Psoriasis and Cardiovascular Comorbidities: Focusing on Severe Vascular Events, Cardiovascular Risk Factors and Implications for Treatment

Abstract
:
1. Introduction
2. Psoriasis and Severe Vascular Events
3. Psoriasis and Atherosclerosis
4. Psoriasis and Cardiovascular Risk Factors
4.1. Hypertension
4.2. Diabetes Mellitus
4.3. Dyslipidemia
4.4. Obesity
4.5. Metabolic Syndrome
4.6. Cigarette Smoking and Alcohol Consumption
5. Relationship between Severity of Psoriasis (in Terms of PASI and BSA) and Cardiovascular Risk
6. Psoriatic Arthritis and Cardiovascular Comorbidities
7. Pathogenic Mechanisms
7.1. Shared Genetic Factors
7.2. Common Inflammatory Pathways
7.3. Adipokines
7.4. Insulin Resistance
7.5. Lipoprotein Composition and Function
7.6. Angiogenesis and Oxidative Stress
7.7. Microparticles
7.8. Hypercoagulability
7.9. Serum Homocysteine Level
8. Biomarkers of Systemic Inflammation
9. Effects of Anti-Psoriasis Therapies on Cardiovascular Comorbidities
9.1. Methotrexate
9.2. Cyclosporine
9.3. Acitretin
9.4. Fumaric Acid Esters
9.5. Tumor Necrosis Factor-Alpha (TNF-α) Inhibitors
9.6. Anti-IL-12/23 Agents
9.7. Anti-IL-17 Agents
9.8. Apremilast
10. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| PET/CT | Positron emission tomography/computed tomography |
| PASI | Psoriasis area and severity index |
| BSA | Body surface area |
| HDL | High-density lipoprotein |
| LDL | Low-density lipoprotein |
| BMI | Body mass index |
| CRP | C-Reactive protein |
| TNF-α | Tumor necrosis factor-α |
References
- Augustin, M.; Radtke, M.A. Quality of life in psoriasis patients. Expert Rev. Pharmacoecon. Outcomes Res. 2014, 14, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Quintard, B.; Constant, A.; Bouyssou-Gauthier, M.L.; Paul, C.; Truchetet, F.; Thomas, P.; Guiguen, Y.; Taieb, A. Validation of a specific health-related quality of life instrument in a large cohort of patients with psoriasis: The QualiPso Questionnaire. Acta Derm. Venereol. 2011, 91, 660–665. [Google Scholar] [CrossRef] [PubMed]
- Gelfand, J.M.; Neimann, A.L.; Shin, D.B.; Wang, X.; Margolis, D.J.; Troxel, A.B. Risk of myocardial infarction in patients with psoriasis. JAMA 2006, 296, 1735–1741. [Google Scholar] [CrossRef] [PubMed]
- Furue, M.; Tsuji, G.; Chiba, T.; Kadono, T. Cardiovascular and Metabolic diseases comorbid with psoriasis: Beyond the skin. Intern. Med. 2017, 56, 1613–1619. [Google Scholar] [CrossRef] [PubMed]
- Shahwan, K.T.; Kimball, A.B. Psoriasis and cardiovascular disease. Med. Clin. N. Am. 2015, 99, 1227–1242. [Google Scholar] [CrossRef] [PubMed]
- Takeshita, J.; Grewal, S.; Langan, S.M.; Mehta, N.N.; Ogdie, A.; van Voorhees, A.S.; Gelfand, J.M. Psoriasis and comorbid diseases: Epidemiology. J. Am. Acad. Dermatol. 2017, 76, 377–390. [Google Scholar] [CrossRef] [PubMed]
- Ryan, C.; Kirby, B. Psoriasis is a systemic disease with multiple cardiovascular and metabolic comorbidities. Dermatol. Clin. 2015, 33, 41–55. [Google Scholar] [CrossRef] [PubMed]
- Kaye, J.A.; Li, L.; Jick, S.S. Incidence of risk factors for myocardial infarction and other vascular diseases in patients with psoriasis. Br. J. Dermatol. 2008, 159, 895–902. [Google Scholar] [CrossRef] [PubMed]
- Shah, K.; Mellars, L.; Changolkar, A.; Feldman, S.R. Real-world burden of comorbidities in US patients with psoriasis. J. Am. Acad. Dermatol. 2017, 77, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Li, M.; Wang, H.; Li, Y.; Bai, B. High prevalence of cardiovascular risk factors in patients with moderate or severe psoriasis in northern China. Arch. Dermatol. Res. 2014, 306, 247–251. [Google Scholar] [CrossRef] [PubMed]
- Gelfand, J.M.; Dommasch, E.D.; Shin, D.B.; Azfar, R.S.; Kurd, S.K.; Wang, X.; Troxel, A.B. The risk of stroke in patients with psoriasis. J. Investig. Dermatol. 2009, 129, 2411–2418. [Google Scholar] [CrossRef] [PubMed]
- Egeberg, A.; Thyssen, J.P.; Jensen, P.; Gislason, G.H.; Skov, L. Risk of myocardial infarction in patients with psoriasis and psoriatic arthritis: A nationwide cohort study. Acta Derm. Venereol. 2017, 97, 819–824. [Google Scholar] [CrossRef] [PubMed]
- Heredi, E.; Vegh, J.; Pogacsas, L.; Gaspar, K.; Varga, J.; Kincse, G.; Zeher, M.; Szegedi, A.; Gaal, J. Subclinical cardiovascular disease and it’s improvement after long-term TNF-alpha inhibitor therapy in severe psoriatic patients. J. Eur. Acad. Dermatol. Venereol. JEADV 2016, 30, 1531–1536. [Google Scholar] [CrossRef] [PubMed]
- Langan, S.M.; Seminara, N.M.; Shin, D.B.; Troxel, A.B.; Kimmel, S.E.; Mehta, N.N.; Margolis, D.J.; Gelfand, J.M. Prevalence of metabolic syndrome in patients with psoriasis: A population-based study in the United Kingdom. J. Investig. Dermatol. 2012, 132, 556–562. [Google Scholar] [CrossRef] [PubMed]
- Takeshita, J.; Wang, S.; Shin, D.B.; Mehta, N.N.; Kimmel, S.E.; Margolis, D.J.; Troxel, A.B.; Gelfand, J.M. Effect of psoriasis severity on hypertension control: A population-based study in the United Kingdom. JAMA Dermatol. 2015, 151, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Masson, W.; Rossi, E.; Galimberti, M.L.; Krauss, J.; Navarro Estrada, J.; Galimberti, R.; Cagide, A. Mortality in patients with psoriasis. A retrospective cohort study. Med. Clin. 2017, 148, 483–488. [Google Scholar] [CrossRef] [PubMed]
- Gelfand, J.M.; Troxel, A.B.; Lewis, J.D.; Kurd, S.K.; Shin, D.B.; Wang, X.; Margolis, D.J.; Strom, B.L. The risk of mortality in patients with psoriasis: Results from a population-based study. Arch. Dermatol. 2007, 143, 1493–1499. [Google Scholar] [CrossRef] [PubMed]
- Mehta, N.N.; Azfar, R.S.; Shin, D.B.; Neimann, A.L.; Troxel, A.B.; Gelfand, J.M. Patients with severe psoriasis are at increased risk of cardiovascular mortality: Cohort study using the General Practice Research Database. Eur. Heart J. 2010, 31, 1000–1006. [Google Scholar] [CrossRef] [PubMed]
- Siegel, D.; Devaraj, S.; Mitra, A.; Raychaudhuri, S.P.; Raychaudhuri, S.K.; Jialal, I. Inflammation, atherosclerosis, and psoriasis. Clin. Rev. Allergy Immunol. 2013, 44, 194–204. [Google Scholar] [CrossRef] [PubMed]
- Augustin, M.; Vietri, J.; Tian, H.; Gilloteau, I. Incremental burden of cardiovascular comorbidity and psoriatic arthritis among adults with moderate-to-severe psoriasis in five European countries. J. Eur. Acad. Dermatol. Venereol. JEADV 2017. [Google Scholar] [CrossRef] [PubMed]
- Feldman, S.R.; Tian, H.; Gilloteau, I.; Mollon, P.; Shu, M. Economic burden of comorbidities in psoriasis patients in the United States: Results from a retrospective U.S. database. BMC Health Serv. Res. 2017, 17, 337. [Google Scholar] [CrossRef] [PubMed]
- Benson, M.M.; Frishman, W.H. The heartbreak of psoriasis: A review of cardiovascular risk in patients with psoriasis. Cardiol. Rev. 2015, 23, 312–316. [Google Scholar] [CrossRef] [PubMed]
- Coumbe, A.G.; Pritzker, M.R.; Duprez, D.A. Cardiovascular risk and psoriasis: Beyond the traditional risk factors. Am. J. Med. 2014, 127, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, E.J.; Harskamp, C.T.; Armstrong, A.W. Psoriasis and major adverse cardiovascular events: A systematic review and meta-analysis of observational studies. J. Am. Heart Assoc. 2013, 2, e000062. [Google Scholar] [CrossRef] [PubMed]
- Ogdie, A.; Yu, Y.; Haynes, K.; Love, T.J.; Maliha, S.; Jiang, Y.; Troxel, A.B.; Hennessy, S.; Kimmel, S.E.; Margolis, D.J.; et al. Risk of major cardiovascular events in patients with psoriatic arthritis, psoriasis and rheumatoid arthritis: A population-based cohort study. Ann. Rheum. Dis. 2015, 74, 326–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, J.J.; Choi, Y.M.; Bebchuk, J.D. Risk of myocardial infarction in psoriasis patients: A retrospective cohort study. J. Dermatol. Treat. 2015, 26, 230–234. [Google Scholar] [CrossRef] [PubMed]
- Lai, Y.C.; Yew, Y.W. Psoriasis as an Independent Risk Factor for Cardiovascular Disease: An Epidemiologic Analysis Using a National Database. J. Cutan. Med. Surg. 2016, 20, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Li, W.Q.; Han, J.L.; Manson, J.E.; Rimm, E.B.; Rexrode, K.M.; Curhan, G.C.; Qureshi, A.A. Psoriasis and risk of nonfatal cardiovascular disease in U.S. women: A cohort study. Br. J. Dermatol. 2012, 166, 811–818. [Google Scholar] [CrossRef] [PubMed]
- Levesque, A.; Lachaine, J.; Bissonnette, R. Risk of myocardial infarction in canadian patients with psoriasis: A retrospective cohort study. J. Cutan. Med. Surg. 2013, 17, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.W.; Wang, K.H.; Lin, H.C.; Lin, H.C. Increased risk of acute myocardial infarction in patients with psoriasis: A 5-year population-based study in Taiwan. J. Am. Acad. Dermatol. 2011, 64, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Shiba, M.; Kato, T.; Funasako, M.; Nakane, E.; Miyamoto, S.; Izumi, T.; Haruna, T.; Inoko, M. Association between psoriasis vulgaris and coronary heart disease in a hospital-based population in Japan. PLoS ONE 2016, 11, e0149316. [Google Scholar] [CrossRef]
- Abuabara, K.; Azfar, R.S.; Shin, D.B.; Neimann, A.L.; Troxel, A.B.; Gelfand, J.M. Cause-specific mortality in patients with severe psoriasis: A population-based cohort study in the U.K. Br. J. Dermatol. 2010, 163, 586–592. [Google Scholar] [CrossRef] [PubMed]
- Stern, R.S.; Huibregtse, A. Very severe psoriasis is associated with increased noncardiovascular mortality but not with increased cardiovascular risk. J. Investig. Dermatol. 2011, 131, 1159–1166. [Google Scholar] [CrossRef] [PubMed]
- Wakkee, M.; Herings, R.M.; Nijsten, T. Psoriasis may not be an independent risk factor for acute ischemic heart disease hospitalizations: Results of a large population-based Dutch cohort. J. Investig. Dermatol. 2010, 130, 962–967. [Google Scholar] [CrossRef] [PubMed]
- Dowlatshahi, E.A.; Kavousi, M.; Nijsten, T.; Ikram, M.A.; Hofman, A.; Franco, O.H.; Wakkee, M. Psoriasis is not associated with atherosclerosis and incident cardiovascular events: The Rotterdam Study. J. Investig. Dermatol. 2013, 133, 2347–2354. [Google Scholar] [CrossRef] [PubMed]
- Ahlehoff, O.; Gislason, G.; Lamberts, M.; Folke, F.; Lindhardsen, J.; Larsen, C.T.; Torp-Pedersen, C.; Hansen, P.R. Risk of thromboembolism and fatal stroke in patients with psoriasis and nonvalvular atrial fibrillation: A Danish nationwide cohort study. J. Intern. Med. 2015, 277, 447–455. [Google Scholar] [CrossRef] [PubMed]
- Samarasekera, E.J.; Neilson, J.M.; Warren, R.B.; Parnham, J.; Smith, C.H. Incidence of cardiovascular disease in individuals with psoriasis: A systematic review and meta-analysis. J. Investig. Dermatol. 2013, 133, 2340–2346. [Google Scholar] [CrossRef] [PubMed]
- Xu, T.; Zhang, Y.H. Association of psoriasis with stroke and myocardial infarction: Meta-analysis of cohort studies. Br. J. Dermatol. 2012, 167, 1345–1350. [Google Scholar] [CrossRef] [PubMed]
- Chiang, C.H.; Huang, C.C.; Chan, W.L.; Huang, P.H.; Chen, Y.C.; Chen, T.J.; Chung, C.M.; Lin, S.J.; Chen, J.W.; Leu, H.B. Psoriasis and increased risk of ischemic stroke in Taiwan: A nationwide study. J. Dermatol. 2012, 39, 279–281. [Google Scholar] [CrossRef] [PubMed]
- Ahlehoff, O.; Gislason, G.H.; Jorgensen, C.H.; Lindhardsen, J.; Charlot, M.; Olesen, J.B.; Abildstrom, S.Z.; Skov, L.; Torp-Pedersen, C.; Hansen, P.R. Psoriasis and risk of atrial fibrillation and ischaemic stroke: A Danish Nationwide Cohort Study. Eur. Heart J. 2012, 33, 2054–2064. [Google Scholar] [CrossRef] [PubMed]
- Ahlehoff, O.; Gislason, G.H.; Charlot, M.; Jorgensen, C.H.; Lindhardsen, J.; Olesen, J.B.; Abildstrom, S.Z.; Skov, L.; Torp-Pedersen, C.; Hansen, P.R. Psoriasis is associated with clinically significant cardiovascular risk: A Danish nationwide cohort study. J. Intern. Med. 2011, 270, 147–157. [Google Scholar] [CrossRef] [PubMed]
- Prodanovich, S.; Kirsner, R.S.; Kravetz, J.D.; Ma, F.; Martinez, L.; Federman, D.G. Association of psoriasis with coronary artery, cerebrovascular, and peripheral vascular diseases and mortality. Arch. Dermatol. 2009, 145, 700–703. [Google Scholar] [CrossRef] [PubMed]
- Miller, I.M.; Ellervik, C.; Yazdanyar, S.; Jemec, G.B. Meta-analysis of psoriasis, cardiovascular disease, and associated risk factors. J. Am. Acad. Dermatol. 2013, 69, 1014–1024. [Google Scholar] [CrossRef] [PubMed]
- Brauchli, Y.B.; Jick, S.S.; Miret, M.; Meier, C.R. Psoriasis and risk of incident myocardial infarction, stroke or transient ischaemic attack: An inception cohort study with a nested case-control analysis. Br. J. Dermatol. 2009, 160, 1048–1056. [Google Scholar] [CrossRef] [PubMed]
- Dregan, A.; Charlton, J.; Chowienczyk, P.; Gulliford, M.C. Chronic inflammatory disorders and risk of type 2 diabetes mellitus, coronary heart disease, and stroke: A population-based cohort study. Circulation 2014, 130, 837–844. [Google Scholar] [CrossRef] [PubMed]
- Raaby, L.; Ahlehoff, O.; de Thurah, A. Psoriasis and cardiovascular events: Updating the evidence. Arch. Dermatol. Res. 2017, 309, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Ahlehoff, O.; Gislason, G.H.; Lindhardsen, J.; Olesen, J.B.; Charlot, M.; Skov, L.; Torp-Pedersen, C.; Hansen, P.R. Prognosis following first-time myocardial infarction in patients with psoriasis: A Danish nationwide cohort study. J. Intern. Med. 2011, 270, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Lan, C.C.; Ko, Y.C.; Yu, H.S.; Wu, C.S.; Li, W.C.; Lu, Y.W.; Chen, Y.C.; Chin, Y.Y.; Yang, Y.H.; Chen, G.S. Methotrexate reduces the occurrence of cerebrovascular events among Taiwanese psoriatic patients: A nationwide population-based study. Acta Derm. Venereol. 2012, 92, 349–352. [Google Scholar] [CrossRef] [PubMed]
- Mallbris, L.; Akre, O.; Granath, F.; Yin, L.; Lindelof, B.; Ekbom, A.; Stahle-Backdahl, M. Increased risk for cardiovascular mortality in psoriasis inpatients but not in outpatients. Eur. J. Epidemiol. 2004, 19, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Su, Y.S.; Yu, H.S.; Li, W.C.; Ko, Y.C.; Chen, G.S.; Wu, C.S.; Lu, Y.W.; Yang, Y.H.; Lan, C.C. Psoriasis as initiator or amplifier of the systemic inflammatory march: Impact on development of severe vascular events and implications for treatment strategy. J. Eur. Acad. Dermatol. Venereol. JEADV 2013, 27, 876–883. [Google Scholar] [CrossRef] [PubMed]
- Chiu, H.Y.; Hsieh, C.F.; Chiang, Y.T.; Tsai, Y.W.; Huang, W.F.; Li, C.Y.; Wang, T.S.; Tsai, T.F. Concomitant sleep disorders significantly increase the risk of cardiovascular disease in patients with psoriasis. PLoS ONE 2016, 11, e0146462. [Google Scholar] [CrossRef] [PubMed]
- Dowlatshahi, E.A.; Wakkee, M.; Arends, L.R.; Nijsten, T. The prevalence and odds of depressive symptoms and clinical depression in psoriasis patients: A systematic review and meta-analysis. J. Investig. Dermatol. 2014, 134, 1542–1551. [Google Scholar] [CrossRef] [PubMed]
- Luca, M.; Luca, A.; Musumeci, M.L.; Fiorentini, F.; Micali, G.; Calandra, C. Psychopathological Variables and Sleep Quality in Psoriatic Patients. Int. J. Mol. Sci. 2016, 17, 1184. [Google Scholar] [CrossRef] [PubMed]
- Egeberg, A.; Khalid, U.; Gislason, G.H.; Mallbris, L.; Skov, L.; Hansen, P.R. Impact of depression on risk of myocardial infarction, stroke and cardiovascular death in patients with psoriasis: A danish nationwide study. Acta Derm. Venereol. 2016, 96, 218–221. [Google Scholar] [CrossRef] [PubMed]
- Lan, C.C.; Yu, H.S.; Li, W.C.; Ko, Y.C.; Wu, C.S.; Lu, Y.W.; Yang, Y.H.; Chen, G.S. Anxiety contributes to the development of cerebrovascular disease in Taiwanese patients with psoriasis: A population-based study. Eur. J. Dermatol. EJD 2013, 23, 290–292. [Google Scholar] [CrossRef] [PubMed]
- Gisondi, P.; Fantin, F.; Del Giglio, M.; Valbusa, F.; Marino, F.; Zamboni, M.; Girolomoni, G. Chronic plaque psoriasis is associated with increased arterial stiffness. Dermatology 2009, 218, 110–113. [Google Scholar] [CrossRef] [PubMed]
- Choi, B.G.; Kim, M.J.; Yang, H.S.; Lee, Y.W.; Choe, Y.B.; Ahn, K.J. Assessment of arterial stiffness in korean patients with psoriasis by cardio-ankle vascular index. Angiology 2017, 68, 608–613. [Google Scholar] [CrossRef] [PubMed]
- Naik, H.B.; Natarajan, B.; Stansky, E.; Ahlman, M.A.; Teague, H.; Salahuddin, T.; Ng, Q.; Joshi, A.A.; Krishnamoorthy, P.; Dave, J.; et al. Severity of psoriasis associates with aortic vascular inflammation detected by FDG PET/CT and neutrophil activation in a prospective observational study. Arterioscler. Thromb. Vasc. Biol. 2015, 35, 2667–2676. [Google Scholar] [CrossRef] [PubMed]
- Dey, A.K.; Joshi, A.A.; Chaturvedi, A.; Lerman, J.B.; Aberra, T.M.; Rodante, J.A.; Teague, H.L.; Harrington, C.L.; Rivers, J.P.; Chung, J.H.; et al. Association between skin and aortic vascular inflammation in patients with psoriasis: A case-cohort study using positron emission tomography/computed tomography. JAMA Cardiol. 2017, 2, 1013–1018. [Google Scholar] [CrossRef] [PubMed]
- Mansouri, B.; Kivelevitch, D.; Natarajan, B.; Joshi, A.A.; Ryan, C.; Benjegerdes, K.; Schussler, J.M.; Rader, D.J.; Reilly, M.P.; Menter, A.; et al. Comparison of coronary artery calcium scores between patients with psoriasis and type 2 diabetes. JAMA Dermatol. 2016, 152, 1244–1253. [Google Scholar] [CrossRef] [PubMed]
- Staniak, H.L.; Bittencourt, M.S.; de Souza Santos, I.; Sharovsky, R.; Sabbag, C.; Goulart, A.C.; Lotufo, P.A.; Bensenor, I.M. Association between psoriasis and coronary calcium score. Atherosclerosis 2014, 237, 847–852. [Google Scholar] [CrossRef] [PubMed]
- Bissonnette, R.; Cademartiti, F.; Maffei, E.; Tardif, J.C. Increase in coronary atherosclerosis severity and the prevalence of coronary artery mixed plaques in patients with psoriasis. Br. J. Dermatol. 2017, 176, 800–802. [Google Scholar] [CrossRef] [PubMed]
- Hjuler, K.F.; Bottcher, M.; Vestergaard, C.; Deleuran, M.; Raaby, L.; Botker, H.E.; Iversen, L.; Kragballe, K. Increased prevalence of coronary artery disease in severe psoriasis and severe atopic dermatitis. Am. J. Med. 2015, 128, 1325–1334. [Google Scholar] [CrossRef] [PubMed]
- Picard, D.; Benichou, J.; Sin, C.; Abasq, C.; Houivet, E.; Koning, R.; Cribier, A.; Veber, B.; Dujardin, F.; Eltchaninoff, H.; et al. Increased prevalence of psoriasis in patients with coronary artery disease: Results from a case-control study. Br. J. Dermatol. 2014, 171, 580–587. [Google Scholar] [CrossRef] [PubMed]
- Zeb, I.; Budoff, M. Coronary artery calcium screening: Does it perform better than other cardiovascular risk stratification tools? Int. J. Mol. Sci. 2015, 16, 6606–6620. [Google Scholar] [CrossRef] [PubMed]
- Eckert, J.; Schmidt, M.; Magedanz, A.; Voigtlander, T.; Schmermund, A. Coronary CT angiography in managing atherosclerosis. Int. J. Mol. Sci. 2015, 16, 3740–3756. [Google Scholar] [CrossRef] [PubMed]
- Lerman, J.B.; Joshi, A.A.; Chaturvedi, A.; Aberra, T.M.; Dey, A.K.; Rodante, J.A.; Salahuddin, T.; Chung, J.H.; Rana, A.; Teague, H.L.; et al. Coronary plaque characterization in psoriasis reveals high-risk features that improve after treatment in a prospective observational study. Circulation 2017, 136, 263–276. [Google Scholar] [CrossRef] [PubMed]
- Salahuddin, T.; Natarajan, B.; Playford, M.P.; Joshi, A.A.; Teague, H.; Masmoudi, Y.; Selwaness, M.; Chen, M.Y.; Bluemke, D.A.; Mehta, N.N. Cholesterol efflux capacity in humans with psoriasis is inversely related to non-calcified burden of coronary atherosclerosis. Eur. Heart J. 2015, 36, 2662–2665. [Google Scholar] [CrossRef] [PubMed]
- Holzer, M.; Wolf, P.; Curcic, S.; Birner-Gruenberger, R.; Weger, W.; Inzinger, M.; El-Gamal, D.; Wadsack, C.; Heinemann, A.; Marsche, G. Psoriasis alters HDL composition and cholesterol efflux capacity. J. Lipid Res. 2012, 53, 1618–1624. [Google Scholar] [CrossRef] [PubMed]
- Evensen, K.; Slevolden, E.; Skagen, K.; Ronning, O.M.; Brunborg, C.; Krogstad, A.L.; Russell, D. Increased subclinical atherosclerosis in patients with chronic plaque psoriasis. Atherosclerosis 2014, 237, 499–503. [Google Scholar] [CrossRef] [PubMed]
- Santilli, S.; Kast, D.R.; Grozdev, I.; Cao, L.; Feig, R.L.; Golden, J.B.; Debanne, S.M.; Gilkeson, R.C.; Orringer, C.E.; McCormick, T.S.; et al. Visualization of atherosclerosis as detected by coronary artery calcium and carotid intima-media thickness reveals significant atherosclerosis in a cross-sectional study of psoriasis patients in a tertiary care center. J. Transl. Med. 2016, 14, 217. [Google Scholar] [CrossRef] [PubMed]
- Shaharyar, S.; Warraich, H.; McEvoy, J.W.; Oni, E.; Ali, S.S.; Karim, A.; Jamal, O.; Blaha, M.J.; Blumenthal, R.S.; Fialkow, J.; et al. Subclinical cardiovascular disease in plaque psoriasis: Association or causal link? Atherosclerosis 2014, 232, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Uyar, B.; Akyildiz, M.; Solak, A.; Genc, B.; Saklamaz, A. Relationship between serum fetuin-A levels and carotid intima-media thickness in turkish patients with mild to moderate psoriasis. A case-control study. Acta Dermatovenerol. Croat. ADC 2015, 23, 171–177. [Google Scholar] [PubMed]
- Steinl, D.C.; Kaufmann, B.A. Ultrasound imaging for risk assessment in atherosclerosis. Int. J. Mol. Sci. 2015, 16, 9749–9769. [Google Scholar] [CrossRef] [PubMed]
- Banska-Kisiel, K.; Haberka, M.; Bergler-Czop, B.; Brzezinska-Wcislo, L.; Okopien, B.; Gasior, Z. Carotid intima-media thickness in patients with mild or moderate psoriasis. Postep. Dermatol. I Alergol. 2016, 33, 286–289. [Google Scholar] [CrossRef] [PubMed]
- Fang, N.; Jiang, M.; Fan, Y. Association between psoriasis and subclinical atherosclerosis: A meta-analysis. Medicine 2016, 95, e3576. [Google Scholar] [CrossRef] [PubMed]
- Akyildiz, Z.I.; Seremet, S.; Emren, V.; Ozcelik, S.; Gediz, B.; Tastan, A.; Nazli, C. Epicardial fat thickness is independently associated with psoriasis. Dermatology 2014, 228, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Balci, A.; Celik, M.; Balci, D.D.; Karazincir, S.; Yonden, Z.; Korkmaz, I.; Celik, E.; Egilmez, E. Patients with psoriasis have an increased amount of epicardial fat tissue. Clin. Exp. Dermatol. 2014, 39, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Torres, T.; Bettencourt, N.; Mendonca, D.; Vasconcelos, C.; Gama, V.; Silva, B.M.; Selores, M. Epicardial adipose tissue and coronary artery calcification in psoriasis patients. J. Eur. Acad. Dermatol. Venereol. JEADV 2015, 29, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Guo, Z.; Zhu, Z.; Bao, Y.; Yang, B. Epicardial fat tissue in patients with psoriasis:a systematic review and meta-analysis. Lipids Health Dis. 2016, 15, 103. [Google Scholar] [CrossRef] [PubMed]
- Raposo, I.; Torres, T. Psoriasis strikes back! Epicardial adipose tissue: Another contributor to the higher cardiovascular risk in psoriasis. Revista Portuguesa de Cardiologia 2015, 34, 613–616. [Google Scholar] [CrossRef] [PubMed]
- Phan, C.; Sigal, M.L.; Lhafa, M.; Barthelemy, H.; Maccari, F.; Esteve, E.; Reguiai, Z.; Perrot, J.L.; Chaby, G.; Maillard, H.; et al. Metabolic comorbidities and hypertension in psoriasis patients in France. Comparisons with French national databases. Annales de Dermatologie et de Venereologie 2016, 143, 264–274. [Google Scholar] [CrossRef] [PubMed]
- Armesto, S.; Coto-Segura, P.; Osuna, C.G.; Camblor, P.M.; Santos-Juanes, J. Psoriasis and hypertension: A case-control study. J. Eur. Acad. Dermatol. Venereol. JEADV 2012, 26, 785–788. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.D.; Weitzman, D.; Dreiher, J. Psoriasis and hypertension: A case-control study. Acta Derm. Venereol. 2010, 90, 23–26. [Google Scholar] [CrossRef] [PubMed]
- Qureshi, A.A.; Choi, H.K.; Setty, A.R.; Curhan, G.C. Psoriasis and the risk of diabetes and hypertension: A prospective study of US female nurses. Arch. Dermatol. 2009, 145, 379–382. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, A.W.; Harskamp, C.T.; Armstrong, E.J. The association between psoriasis and hypertension: A systematic review and meta-analysis of observational studies. J. Hypertens. 2013, 31, 433–442, discussion 442–433. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Han, J.; Li, W.Q.; Qureshi, A.A. Hypertension, antihypertensive medication use, and risk of psoriasis. JAMA Dermatol. 2014, 150, 957–963. [Google Scholar] [CrossRef] [PubMed]
- Lonnberg, A.S.; Skov, L.; Skytthe, A.; Kyvik, K.O.; Pedersen, O.B.; Thomsen, S.F. Association of psoriasis with the risk for type 2 diabetes mellitus and obesity. JAMA Dermatol. 2016, 152, 761–767. [Google Scholar] [CrossRef] [PubMed]
- Dubreuil, M.; Rho, Y.H.; Man, A.; Zhu, Y.; Zhang, Y.; Love, T.J.; Ogdie, A.; Gelfand, J.M.; Choi, H.K. Diabetes incidence in psoriatic arthritis, psoriasis and rheumatoid arthritis: A UK population-based cohort study. Rheumatology 2014, 53, 346–352. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, A.W.; Harskamp, C.T.; Armstrong, E.J. Psoriasis and the risk of diabetes mellitus: A systematic review and meta-analysis. JAMA Dermatol. 2013, 149, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.S.; Lin, R.Y.; Lai, M.S. Increased risk of diabetes mellitus in relation to the severity of psoriasis, concomitant medication, and comorbidity: A nationwide population-based cohort study. J. Am. Acad. Dermatol. 2014, 70, 691–698. [Google Scholar] [CrossRef] [PubMed]
- Gyldenlove, M.; Storgaard, H.; Holst, J.J.; Vilsboll, T.; Knop, F.K.; Skov, L. Patients with psoriasis are insulin resistant. J. Am. Acad. Dermatol. 2015, 72, 599–605. [Google Scholar] [CrossRef] [PubMed]
- Ip, W.; Kirchhof, M.G. Glycemic control in the treatment of psoriasis. Dermatology 2017, 233, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Glossmann, H.; Reider, N. A marriage of two “Methusalem” drugs for the treatment of psoriasis?: Arguments for a pilot trial with metformin as add-on for methotrexate. Derm. Endocrinol. 2013, 5, 252–263. [Google Scholar] [CrossRef] [PubMed]
- Knowler, W.C.; Barrett-Connor, E.; Fowler, S.E.; Hamman, R.F.; Lachin, J.M.; Walker, E.A.; Nathan, D.M. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N. Engl. J. Med. 2002, 346, 393–403. [Google Scholar] [CrossRef] [PubMed]
- The 10-year cost-effectiveness of lifestyle intervention or metformin for diabetes prevention: An intent-to-treat analysis of the DPP/DPPOS. Diabetes Care 2012, 35, 723–730. [CrossRef]
- Orchard, T.J.; Temprosa, M.; Goldberg, R.; Haffner, S.; Ratner, R.; Marcovina, S.; Fowler, S. The effect of metformin and intensive lifestyle intervention on the metabolic syndrome: The Diabetes Prevention Program randomized trial. Ann. Intern. Med. 2005, 142, 611–619. [Google Scholar] [CrossRef] [PubMed]
- Long-term safety, tolerability, and weight loss associated with metformin in the Diabetes Prevention Program Outcomes Study. Diabetes Care 2012, 35, 731–737. [CrossRef]
- Singh, S.; Bhansali, A. Randomized placebo control study of insulin sensitizers (Metformin and Pioglitazone) in psoriasis patients with metabolic syndrome (Topical Treatment Cohort). BMC Dermatol. 2016, 16, 12. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Bhansali, A. Randomized placebo control study of metformin in psoriasis patients with metabolic syndrome (systemic treatment cohort). Indian J. Endocrinol. Metab. 2017, 21, 581–587. [Google Scholar] [CrossRef] [PubMed]
- Brauchli, Y.B.; Jick, S.S.; Curtin, F.; Meier, C.R. Association between use of thiazolidinediones or other oral antidiabetics and psoriasis: A population based case-control study. J. Am. Acad. Dermatol. 2008, 58, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.Y.; Shieh, J.J.; Shen, J.L.; Liu, Y.Y.; Chang, Y.T.; Chen, Y.J. Association between antidiabetic drugs and psoriasis risk in diabetic patients: Results from a nationwide nested case-control study in Taiwan. J. Am. Acad. Dermatol. 2015, 72, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, A.W.; Guerin, A.; Sundaram, M.; Wu, E.Q.; Faust, E.S.; Ionescu-Ittu, R.; Mulani, P. Psoriasis and risk of diabetes-associated microvascular and macrovascular complications. J. Am. Acad. Dermatol. 2015, 72, 968–977. [Google Scholar] [CrossRef] [PubMed]
- Papagrigoraki, A.; Del Giglio, M.; Cosma, C.; Maurelli, M.; Girolomoni, G.; Lapolla, A. Advanced glycation end products are increased in the skin and blood of patients with severe psoriasis. Acta Derm. Venereol. 2017, 97, 782–787. [Google Scholar] [CrossRef] [PubMed]
- Dreiher, J.; Weitzman, D.; Davidovici, B.; Shapiro, J.; Cohen, A.D. Psoriasis and dyslipidaemia: A population-based study. Acta Derm. Venereol. 2008, 88, 561–565. [Google Scholar] [CrossRef] [PubMed]
- Miller, I.M.; Ellervik, C.; Zarchi, K.; Ibler, K.S.; Vinding, G.R.; Knudsen, K.M.; Jemec, G.B. The association of metabolic syndrome and psoriasis: A population- and hospital-based cross-sectional study. J. Eur. Acad. Dermatol. Venereol. JEADV 2015, 29, 490–497. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.; Harskamp, C.T.; Armstrong, E.J.; Armstrong, A.W. The association between psoriasis and dyslipidaemia: A systematic review. Br. J. Dermatol. 2013, 168, 486–495. [Google Scholar] [CrossRef] [PubMed]
- Santos-Juanes, J.; Coto-Segura, P.; Fernandez-Vega, I.; Armesto, S.; Martinez-Camblor, P. Psoriasis vulgaris with or without arthritis and independent of disease severity or duration is a risk factor for hypercholesterolemia. Dermatology 2015, 230, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Sunitha, S.; Rajappa, M.; Thappa, D.M.; Chandrashekar, L.; Munisamy, M.; Revathy, G.; Priyadarssini, M. Comprehensive lipid tetrad index, atherogenic index and lipid peroxidation: Surrogate markers for increased cardiovascular risk in psoriasis. Indian J. Dermatol. Venereol. Leprol. 2015, 81, 464–471. [Google Scholar] [CrossRef] [PubMed]
- Miller, I.M.; Skaaby, T.; Ellervik, C.; Jemec, G.B. Quantifying cardiovascular disease risk factors in patients with psoriasis: A meta-analysis. Br. J. Dermatol. 2013, 169, 1180–1187. [Google Scholar] [CrossRef] [PubMed]
- Akhyani, M.; Ehsani, A.H.; Robati, R.M.; Robati, A.M. The lipid profile in psoriasis: A controlled study. J. Eur. Acad. Dermatol. Venereol. JEADV 2007, 21, 1330–1332. [Google Scholar] [CrossRef] [PubMed]
- Reynoso-von Drateln, C.; Martinez-Abundis, E.; Balcazar-Munoz, B.R.; Bustos-Saldana, R.; Gonzalez-Ortiz, M. Lipid profile, insulin secretion, and insulin sensitivity in psoriasis. J. Am. Acad. Dermatol. 2003, 48, 882–885. [Google Scholar] [CrossRef] [PubMed]
- Tom, W.L.; Playford, M.P.; Admani, S.; Natarajan, B.; Joshi, A.A.; Eichenfield, L.F.; Mehta, N.N. Characterization of lipoprotein composition and function in pediatric psoriasis reveals a more atherogenic profile. J. Investig. Dermatol. 2016, 136, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Mysliwiec, H.; Baran, A.; Harasim-Symbor, E.; Mysliwiec, P.; Milewska, A.J.; Chabowski, A.; Flisiak, I. Serum fatty acid profile in psoriasis and its comorbidity. Arch. Dermatol. Res. 2017, 309, 371–380. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Li, W.Q.; Han, J.; Sun, Q.; Qureshi, A.A. Hypercholesterolemia and risk of incident psoriasis and psoriatic arthritis in US women. Arthritis Rheumatol. 2014, 66, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Setty, A.R.; Curhan, G.; Choi, H.K. Obesity, waist circumference, weight change, and the risk of psoriasis in women: Nurses’ Health Study II. Arch. Intern. Med. 2007, 167, 1670–1675. [Google Scholar] [CrossRef] [PubMed]
- Correia, B.; Torres, T. Obesity: A key component of psoriasis. Acta Bio-Med. Atenei Parm. 2015, 86, 121–129. [Google Scholar]
- Duarte, G.V.; Silva, L.P. Correlation between psoriasis’ severity and waist-to-height ratio. Anais Brasileiros de Dermatologia 2014, 89, 846–847. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.; Smith, S.D.; Hong, E.; Garnett, S.; Fischer, G. Association between pediatric psoriasis and waist-to-height ratio in the absence of obesity: A multicenter australian study. JAMA Dermatol. 2016, 152, 1314–1319. [Google Scholar] [CrossRef] [PubMed]
- Jacobi, A.; Langenbruch, A.; Purwins, S.; Augustin, M.; Radtke, M.A. Prevalence of obesity in patients with psoriasis: Results of the national study PsoHealth3. Dermatology 2015, 231, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Fleming, P.; Kraft, J.; Gulliver, W.P.; Lynde, C. The relationship of obesity with the severity of psoriasis: A systematic review. J. Cutan. Med. Surg. 2015, 19, 450–456. [Google Scholar] [CrossRef] [PubMed]
- Gutmark-Little, I.; Shah, K.N. Obesity and the metabolic syndrome in pediatric psoriasis. Clin. Dermatol. 2015, 33, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Mahe, E.; Beauchet, A.; Bodemer, C.; Phan, A.; Bursztejn, A.C.; Boralevi, F.; Souillet, A.L.; Chiaverini, C.; Bourrat, E.; Miquel, J.; et al. Psoriasis and obesity in French children: A case-control, multicentre study. Br. J. Dermatol. 2015, 172, 1593–1600. [Google Scholar] [CrossRef] [PubMed]
- Torres, T.; Machado, S.; Mendonca, D.; Selores, M. Cardiovascular comorbidities in childhood psoriasis. Eur. J. Dermatol. EJD 2014, 24, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Paller, A.S.; Mercy, K.; Kwasny, M.J.; Choon, S.E.; Cordoro, K.M.; Girolomoni, G.; Menter, A.; Tom, W.L.; Mahoney, A.M.; Oostveen, A.M.; et al. Association of pediatric psoriasis severity with excess and central adiposity: An international cross-sectional study. JAMA Dermatol. 2013, 149, 166–176. [Google Scholar] [CrossRef] [PubMed]
- Jensen, P.; Skov, L. Psoriasis and Obesity. Dermatology 2016, 232, 633–639. [Google Scholar] [CrossRef] [PubMed]
- Danielsen, K.; Wilsgaard, T.; Olsen, A.O.; Furberg, A.S. Overweight and weight gain predict psoriasis development in a population-based cohort. Acta Derm. Venereol. 2017, 97, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Herron, M.D.; Hinckley, M.; Hoffman, M.S.; Papenfuss, J.; Hansen, C.B.; Callis, K.P.; Krueger, G.G. Impact of obesity and smoking on psoriasis presentation and management. Arch. Dermatol. 2005, 141, 1527–1534. [Google Scholar] [CrossRef] [PubMed]
- Debbaneh, M.; Millsop, J.W.; Bhatia, B.K.; Koo, J.; Liao, W. Diet and psoriasis, part I: Impact of weight loss interventions. J. Am. Acad. Dermatol. 2014, 71, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Jensen, P.; Christensen, R.; Zachariae, C.; Geiker, N.R.; Schaadt, B.K.; Stender, S.; Hansen, P.R.; Astrup, A.; Skov, L. Long-term effects of weight reduction on the severity of psoriasis in a cohort derived from a randomized trial: A prospective observational follow-up study. Am. J. Clin. Nutr. 2016, 104, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Naldi, L.; Conti, A.; Cazzaniga, S.; Patrizi, A.; Pazzaglia, M.; Lanzoni, A.; Veneziano, L.; Pellacani, G. Diet and physical exercise in psoriasis: A randomized controlled trial. Br. J. Dermatol. 2014, 170, 634–642. [Google Scholar] [CrossRef] [PubMed]
- Roongpisuthipong, W.; Pongpudpunth, M.; Roongpisuthipong, C.; Rajatanavin, N. The effect of weight loss in obese patients with chronic stable plaque-type psoriasis. Dermatol. Res. Pract. 2013, 2013, 795932. [Google Scholar] [CrossRef] [PubMed]
- Upala, S.; Sanguankeo, A. Effect of lifestyle weight loss intervention on disease severity in patients with psoriasis: A systematic review and meta-analysis. Int. J. Obes. 2015, 39, 1197–1202. [Google Scholar] [CrossRef] [PubMed]
- Babino, G.; Giunta, A.; Bianchi, L.; Esposito, M. Morbid obesity and psoriasis: Disease remission after laparoscopic sleeve gastrectomy. Obes. Res. Clin. Pract. 2017, 11, 370–372. [Google Scholar] [CrossRef] [PubMed]
- Al-Mutairi, N.; Nour, T. The effect of weight reduction on treatment outcomes in obese patients with psoriasis on biologic therapy: A randomized controlled prospective trial. Expert Opin. Biol. Ther. 2014, 14, 749–756. [Google Scholar] [CrossRef] [PubMed]
- Chiricozzi, A.; Raimondo, A.; Lembo, S.; Fausti, F.; Dini, V.; Costanzo, A.; Monfrecola, G.; Balato, N.; Ayala, F.; Romanelli, M.; et al. Crosstalk between skin inflammation and adipose tissue-derived products: Pathogenic evidence linking psoriasis to increased adiposity. Expert Rev. Clin. Immunol. 2016, 12, 1299–1308. [Google Scholar] [CrossRef] [PubMed]
- Coimbra, S.; Catarino, C.; Santos-Silva, A. The triad psoriasis-obesity-adipokine profile. J. Eur. Acad. Dermatol. Venereol. JEADV 2016, 30, 1876–1885. [Google Scholar] [CrossRef] [PubMed]
- Engin, A. The definition and prevalence of obesity and metabolic syndrome. Adv. Exp. Med. Biol. 2017, 960, 1–17. [Google Scholar] [CrossRef] [PubMed]
- De la Iglesia, R.; Loria-Kohen, V.; Zulet, M.A.; Martinez, J.A.; Reglero, G.; Ramirez de Molina, A. Dietary strategies implicated in the prevention and treatment of metabolic syndrome. Int. J. Mol. Sci. 2016, 17, 1877. [Google Scholar] [CrossRef] [PubMed]
- Danielsen, K.; Wilsgaard, T.; Olsen, A.O.; Eggen, A.E.; Olsen, K.; Cassano, P.A.; Furberg, A.S. Elevated odds of metabolic syndrome in psoriasis: A population-based study of age and sex differences. Br. J. Dermatol. 2015, 172, 419–427. [Google Scholar] [CrossRef] [PubMed]
- Milcic, D.; Jankovic, S.; Vesic, S.; Milinkovic, M.; Marinkovic, J.; Cirkovic, A.; Jankovic, J. Prevalence of metabolic syndrome in patients with psoriasis: A hospital-based cross-sectional study. Anais Brasileiros de Dermatologia 2017, 92, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Parodi, A.; Aste, N.; Calvieri, C.; Cantoresi, F.; Carlesimo, M.; Fabbri, P.; Filosa, G.; Galluccio, A.; Lisi, P.; Micali, G.; et al. Metabolic syndrome prevalence in psoriasis: A cross-sectional study in the Italian population. Am. J. Clin. Dermatol. 2014, 15, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Zuniga, M.J.M.; Cortez-Franco, F.; Quijano-Gomero, E. Association of psoriasis and metabolic syndrome in Latin America: A systematic review and meta-analysis. Actas Derm. Sifiliogr. 2017, 108, 326–334. [Google Scholar] [CrossRef]
- Malkic Salihbegovic, E.; Hadzigrahic, N.; Cickusic, A.J. Psoriasis and metabolic syndrome. Med. Arch. 2015, 69, 85–87. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Young, P.; Armstrong, A.W. Relationship between psoriasis and metabolic syndrome: A systematic review. Giornale Italiano di Dermatologia e Venereologia 2016, 151, 663–677. [Google Scholar] [PubMed]
- Kokpol, C.; Aekplakorn, W.; Rajatanavin, N. Prevalence and characteristics of metabolic syndrome in South-East Asian psoriatic patients: A case-control study. J. Dermatol. 2014, 41, 898–902. [Google Scholar] [CrossRef] [PubMed]
- Gui, X.Y.; Yu, X.L.; Jin, H.Z.; Zuo, Y.G.; Wu, C. Prevalence of metabolic syndrome in Chinese psoriasis patients: A hospital-based cross-sectional study. J. Diabetes Investig. 2017. [Google Scholar] [CrossRef] [PubMed]
- Sharma, Y.K.; Prakash, N.; Gupta, A. Prevalence of metabolic syndrome as per the NCEP and IDF definitions vis-a-vis severity and duration of psoriasis in a semi-urban Maharashtrian population: A case control study. Diabetes Metab. Syndr. 2016, 10, S72–S76. [Google Scholar] [CrossRef] [PubMed]
- Pietrzak, A.; Grywalska, E.; Walankiewicz, M.; Lotti, T.; Rolinski, J.; Myslinski, W.; Chabros, P.; Piekarska-Myslinska, D.; Reich, K. Psoriasis and metabolic syndrome in children: Current data. Clin. Exp. Dermatol. 2017, 42, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Lonnberg, A.S.; Skov, L.; Skytthe, A.; Kyvik, K.O.; Pedersen, O.B.; Thomsen, S.F. Smoking and risk for psoriasis: A population-based twin study. Int. J. Dermatol. 2016, 55, e72–e78. [Google Scholar] [CrossRef] [PubMed]
- Adamzik, K.; McAleer, M.A.; Kirby, B. Alcohol and psoriasis: Sobering thoughts. Clin. Exp. Dermatol. 2013, 38, 819–822. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, A.W.; Harskamp, C.T.; Dhillon, J.S.; Armstrong, E.J. Psoriasis and smoking: A systematic review and meta-analysis. Br. J. Dermatol. 2014, 170, 304–314. [Google Scholar] [CrossRef] [PubMed]
- Brenaut, E.; Horreau, C.; Pouplard, C.; Barnetche, T.; Paul, C.; Richard, M.A.; Joly, P.; Le Maitre, M.; Aractingi, S.; Aubin, F.; et al. Alcohol consumption and psoriasis: A systematic literature review. J. Eur. Acad. Dermatol. Venereol. JEADV 2013, 27 (Suppl. S3), 30–35. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Han, J.; Choi, H.K.; Qureshi, A.A. Smoking and risk of incident psoriasis among women and men in the United States: A combined analysis. Am. J. Epidemiol. 2012, 175, 402–413. [Google Scholar] [CrossRef] [PubMed]
- Setty, A.R.; Curhan, G.; Choi, H.K. Smoking and the risk of psoriasis in women: Nurses’ Health Study II. Am. J. Med. 2007, 120, 953–959. [Google Scholar] [CrossRef] [PubMed]
- Naldi, L.; Peli, L.; Parazzini, F. Association of early-stage psoriasis with smoking and male alcohol consumption: Evidence from an Italian case-control study. Arch. Dermatol. 1999, 135, 1479–1484. [Google Scholar] [CrossRef] [PubMed]
- Fortes, C.; Mastroeni, S.; Leffondre, K.; Sampogna, F.; Melchi, F.; Mazzotti, E.; Pasquini, P.; Abeni, D. Relationship between smoking and the clinical severity of psoriasis. Arch. Dermatol. 2005, 141, 1580–1584. [Google Scholar] [CrossRef] [PubMed]
- Richer, V.; Roubille, C.; Fleming, P.; Starnino, T.; McCourt, C.; McFarlane, A.; Siu, S.; Kraft, J.; Lynde, C.; Pope, J.E.; et al. Psoriasis and Smoking: A systematic literature review and meta-analysis with qualitative analysis of effect of smoking on psoriasis severity. J. Cutan. Med. Surg. 2016, 20, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Torii, K.; Saito, C.; Furuhashi, T.; Nishioka, A.; Shintani, Y.; Kawashima, K.; Kato, H.; Morita, A. Tobacco smoke is related to Th17 generation with clinical implications for psoriasis patients. Exp. Dermatol. 2011, 20, 371–373. [Google Scholar] [CrossRef] [PubMed]
- Ku, S.H.; Kwon, W.J.; Cho, E.B.; Park, E.J.; Kim, K.H.; Kim, K.J. The association between psoriasis area and severity index and cardiovascular risk factor in korean psoriasis patients. Ann. Dermatol. 2016, 28, 360–363. [Google Scholar] [CrossRef] [PubMed]
- Irimie, M.; Oanta, A.; Irimie, C.A.; Fekete, L.G.; Minea, D.I.; Pascu, A. Cardiovascular risk factors in patients with chronic plaque psoriasis: A case-control study on the Brasov County population. Acta Dermatovenerol. Croat. ADC 2015, 23, 28–35. [Google Scholar] [PubMed]
- Al-Mutairi, N.; Al-Farag, S.; Al-Mutairi, A.; Al-Shiltawy, M. Comorbidities associated with psoriasis: An experience from the Middle East. J. Dermatol. 2010, 37, 146–155. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, A.W.; Schupp, C.; Bebo, B. Psoriasis comorbidities: Results from the National Psoriasis Foundation surveys 2003 to 2011. Dermatology 2012, 225, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Curco, N.; Barriendos, N.; Barahona, M.J.; Arteaga, C.; Garcia, M.; Yordanov, S.; de La Barrera, O.; Prat, C.; Vives, P.; Gimenez, N. Factors influencing cardiometabolic risk profile in patients with psoriasis. Australas. J. Dermatol. 2017. [Google Scholar] [CrossRef] [PubMed]
- Itani, S.; Arabi, A.; Harb, D.; Hamzeh, D.; Kibbi, A.G. High prevalence of metabolic syndrome in patients with psoriasis in Lebanon: A prospective study. Int. J. Dermatol. 2016, 55, 390–395. [Google Scholar] [CrossRef] [PubMed]
- Hagforsen, E.; Michaelsson, K.; Lundgren, E.; Olofsson, H.; Petersson, A.; Lagumdzija, A.; Hedstrand, H.; Michaelsson, G. Women with palmoplantar pustulosis have disturbed calcium homeostasis and a high prevalence of diabetes mellitus and psychiatric disorders: A case-control study. Acta Derm. Venereol. 2005, 85, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Zhu, K.; Zhou, H.; Liu, J.; Xu, G.; Liu, W. Metabolic abnormalities are absent in patients with generalized pustular psoriasis. J. Dermatol. Sci. 2015, 78, 239–240. [Google Scholar] [CrossRef] [PubMed]
- Eder, L.; Wu, Y.; Chandran, V.; Cook, R.; Gladman, D.D. Incidence and predictors for cardiovascular events in patients with psoriatic arthritis. Ann. Rheum. Dis. 2016, 75, 1680–1686. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Hagberg, K.W.; Peng, M.; Shah, K.; Paris, M.; Jick, S. Rates of cardiovascular disease and major adverse cardiovascular events in patients with psoriatic arthritis compared to patients without psoriatic arthritis. J. Clin. Rheumatol. 2015, 21, 405–410. [Google Scholar] [CrossRef] [PubMed]
- Polachek, A.; Touma, Z.; Anderson, M.; Eder, L. Risk of Cardiovascular morbidity in patients with psoriatic arthritis: A meta-analysis of observational studies. Arthritis Care Res. 2017, 69, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Horreau, C.; Pouplard, C.; Brenaut, E.; Barnetche, T.; Misery, L.; Cribier, B.; Jullien, D.; Aractingi, S.; Aubin, F.; Joly, P.; et al. Cardiovascular morbidity and mortality in psoriasis and psoriatic arthritis: A systematic literature review. J. Eur. Acad. Dermatol. Venereol. JEADV 2013, 27 (Suppl. S3), 12–29. [Google Scholar] [CrossRef] [PubMed]
- Di Minno, M.N.; Ambrosino, P.; Lupoli, R.; di Minno, A.; Tasso, M.; Peluso, R.; Tremoli, E. Cardiovascular risk markers in patients with psoriatic arthritis: A meta-analysis of literature studies. Ann. Med. 2015, 47, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Shen, J.; Wong, K.T.; Cheng, I.T.; Shang, Q.; Li, E.K.; Wong, P.; Kun, E.W.; Law, M.Y.; Yip, R.; Yim, I.; et al. Increased prevalence of coronary plaque in patients with psoriatic arthritis without prior diagnosis of coronary artery disease. Ann. Rheum. Dis. 2017, 76, 1237–1244. [Google Scholar] [CrossRef] [PubMed]
- Eder, L.; Abji, F.; Rosen, C.F.; Chandran, V.; Gladman, D.D. The association between obesity and clinical features of psoriatic arthritis: A case-control study. J. Rheumatol. 2017, 44, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Eder, L.; Chandran, V.; Cook, R.; Gladman, D.D. The risk of developing diabetes mellitus in patients with psoriatic arthritis: A cohort study. J. Rheumatol. 2017, 44, 286–291. [Google Scholar] [CrossRef] [PubMed]
- Gulati, A.M.; Semb, A.G.; Rollefstad, S.; Romundstad, P.R.; Kavanaugh, A.; Gulati, S.; Haugeberg, G.; Hoff, M. On the HUNT for cardiovascular risk factors and disease in patients with psoriatic arthritis: Population-based data from the Nord-Trondelag Health Study. Ann. Rheum. Dis. 2016, 75, 819–824. [Google Scholar] [CrossRef] [PubMed]
- Haroon, M.; Gallagher, P.; Heffernan, E.; FitzGerald, O. High prevalence of metabolic syndrome and of insulin resistance in psoriatic arthritis is associated with the severity of underlying disease. J. Rheumatol. 2014, 41, 1357–1365. [Google Scholar] [CrossRef] [PubMed]
- Jafri, K.; Bartels, C.M.; Shin, D.; Gelfand, J.M.; Ogdie, A. Incidence and management of cardiovascular risk factors in psoriatic arthritis and rheumatoid arthritis: A population-based study. Arthritis Care Res. 2017, 69, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Chin, Y.Y.; Yu, H.S.; Li, W.C.; Ko, Y.C.; Chen, G.S.; Wu, C.S.; Lu, Y.W.; Yang, Y.H.; Lan, C.C. Arthritis as an important determinant for psoriatic patients to develop severe vascular events in Taiwan: A nation-wide study. J. Eur. Acad. Dermatol. Venereol. JEADV 2013, 27, 1262–1268. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Chen, H.; Nikamo, P.; Qi Low, H.; Helms, C.; Seielstad, M.; Liu, J.; Bowcock, A.M.; Stahle, M.; Liao, W. Association of cardiovascular and metabolic disease genes with psoriasis. J. Investig. Dermatol. 2013, 133, 836–839. [Google Scholar] [CrossRef] [PubMed]
- Wolf, N.; Quaranta, M.; Prescott, N.J.; Allen, M.; Smith, R.; Burden, A.D.; Worthington, J.; Griffiths, C.E.; Mathew, C.G.; Barker, J.N.; et al. Psoriasis is associated with pleiotropic susceptibility loci identified in type II diabetes and Crohn disease. J. Med. Genet. 2008, 45, 114–116. [Google Scholar] [CrossRef] [PubMed]
- Campalani, E.; Allen, M.H.; Fairhurst, D.; Young, H.S.; Mendonca, C.O.; Burden, A.D.; Griffiths, C.E.; Crook, M.A.; Barker, J.N.; Smith, C.H. Apolipoprotein E gene polymorphisms are associated with psoriasis but do not determine disease response to acitretin. Br. J. Dermatol. 2006, 154, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Eiris, N.; Gonzalez-Lara, L.; Santos-Juanes, J.; Queiro, R.; Coto, E.; Coto-Segura, P. Genetic variation at IL12B, IL23R and IL23A is associated with psoriasis severity, psoriatic arthritis and type 2 diabetes mellitus. J. Dermatol. Sci. 2014, 75, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Koch, M.; Baurecht, H.; Ried, J.S.; Rodriguez, E.; Schlesinger, S.; Volks, N.; Gieger, C.; Ruckert, I.M.; Heinrich, L.; Willenborg, C.; et al. Psoriasis and cardiometabolic traits: Modest association but distinct genetic architectures. J. Investig. Dermatol. 2015, 135, 1283–1293. [Google Scholar] [CrossRef] [PubMed]
- Gupta, Y.; Moller, S.; Zillikens, D.; Boehncke, W.H.; Ibrahim, S.M.; Ludwig, R.J. Genetic control of psoriasis is relatively distinct from that of metabolic syndrome and coronary artery disease. Exp. Dermatol. 2013, 22, 552–553. [Google Scholar] [CrossRef] [PubMed]
- Davidovici, B.B.; Sattar, N.; Prinz, J.; Puig, L.; Emery, P.; Barker, J.N.; van de Kerkhof, P.; Stahle, M.; Nestle, F.O.; Girolomoni, G.; et al. Psoriasis and systemic inflammatory diseases: Potential mechanistic links between skin disease and co-morbid conditions. J. Investig. Dermatol. 2010, 130, 1785–1796. [Google Scholar] [CrossRef] [PubMed]
- Spah, F. Inflammation in atherosclerosis and psoriasis: Common pathogenic mechanisms and the potential for an integrated treatment approach. Br. J. Dermatol. 2008, 159 (Suppl. S2), 10–17. [Google Scholar] [CrossRef] [PubMed]
- Hjuler, K.F.; Gormsen, L.C.; Vendelbo, M.H.; Egeberg, A.; Nielsen, J.; Iversen, L. Increased global arterial and subcutaneous adipose tissue inflammation in patients with moderate-to-severe psoriasis. Br. J. Dermatol. 2017, 176, 732–740. [Google Scholar] [CrossRef] [PubMed]
- Rose, S.; Sheth, N.H.; Baker, J.F.; Ogdie, A.; Raper, A.; Saboury, B.; Werner, T.J.; Thomas, P.; Vanvoorhees, A.; Alavi, A.; et al. A comparison of vascular inflammation in psoriasis, rheumatoid arthritis, and healthy subjects by FDG-PET/CT: A pilot study. Am. J. Cardiovasc. Dis. 2013, 3, 273–278. [Google Scholar] [PubMed]
- Youn, S.W.; Kang, S.Y.; Kim, S.A.; Park, G.Y.; Lee, W.W. Subclinical systemic and vascular inflammation detected by (18) F-fluorodeoxyglucose positron emission tomography/computed tomography in patients with mild psoriasis. J. Dermatol. 2015, 42, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Mehta, N.N.; Yu, Y.; Saboury, B.; Foroughi, N.; Krishnamoorthy, P.; Raper, A.; Baer, A.; Antigua, J.; Van Voorhees, A.S.; Torigian, D.A.; et al. Systemic and vascular inflammation in patients with moderate to severe psoriasis as measured by [18F]-fluorodeoxyglucose positron emission tomography-computed tomography (FDG-PET/CT): A pilot study. Arch. Dermatol. 2011, 147, 1031–1039. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Gao, H.; Loyd, C.M.; Fu, W.; Diaconu, D.; Liu, S.; Cooper, K.D.; McCormick, T.S.; Simon, D.I.; Ward, N.L. Chronic skin-specific inflammation promotes vascular inflammation and thrombosis. J. Investig. Dermatol. 2012, 132, 2067–2075. [Google Scholar] [CrossRef] [PubMed]
- Chodorowska, G.; Wojnowska, D.; Juszkiewicz-Borowiec, M. C-reactive protein and alpha2-macroglobulin plasma activity in medium-severe and severe psoriasis. J. Eur. Acad. Dermatol. Venereol. JEADV 2004, 18, 180–183. [Google Scholar] [CrossRef] [PubMed]
- Coimbra, S.; Oliveira, H.; Reis, F.; Belo, L.; Rocha, S.; Quintanilha, A.; Figueiredo, A.; Teixeira, F.; Castro, E.; Rocha-Pereira, P.; et al. C-reactive protein and leucocyte activation in psoriasis vulgaris according to severity and therapy. J. Eur. Acad. Dermatol. Venereol. JEADV 2010, 24, 789–796. [Google Scholar] [CrossRef] [PubMed]
- Tian, S.; Krueger, J.G.; Li, K.; Jabbari, A.; Brodmerkel, C.; Lowes, M.A.; Suarez-Farinas, M. Meta-analysis derived (MAD) transcriptome of psoriasis defines the “core” pathogenesis of disease. PLoS ONE 2012, 7, e44274. [Google Scholar] [CrossRef] [PubMed]
- Boehncke, W.H.; Boehncke, S.; Tobin, A.M.; Kirby, B. The ‘psoriatic march’: A concept of how severe psoriasis may drive cardiovascular comorbidity. Exp. Dermatol. 2011, 20, 303–307. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, A.W.; Voyles, S.V.; Armstrong, E.J.; Fuller, E.N.; Rutledge, J.C. A tale of two plaques: Convergent mechanisms of T-cell-mediated inflammation in psoriasis and atherosclerosis. Exp. Dermatol. 2011, 20, 544–549. [Google Scholar] [CrossRef] [PubMed]
- Grozdev, I.; Korman, N.; Tsankov, N. Psoriasis as a systemic disease. Clin. Dermatol. 2014, 32, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Butcher, M.; Galkina, E. Current views on the functions of interleukin-17A-producing cells in atherosclerosis. Thromb. Haemost. 2011, 106, 787–795. [Google Scholar] [CrossRef] [PubMed]
- Furuhashi, T.; Saito, C.; Torii, K.; Nishida, E.; Yamazaki, S.; Morita, A. Photo(chemo)therapy reduces circulating Th17 cells and restores circulating regulatory T cells in psoriasis. PLoS ONE 2013, 8, e54895. [Google Scholar] [CrossRef] [PubMed]
- Lo, Y.H.; Torii, K.; Saito, C.; Furuhashi, T.; Maeda, A.; Morita, A. Serum IL-22 correlates with psoriatic severity and serum IL-6 correlates with susceptibility to phototherapy. J. Dermatol. Sci. 2010, 58, 225–227. [Google Scholar] [CrossRef] [PubMed]
- Qu, Y.; Zhang, Q.; Ma, S.; Liu, S.; Chen, Z.; Mo, Z.; You, Z. Interleukin-17A differentially induces inflammatory and metabolic gene expression in the adipose tissues of lean and obese mice. Int. J. Mol. Sci. 2016, 17, 522. [Google Scholar] [CrossRef] [PubMed]
- Hashmi, S.; Zeng, Q.T. Role of interleukin-17 and interleukin-17-induced cytokines interleukin-6 and interleukin-8 in unstable coronary artery disease. Coron. Artery Dis. 2006, 17, 699–706. [Google Scholar] [CrossRef] [PubMed]
- Karbach, S.; Croxford, A.L.; Oelze, M.; Schuler, R.; Minwegen, D.; Wegner, J.; Koukes, L.; Yogev, N.; Nikolaev, A.; Reissig, S.; et al. Interleukin 17 drives vascular inflammation, endothelial dysfunction, and arterial hypertension in psoriasis-like skin disease. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 2658–2668. [Google Scholar] [CrossRef] [PubMed]
- Owczarczyk-Saczonek, A.; Placek, W. Interleukin-17 as a factor linking the pathogenesis of psoriasis with metabolic disorders. Int. J. Dermatol. 2017, 56, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Mehta, N.N.; Li, K.; Szapary, P.; Krueger, J.; Brodmerkel, C. Modulation of cardiometabolic pathways in skin and serum from patients with psoriasis. J. Trans. Med. 2013, 11, 194. [Google Scholar] [CrossRef] [PubMed]
- Furue, M.; Kadono, T. “Inflammatory skin march” in atopic dermatitis and psoriasis. Inflamm. Res. 2017. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.; Scherer, P.E. Adipokines as novel biomarkers and regulators of the metabolic syndrome. Ann. N.Y. Acad. Sci. 2010, 1212, e1–e19. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.J.; Wu, C.Y.; Shen, J.L.; Chu, S.Y.; Chen, C.K.; Chang, Y.T.; Chen, C.M. Psoriasis independently associated with hyperleptinemia contributing to metabolic syndrome. Arch. Dermatol. 2008, 144, 1571–1575. [Google Scholar] [CrossRef] [PubMed]
- Cerman, A.A.; Bozkurt, S.; Sav, A.; Tulunay, A.; Elbasi, M.O.; Ergun, T. Serum leptin levels, skin leptin and leptin receptor expression in psoriasis. Br. J. Dermatol. 2008, 159, 820–826. [Google Scholar] [CrossRef] [PubMed]
- Oh, Y.J.; Lim, H.K.; Choi, J.H.; Lee, J.W.; Kim, N.I. Serum leptin and adiponectin levels in Korean patients with psoriasis. J. Korean Med. Sci. 2014, 29, 729–734. [Google Scholar] [CrossRef] [PubMed]
- Stjernholm, T.; Ommen, P.; Langkilde, A.; Johansen, C.; Iversen, L.; Rosada, C.; Stenderup, K. Leptin deficiency in mice counteracts imiquimod (IMQ)-induced psoriasis-like skin inflammation while leptin stimulation induces inflammation in human keratinocytes. Exp. Dermatol. 2017, 26, 338–345. [Google Scholar] [CrossRef] [PubMed]
- Pina, T.; Genre, F.; Lopez-Mejias, R.; Armesto, S.; Ubilla, B.; Mijares, V.; Dierssen-Sotos, T.; Gonzalez-Lopez, M.A.; Gonzalez-Vela, M.C.; Blanco, R.; et al. Relationship of leptin with adiposity and inflammation and resistin with disease severity in psoriatic patients undergoing anti-TNF-alpha therapy. J. Eur. Acad. Dermatol. Venereol. JEADV 2015, 29, 1995–2001. [Google Scholar] [CrossRef] [PubMed]
- Robati, R.M.; Partovi-Kia, M.; Haghighatkhah, H.R.; Younespour, S.; Abdollahimajd, F. Increased serum leptin and resistin levels and increased carotid intima-media wall thickness in patients with psoriasis: Is psoriasis associated with atherosclerosis? J. Am. Acad. Dermatol. 2014, 71, 642–648. [Google Scholar] [CrossRef] [PubMed]
- Li, R.C.; Krishnamoorthy, P.; DerOhannessian, S.; Doveikis, J.; Wilcox, M.; Thomas, P.; Rader, D.J.; Reilly, M.P.; Van Voorhees, A.; Gelfand, J.M.; et al. Psoriasis is associated with decreased plasma adiponectin levels independently of cardiometabolic risk factors. Clin. Exp. Dermatol. 2014, 39, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Johnston, A.; Arnadottir, S.; Gudjonsson, J.E.; Aphale, A.; Sigmarsdottir, A.A.; Gunnarsson, S.I.; Steinsson, J.T.; Elder, J.T.; Valdimarsson, H. Obesity in psoriasis: Leptin and resistin as mediators of cutaneous inflammation. Br. J. Dermatol. 2008, 159, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Okan, G.; Baki, A.M.; Yorulmaz, E.; Dogru-Abbasoglu, S.; Vural, P. Serum visfatin, fetuin-A, and pentraxin 3 levels in patients with psoriasis and their relation to disease severity. J. Clin. Lab. Anal. 2016, 30, 284–289. [Google Scholar] [CrossRef] [PubMed]
- He, L.; Qin, S.; Dang, L.; Song, G.; Yao, S.; Yang, N.; Li, Y. Psoriasis decreases the anti-oxidation and anti-inflammation properties of high-density lipoprotein. Biochim. Biophys. Acta 2014, 1841, 1709–1715. [Google Scholar] [CrossRef] [PubMed]
- Holzer, M.; Wolf, P.; Inzinger, M.; Trieb, M.; Curcic, S.; Pasterk, L.; Weger, W.; Heinemann, A.; Marsche, G. Anti-psoriatic therapy recovers high-density lipoprotein composition and function. J. Investig. Dermatol. 2014, 134, 635–642. [Google Scholar] [CrossRef] [PubMed]
- Chua, R.A.; Arbiser, J.L. The role of angiogenesis in the pathogenesis of psoriasis. Autoimmunity 2009, 42, 574–579. [Google Scholar] [CrossRef] [PubMed]
- Sluimer, J.C.; Daemen, M.J. Novel concepts in atherogenesis: Angiogenesis and hypoxia in atherosclerosis. J. Pathol. 2009, 218, 7–29. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Lu, X.; Shi, G.P. Vasa vasorum in atherosclerosis and clinical significance. Int. J. Mol. Sci. 2015, 16, 11574–11608. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, A.W.; Voyles, S.V.; Armstrong, E.J.; Fuller, E.N.; Rutledge, J.C. Angiogenesis and oxidative stress: Common mechanisms linking psoriasis with atherosclerosis. J. Dermatol. Sci. 2011, 63, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Malecic, N.; Young, H.S. Excessive angiogenesis associated with psoriasis as a cause for cardiovascular ischaemia. Exp. Dermatol. 2017, 26, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Rocha-Pereira, P.; Santos-Silva, A.; Rebelo, I.; Figueiredo, A.; Quintanilha, A.; Teixeira, F. Dislipidemia and oxidative stress in mild and in severe psoriasis as a risk for cardiovascular disease. Clin. Chim. Acta Int. J. Clin. Chem. 2001, 303, 33–39. [Google Scholar] [CrossRef]
- He, F.; Zuo, L. Redox roles of reactive oxygen species in cardiovascular diseases. Int. J. Mol. Sci. 2015, 16, 27770–27780. [Google Scholar] [CrossRef] [PubMed]
- Baron, M.; Boulanger, C.M.; Staels, B.; Tailleux, A. Cell-derived microparticles in atherosclerosis: Biomarkers and targets for pharmacological modulation? J. Cell. Mol. Med. 2012, 16, 1365–1376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takeshita, J.; Mohler, E.R.; Krishnamoorthy, P.; Moore, J.; Rogers, W.T.; Zhang, L.; Gelfand, J.M.; Mehta, N.N. Endothelial cell-, platelet-, and monocyte/macrophage-derived microparticles are elevated in psoriasis beyond cardiometabolic risk factors. J. Am. Heart Assoc. 2014, 3, e000507. [Google Scholar] [CrossRef] [PubMed]
- Tamagawa-Mineoka, R.; Katoh, N.; Kishimoto, S. Platelet activation in patients with psoriasis: Increased plasma levels of platelet-derived microparticles and soluble P-selectin. J. Am. Acad. Dermatol. 2010, 62, 621–626. [Google Scholar] [CrossRef] [PubMed]
- Papadavid, E.; Diamanti, K.; Spathis, A.; Varoudi, M.; Andreadou, I.; Gravanis, K.; Theodoropoulos, K.; Karakitsos, P.; Lekakis, J.; Rigopoulos, D.; et al. Increased levels of circulating platelet-derived microparticles in psoriasis: Possible implications for the associated cardiovascular risk. World J. Cardiol. 2016, 8, 667–675. [Google Scholar] [CrossRef] [PubMed]
- Kasperska-Zajac, A.; Brzoza, Z.; Rogala, B. Platelet function in cutaneous diseases. Platelets 2008, 19, 317–321. [Google Scholar] [CrossRef] [PubMed]
- Chandrashekar, L.; Rajappa, M.; Revathy, G.; Sundar, I.; Munisamy, M.; Ananthanarayanan, P.H.; Thappa, D.M.; Basu, D. Is enhanced platelet activation the missing link leading to increased cardiovascular risk in psoriasis? Clin. Chim. Acta Int. J. Clin. Chem. 2015, 446, 181–185. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, H.J.; Christensen, I.J.; Svendsen, M.N.; Hansen, U.; Werther, K.; Brunner, N.; Petersen, L.J.; Kristensen, J.K. Elevated plasma levels of vascular endothelial growth factor and plasminogen activator inhibitor-1 decrease during improvement of psoriasis. Inflamm. Res. 2002, 51, 563–567. [Google Scholar] [CrossRef] [PubMed]
- Graham, I.M.; Daly, L.E.; Refsum, H.M.; Robinson, K.; Brattstrom, L.E.; Ueland, P.M.; Palma-Reis, R.J.; Boers, G.H.; Sheahan, R.G.; Israelsson, B.; et al. Plasma homocysteine as a risk factor for vascular disease. The European Concerted Action Project. JAMA 1997, 277, 1775–1781. [Google Scholar] [CrossRef] [PubMed]
- Skovierova, H.; Vidomanova, E.; Mahmood, S.; Sopkova, J.; Drgova, A.; Cervenova, T.; Halasova, E.; Lehotsky, J. The molecular and cellular effect of homocysteine metabolism imbalance on human health. Int. J. Mol. Sci. 2016, 17, 1733. [Google Scholar] [CrossRef] [PubMed]
- Malerba, M.; Gisondi, P.; Radaeli, A.; Sala, R.; Calzavara Pinton, P.G.; Girolomoni, G. Plasma homocysteine and folate levels in patients with chronic plaque psoriasis. Br. J. Dermatol. 2006, 155, 1165–1169. [Google Scholar] [CrossRef] [PubMed]
- Gerdes, S.; Osadtschy, S.; Buhles, N.; Baurecht, H.; Mrowietz, U. Cardiovascular biomarkers in patients with psoriasis. Exp. Dermatol. 2014, 23, 322–325. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, H.; Iinuma, S.; Honma, M.; Iizuka, H. Increased serum C-reactive protein level in Japanese patients of psoriasis with cardio- and cerebrovascular disease. J. Dermatol. 2014, 41, 981–985. [Google Scholar] [CrossRef] [PubMed]
- Erturan, I.; Koroglu, B.K.; Adiloglu, A.; Ceyhan, A.M.; Akkaya, V.B.; Tamer, N.; Basak, P.Y.; Korkmaz, S.; Ersoy, I.H.; Kilinc, O. Evaluation of serum sCD40L and homocysteine levels with subclinical atherosclerosis indicators in patients with psoriasis: A pilot study. Int. J. Dermatol. 2014, 53, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Baran, A.; Mysliwiec, H.; Szterling-Jaworowska, M.; Kiluk, P.; Swiderska, M.; Flisiak, I. Serum YKL-40 as a potential biomarker of inflammation in psoriasis. J. Dermatol. Treat. 2017, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Joshi, A.A.; Lerman, J.B.; Aberra, T.M.; Afshar, M.; Teague, H.L.; Rodante, J.A.; Krishnamoorthy, P.; Ng, Q.; Aridi, T.Z.; Salahuddin, T.; et al. GlycA is a novel biomarker of inflammation and subclinical cardiovascular disease in psoriasis. Circ. Res. 2016, 119, 1242–1253. [Google Scholar] [CrossRef] [PubMed]
- Torres, T.; Bettencourt, N.; Mendonca, D.; Vasconcelos, C.; Silva, B.M.; Selores, M. Complement C3 as a marker of cardiometabolic risk in psoriasis. Arch. Dermatol. Res. 2014, 306, 653–660. [Google Scholar] [CrossRef] [PubMed]
- Yurtdas, M.; Yaylali, Y.T.; Kaya, Y.; Ozdemir, M.; Ozkan, I.; Aladag, N. Neutrophil-to-lymphocyte ratio may predict subclinical atherosclerosis in patients with psoriasis. Echocardiography 2014, 31, 1095–1104. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.S.; Shin, D.; Lee, M.S.; Kim, H.J.; Kim, D.Y.; Kim, S.M.; Lee, M.G. Assessments of neutrophil to lymphocyte ratio and platelet to lymphocyte ratio in Korean patients with psoriasis vulgaris and psoriatic arthritis. J. Dermatol. 2016, 43, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Cao, L.Y.; Soler, D.C.; Debanne, S.M.; Grozdev, I.; Rodriguez, M.E.; Feig, R.L.; Carman, T.L.; Gilkeson, R.C.; Orringer, C.E.; Kern, E.F.; et al. Psoriasis and cardiovascular risk factors: Increased serum myeloperoxidase and corresponding immunocellular overexpression by Cd11b(+) CD68(+) macrophages in skin lesions. Am. J. Transl. Res. 2013, 6, 16–27. [Google Scholar] [PubMed]
- Menter, A.; Korman, N.J.; Elmets, C.A.; Feldman, S.R.; Gelfand, J.M.; Gordon, K.B.; Gottlieb, A.B.; Koo, J.Y.; Lebwohl, M.; Lim, H.W.; et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: Section 4. Guidelines of care for the management and treatment of psoriasis with traditional systemic agents. J. Am. Acad. Dermatol. 2009, 61, 451–485. [Google Scholar] [CrossRef] [PubMed]
- Mehta, D.; Lim, H.W. Ultraviolet B phototherapy for psoriasis: review of practical guidelines. Am. J. Clin. Dermatol. 2016, 17, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Hugh, J.; Van Voorhees, A.S.; Nijhawan, R.I.; Bagel, J.; Lebwohl, M.; Blauvelt, A.; Hsu, S.; Weinberg, J.M. From the Medical Board Of The National Psoriasis Foundation: The risk of cardiovascular disease in individuals with psoriasis and the potential impact of current therapies. J. Am. Acad. Dermatol. 2014, 70, 168–177. [Google Scholar] [CrossRef] [PubMed]
- Sigurdardottir, G.; Ekman, A.K.; Stahle, M.; Bivik, C.; Enerback, C. Systemic treatment and narrowband ultraviolet B differentially affect cardiovascular risk markers in psoriasis. J. Am. Acad. Dermatol. 2014, 70, 1067–1075. [Google Scholar] [CrossRef] [PubMed]
- Churton, S.; Brown, L.; Shin, T.M.; Korman, N.J. Does treatment of psoriasis reduce the risk of cardiovascular disease? Drugs 2014, 74, 169–182. [Google Scholar] [CrossRef] [PubMed]
- Prodanovich, S.; Ma, F.; Taylor, J.R.; Pezon, C.; Fasihi, T.; Kirsner, R.S. Methotrexate reduces incidence of vascular diseases in veterans with psoriasis or rheumatoid arthritis. J. Am. Acad. Dermatol. 2005, 52, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Ahlehoff, O.; Skov, L.; Gislason, G.; Gniadecki, R.; Iversen, L.; Bryld, L.E.; Lasthein, S.; Lindhardsen, J.; Kristensen, S.L.; Torp-Pedersen, C.; et al. Cardiovascular outcomes and systemic anti-inflammatory drugs in patients with severe psoriasis: 5-year follow-up of a Danish nationwide cohort. J. Eur. Acad. Dermatol. Venereol. JEADV 2015, 29, 1128–1134. [Google Scholar] [CrossRef] [PubMed]
- Gulliver, W.P.; Young, H.M.; Bachelez, H.; Randell, S.; Gulliver, S.; Al-Mutairi, N. Psoriasis patients treated with biologics and methotrexate have a reduced rate of myocardial infarction: A collaborative analysis using international cohorts. J. Cutan. Med. Surg. 2016, 20, 550–554. [Google Scholar] [CrossRef] [PubMed]
- Ahlehoff, O.; Skov, L.; Gislason, G.; Lindhardsen, J.; Kristensen, S.L.; Iversen, L.; Lasthein, S.; Gniadecki, R.; Dam, T.N.; Torp-Pedersen, C.; et al. Cardiovascular disease event rates in patients with severe psoriasis treated with systemic anti-inflammatory drugs: A Danish real-world cohort study. J. Intern. Med. 2013, 273, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Mahmoudi, M.J.; Saboor-Yaraghi, A.A.; Zabetian-Targhi, F.; Siassi, F.; Zarnani, A.H.; Eshraghian, M.R.; Shokri, F.; Rezaei, N.; Kalikias, Y.; Mahmoudi, M. Vitamin A decreases cytotoxicity of oxidized low-density lipoprotein in patients with atherosclerosis. Immunol. Investig. 2016, 45, 52–62. [Google Scholar] [CrossRef] [PubMed]
- Zhou, W.; Lin, J.; Chen, H.; Wang, J.; Liu, Y.; Xia, M. Retinoic acid induces macrophage cholesterol efflux and inhibits atherosclerotic plaque formation in apoE-deficient mice. Br. J. Nutr. 2015, 114, 509–518. [Google Scholar] [CrossRef] [PubMed]
- Relevy, N.Z.; Harats, D.; Harari, A.; Ben-Amotz, A.; Bitzur, R.; Ruhl, R.; Shaish, A. Vitamin A-deficient diet accelerated atherogenesis in apolipoprotein E(-/-) mice and dietary beta-carotene prevents this consequence. BioMed Res. Int. 2015, 2015, 758723. [Google Scholar] [CrossRef] [PubMed]
- Mottaghi, A.; Ebrahimof, S.; Angoorani, P.; Saboor-Yaraghi, A.A. Vitamin A supplementation reduces IL-17 and RORc gene expression in atherosclerotic patients. Scand. J. Immunol. 2014, 80, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Bilbija, D.; Elmabsout, A.A.; Sagave, J.; Haugen, F.; Bastani, N.; Dahl, C.P.; Gullestad, L.; Sirsjo, A.; Blomhoff, R.; Valen, G. Expression of retinoic acid target genes in coronary artery disease. Int. J. Mol. Med. 2014, 33, 677–686. [Google Scholar] [CrossRef] [PubMed]
- Mottaghi, A.; Salehi, E.; Keshvarz, A.; Sezavar, H.; Saboor-Yaraghi, A.A. The influence of vitamin A supplementation on Foxp3 and TGF-beta gene expression in atherosclerotic patients. J. Nutrigenet. Nutrigenom. 2012, 5, 314–326. [Google Scholar] [CrossRef] [PubMed]
- Zhou, B.; Pan, Y.; Hu, Z.; Wang, X.; Han, J.; Zhou, Q.; Zhai, Z.; Wang, Y. All-trans-retinoic acid ameliorated high fat diet-induced atherosclerosis in rabbits by inhibiting platelet activation and inflammation. J. Biomed. Biotechnol. 2012, 2012, 259693. [Google Scholar] [CrossRef] [PubMed]
- Abuabara, K.; Lee, H.; Kimball, A.B. The effect of systemic psoriasis therapies on the incidence of myocardial infarction: A cohort study. Br. J. Dermatol. 2011, 165, 1066–1073. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.J.; Poon, K.Y.; Channual, J.C.; Shen, A.Y. Association between tumor necrosis factor inhibitor therapy and myocardial infarction risk in patients with psoriasis. Arch. Dermatol. 2012, 148, 1244–1250. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.J.; Poon, K.Y. Association of ethnicity, tumor necrosis factor inhibitor therapy, and myocardial infarction risk in patients with psoriasis. J. Am. Acad. Dermatol. 2013, 69, 167–168. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.J.; Poon, K.Y.; Bebchuk, J.D. Association between the type and length of tumor necrosis factor inhibitor therapy and myocardial infarction risk in patients with psoriasis. J. Drugs Dermatol. JDD 2013, 12, 899–903. [Google Scholar]
- Wu, J.J.; Poon, K.Y.; Bebchuk, J.D. Tumor necrosis factor inhibitor therapy and myocardial infarction risk in patients with psoriasis, psoriatic arthritis, or both. J. Drugs Dermatol. JDD 2014, 13, 932–934. [Google Scholar] [PubMed]
- Wu, J.J.; Guerin, A.; Sundaram, M.; Dea, K.; Cloutier, M.; Mulani, P. Cardiovascular event risk assessment in psoriasis patients treated with tumor necrosis factor-alpha inhibitors versus methotrexate. J. Am. Acad. Dermatol. 2017, 76, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Boehncke, S.; Fichtlscherer, S.; Salgo, R.; Garbaraviciene, J.; Beschmann, H.; Diehl, S.; Hardt, K.; Thaci, D.; Boehncke, W.H. Systemic therapy of plaque-type psoriasis ameliorates endothelial cell function: Results of a prospective longitudinal pilot trial. Arch. Dermatol. Res. 2011, 303, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Schmieder, A.; Poppe, M.; Hametner, C.; Meyer-Schraml, H.; Schaarschmidt, M.L.; Findeisen, P.; Benoit, S.; Bauer, B.; Schmid, S.; Goebeler, M.; et al. Impact of fumaric acid esters on cardiovascular risk factors and depression in psoriasis: A prospective pilot study. Arch. Dermatol. Res. 2015, 307, 413–424. [Google Scholar] [CrossRef] [PubMed]
- Famenini, S.; Sako, E.Y.; Wu, J.J. Effect of treating psoriasis on cardiovascular co-morbidities: Focus on TNF inhibitors. Am. J. Clin. Dermatol. 2014, 15, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.; Wu, J.J. Relationship between tumor necrosis factor-alpha inhibitors and cardiovascular disease in psoriasis: A review. Perm. J. 2014, 18, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Shaaban, D.; Al-Mutairi, N. The effect of tumour necrosis factor inhibitor therapy on the incidence of myocardial infarction in patients with psoriasis: A retrospective study. J. Dermatol. Treat. 2016. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.S.; Lin, N.N.; Li, L.; Li, Y. The effect of TNF inhibitors on cardiovascular events in psoriasis and psoriatic arthritis: An updated meta-analysis. Clin. Rev. Allergy Immunol. 2016, 51, 240–247. [Google Scholar] [CrossRef] [PubMed]
- Piaserico, S.; Osto, E.; Famoso, G.; Zanetti, I.; Gregori, D.; Poretto, A.; Iliceto, S.; Peserico, A.; Tona, F. Treatment with tumor necrosis factor inhibitors restores coronary microvascular function in young patients with severe psoriasis. Atherosclerosis 2016, 251, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Hjuler, K.F.; Bottcher, M.; Vestergaard, C.; Botker, H.E.; Iversen, L.; Kragballe, K. Association between changes in coronary artery disease progression and treatment with biologic agents for severe psoriasis. JAMA Dermatol. 2016, 152, 1114–1121. [Google Scholar] [CrossRef] [PubMed]
- Pina, T.; Corrales, A.; Lopez-Mejias, R.; Armesto, S.; Gonzalez-Lopez, M.A.; Gomez-Acebo, I.; Ubilla, B.; Remuzgo-Martinez, S.; Gonzalez-Vela, M.C.; Blanco, R.; et al. Anti-tumor necrosis factor-alpha therapy improves endothelial function and arterial stiffness in patients with moderate to severe psoriasis: A 6-month prospective study. J. Dermatol. 2016, 43, 1267–1272. [Google Scholar] [CrossRef] [PubMed]
- Bissonnette, R.; Harel, F.; Krueger, J.G.; Guertin, M.C.; Chabot-Blanchet, M.; Gonzalez, J.; Maari, C.; Delorme, I.; Lynde, C.W.; Tardif, J.C. TNF-alpha antagonist and vascular inflammation in patients with psoriasis vulgaris: A randomized placebo-controlled study. J. Investig. Dermatol. 2017. [Google Scholar] [CrossRef] [PubMed]
- Solomon, D.H.; Massarotti, E.; Garg, R.; Liu, J.; Canning, C.; Schneeweiss, S. Association between disease-modifying antirheumatic drugs and diabetes risk in patients with rheumatoid arthritis and psoriasis. JAMA 2011, 305, 2525–2531. [Google Scholar] [CrossRef] [PubMed]
- Al-Mutairi, N.; Shabaan, D. Effects of tumor necrosis factor alpha inhibitors extend beyond psoriasis: Insulin sensitivity in psoriasis patients with type 2 diabetes mellitus. Cutis 2016, 97, 235–241. [Google Scholar] [PubMed]
- Pina, T.; Armesto, S.; Lopez-Mejias, R.; Genre, F.; Ubilla, B.; Gonzalez-Lopez, M.A.; Gonzalez-Vela, M.C.; Corrales, A.; Blanco, R.; Garcia-Unzueta, M.T.; et al. Anti-TNF-alpha therapy improves insulin sensitivity in non-diabetic patients with psoriasis: A 6-month prospective study. J. Eur. Acad. Dermatol. Venereol. JEADV 2015, 29, 1325–1330. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.J.; Rowan, C.G.; Bebchuk, J.D.; Anthony, M.S. No association between TNF inhibitor and methotrexate therapy versus methotrexate in changes in hemoglobin A1C and fasting glucose among psoriasis, psoriatic arthritis, and rheumatoid arthritis patients. J. Drugs Dermatol. JDD 2015, 14, 159–166. [Google Scholar] [PubMed]
- Gisondi, P.; Cotena, C.; Tessari, G.; Girolomoni, G. Anti-tumour necrosis factor-alpha therapy increases body weight in patients with chronic plaque psoriasis: A retrospective cohort study. J. Eur. Acad. Dermatol. Venereol. JEADV 2008, 22, 341–344. [Google Scholar] [CrossRef] [PubMed]
- Renzo, L.D.; Saraceno, R.; Schipani, C.; Rizzo, M.; Bianchi, A.; Noce, A.; Esposito, M.; Tiberti, S.; Chimenti, S.; A, D.E.L. Prospective assessment of body weight and body composition changes in patients with psoriasis receiving anti-TNF-alpha treatment. Dermatol. Ther. 2011, 24, 446–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saraceno, R.; Schipani, C.; Mazzotta, A.; Esposito, M.; di Renzo, L.; de Lorenzo, A.; Chimenti, S. Effect of anti-tumor necrosis factor-alpha therapies on body mass index in patients with psoriasis. Pharmacol. Res. 2008, 57, 290–295. [Google Scholar] [CrossRef] [PubMed]
- Gkalpakiotis, S.; Arenbergerova, M.; Gkalpakioti, P.; Potockova, J.; Arenberger, P.; Kraml, P. Impact of adalimumab treatment on cardiovascular risk biomarkers in psoriasis: Results of a pilot study. J. Dermatol. 2017, 44, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Genre, F.; Armesto, S.; Corrales, A.; Lopez-Mejias, R.; Remuzgo-Martinez, S.; Pina, T.; Ubilla, B.; Mijares, V.; Martin-Varillas, J.L.; Rueda-Gotor, J.; et al. Significant sE-Selectin levels reduction after 6 months of anti-TNF-alpha therapy in non-diabetic patients with moderate-to-severe psoriasis. J. Dermatol. Treat. 2017, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Strober, B.; Teller, C.; Yamauchi, P.; Miller, J.L.; Hooper, M.; Yang, Y.C.; Dann, F. Effects of etanercept on C-reactive protein levels in psoriasis and psoriatic arthritis. Br. J. Dermatol. 2008, 159, 322–330. [Google Scholar] [CrossRef] [PubMed]
- Kanelleas, A.; Liapi, C.; Katoulis, A.; Stavropoulos, P.; Avgerinou, G.; Georgala, S.; Economopoulos, T.; Stavrianeas, N.G.; Katsambas, A. The role of inflammatory markers in assessing disease severity and response to treatment in patients with psoriasis treated with etanercept. Clin. Exp. Dermatol. 2011, 36, 845–850. [Google Scholar] [CrossRef] [PubMed]
- Campanati, A.; Ganzetti, G.; Giuliodori, K.; Marra, M.; Bonfigli, A.; Testa, R.; Offidani, A. Serum levels of adipocytokines in psoriasis patients receiving tumor necrosis factor-alpha inhibitors: Results of a retrospective analysis. Int. J. Dermatol. 2015, 54, 839–845. [Google Scholar] [CrossRef] [PubMed]
- Pelletier, F.; Garnache-Ottou, F.; Biichle, S.; Vivot, A.; Humbert, P.; Saas, P.; Seilles, E.; Aubin, F. Effects of anti-TNF-alpha agents on circulating endothelial-derived and platelet-derived microparticles in psoriasis. Exp. Dermatol. 2014, 23, 924–925. [Google Scholar] [CrossRef] [PubMed]
- Ryan, C.; Leonardi, C.L.; Krueger, J.G.; Kimball, A.B.; Strober, B.E.; Gordon, K.B.; Langley, R.G.; de Lemos, J.A.; Daoud, Y.; Blankenship, D.; et al. Association between biologic therapies for chronic plaque psoriasis and cardiovascular events: A meta-analysis of randomized controlled trials. JAMA 2011, 306, 864–871. [Google Scholar] [CrossRef] [PubMed]
- Tzellos, T.; Kyrgidis, A.; Zouboulis, C.C. Re-evaluation of the risk for major adverse cardiovascular events in patients treated with anti-IL-12/23 biological agents for chronic plaque psoriasis: A meta-analysis of randomized controlled trials. J. Eur. Acad. Dermatol. Venereol. JEADV 2013, 27, 622–627. [Google Scholar] [CrossRef] [PubMed]
- Papp, K.A.; Griffiths, C.E.; Gordon, K.; Lebwohl, M.; Szapary, P.O.; Wasfi, Y.; Chan, D.; Hsu, M.C.; Ho, V.; Ghislain, P.D.; et al. Long-term safety of ustekinumab in patients with moderate-to-severe psoriasis: Final results from 5 years of follow-up. Br. J. Dermatol. 2013, 168, 844–854. [Google Scholar] [CrossRef] [PubMed]
- Rungapiromnan, W.; Yiu, Z.Z.N.; Warren, R.B.; Griffiths, C.E.M.; Ashcroft, D.M. Impact of biologic therapies on risk of major adverse cardiovascular events in patients with psoriasis: Systematic review and meta-analysis of randomized controlled trials. Br. J. Dermatol. 2017, 176, 890–901. [Google Scholar] [CrossRef] [PubMed]
- Reich, K.; Langley, R.G.; Lebwohl, M.; Szapary, P.; Guzzo, C.; Yeilding, N.; Li, S.; Hsu, M.C.; Griffiths, C.E. Cardiovascular safety of ustekinumab in patients with moderate to severe psoriasis: Results of integrated analyses of data from phase II and III clinical studies. Br. J. Dermatol. 2011, 164, 862–872. [Google Scholar] [CrossRef] [PubMed]
- Ikonomidis, I.; Papadavid, E.; Makavos, G.; Andreadou, I.; Varoudi, M.; Gravanis, K.; Theodoropoulos, K.; Pavlidis, G.; Triantafyllidi, H.; Moutsatsou, P.; et al. Lowering interleukin-12 activity improves myocardial and vascular function compared with tumor necrosis factor-a antagonism or cyclosporine in psoriasis. Circ. Cardiovasc Imaging 2017, 10. [Google Scholar] [CrossRef] [PubMed]
- Ng, C.Y.; Tzeng, I.S.; Liu, S.H.; Chang, Y.C.; Huang, Y.H. Metabolic parameters in psoriatic patients treated with interleukin-12/23 blockade (ustekinumab). J. Dermatol. 2017. [Google Scholar] [CrossRef] [PubMed]
- Van de Kerkhof, P.C.; Griffiths, C.E.; Reich, K.; Leonardi, C.L.; Blauvelt, A.; Tsai, T.F.; Gong, Y.; Huang, J.; Papavassilis, C.; Fox, T. Secukinumab long-term safety experience: A pooled analysis of 10 phase II and III clinical studies in patients with moderate to severe plaque psoriasis. J. Am. Acad. Dermatol. 2016, 75, 83–98. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.; Hou, S.Y.; Zhao, S.; Hou, L.X.; Jiao, T.; Xu, N.N.; Zhang, N. Efficacy and safety of interleukin-17 antagonists in patients with plaque psoriasis: A meta-analysis from phase 3 randomized controlled trials. J. Eur. Acad. Dermatol. Venereol. JEADV 2017, 31, 992–1003. [Google Scholar] [CrossRef] [PubMed]
- Torres, T.; Raposo, I.; Selores, M. IL-17 blockade in psoriasis: Friend or foe in cardiovascular risk? Am. J. Clin. Dermatol. 2016, 17, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Deeks, E.D. Apremilast: A review in psoriasis and psoriatic arthritis. Drugs 2015, 75, 1393–1403. [Google Scholar] [CrossRef] [PubMed]
- Crowley, J.; Thaci, D.; Joly, P.; Peris, K.; Papp, K.A.; Goncalves, J.; Day, R.M.; Chen, R.; Shah, K.; Ferrandiz, C.; et al. Long-term safety and tolerability of apremilast in patients with psoriasis: Pooled safety analysis for >/= 156 weeks from 2 phase 3, randomized, controlled trials (ESTEEM 1 and 2). J. Am. Acad. Dermatol. 2017, 77, 310–317. [Google Scholar] [CrossRef] [PubMed]
- Kavanaugh, A.; Mease, P.J.; Gomez-Reino, J.J.; Adebajo, A.O.; Wollenhaupt, J.; Gladman, D.D.; Lespessailles, E.; Hall, S.; Hochfeld, M.; Hu, C.; et al. Treatment of psoriatic arthritis in a phase 3 randomised, placebo-controlled trial with apremilast, an oral phosphodiesterase 4 inhibitor. Ann. Rheum. Dis. 2014, 73, 1020–1026. [Google Scholar] [CrossRef] [PubMed]

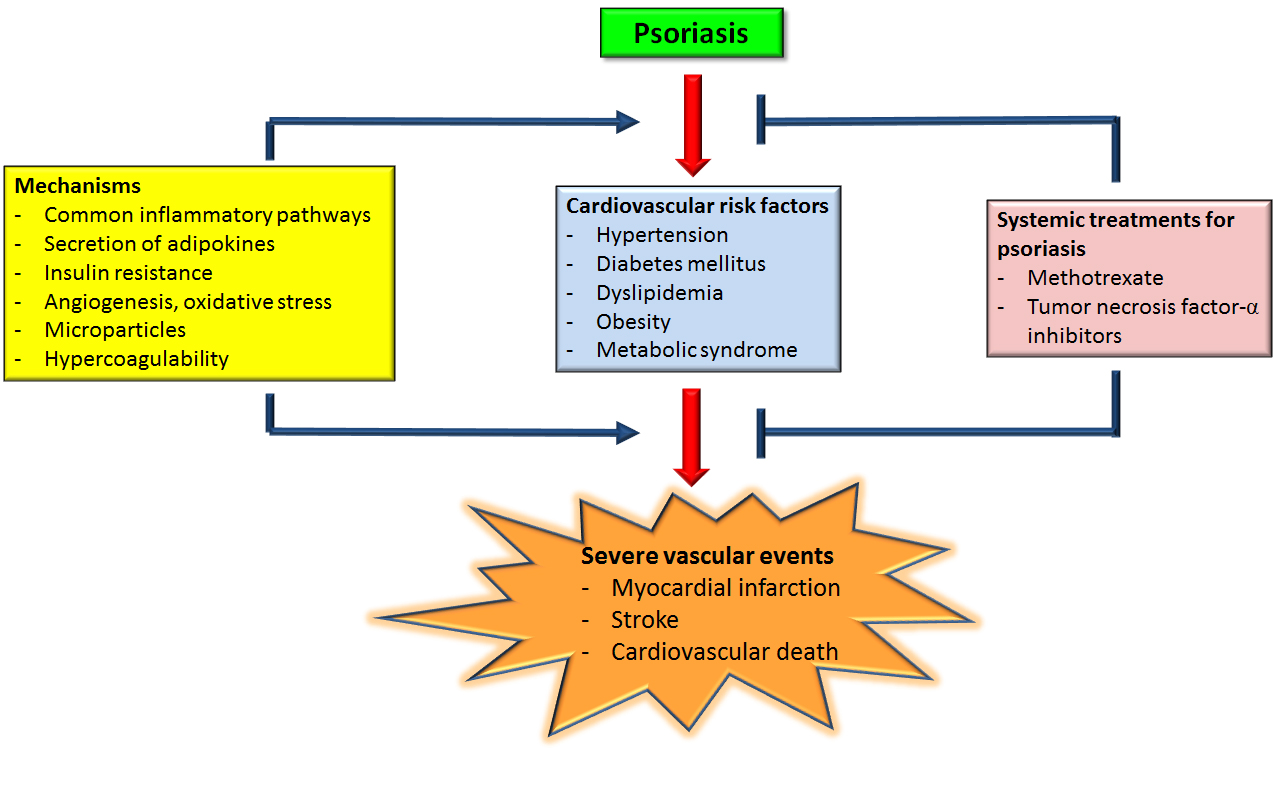{kind=link}
| Study | Cardiovascular Comorbidities | Number of Patients/Controls | Relative Risk | Population/Type of Study |
|---|---|---|---|---|
| Abuabara et al., 2010 [32] | Cardiovascular death | Severe psoriasis: 3603; Controls: 14,330 | Hazard ratio: 1.57 (95% CI 1.26–1.96) | United Kingdom/Cohort study |
| Ahlehoff et al., 2011 [41] | Composite endpoint (myocardial infarction, stroke and cardiovascular death) | Mild psoriasis: 34,371; Severe psoriasis: 2621; Controls: 4,003,265 | Rate ratio: Composite endpoint: Mild psoriasis: 1.20 (95% CI 1.14–1.25); Severe psoriasis: 1.58 (95% CI 1.36–1.82); Stroke: Mild psoriasis: 1.25 (95% CI 1.16–1.33); Severe psoriasis: 1.71 (95% CI 1.39–2.11); Myocardial infarction: Mild psoriasis: 1.22 (95% CI 1.12–1.33); Severe psoriasis: 1.45 (95% CI 1.10–1.90); Cardiovascular death: Mild psoriasis: 1.14 (95% CI 1.06–1.22); Severe psoriasis 1.57 (95% CI 1.27–1.94) | Denmark/Cohort study |
| Ahlehoff et al., 2011 [47] | Composite cardiovascular endpoint (recurrent myocardial infarction, stroke and cardiovascular death) after first time myocardial infarction | Patients with first time myocardial infarction; Psoriasis: 462; Controls: 48,935 | Hazard ratio: 1.26 (95% CI 1.06–1.54) | Denmark/Cohort study |
| Ahlehoff et al., 2012 [40] | Ischemic stroke | Mild psoriasis: 36,765; Severe psoriasis: 2793; Controls: 4,478,926 | Rate ratio: Age < 50 years: Mild psoriasis: 1.97 (95% CI 1.66–2.34); Severe psoriasis: 2.80 (95% CI 1.81–4.34); Age ≥ 50 years: Mild psoriasis: 1.13 (95% CI 1.04–1.21); Severe psoriasis: 1.34 (95% CI 1.04–1.71) | Denmark/Cohort study |
| Brauchli et al., 2009 [44] | Myocardial infarction, stroke or transient ischemic attack | Psoriasis: 36,702; Controls: 36,702 | Odds ratio: Myocardial infarction: Overall: 1.14 (95% CI 0.93–1.41); Age < 60 years: 1.66 (95% CI 1.03–2.66); Age ≥ 60 years: 0.99 (95% CI 0.77–1.26); Stroke: Overall: 0.93 (95% CI 0.77–1.13); Age < 60 years: 0.52 (95% CI 0.29–0.93); Age ≥ 60 years: 0.99 (95% CI 0.80–1.22); Transient ischemic attack: Overall: 1.00 (95% CI 0.81–1.25); Age < 60 years: 1.28 (95% CI 0.61–2.68); Age ≥ 60 years: 1.02 (95% CI 0.80–1.29) | United Kingdom/Inception cohort study with nested case-control analysis |
| Chiang et al., 2012 [39] | Ischemic stroke | Psoriasis: 2783; Controls: 13,910 | Hazard ratio: 1.27 (95% CI 1.05–1.52) | Taiwan/Retrospective cohort study |
| Dowlatshahi et al., 2013 [35] | Cardiovascular disease (coronary heart disease, stroke, heart failure) | Psoriasis: 262; Controls: 8009 | Hazard ratio: 0.73 (95% CI 0.50–1.06) | Netherlands/Prospective cohort study |
| Dregan et al., 2014 [45] | Coronary heart disease Stroke | Severe psoriasis: 5648; Mild psoriasis: 85,232; Controls: 373,851 | Hazard ratio: Mild psoriasis: Stroke: 1.08 (95% CI 0.98–1.18); Coronary heart disease: 1.03 (95% CI 0.97–1.11); Severe psoriasis: Stroke: 0.93 (95% CI 0.64–1.36); Coronary heart disease: 1.29 (95% CI 1.01–1.64) | United Kingdom/Cohort study |
| Egeberg et al., 2017 [12] | Myocardial infarction | Mild psoriasis: 49,646; Severe psoriasis: 11,957; Controls: 4,300,085 | Hazard ratio: Mild psoriasis: 1.02 (95% CI 0.96–1.09); Severe psoriasis: 1.21 (95% CI 1.07–1.37) | Denmark/Cohort study |
| Gelfand et al., 2006 [3] | Myocardial infarction | Mild psoriasis: 127,139; Severe psoriasis: 3837; Controls: 556,995 | Relative risk: 30-year-old: Mild psoriasis: 1.29 (95% CI 1.14–1.46); Severe psoriasis: 3.10 (95% CI 1.98–4.86); 60-year-old: Mild psoriasis: 1.08 (95% CI 1.03–1.13); Severe psoriasis: 1.36 (95% CI 1.13–1.64) | United Kingdom/Prospective cohort study |
| Gelfand et al., 2009 [11] | Stroke | Mild psoriasis: 129,143 (controls: 496,666); Severe psoriasis: 3603 (controls 14,330) | Hazard ratio: Mild psoriasis: 1.06 (95% CI 1.0–1.1); Severe psoriasis: 1.43 (95% CI 1.1–1.9) | United Kingdom/Cohort study |
| Kaye et al., 2008 [8] | Myocardial infarction Stroke | Psoriasis: 44,164; Controls: 219,784 | Hazard ratio: Myocardial infarction: 1.21 (95% CI 1.10–1.32); Stroke: 1.12 (95% CI 1.00–1.25) | United Kingdom/Cohort study |
| Lai et al., 2016 [27] | Myocardial infarction Ischemic heart disease Stroke | Psoriasis: 520; Total subjects: 19,065 | Odds ratio: Myocardial infarction: 2.24 (95% CI 1.27–3.95); Ischemic heart disease: 1.90 (95% CI 1.18–3.05); Stroke: 1.01 (95% CI 0.48–2.16) | United States/Cross-sectional study |
| Lan et al., 2012 [48] | Cerebrovascular disease | Psoriasis: 8180; Controls: 163,600 | Hazard ratio: 1.28 (95% CI 1.162–1.413) | Taiwan/Retrospective cohort study |
| Levesque et al., 2013 [29] | Myocardial infarction | Psoriasis: 31,421; Controls: 31,421 | Hazard ratio: 1.17 (95% CI 1.04–1.31) | Canada/Retrospective cohort study |
| Li et al., 2012 [28] | Nonfatal cardiovascular disease (nonfatal myocardial infarction, nonfatal stroke) | Participants: 96,008 (women); Psoriasis: 2463 | Hazard ratio: Myocardial infarction: 1.70 (95% CI 1.01–2.86); Stroke: 1.45 (95% CI 0.80–2.65) | United States/Cohort study |
| Lin et al., 2011 [30] | Myocardial infarction | Psoriasis: 4752; Controls: 23,760 | Hazard ratio: 2.10 (95% CI 1.27–3.43) | Taiwan/Retrospective cohort study |
| Mallbris et al., 2004 [49] | Cardiovascular mortality | Psoriasis inpatients: 8991; Psoriasis outpatients: 19,757 | Standardized mortality ratio: Inpatients: 1.52 (95% CI 1.44–1.60); Outpatients: 0.94 (95% CI 0.89–0.99) | Sweden/Cohort study |
| Mehta et al., 2010 [18] | Cardiovascular mortality | Severe psoriasis: 3603; Controls: 14,330 | Hazard ratio: 1.57 (95% CI 1.26–1.96) | United Kingdom/Cohort study |
| Ogdie et al., 2015 [25] | Major adverse cardiovascular events (including myocardial infarction, cerebrovascular accidents and cardiovascular death) | Psoriasis: 138,424; Controls: 81,573 | Hazard ratio: Mild psoriasis (no DMARD): 1.08 (95% CI 1.02–1.15); Severe psoriasis (DMARD user): 1.42 (95% CI 1.17–1.73) | United Kingdom/Cohort study |
| Prodanovich et al., 2009 [42] | Ischemic heart disease; Cerebrovascular disease; Peripheral vascular disease | Psoriasis: 3236; Controls: 2500 | Odds ratio: Ischemic heart disease: 1.78 (95% CI 1.51–2.11); Cerebrovascular disease: 1.70 (95% CI 1.33–2.17); Peripheral vascular disease: 1.98 (95% CI 1.38–2.82) | United States/Observational cross-sectional study |
| Shiba et al., 2016 [31] | Coronary heart disease | Hospital-based population: 113,065; Psoriasis: 1197 | Odds ratio: 1.27 (95% CI 1.01–1.58) | Japan/Cross-sectional study |
| Stern et al., 2011 [33] | Cardiovascular mortality | Severe psoriasis: 1376 | Standard mortality ratio: 1.02 (95% CI 0.90–1.16) | United States/Prospective cohort study |
| Wakkee et al., 2010 [34] | Ischemic heart disease hospitalization | Psoriasis: 15,820; Controls: 27,577 | Hazard ratio: 1.05 (95% CI 0.95–1.17) | Netherlands/Cohort study |
| Wu et al., 2015 [26] | Myocardial infarction | Mild psoriasis: 10,173 (controls: 50,865); Severe psoriasis: 3841 (controls: 19,205) | Hazard ratio: Mild psoriasis: 1.31 (95% CI 1.14–1.51); Severe psoriasis: 1.28 (95% CI 1.02–1.60) | United States/Retrospective cohort study |
| Study | Treatment for Psoriasis | Cardiovascular Endpoint | Number of Patients | Relative Risk | Population/Type of Study |
|---|---|---|---|---|---|
| Abuabara et al., 2011 [262] | Systemic immunomodulatory therapies (methotrexate, cyclosporine, alefacept, efalizumab, adalimumab, etanercept, infliximab) | Myocardial infarction | Psoriasis: 25,554; Phototherapy: 4220; Systemic treatment: 20,094; Both treatments: 1240 | Hazard ratio (compared to UVB phototherapy): 1.33 (95% CI 0.90–1.96) | United States/Cohort study |
| Ahlehoff et al., 2013 [254] | Biological agents; Methotrexate | Cardiovascular death, myocardial infarction and stroke | Severe psoriasis: 2400; Biological agents: 693; Methotrexate: 799; Other therapies: 908 | Hazard ratio (compared to other therapies): Biological agents: 0.48 (95% CI 0.17–1.38); Methotrexate: 0.50 (95% CI 0.26–0.97) | Denmark/Retrospective cohort study |
| Ahlehoff et al., 2015 [252] | Methotrexate; Cyclosporine; Retinoids; TNF-α inhibitors; Ustekinumab | Cardiovascular events (cardiovascular death, myocardial infarction, stroke) | Severe psoriasis: 6902; Methotrexate: 3564; Cyclosporine: 244; Retinoids: 756; TNF-α inhibitors: 959; Ustekinumab: 178 | Hazard ratio (compared to other therapies): Methotrexate: 0.53 (95% CI 0.34–0.83); Cyclosporine: 1.06 (95% CI 0.26–4.27); Retinoids: 1.80 (95% CI 1.03–2.96); TNF-α inhibitors: 0.46 (95% CI 0.22–0.98); Ustekinumab: 1.52 (95% CI 0.47–4.94) | Denmark/Cohort study |
| Chin et al., 2013 [179] | Methotrexate; Retinoid | Cardiovascular disease; Cerebrovascular disease | Psoriasis patients without arthritis: 7648 | Hazard ratio (compared to no methotrexate and no retinoid treatment): Cardiovascular disease: Methotrexate: 0.39 (95% CI 0.20–0.76); Retinoid 0.47 (95% CI 0.26–0.83); Cerebrovascular disease: Methotrexate: 0.42 (95% CI 0.19–0.95); Retinoid: 0.67 (95% CI 0.35–1.31) | Taiwan/Retrospective cohort study |
| Lan et al., 2012 [48] | Methotrexate; Retinoid | Cerebrovascular disease | Psoriasis: 8180; Methotrexate: 258; Retinoid: 193 | Hazard ratio (compared to no methotrexate and no retinoid treatment): Methotrexate: 0.50 (95% CI 0.27–0.92); Retinoid: 0.70 (95% CI 0.39–1.23) | Taiwan/Retrospective cohort study |
| Prodanovich et al., 2005 [251] | Methotrexate | Vascular disease (including cardiovascular disease, cerebrovascular disease, atherosclerosis) | Psoriasis: 7615 | Relative risk (compared to no methotrexate treatment): Methotrexate: 0.73 (95% CI 0.55–0.98); Low cumulative dose methotrexate: 0.50 (95% CI 0.31–0.79) | United States/Retrospective cohort study |
| Wu et al., 2012 [263] | TNF inhibitor | Myocardial infarction | Psoriasis: 8845; TNF inhibitor: 1673 | Hazard ratio (compared to topical therapy): TNF inhibitor: 0.50 (95% CI 0.32–0.79) | United States/Retrospective cohort study |
| Wu et al., 2013 [264] | TNF inhibitor; Oral/phototherapy | Myocardial infarction | Psoriasis: 8845; Caucasians: 4645 (TNF inhibitor: 857; Oral/phototherapy: 1011; Topical: 2777); Non-Caucasians: 4200 (TNF inhibitor: 816; Oral/phototherapy: 1086; Topical: 2298) | Hazard ratio (compared to topical therapy): Caucasians: TNF inhibitors: 0.35 (95% CI 0.20–0.62); Oral/phototherapy: 0.36 (95% CI 0.22–0.59); Non-Caucasians: TNF inhibitors: 0.27 (95% CI 0.11–0.67); Oral/phototherapy: 0.58 (95% CI 0.32–1.04) | United States/Retrospective cohort study |
| Wu et al., 2013 [265] | TNF inhibitor (etanercept or monoclonal antibody) | Myocardial infarction | Etanercept: 976; Monoclonal antibody: 217; Topical therapy: 5075 | Hazard ratio (compared to topical agents): Etanercept: 0.53 (95% CI 0.31–0.92); Monoclonal antibody: 0.25 (95% CI 0.06–1.03) | United States/Retrospective cohort study |
| Wu et al., 2014 [266] | TNF inhibitor | Myocardial infarction | Psoriasis (treated with TNF inhibitor): 846; Psoriasis (not treated with TNF inhibitor): 7172 | Hazard ratio (compared to psoriasis patients not treated with TNF inhibitors): 0.26 (95% CI 0.12–0.56) | United States/Retrospective cohort study |
| Wu et al., 2017 [267] | TNF inhibitor | Major cardiovascular events (myocardial infarction, stroke or transient ischemic attack, unstable angina) | TNF inhibitor: 9148; Methotrexate: 8581 | Hazard ratio (compared to methotrexate): Major cardiovascular event: 0.55 (95% CI 0.45–0.67) Myocardial infarction: 0.49 (95% CI 0.34–0.71); Stroke or TIA: 0.55 (95% CI 0.42–0.71); Unstable angina: 0.58 (95% CI 0.41–0.82) | United States/Retrospective cohort study |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, S.C.-S.; Lan, C.-C.E. Psoriasis and Cardiovascular Comorbidities: Focusing on Severe Vascular Events, Cardiovascular Risk Factors and Implications for Treatment. Int. J. Mol. Sci. 2017, 18, 2211. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms18102211
Hu SC-S, Lan C-CE. Psoriasis and Cardiovascular Comorbidities: Focusing on Severe Vascular Events, Cardiovascular Risk Factors and Implications for Treatment. International Journal of Molecular Sciences. 2017; 18(10):2211. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms18102211
Chicago/Turabian StyleHu, Stephen Chu-Sung, and Cheng-Che E. Lan. 2017. "Psoriasis and Cardiovascular Comorbidities: Focusing on Severe Vascular Events, Cardiovascular Risk Factors and Implications for Treatment" International Journal of Molecular Sciences 18, no. 10: 2211. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms18102211