3.1. Data Extraction
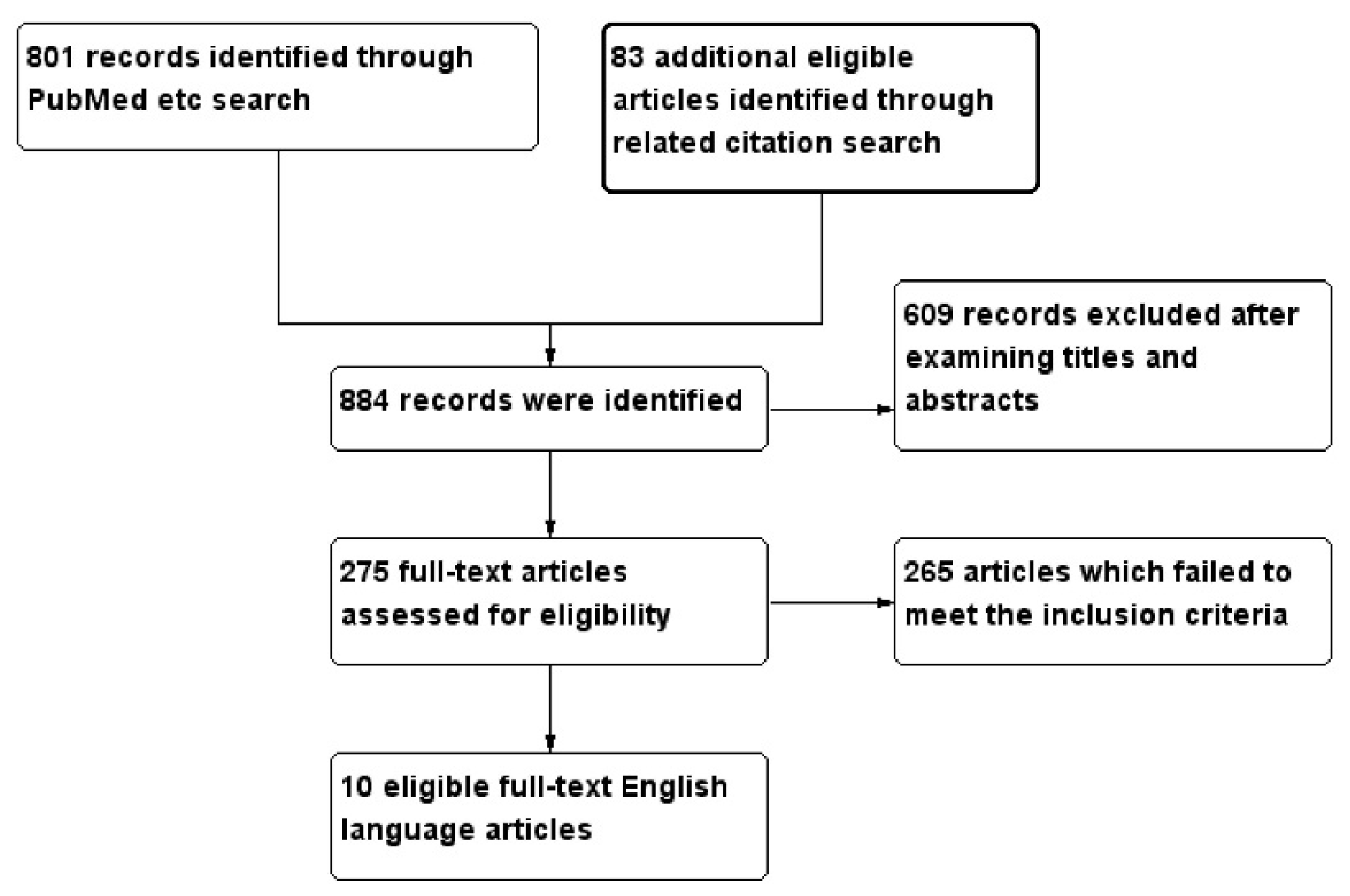
A total of 884 studies were identified. After exclusion of duplicates and review of the retrieved papers for the above criteria (the selection process is shown in
Figure 1), 10 studies comprising 15,769 symptomatic patients [
10,
11,
12,
13,
14,
15,
16,
17,
18,
19] were eligible for inclusion in the systematic review, while seven studies comprising 12,682 patients [
10,
11,
12,
14,
16,
17,
18] were eligible for inclusion in the meta-analysis. All are listed in
Table 1. A risk factor was included in the meta-analysis when at least three papers had provided data on that risk factor. The papers were then divided according to CAC assessment type (i.e., CAC presence, extent or progression). One study, Lai et al. [
10], assessed both CAC presence and extent and is, consequently, shown twice in both the systematic review and meta-analysis, while studies by Mayer et al. [
11] and Mitsutake et al. [
12] could be used for both CAC presence and extent in the meta-analysis but were used only for CAC extent in the systematic review.
CAC presence was defined as any CAC score >0. CAC extent was defined as the amount of the CAC score in studies which did not use a CAC score threshold or, in studies which did use a CAC score threshold, CAC extent was defined as any CAC score >100 compared to CAC = 0; any study with a CAC score threshold ≤100 was taken as a study of CAC presence. Similarly in angiographic studies, where moderate/severe calcification was compared with mild/no calcification, this was also taken as a study of CAC presence. CAC progression was defined as an increase in the CAC score over time.
Ten studies fitted our inclusion criteria [
10,
11,
12,
13,
14,
15,
16,
17,
18,
19], comprising 15,769 symptomatic patients, as outlined in
Table 1. The number of patients ranged from 114 in Maragiannis et al. [
17], to 1560 in Greif et al. [
15], with one study of CAC presence by Kovacic et al. [
16] comprising 9993 patients; due to the large numbers in this study, it will be separately mentioned in the analysis unless its results conform to those of all other studies. Three studies had a solely Japanese population [
12,
13,
19], two studies were Chinese [
10,
18], while one was Turkish [
14]. All studies were mixed gender, except for Lai et al. [
10] and Mayer et al. [
11], which investigated exclusively male patients. One study, Greif et al. [
15], separately investigated males and females and, consequently, this was treated as two separate studies [
15] in the analysis. All studies investigated a wide age range except Lai et al. [
10], whose patients were aged ≥65. All patients in the study by Kovacic et al. [
16] had coronary stenosis ≥60%, while those in the study by Mayer et al. [
11] had CAD and a close relative who had suffered a myocardial infarction before the age of 60 years. Eight of the 10 studies had CAC assessed by CT scanner, either 16- or 64-slice, but the remaining two were investigated angiographically. Kovacic et al. [
16] assessed the extent of CAC on the stenotic lesion undergoing percutaneous coronary intervention (PCI), with CAC being graded as none, mild, moderate or severe, while Mayer et al. [
11] assessed the CAC observed in the coronary vessels as none, mild-moderate, or severe. Kovacic et al. [
16] assessed predictors for calcification as moderate-severe calcification compared to no calcification; we have included this in the analysis as a study of CAC presence rather than CAC extent.
3.1.1. Systematic Review
We analysed the following numbers of studies in each category:
| CAC presence cross-sectional | six studies | 12,830 patients |
| CAC extent cross-sectional | four studies | 2986 patients |
| CAC progression | one study | 164 patients |
| Total symptomatic patients | 15,980 patients |
However, Lai et al. [
10], with 211 patients, was included in both CAC presence and extent.
3.1.2. Meta-Analyses
We analysed the following numbers of studies in each category, with three studies providing data for both CAC presence and extent:
| CAC presence cross-sectional | seven studies | 12,682 patients |
| CAC extent cross-sectional | three studies | 1623 patients |
The unadjusted ORs of each risk factors were estimated from the exposure distributions for CAC presence or absence [
20,
21], with the exception of the ORs from the study by Kovacic et al. [
16], which directly showed the univariate ORs in the results. Since age was a continuous parameter, the OR for age was pooled from multivariate results. For the remaining risk factors, few papers provided the multivariate ORs, so consequently the pooled ORs from multivariate results were not analysed. In the three papers which provided the ORs for both CAC presence and extent [
10,
11,
12], we extracted the exposure distributions for moderate and severe CAC and combined them as CAC presence. In these three papers, the ORs for the comparison between mild to moderate CAC and zero CAC and the comparison between severe CAC and zero CAC were pooled from the exposure distribution separately to assess the risk factors which predicted CAC extent.
3.2. Systematic Review
The papers were then analysed by age, gender, ethnicity, diabetes, dyslipidaemia, family history, hypertension, obesity, and smoking (
Table 2). In none of the studies was physical activity assessed. In several studies the definition of the risk factor comprised multiple components for example, dyslipidaemia could include any of elevated total, LDL cholesterol or the total/HDL cholesterol ratio, or decreased HDL cholesterol. For the purposes of analysis for the systematic review, a risk factor was assessed if any one of its components was present (so dyslipidaemia was predictive if only LDL cholesterol was elevated and all other components were in normal range). Analysis of the precise risk factor components is also provided in each relevant section, where any modifying effect of age is also considered.
Age: There are five studies showing that age is predictive of CAC presence [
14,
15,
16,
17,
18], compared to one which is not predictive [
10], although in this study all patients were as ≥65. Three studies showed that age was predictive of CAC extent [
11,
12,
13] and the same study of patients aged ≥65 found age not to be predictive [
10]. The only study of CAC progression found that age was not predictive [
19].
Male gender: two studies of CAC presence showed that gender was not predictive [
14,
16], including the angiographic study of 9993 patients [
16], although in two studies of CAC presence [
17,
18] and two studies of CAC extent it was predictive [
12,
13].
Ethnicity: The study of 9993 patients was the only one to consider ethnicity and this found that being white was predictive of CAC presence [
16].
Diabetes mellitus: The two Greif et al. studies [
15] and the angiographic study of 9993 patients [
16] found diabetes to be predictive of CAC presence, although four smaller studies showed that it is not [
10,
14,
17,
18]. Although one study of 1363 patients found diabetes to be predictive of CAC extent [
13], three studies with a total of 1623 patients showed that it was not predictive [
10,
11,
12]. The only study of CAC progression showed that diabetes was predictive [
19].
When the studies are analysed by markers for diabetes:
Blood glucose was not predictive of CAC presence [
14] or extent [
12].
Insulin was not predictive in one study of CAC presence and extent [
10].
HbA1c was not predictive of CAC presence [
15,
18] or extent [
11,
12], although it did show predictive ability for CAC progression [
19].
Oral hypoglycaemic medication was not predictive in one study of CAC presence and extent [
10].
Homeostatic Model Assessment-Insulin Resistance (HOMA-IR) was not predictive of CAC presence [
15].
Dyslipidaemia: Thee studies showed that dyslipidaemia was predictive of CAC presence [
15,
18], while four studies, including the study of 9333 patients, shows that it is not predictive [
10,
14,
16,
17]. For CAC extent, however, one study showed that dyslipidaemia was predictive [
11] but three studies, with more than twice as many patients, found it not to be predictive [
10,
12,
13]. The one study of CAC progression [
19] showed that it was not predictive.
When the studies are analysed by markers and biomarkers for dyslipidaemia:
Elevated LDL cholesterol was not predictive in all four studies of CAC presence [
14,
15,
16] and in two studies of CAC extent [
11,
12].
Elevated total cholesterol was not predictive in two studies of CAC presence [
14,
18], two studies of CAC extent [
11,
12], and one study of CAC progression [
19].
Decreased HDL was not predictive in three studies of CAC presence [
14,
15] and one study of CAC extent [
12], but was predictive of severe CAC extent in one study [
11].
Lipid-lowering medication was predictive in three studies of CAC presence [
15,
18], but was not predictive in one study of CAC presence [
10] and two studies of CAC extent [
10,
12].
Hypertension: Although two studies, including the study of 9993 patients, [
16,
17] found that hypertension was predictive of CAC presence, the remaining studies showed that it had no predictive ability for CAC presence [
10,
13,
15,
18]. Three studies of CAC extent found that it was predictive [
11,
12,
13], but one study found it not to be predictive [
10]; the one study of CAC progression was also predictive [
19].
When the studies are analysed by markers for hypertension:
Systolic blood pressure (SBP) was not predictive in three studies of CAC presence [
10,
15] and two studies of CAC extent [
10,
12] but one angiographic study showed it was predictive of severe CAC extent [
11]. SBP was also predictive of CAC progression [
19].
Diastolic blood pressure (DBP) was not predictive in three studies of CAC presence [
10,
15] and three studies of CAC extent [
10,
11,
12].
Antihypertensive medications were not predictive in four studies of CAC presence [
10,
15,
18] and one of CAC extent [
10].
Pulse pressure was not predictive in one study of CAC extent [
11] and the study of CAC progression [
19].
Family history of premature CHD: The only study to assess predictive ability for CAC presence was the study of 9993 patients [
16], which found it was not predictive. Among those investigating CAC extent, one was predictive, with 877 patients, [
11] but another was not, with 535 patients [
12]. The one predictive study of CAC extent was angiographic and investigated a family history of CAC since the population was preselected to comprise males with a family history of CAD [
11].
Obesity: Five studies found no ability for obesity to predict CAC presence [
10,
15,
17,
18], although the large study by Kovacic et al. found that there was an inverse predictive ability between obesity and CAC presence, making obesity protective against CAC [
16]. No study of CAC extent, found that obesity was predictive [
10,
11,
12]. The only study of CAC progression did not find obesity to be predictive [
19].
When the studies are analysed by markers for obesity:
Body mass index (BMI) was inversely predictive in the angiographic study of CAC presence involving 9993 patients [
16], but not in a further three studies of CAC presence [
10,
17,
18] and one of CAC extent [
10]. BMI was not predictive in one study of CAC progression [
19].
Weight was not predictive in one study of CAC extent [
16].
Smoking: With respect to CAC presence, only one small study found it to be predictive [
14], while the remainder, including the study of 9993 patients, found that smoking was not predictive of CAC presence [
10,
15,
16,
18]. None of the four studies of CAC extent [
10,
11,
12,
13] found smoking to be predictive.
When the studies are analysed by markers for smoking, current smoking was not predictive in two studies of CAC presence [
15].
3.3. Meta-Analysis
Out of the ten papers that were eligible for the systematic review [
10,
11,
12,
13,
14,
15,
16,
17,
18,
19], seven were also suitable for the meta-analysis: Lai et al. [
10], Mayer et al. [
11], Mitsutake et al. [
12], Atar et al. [
14], Kovacic et al. [
16], Maragiannis et al. [
17], and Qing et al. [
18].
The meta-analysis investigated the predictive ability of age, male gender, diabetes, dyslipidaemia, hypertension, and smoking for CAC presence and extent (
Supplementary Materials, Figure S1). It was not possible to include ethnicity, obesity, exercise, or number of risk factors, although family history of CAD was not predictive; since no other study assessed these two risk factors, they have not been entered in the meta-analysis. As mentioned above, data from three studies investigating CAC extent in the systematic review (Lai et al. [
10], Mayer et al. [
11], and Mitsutake et al. [
12]) have been re-analysed to identify potential risk factor predictors of CAC presence in the meta-analysis.
3.3.1. Predictors of CAC Presence
Table 3 gives the pooled results from the meta-analysis. The predictors of CAC presence in order of importance were hypertension (OR = 1.71,
p < 0.00001), male gender (OR = 1.47,
p = 0.02), diabetes (OR = 1.34,
p = 0.03), and age (OR = 1.07,
p = 0.04). Smoking and dyslipidaemia were not predictive of CAC presence. The Egger’s regression interception test was not significant suggesting no significant publication bias (
Table 3). Age, being a continuous variable, could not be entered into the Egger test. The funnel plots for each risk factor are provided in the
supplementary Figure S2 and, similarly, show no publication bias.
Due to the disproportionately large number of patients in the study by Kovavic et al. [
16], we repeated the meta-analysis after excluding this paper (shown in the
supplementary data, Table S1). This slightly increased the ORs for hypertension to 1.89 (
p < 0.00001), male gender to 1.74 (
p < 0.00001), diabetes to 1.45 (
p < 0.00001). Smoking and dyslipidaemia were still not significant.
3.3.2. Predictors of CAC Extent
Only three studies (Lai et al. [
10], Mayer et al. [
11], and Mitsutake et al. [
12]) analysed the predictors of CAC extent, among which Mayer et al. was an angiographic study classifying CAC as either “no calcification”, “mild to moderate calcification”, or “severe calcification”. Mitsutake et al. [
12] used CAC scoring and classified the lowest group (taken to be CAC = 0) as a CAC score of 0–12, the mild-moderate group as a CAC score of 13–445, and the severe calcification group as a CAC score of >445, while Lai et al. [
10] used a threshold CAC score of ≥400 The results are shown in
Table 4.
The presence of mild-moderate CAC, compared with zero CAC, was independently predicted only by hypertension (OR 1.61, p < 0.0001), with diabetes, dyslipidaemia, and smoking proving not to be predictive of mild-moderate CAC. The presence of severe CAC, compared with zero CAC, was predicted by hypertension (OR 2.09, p = 0.01) and diabetes (OR 1.55, p = 0.005); dyslipidaemia and smoking were not independently predictive of severe CAC. It was not possible to analyse age or male gender as predictors of CAC extent.
A summary of the studies showing the predictive ability of the risk factors from the systematic review and meta-analysis are shown at
Table 5.
3.3.3. Quality Assessment
We carried out a MINORS evaluation of the studies included in the meta-analysis, as shown at
Table 6. The items are scored 0 (not reported), 1 (reported but inadequate), or 2 (reported and adequate), with the global ideal score being 16 for non-comparative studies. Most studies scored 2 for all parameters, except follow-up data and prospectivity, which were obviously not in the design for our case-control studies. These results were considered quite satisfactory.




{kind=link}