Chronic Venous Insufficiency: Transforming Growth Factor-β Isoforms and Soluble Endoglin Concentration in Different States of Wound Healing



Abstract
:
1. Introduction
2. Results
2.1. Demographic Data
2.2. Pain Scale
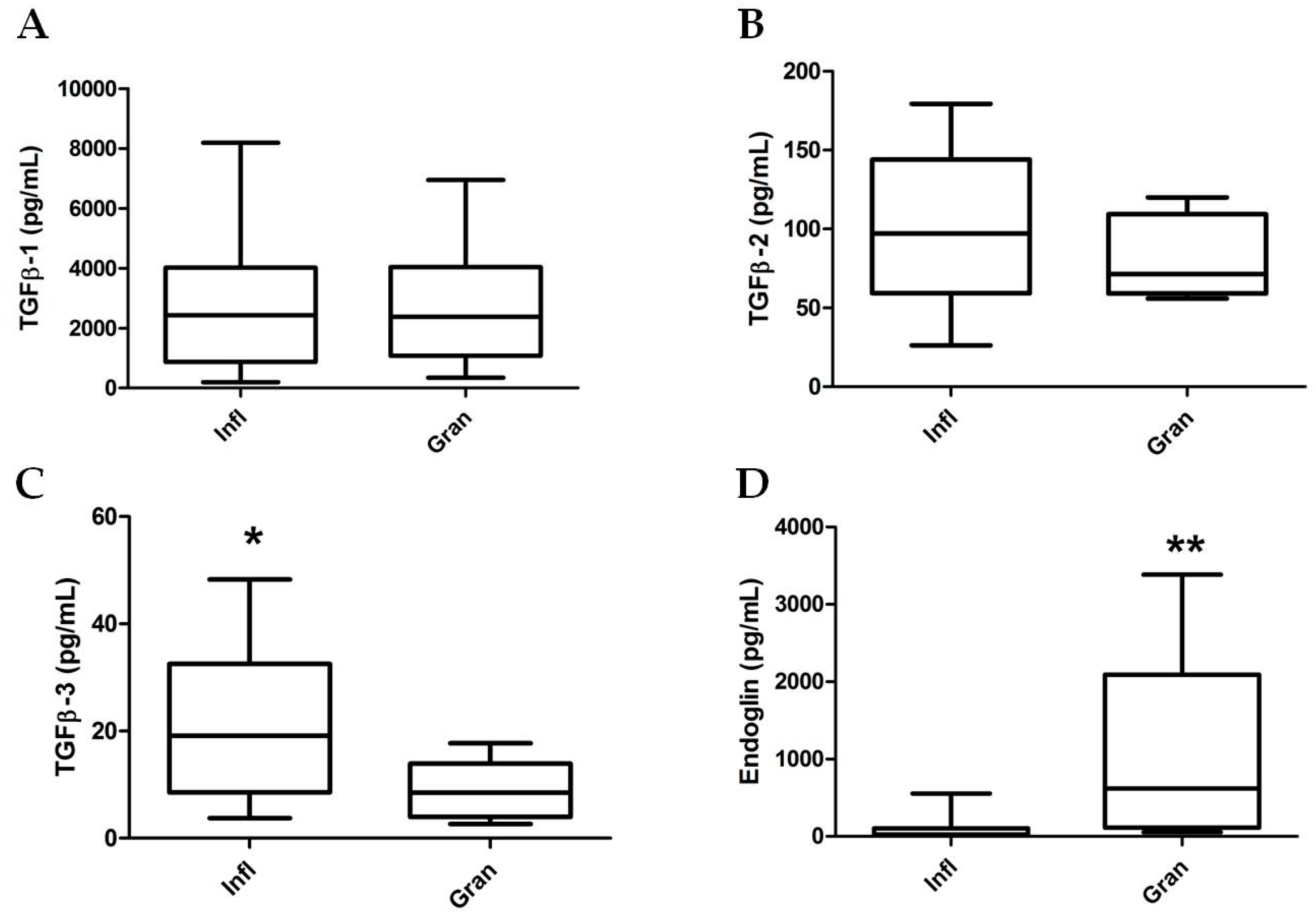
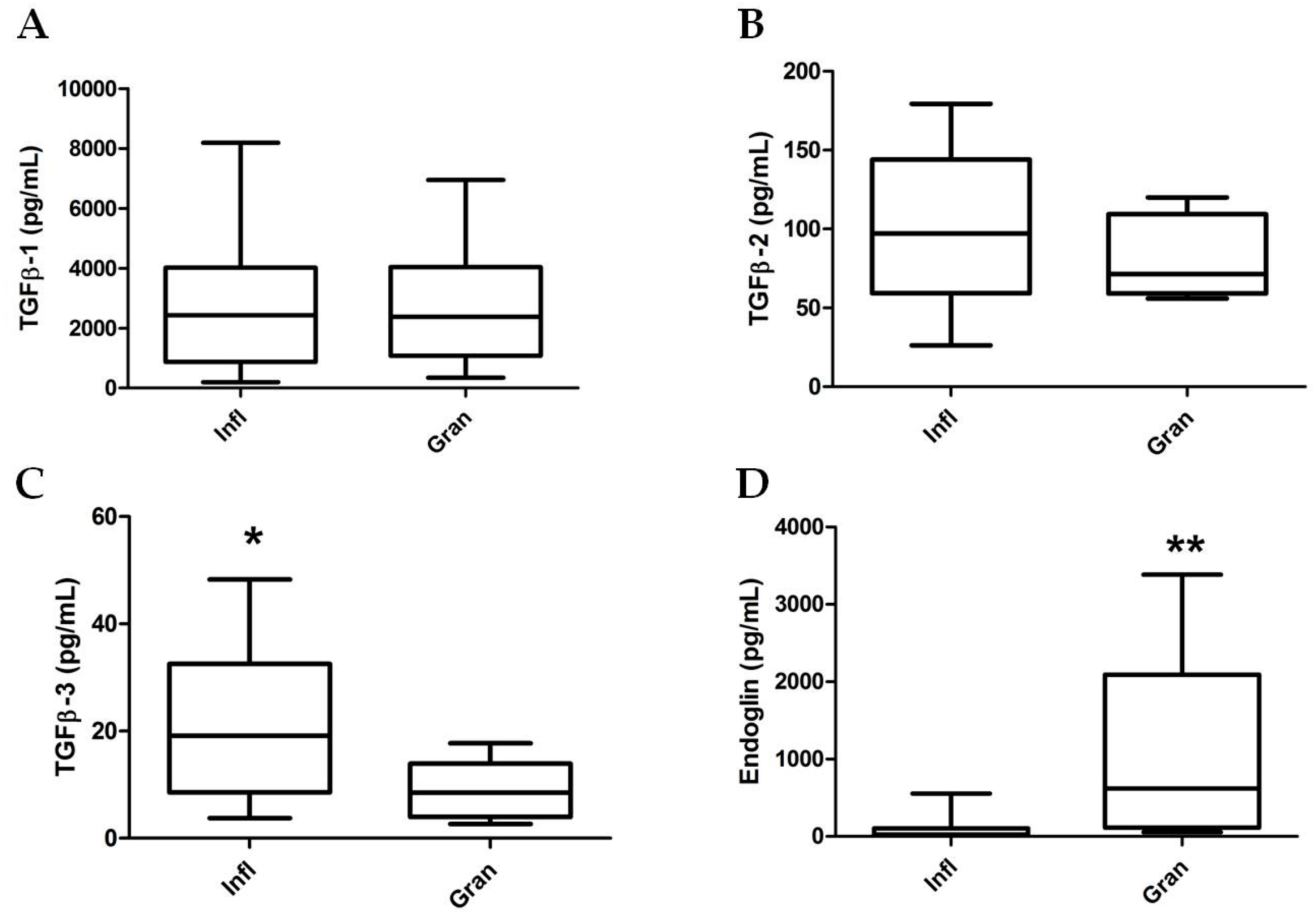
2.3. TGF-β Isoform and sEng Determination in Wound Fluids
2.4. Effects of Sulodexide on WF-Stimulated THP-1 Monocytes
3. Discussion
4. Materials and Methods
4.1. Patient Selection and Recruitment Criteria
4.2. Chronic Venous Ulcer Wound Fluid Protocol
4.3. Cell Culture and Treatments
4.4. Magnetic Multiplex Immunoassay
4.5. Chemicals
4.6. Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| CEAP | Clinical, etiological, anatomical, and pathophysiological classification |
| CVeD | Chronic venous disease |
| CVI | Chronic venous insufficiency |
| ECM | Extracellular matrix |
| IL | Interleukin |
| MMP | Matrix metalloproteinase |
| TGF-β | Transforming growth factor-β |
| VLU | Venous leg ulcer |
| WF | Wound fluid |
References
- Raffetto, J.D.; Mannello, F. Pathophysiology of chronic venous disease. Int. Angiol. 2014, 33, 212–221. [Google Scholar] [PubMed]
- Mannello, F.; Ligi, D.; Canale, M.; Raffetto, J.D. Omics profiles in chronic venous ulcer wound fluid: Innovative applications for translational medicine. Expert Rev. Mol. Diagn. 2014, 14, 737–762. [Google Scholar] [CrossRef] [PubMed]
- Raffetto, J.D.; Eberhardt, R.T.; Dean, S.M.; Ligi, D.; Mannello, F. Pharmacologic treatment to improve venous leg ulcer healing. J. Vasc. Surg. Venous. Lymphat. Disord. 2016, 4, 371–374. [Google Scholar] [CrossRef] [PubMed]
- Ligi, D.; Mosti, G.; Croce, L.; Raffetto, J.D.; Mannello, F. Chronic venous disease—Part II: Proteolytic biomarkers in wound healing. Biochim. Biophys. Acta 2016, 1862, 1900–1908. [Google Scholar] [CrossRef] [PubMed]
- Ligi, D.; Mosti, G.; Croce, L.; Raffetto, J.D.; Mannello, F. Chronic venous disease—Part I: Inflammatory biomarkers in wound healing. Biochim. Biophys. Acta 2016, 1862, 1964–1974. [Google Scholar] [CrossRef] [PubMed]
- Rossi, E.; Sanz-Rodriguez, F.; Eleno, N.; Duwell, A.; Blanco, F.J.; Langa, C.; Botella, L.M.; Cabanas, C.; Lopez-Novoa, J.M.; Bernabeu, C. Endothelial endoglin is involved in inflammation: Role in leukocyte adhesion and transmigration. Blood 2013, 121, 403–415. [Google Scholar] [CrossRef] [PubMed]
- Barrientos, S.; Stojadinovic, O.; Golinko, M.S.; Brem, H.; Tomic-Canic, M. Growth factors and cytokines in wound healing. Wound Repair Regen. 2008, 16, 585–601. [Google Scholar] [CrossRef] [PubMed]
- Sudgen, W.W.; Meissner, R.; Aegerter-Wilmsen, T.; Tsaryk, R.; Leonard, E.V.; Bussmann, J.; Hamm, M.J.; Herzog, W.; Jin, Y.; Jakobsson, L.; et al. Endoglin controls blood vessel diameter through endothelial cell shape changes in response to haemodynamic cues. Nat. Cell Biol. 2017, 19, 653–661. [Google Scholar]
- Kapur, N.K.; Morine, K.J.; Letarte, M. Endoglin: A critical mediator of cardiovascular health. Vasc. Health Risk Manag. 2013, 9, 195–206. [Google Scholar] [CrossRef] [PubMed]
- Goumans, M.J.; Liu, Z.; ten Dijke, P. TGF-β signaling in vascular biology and dysfunction. Cell Res. 2009, 19, 116–127. [Google Scholar] [CrossRef] [PubMed]
- Valluru, M.; Staton, C.A.; Reed, M.W.; Brown, N.J. Transforming growth factor-β and endoglin signaling orchestrate wound healing. Front. Physiol. 2011, 2, 89. [Google Scholar] [CrossRef] [PubMed]
- Pakyari, M.; Farrokhi, A.; Maharlooei, M.K.; Ghahary, A. Critical role of transforming growth factor β in different phases of wound healing. Adv. Wound Care 2013, 2, 215–224. [Google Scholar] [CrossRef] [PubMed]
- O’Kane, S.; Ferguson, M.W. Transforming growth factor βs and wound healing. Int. J. Biochem. Cell Biol. 1997, 29, 63–78. [Google Scholar] [CrossRef]
- Lal, B.K.; Saito, S.; Pappas, P.J.; Padberg, F.T.; Cerveira, J.J.; Hobson, R.W., 2nd; Duran, W.N. Altered proliferative responses of dermal fibroblasts to TGF-β1 may contribute to chronic venous stasis ulcer. J. Vasc. Surg. 2003, 37, 1285–1293. [Google Scholar] [CrossRef]
- Cowin, A.J.; Hatzirodos, N.; Holding, C.A.; Dunaiski, V.; Harries, R.H.; Rayner, T.E.; Fitridge, R.; Cooter, R.D.; Schultz, G.S.; Belford, D.A. Effect of healing on the expression of transforming growth factor β(s) and their receptors in chronic venous leg ulcers. J. Investig. Dermatol. 2001, 117, 1282–1289. [Google Scholar] [CrossRef] [PubMed]
- Montesano, R.; Orci, L. Transforming growth factor β stimulates collagen-matrix contraction by fibroblasts: Implications for wound healing. Proc. Natl. Acad. Sci. USA 1988, 85, 4894–4897. [Google Scholar] [CrossRef] [PubMed]
- Pocock, E.S.; Alsaigh, T.; Mazor, R.; Schmid-Schonbein, G.W. Cellular and molecular basis of Venous insufficiency. Vasc. Cell 2014, 6, 24. [Google Scholar] [CrossRef] [PubMed]
- Pastar, I.; Stojadinovic, O.; Krzyzanowska, A.; Barrientos, S.; Stuelten, C.; Zimmerman, K.; Blumenberg, M.; Brem, H.; Tomic-Canic, M. Attenuation of the transforming growth factor β-signaling pathway in chronic venous ulcers. Mol. Med. 2010, 16, 92–101. [Google Scholar] [CrossRef] [PubMed]
- Bautch, V.L. Endoglin moves and shapes endothelial cells. Nat. Cell Biol. 2017, 19, 593–595. [Google Scholar] [CrossRef] [PubMed]
- Torsney, E.; Charlton, R.; Parums, D.; Collis, M.; Arthur, H.M. Inducible expression of human endoglin during inflammation and wound healing in vivo. Inflamm. Res. 2002, 51, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Mannello, F.; Medda, V.; Ligi, D.; Raffetto, J.D. Glycosaminoglycan sulodexide inhibition of MMP-9 gelatinase secretion and activity: Possible pharmacological role against collagen degradation in vascular chronic diseases. Curr. Vasc. Pharmacol. 2013, 11, 354–365. [Google Scholar] [CrossRef] [PubMed]
- Hoppensteadt, D.A.; Fareed, J. Pharmacological profile of sulodexide. Int. Angiol. 2014, 33, 229–235. [Google Scholar] [PubMed]
- Andreozzi, G.M. Sulodexide in the treatment of chronic venous disease. Am. J. Cardiovasc. Drugs 2012, 12, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Mannello, F.; Ligi, D.; Raffetto, J.D. Glycosaminoglycan sulodexide modulates inflammatory pathways in chronic venous disease. Int. Angiol. 2014, 33, 236–242. [Google Scholar] [PubMed]
- Mattana, P.; Mannello, F.; Ferrari, P.; Agus, G.B. Vascular pathologies and inflammation: The anti-inflammatory properties of sulodexide. J. Vasc. Endovasc. Surg. 2012, 19, 1–7. [Google Scholar]
- Mosti, G.; de Maeseneer, M.; Cavezzi, A.; Parsi, K.; Morrison, N.; Nelzen, O.; Rabe, E.; Partsch, H.; Caggiati, A.; Simka, M.; et al. Society for Vascular Surgery and American Venous Forum Guidelines on the management of venous leg ulcers: The point of view of the International Union of Phlebology. Int. Angiol. 2015, 34, 202–218. [Google Scholar] [PubMed]
- Coccheri, S.; Mannello, F. Development and use of sulodexide in vascular diseases: Implications for treatment. Drug Des. Dev. Ther. 2014, 8, 49–65. [Google Scholar] [CrossRef] [PubMed]
- Raffetto, J.D. Dermal pathology, cellular biology, and inflammation in chronic venous disease. Thromb. Res. 2009, 123 (Suppl. S4), S66–S71. [Google Scholar] [CrossRef]
- Gohel, M.S.; Windhaber, R.A.; Tarlton, J.F.; Whyman, M.R.; Poskitt, K.R. The relationship between cytokine concentrations and wound healing in chronic venous ulceration. J. Vasc. Surg. 2008, 48, 1272–1277. [Google Scholar] [CrossRef] [PubMed]
- Trengove, N.J.; Stacey, M.C.; MacAuley, S.; Bennett, N.; Gibson, J.; Burslem, F.; Murphy, G.; Schultz, G. Analysis of the acute and chronic wound environments: The role of proteases and their inhibitors. Wound Repair Regen. 1999, 7, 442–452. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, R.; Vickaryous, M.; Viloria-Petit, A. Signalling by Transforming Growth Factor β Isoforms in Wound Healing and Tissue Regeneration. J. Dev. Biol. 2016, 4, 21. [Google Scholar] [CrossRef]
- Serini, G.; Gabbiana, G. Modulation of alpha-smooth muscle actin expression in fibroblasts by transforming growth factor-β isoforms: An in vivo and in vitro study. Wound Repair Regen. 1996, 4, 278–287. [Google Scholar] [CrossRef] [PubMed]
- Grainger, D.J.; Mosedale, D.E.; Metcalfe, J.C. TGF-β in blood: A complex problem. Cytokine Growth Factor Rev. 2000, 11, 133–145. [Google Scholar] [CrossRef]
- Simka, M. Cellular and molecular mechanisms of venous leg ulcers development—The “puzzle” theory. Int. Angiol. 2010, 29, 1–19. [Google Scholar] [PubMed]
- Kowalewski, R.; Malkowski, A.; Sobolewski, K.; Gacko, M. Evaluation of transforming growth factor-β signaling pathway in the wall of normal and varicose veins. Pathobiology 2010, 77, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Eickelberg, O.; Centrella, M.; Reiss, M.; Kashgarian, M.; Wells, R.G. βglycan inhibits TGF-β signaling by preventing type I-type II receptor complex formation: Glycosaminoglycan modifications alter betaglycan function. J. Biol. Chem. 2002, 277, 823–829. [Google Scholar] [CrossRef] [PubMed]
- Rathouska, J.; Jezkova, K.; Nemeckova, I.; Nachtigal, P. Soluble endoglin, hypercholesterolemia and endothelial dysfunction. Atherosclerosis 2015, 243, 383–388. [Google Scholar] [CrossRef] [PubMed]
- Lichtman, M.K.; Otero-Vinas, M.; Falanga, V. Transforming growth factor β isoforms in wound healing and fibrosis. Wound Repair Regen. 2016, 24, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Labropoulos, N.; Tiongson, J.; Pryor, L.; Tassiopoulos, A.K.; Kang, S.S.; Ashraf Mansour, M.; Baker, W.H. Definition of venous reflux in lower-extremity veins. J. Vasc. Surg. 2003, 38, 793–798. [Google Scholar] [CrossRef]
- Eklof, B.; Rutherford, R.B.; Bergan, J.J.; Carpentier, P.H.; Gloviczki, P.; Kistner, R.L.; Meissner, M.H.; Moneta, G.L.; Myers, K.; Padberg, F.T.; et al. Revision of the CEAP classification for chronic venous disorders: Consensus statement. J. Vasc. Surg. 2004, 40, 1248–1252. [Google Scholar] [CrossRef] [PubMed]
- Breivik, H.; Borchgrevink, P.C.; Allen, S.M.; Rosseland, L.A.; Romundstad, L.; Hals, E.K.; Kvarstein, G.; Stubhaug, A. Assessment of pain. Br. J. Anaesth. 2008, 101, 17–24. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Inflammatory | Granulating | p Value |
|---|---|---|---|
| Number, n (%) | 20 (67) | 10 (33) | |
| Age range, years | 43–91 | 65–85 | |
| Mean age (±SD), years | 71.4 ± 14.4 | 77.9 ± 6.6 | 0.370 |
| Sex | 0.231 | ||
| Male, n (%) | 5 (25) | 5 (50) | |
| Female, n (%) | 15 (75) | 5 (50) | |
| Comorbidities | |||
| Diabetes, n (%) | 7 (35) | 2 (20) | 0.675 |
| Hypertension, n (%) | 11 (55) | 9 (90) | 0.101 |
| Hyperlipidemia, n (%) | 12 (60) | 1 (10) | 0.017 |
| Smoking, n (%) | 2 (10) | 0 (0) | 0.540 |
| Rheumatic disease, n (%) | 2 (10) | 0 (0) | 0.540 |
| Ulcer History | 0.702 | ||
| Primary | 8 (40) | 3 (30) | |
| Recurrent | 12 (60) | 7 (70) | |
| Infection | 14 (70) | 0 (0) | <0.001 |
| Duration, months, mean ± SD | 51.4 ± 63.9 | 22.2 ± 18.3 | 0.481 |
| Surface area, cm2, mean ± SD | 12.7 ± 17.9 | 6.7 ± 4.2 | 0.947 |
| VAS * score, mean ± SD | 5.3 ± 1.3 | 3.4 ± 0.8 | <0.001 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ligi, D.; Croce, L.; Mosti, G.; Raffetto, J.D.; Mannello, F. Chronic Venous Insufficiency: Transforming Growth Factor-β Isoforms and Soluble Endoglin Concentration in Different States of Wound Healing. Int. J. Mol. Sci. 2017, 18, 2206. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms18102206
Ligi D, Croce L, Mosti G, Raffetto JD, Mannello F. Chronic Venous Insufficiency: Transforming Growth Factor-β Isoforms and Soluble Endoglin Concentration in Different States of Wound Healing. International Journal of Molecular Sciences. 2017; 18(10):2206. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms18102206
Chicago/Turabian StyleLigi, Daniela, Lidia Croce, Giovanni Mosti, Joseph D. Raffetto, and Ferdinando Mannello. 2017. "Chronic Venous Insufficiency: Transforming Growth Factor-β Isoforms and Soluble Endoglin Concentration in Different States of Wound Healing" International Journal of Molecular Sciences 18, no. 10: 2206. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms18102206