
Leptin Receptor Metabolism Disorder in Primary Chondrocytes from Adolescent Idiopathic Scoliosis Girls


Abstract
:1. Introduction
2. Results
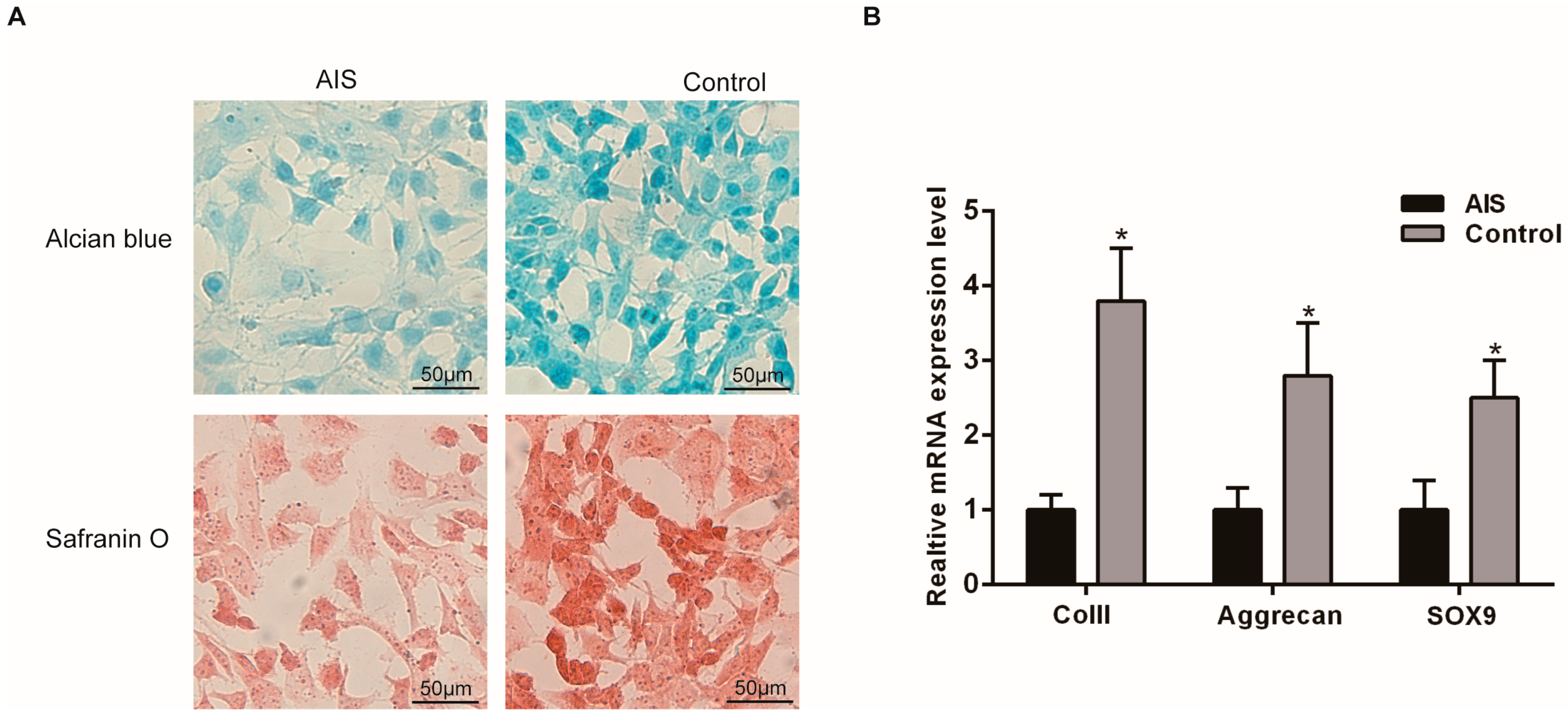
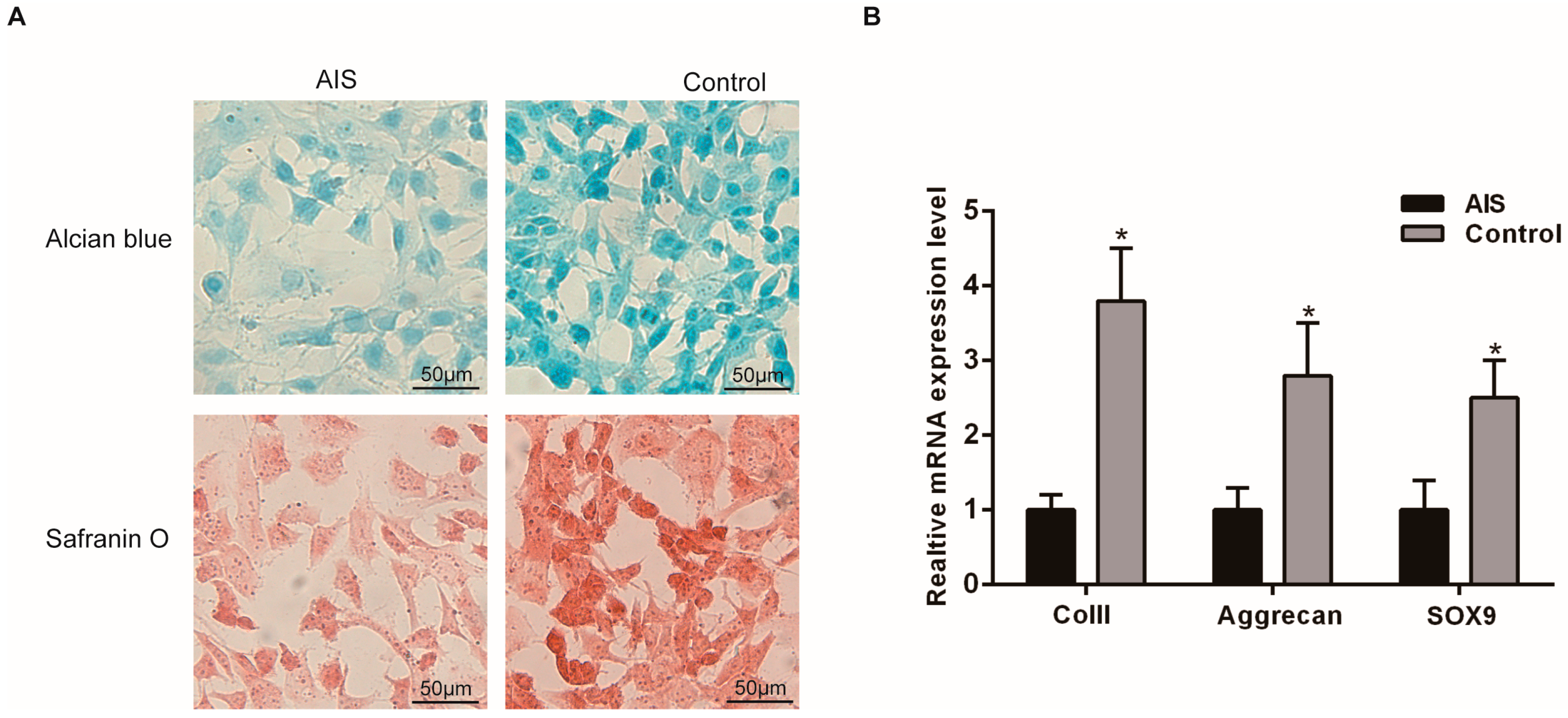
2.1. Chondrocytes Isolated from the Facet Joint of AIS Patients Showed Low Metabolic Activity
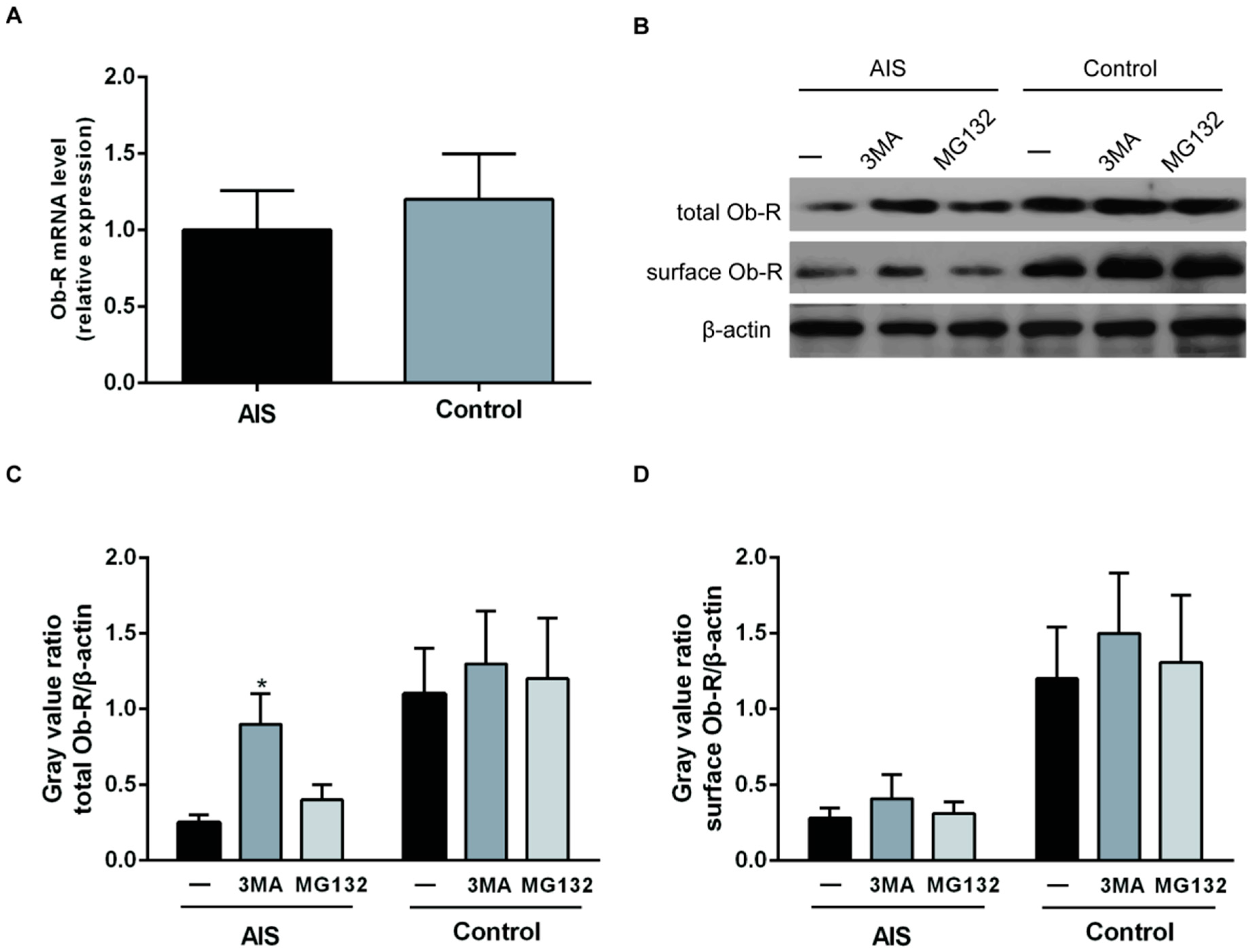
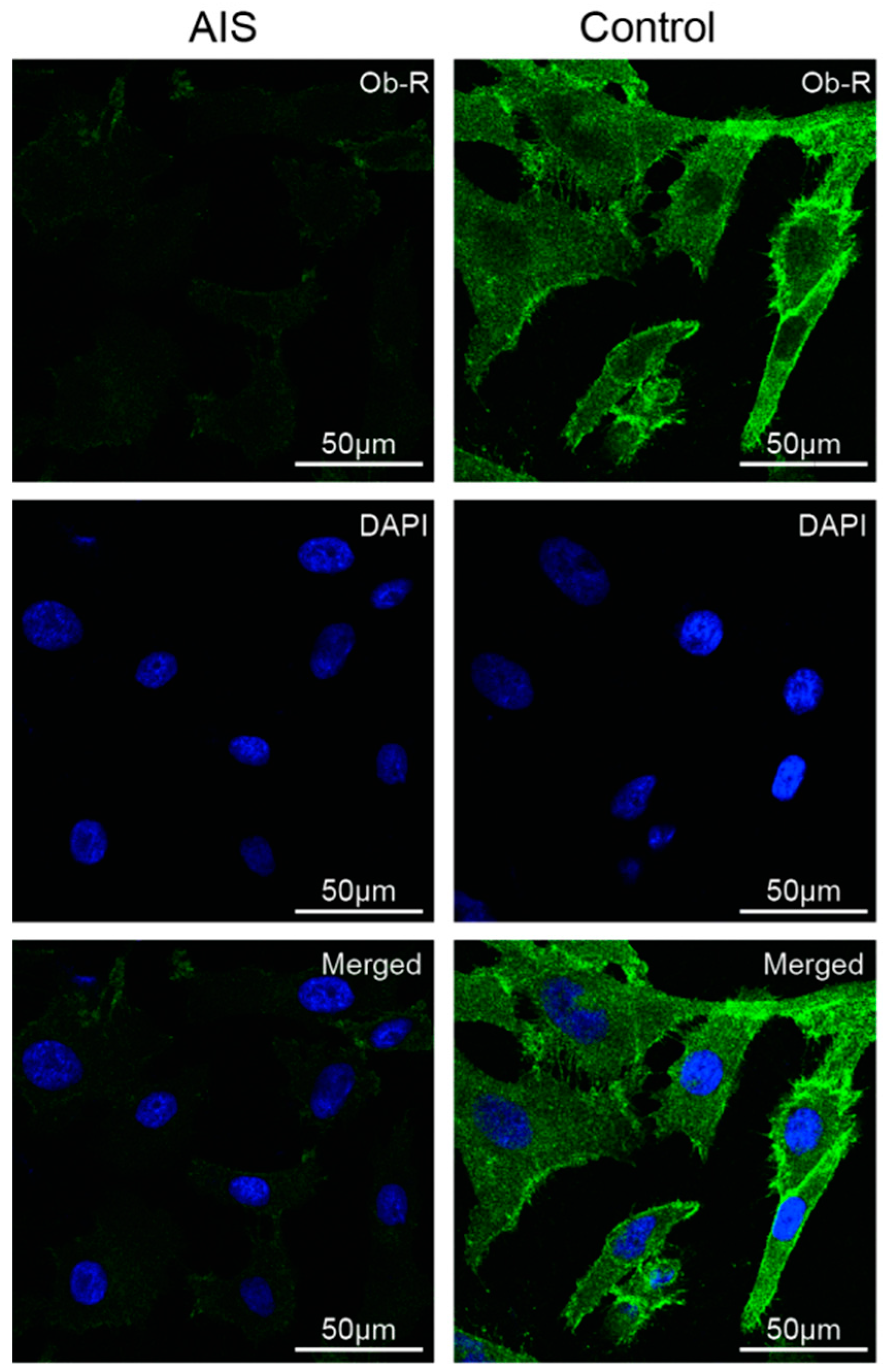
2.2. AIS Patients Showed Similar Total Serum Leptin Levels to those of the Controls but Lower Membrane Ob-R Expression in Primary Chondrocytes
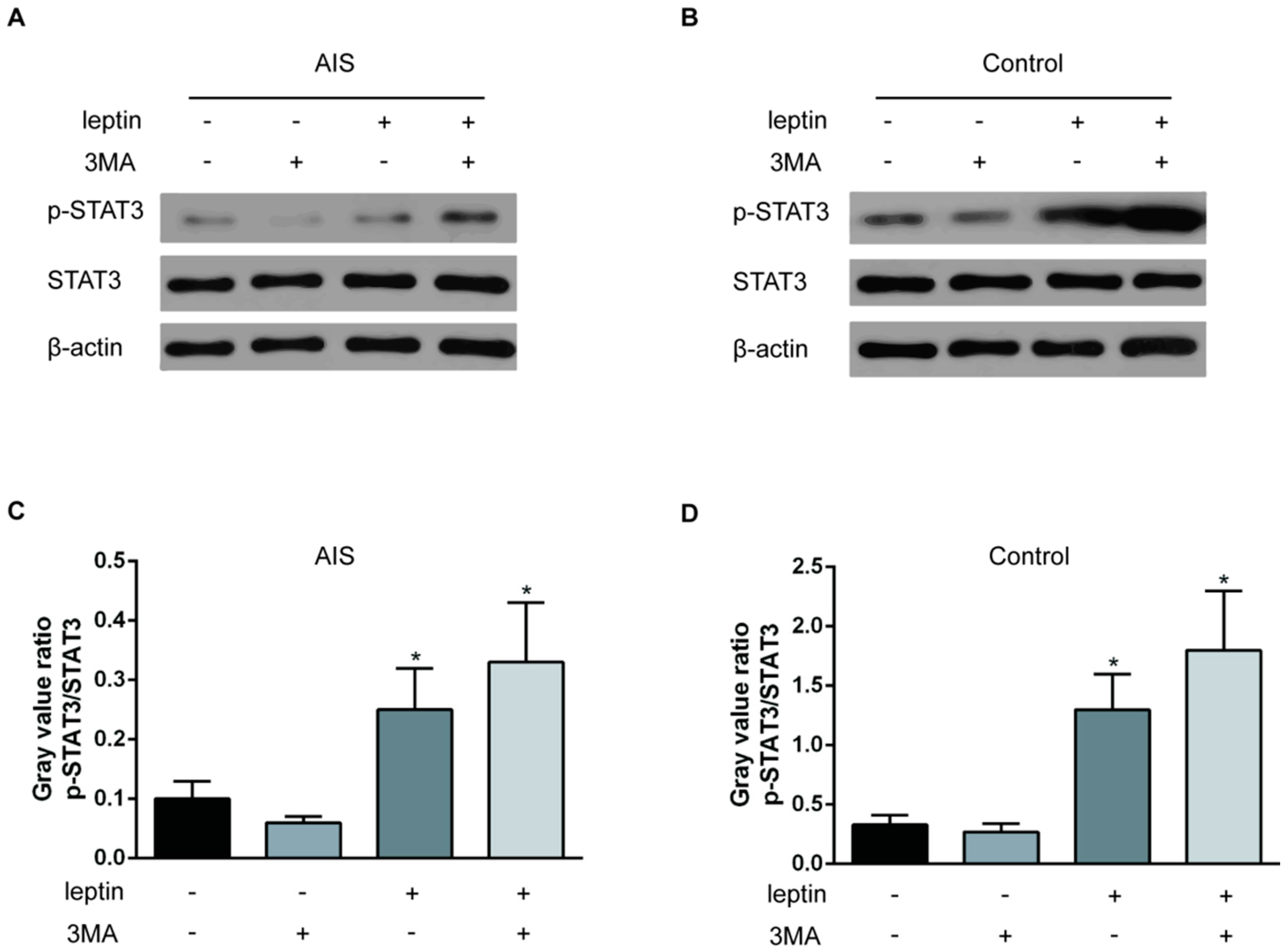
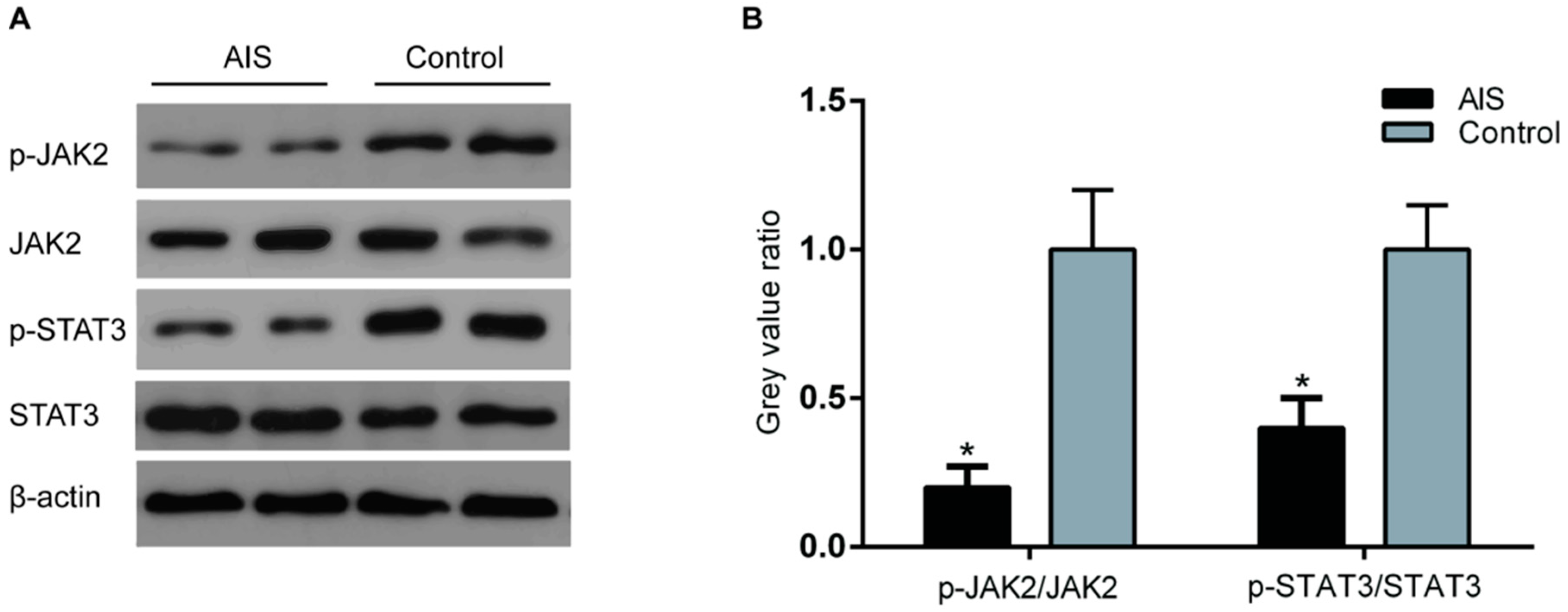
2.3. Chondrocytes of AIS Girls Showed Reduced JAK2 and STAT3 Phosphorylation
2.4. Lysosome Inhibition Increases the Ob-R Content but Has No Effect on Ob-R Membrane Expression or Leptin’s Effects on AIS Primary Chondrocytes
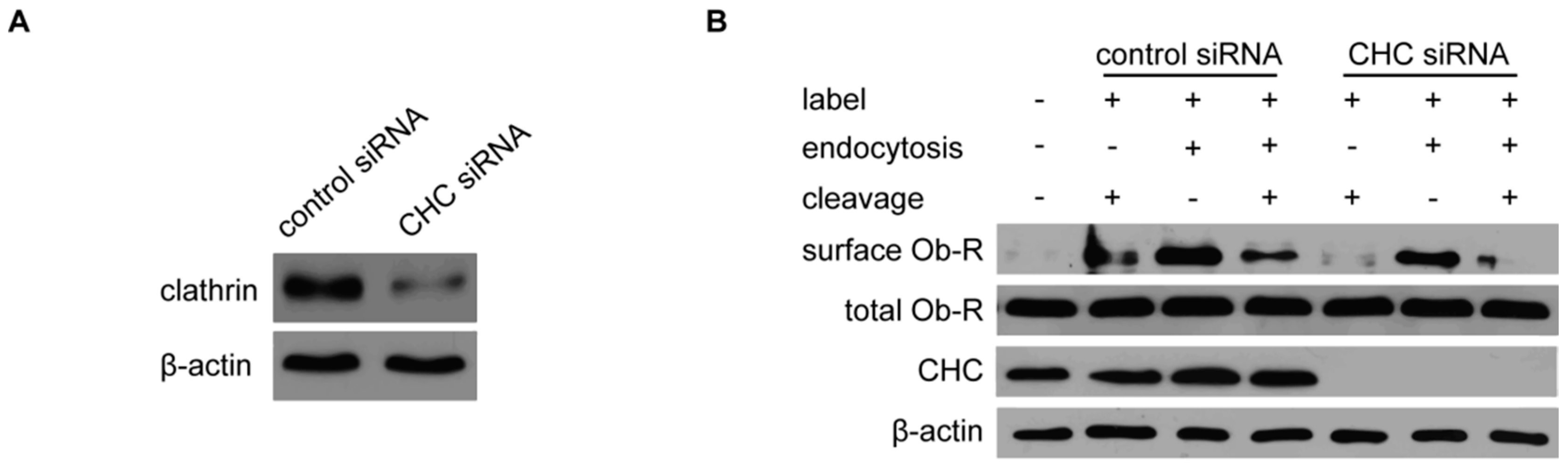
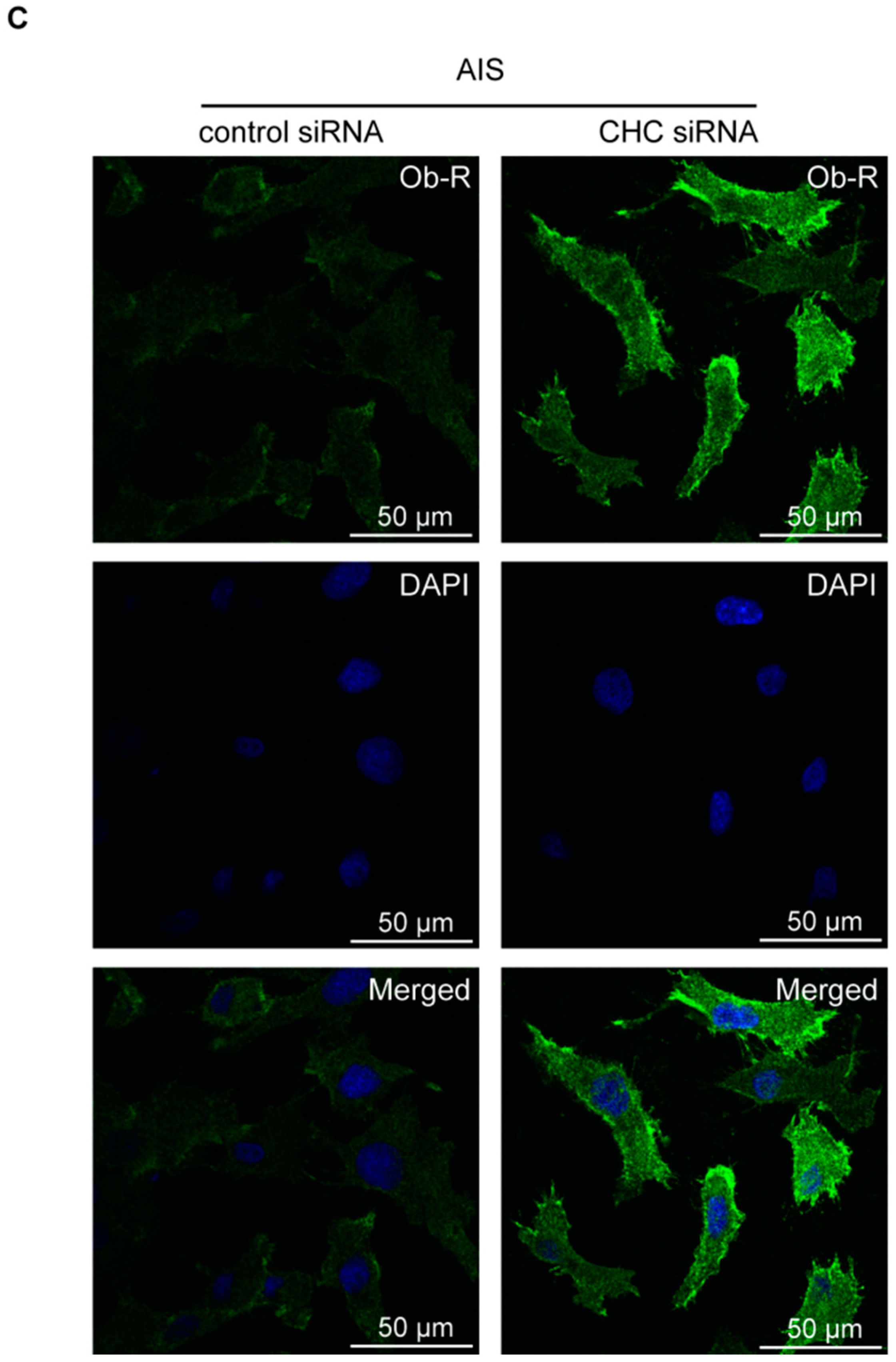
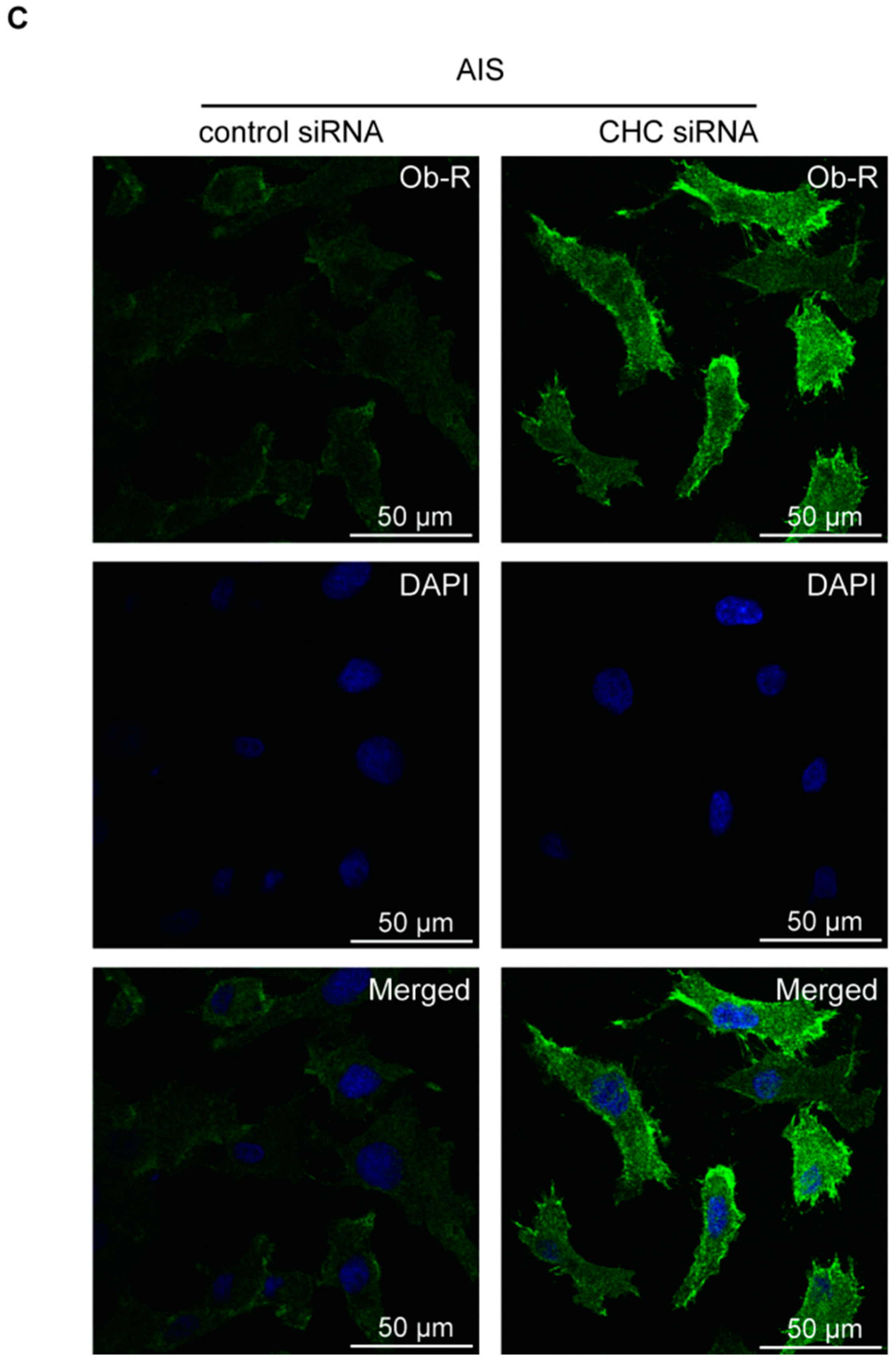
2.5. CHC Knockdown Upregulates the Membrane Ob-R Levels
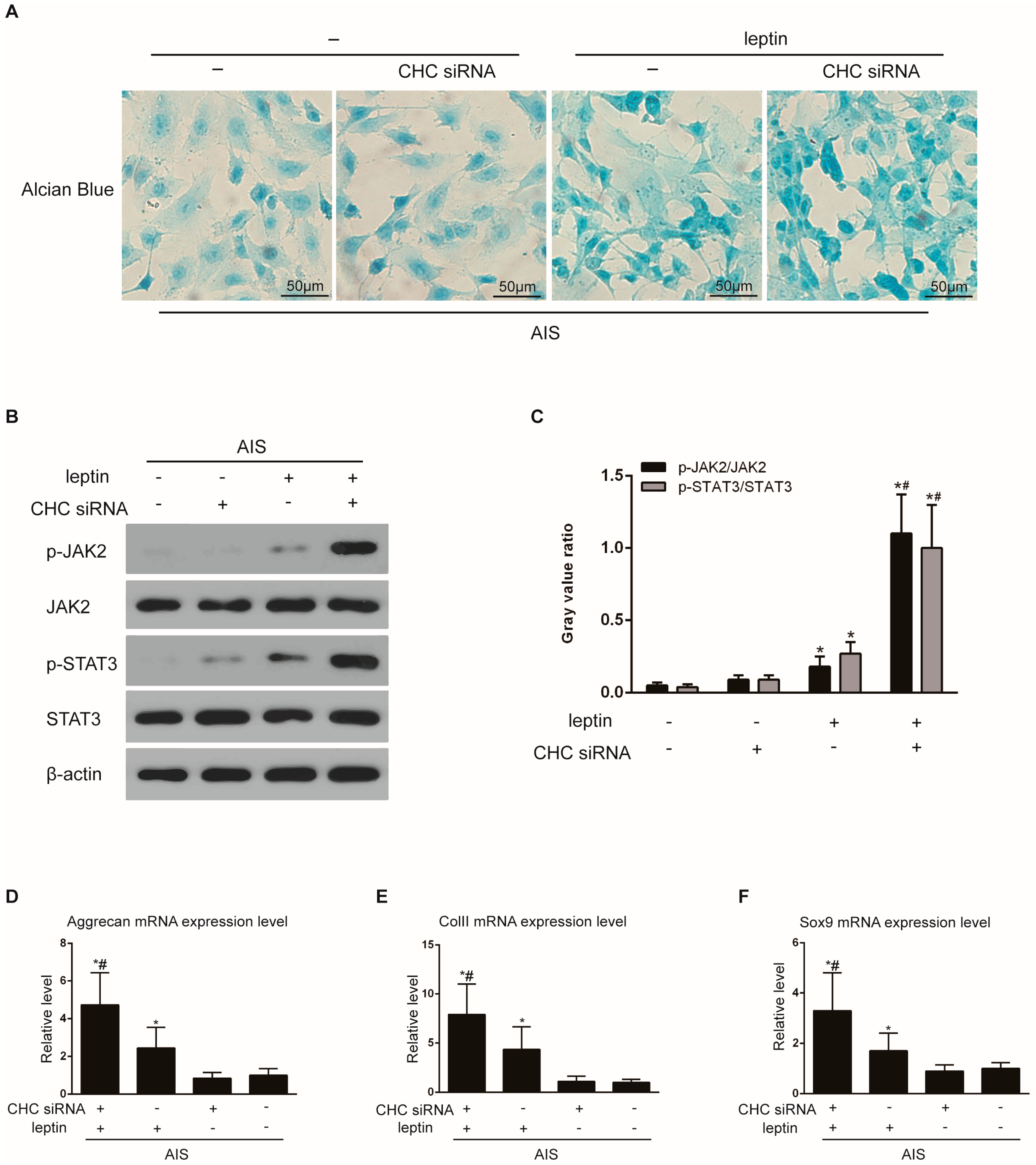
2.6. CHC Knockdown Enhances Leptin’s Effects on AIS Primary Chondrocytes
3. Discussion
4. Materials and Methods
4.1. Ethics Statement
4.2. Reagents
4.3. Patients and Samples
4.4. Isolation and Culture of Human Primary Chondrocytes
4.5. Cell Staining
4.6. Immunofluorescence and Confocal Microscopy
4.7. RNA Extraction and Real-Time PCR
4.8. siRNA Transfection
4.9. ELISA
4.10. Membrane Protein Isolation and Western Blot Analysis
4.11. Statistical Analysis
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| Ob-R | leptin receptor |
| AIS | adolescent idiopathic scoliosis |
| BMI | body mass index |
| CHC | clathrin heavy chain |
| RASO | relative anterior spinal overgrowth |
| BMP | bone morphogenetic protein |
| MMP | matrix metalloproteinase |
| PFA | Paraformaldehyde |
| PBS | phosphate-buffered saline |
| DAPI | 4, 6-diamidino-2-phenylindole |
| GSH | l-glutathione |
| GAGs | Glycosaminoglycans |
| SNS | sympathetic nervous system |
| PVDF | Polyvinylidene Difluoride |
References
- Hengwei, F.; Zifang, H.; Qifei, W.; Weiqing, T.; Nali, D.; Ping, Y.; Junlin, Y. Prevalence of idiopathic scoliosis in Chinese schoolchildren: A large, population-based study. Spine 2016, 41, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Ahn, U.M.; Ahn, N.U.; Nallamshetty, L.; Buchowski, J.M.; Rose, P.S.; Miller, N.H.; Kostuik, J.P.; Sponseller, P.D. The etiology of adolescent idiopathic scoliosis. Am. J. Orthop. 2002, 31, 387–395. [Google Scholar] [PubMed]
- Guo, X.; Chau, W.W.; Chan, Y.L.; Cheng, J.C.; Burwell, R.G.; Dangerfield, P.H. Relative anterior spinal overgrowth in adolescent idiopathic scoliosis—Result of disproportionate endochondral-membranous bone growth? Summary of an electronic focus group debate of the IBSE. Eur. Spine J. 2005, 14, 862–873. [Google Scholar] [CrossRef] [PubMed]
- Chu, W.C.; Lam, W.M.; Ng, B.K.; Tze-Ping, L.; Lee, K.M.; Guo, X.; Cheng, J.C.; Burwell, R.G.; Dangerfield, P.H.; Jaspan, T. Relative shortening and functional tethering of spinal cord in adolescent scoliosis—Result of asynchronous neuro-osseous growth, summary of an electronic focus group debate of the ibse. Scoliosis Spinal J. 2008, 3. [Google Scholar] [CrossRef] [PubMed]
- Cheung, C.S.; Lee, W.T.; Tse, Y.K.; Lee, K.M.; Guo, X.; Qin, L.; Cheng, J.C. Generalized osteopenia in adolescent idiopathic scoliosis—Association with abnormal pubertal growth, bone turnover, and calcium intake? Spine 2006, 31, 330–338. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.C.; Qin, L.; Cheung, C.S.; Sher, A.H.; Lee, K.M.; Ng, S.W.; Guo, X. Generalized low areal and volumetric bone mineral density in adolescent idiopathic scoliosis. J. Bone Miner. Res. 2000, 15, 1587–1595. [Google Scholar] [CrossRef] [PubMed]
- Sinha, M.K.; Sturis, J.; Ohannesian, J.; Magosin, S.; Stephens, T.; Heiman, M.L.; Polonsky, K.S.; Caro, J.F. Ultradian oscillations of leptin secretion in humans. Biochem. Biophys. Res. Commun. 1996, 228, 733–738. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, M.; Leibel, R.L. 20 years of leptin: Role of leptin in energy homeostasis in humans. J. Endocrinol. 2014, 223, T83–T96. [Google Scholar] [CrossRef] [PubMed]
- Turner, R.T.; Kalra, S.P.; Wong, C.P.; Philbrick, K.A.; Lindenmaier, L.B.; Boghossian, S.; Iwaniec, U.T. Peripheral leptin regulates bone formation. J. Bone Miner. Res. 2013, 28, 22–34. [Google Scholar] [CrossRef] [PubMed]
- Ducy, P.; Amling, M.; Takeda, S.; Priemel, M.; Schilling, A.F.; Beil, F.T.; Shen, J.; Vinson, C.; Rueger, J.M.; Karsenty, G. Leptin inhibits bone formation through a hypothalamic relay: A central control of bone mass. Cell 2000, 100, 197–207. [Google Scholar] [CrossRef]
- Figenschau, Y.; Knutsen, G.; Shahazeydi, S.; Johansen, O.; Sveinbjornsson, B. Human articular chondrocytes express functional leptin receptors. Biochem. Biophys. Res. Commun. 2001, 287, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Han, G.; Jing, Y.; Zhang, Y.; Yue, Z.; Hu, X.; Wang, L.; Liang, J.; Liu, J. Osteogenic differentiation of bone marrow mesenchymal stem cells by adenovirus-mediated expression of leptin. Regul. Pept. 2010, 163, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Shao, Y.Y.; Ballock, R.T. Leptin synergizes with thyroid hormone signaling in promoting growth plate chondrocyte proliferation and terminal differentiation in vitro. Bone 2011, 48, 1022–1027. [Google Scholar] [CrossRef] [PubMed]
- Kishida, Y.; Hirao, M.; Tamai, N.; Nampei, A.; Fujimoto, T.; Nakase, T.; Shimizu, N.; Yoshikawa, H.; Myoui, A. Leptin regulates chondrocyte differentiation and matrix maturation during endochondral ossification. Bone 2005, 37, 607–621. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.F.; Hsieh, R.Z.; Huang, K.C.; Chang, C.A.; Chiu, F.Y.; Kuo, H.C.; Chen, C.N.; Su, Y.P. Upregulation of bone morphogenetic protein-2 synthesis and consequent collagen II expression in leptin-stimulated human chondrocytes. PLoS ONE 2015, 10, e0144252. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Shen, J.; Wu, W.K.; Yu, X.; Liang, J.; Qiu, G.; Liu, J. The role of leptin on the organization and expression of cytoskeleton elements in nucleus pulposus cells. J. Orthop. Res. 2013, 31, 847–857. [Google Scholar] [CrossRef] [PubMed]
- Tam, E.M.; Yu, F.W.; Hung, V.W.; Liu, Z.; Liu, K.L.; Ng, B.K.; Lee, S.K.; Qiu, Y.; Cheng, J.C.; Lam, T.P. Are volumetric bone mineral density and bone micro-architecture associated with leptin and soluble leptin receptor levels in adolescent idiopathic scoliosis?—A case-control study. PLoS ONE 2014, 9, e87939. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Tam, E.M.; Sun, G.Q.; Lam, T.P.; Zhu, Z.Z.; Sun, X.; Lee, K.M.; Ng, T.B.; Qiu, Y.; Cheng, J.C.; et al. Abnormal leptin bioavailability in adolescent idiopathic scoliosis: An important new finding. Spine 2012, 37, 599–604. [Google Scholar] [CrossRef] [PubMed]
- Liang, G.; Gao, W.; Liang, A.; Ye, W.; Peng, Y.; Zhang, L.; Sharma, S.; Su, P.; Huang, D. Normal leptin expression, lower adipogenic ability, decreased leptin receptor and hyposensitivity to leptin in adolescent idiopathic scoliosis. PLoS ONE 2012, 7, e36648. [Google Scholar] [CrossRef] [PubMed]
- Zhu, F.; Qiu, Y.; Yeung, H.Y.; Lee, K.M.; Cheng, J.C. Histomorphometric study of the spinal growth plates in idiopathic scoliosis and congenital scoliosis. Pediatr. Int. 2006, 48, 591–598. [Google Scholar] [CrossRef] [PubMed]
- Burwell, R.G.; Dangerfield, P.H.; Moulton, A.; Anderson, S.I. Etiologic theories of idiopathic scoliosis: Autonomic nervous system and the leptin-sympathetic nervous system concept for the pathogenesis of adolescent idiopathic scoliosis. Stud. Health Technol. Inform. 2008, 140, 197–207. [Google Scholar] [PubMed]
- Qiu, Y.; Sun, X.; Qiu, X.; Li, W.; Zhu, Z.; Zhu, F.; Wang, B.; Yu, Y.; Qian, B. Decreased circulating leptin level and its association with body and bone mass in girls with adolescent idiopathic scoliosis. Spine 2007, 32, 2703–2710. [Google Scholar] [CrossRef] [PubMed]
- Upadhyay, J.; Farr, O.M.; Mantzoros, C.S. The role of leptin in regulating bone metabolism. Metab. Clin. Exp. 2015, 64, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Nakajima, R.; Inada, H.; Koike, T.; Yamano, T. Effects of leptin to cultured growth plate chondrocytes. Horm. Res. 2003, 60, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Yang, R.; Barouch, L.A. Leptin signaling and obesity: Cardiovascular consequences. Circ. Res. 2007, 101, 545–559. [Google Scholar] [CrossRef] [PubMed]
- Myers, M.G.; Cowley, M.A.; Munzberg, H. Mechanisms of leptin action and leptin resistance. Annu. Rev. Physiol. 2008, 70, 537–556. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Ceccarini, G.; Eisenstein, M.; Tan, K.; Friedman, J.M. Phenotypic effects of an induced mutation of the OBRA isoform of the leptin receptor. Mol. Metab. 2013, 2, 364–375. [Google Scholar] [CrossRef] [PubMed]
- Kimber, W.; Peelman, F.; Prieur, X.; Wangensteen, T.; O’Rahilly, S.; Tavernier, J.; Farooqi, I.S. Functional characterization of naturally occurring pathogenic mutations in the human leptin receptor. Endocrinology 2008, 149, 6043–6052. [Google Scholar] [CrossRef] [PubMed]
- Lundin, A.; Rondahl, H.; Walum, E.; Wilcke, M. Expression and intracellular localization of leptin receptor long isoform-GFP chimera. Biochim. Biophys. Acta 2000, 1499, 130–138. [Google Scholar] [CrossRef]
- Belouzard, S.; Delcroix, D.; Rouille, Y. Low levels of expression of leptin receptor at the cell surface result from constitutive endocytosis and intracellular retention in the biosynthetic pathway. J. Biol. Chem. 2004, 279, 28499–28508. [Google Scholar] [CrossRef] [PubMed]
- Belouzard, S.; Rouille, Y. Ubiquitylation of leptin receptor Ob-RA regulates its clathrin-mediated endocytosis. EMBO J. 2006, 25, 932–942. [Google Scholar] [CrossRef] [PubMed]
- Couturier, C.; Sarkis, C.; Seron, K.; Belouzard, S.; Chen, P.; Lenain, A.; Corset, L.; Dam, J.; Vauthier, V.; Dubart, A.; et al. Silencing of Ob-RGRP in mouse hypothalamic arcuate nucleus increases leptin receptor signaling and prevents diet-induced obesity. Proc. Natl. Acad. Sci. USA 2007, 104, 19476–19481. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| AIS (n = 31) | Controls (n = 15) | t Test | p | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| Age | 12.81 | 1.82 | 13.67 | 1.67 | −0.46 | 0.642 |
| Weight | 40.90 | 4.56 | 44.87 | 4.47 | −2.78 | 0.008 * |
| Height (cm) | 152.06 | 7.11 | 150.93 | 6.49 | 0.52 | 0.606 |
| BMI (kg/m2) | 17.66 | 1.15 | 19.66 | 0.91 | −5.90 | <0.001 * |
| Leptin levels (ng/mL) | 7.62 | 2.80 | 8.89 | 4.15 | −1.08 | 0.294 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.-J.; Yu, H.-G.; Zhou, Z.-H.; Guo, Q.; Wang, L.-J.; Zhang, H.-Q. Leptin Receptor Metabolism Disorder in Primary Chondrocytes from Adolescent Idiopathic Scoliosis Girls. Int. J. Mol. Sci. 2016, 17, 1160. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17071160
Wang Y-J, Yu H-G, Zhou Z-H, Guo Q, Wang L-J, Zhang H-Q. Leptin Receptor Metabolism Disorder in Primary Chondrocytes from Adolescent Idiopathic Scoliosis Girls. International Journal of Molecular Sciences. 2016; 17(7):1160. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17071160
Chicago/Turabian StyleWang, Yun-Jia, Hong-Gui Yu, Zhen-Hai Zhou, Qiang Guo, Long-Jie Wang, and Hong-Qi Zhang. 2016. "Leptin Receptor Metabolism Disorder in Primary Chondrocytes from Adolescent Idiopathic Scoliosis Girls" International Journal of Molecular Sciences 17, no. 7: 1160. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17071160