google Scholar] [CrossRef] [PubMed]
- Peppas, N.A.; Bures, P.; Leobandung, W.; Ichikawa, H. Hydrogels in pharmaceutical formulations. Eur. J. Pharm. Biopharm. 2000, 50, 27–46. [Google Scholar] [CrossRef]
- Boateng, J.; Catanzano, O. Advanced therapeutic dressings for effective wound healing—A review. J. Pharm. Sci. 2015, 104, 3653–3680. [Google Scholar] [CrossRef] [PubMed]
- Coviello, T.; Matricardi, P.; Marianecci, C.; Alhaique, F. Polysaccharide hydrogels for modified release formulations. J. Control. Release 2007, 119, 5–24. [Google Scholar] [CrossRef] [PubMed]
- Shi, K.; Wang, Y.L.; Qu, Y.; Liao, J.F.; Chu, B.Y.; Zhang, H.P.; Qian, Z.Y. Synthesis, characterization, and application of reversible PDLLA-PEG-PDLLA copolymer thermogels in vitro and in vivo. Sci. Rep. 2016, 6, 19077. [Google Scholar] [CrossRef] [PubMed]
- Zentner, G.M.; Rathi, R.; Shih, C.; McRea, J.C.; Seo, M.H.; Oh, H.; Weitman, S. Biodegradable block copolymers for delivery of proteins and water-insoluble drugs. J. Control. Release 2001, 72, 203–215. [Google Scholar] [CrossRef]
- Li, X.; Yi, W.; Jin, A.; Duan, Y.; Min, S. Effects of sequentially released BMP-2 and BMP-7 from PELA microcapsule-based scaffolds on the bone regeneration. Am. J. Transl. Res. 2015, 7, 1417. [Google Scholar] [PubMed]
- Li, X.; Min, S.; Zhao, X.; Lu, Z.; Jin, A. Optimization of entrapping conditions to improve the release of BMP-2 from PELA carriers by response surface methodology. Biomed. Mater. 2015, 10, 015002. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.; Zhang, H.; Ding, J. Effects of precipitate agents on temperature-responsive sol–gel transitions of PLGA–PEG–PLGA copolymers in water. Colloid Polym. Sci. 2010, 288, 1151–1159. [Google Scholar] [CrossRef]
- Gao, N.; Chen, Z.; Xiao, X.; Ruan, C.; Mei, L.; Liu, Z.; Zeng, X. Surface modification of paclitaxel-loaded tri-block copolymer PLGA-b-PEG-b-PLGA nanoparticles with protamine for liver cancer therapy. J. Nanopart. Res. 2015, 17, 1–11. [Google Scholar] [CrossRef]
- Li, Y.; Qi, X.R.; Maitani, Y.; Nagai, T. PEG–PLA diblock copolymer micelle-like nanoparticles as all-trans-retinoic acid carrier: In vitro and in vivo characterizations. Nanotechnology 2009, 20, 055106. [Google Scholar] [CrossRef] [PubMed]
- Hwang, M.J.; Suh, J.M.; Bae, Y.H.; Kim, S.W.; Jeong, B. Caprolactonic poloxamer analog: PEG-PCL-PEG. Biomacromolecules 2005, 6, 885–890. [Google Scholar] [CrossRef] [PubMed]
- Bae, S.J.; Suh, J.M.; Sohn, Y.S.; Bae, Y.H.; Kim, S.W.; Jeong, B. Thermogelling poly (caprolactone-b-ethylene glycol-b-caprolactone) aqueous solutions. Macromolecules 2005, 38, 5260–5265. [Google Scholar] [CrossRef]
- Choi, S.W.; Choi, S.Y.; Jeong, B.; Kim, S.W.; Lee, D.S. Thermoreversible gelation of poly (ethylene oxide) biodegradable polyester block copolymers. II. J. Polym. Sci. A 1999, 37, 2207–2218. [Google Scholar] [CrossRef]
- Marx, R.E. Platelet-rich plasma: Evidence to support its use. J. Oral Maxillofac. Surg. 2004, 62, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Hardwicke, J.T.; Hart, J.; Bell, A.; Duncan, R.; Thomas, D.W.; Moseley, R. The effect of dextrin–rhEGF on the healing of full-thickness, excisional wounds in the (db/db) diabetic mouse. J. Control. Release 2011, 152, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Sebastian, A.; Syed, F.; Perry, D.; Balamurugan, V.; Colthurst, J.; Chaudhry, I.H.; Bayat, A. Acceleration of cutaneous healing by electrical stimulation: Degenerate electrical waveform down-regulates inflammation, up-regulates angiogenesis and advances remodeling in temporal punch biopsies in a human volunteer study. Wound Repair Regen. 2011, 19, 693–708. [Google Scholar] [CrossRef] [PubMed]
- Matsui, M.; Tabata, Y. Enhanced angiogenesis by multiple release of platelet-rich plasma contents and basic fibroblast growth factor from gelatin hydrogels. Acta Biomater. 2012, 8, 1792–1801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, S.; Li, L.; Wang, H.; Zhang, Y.; Cheng, X.; Zhou, N.; Zhang, C. Wound dressings composed of copper-doped borate bioactive glass microfibers stimulate angiogenesis and heal full-thickness skin defects in a rodent model. Biomaterials 2015, 53, 379–391. [Google Scholar] [CrossRef] [PubMed]
- Valarmathi, M.T.; Davis, J.M.; Yost, M.J.; Goodwin, R.L.; Potts, J.D. A three-dimensional model of vasculogenesis. Biomaterials 2009, 30, 1098–1112. [Google Scholar] [CrossRef] [PubMed]
- Winter, G.D. Formation of the scab and the rate of epithelisation of superficial wounds in the skin of the young domestic pig. 1962. J. Wound Care 1995, 4, 366. [Google Scholar] [PubMed]
- Hajimiri, M.; Shahverdi, S.; Esfandiari, M.A.; Larijani, B.; Atyabi, F.; Rajabiani, A.; Dinarvand, R. Preparation of hydrogel embedded polymer-growth factor conjugated nanoparticles as a diabetic wound dressing. Drug Dev. Ind. Pharm. 2015. [Google Scholar] [CrossRef] [PubMed]
- Nagashima, M.; Yoshino, S.; Ishiwata, T.; Asano, G. Role of vascular endothelial growth factor in angiogenesis of rheumatoid arthritis. J. Rheumatol. 1995, 22, 1624–1630. [Google Scholar] [PubMed]
- Huang, C.; Orbay, H.; Tobita, M.; Miyamoto, M.; Tabata, Y.; Hyakusoku, H.; Mizuno, H. Proapoptotic effect of control-released basic fibroblast growth factor on skin wound healing in a diabetic mouse model. Wound Repair Regen. 2015. [Google Scholar] [CrossRef] [PubMed]
- Deng, X.M.; Xiong, C.D.; Cheng, L.M.; Xu, R.P. Synthesis and characterization of block copolymers from d,l-lactide and poly (ethylene glycol) with stannous chloride. J. Polym. Sci. C 1990, 28, 411–416. [Google Scholar] [CrossRef]
- Wu, Q.; Gong, C.; Shi, S.; Wang, Y.; Huang, M.; Yang, L.; Qian, Z. Mannan loaded biodegradable and injectable thermosensitive PCL–PEG–PCL hydrogel for vaccine delivery. Soft Mater. 2012, 10, 472–486. [Google Scholar] [CrossRef]
- Dhurat, R.; Sukesh, M.S. Principles and methods of preparation of platelet-rich plasma: A review and author’s perspective. J. Cutan. Aesthet. Surg. 2014, 7, 189. [Google Scholar] [CrossRef] [PubMed]
- Fu, Y.; Guan, J.; Guo, S.; Guo, F.; Niu, X.; Liu, Q.; Wang, Y. Human urine-derived stem cells in combination with polycaprolactone/gelatin nanofibrous membranes enhance wound healing by promoting angiogenesis. J. Transl. Med. 2014, 12, 274. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, Y.; Ishikawa, H.; Kawai, K.; Tabata, Y.; Suzuki, S. Enhanced wound healing by topical administration of mesenchymal stem cells transfected with stromal cell-derived factor-1. Biomaterials 2013, 34, 9393–9400. [Google Scholar] [CrossRef] [PubMed]










© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qiu, M.; Chen, D.; Shen, C.; Shen, J.; Zhao, H.; He, Y. Platelet-Rich Plasma-Loaded Poly(d,l-lactide)-Poly(ethylene glycol)-Poly(d,l-lactide) Hydrogel Dressing Promotes Full-Thickness Skin Wound Healing in a Rodent Model. Int. J. Mol. Sci. 2016, 17, 1001. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17071001
Qiu M, Chen D, Shen C, Shen J, Zhao H, He Y. Platelet-Rich Plasma-Loaded Poly(d,l-lactide)-Poly(ethylene glycol)-Poly(d,l-lactide) Hydrogel Dressing Promotes Full-Thickness Skin Wound Healing in a Rodent Model. International Journal of Molecular Sciences. 2016; 17(7):1001. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17071001
Chicago/Turabian StyleQiu, Manle, Daoyun Chen, Chaoyong Shen, Ji Shen, Huakun Zhao, and Yaohua He. 2016. "Platelet-Rich Plasma-Loaded Poly(d,l-lactide)-Poly(ethylene glycol)-Poly(d,l-lactide) Hydrogel Dressing Promotes Full-Thickness Skin Wound Healing in a Rodent Model" International Journal of Molecular Sciences 17, no. 7: 1001. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17071001