Does Locoregional Chemotherapy Still Matter in the Treatment of Advanced Pelvic Melanoma?

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Results
2.1. Patients Characteristics
2.2. Treatments
2.3. BRAF Mutational Status
2.4. Tumor Responses
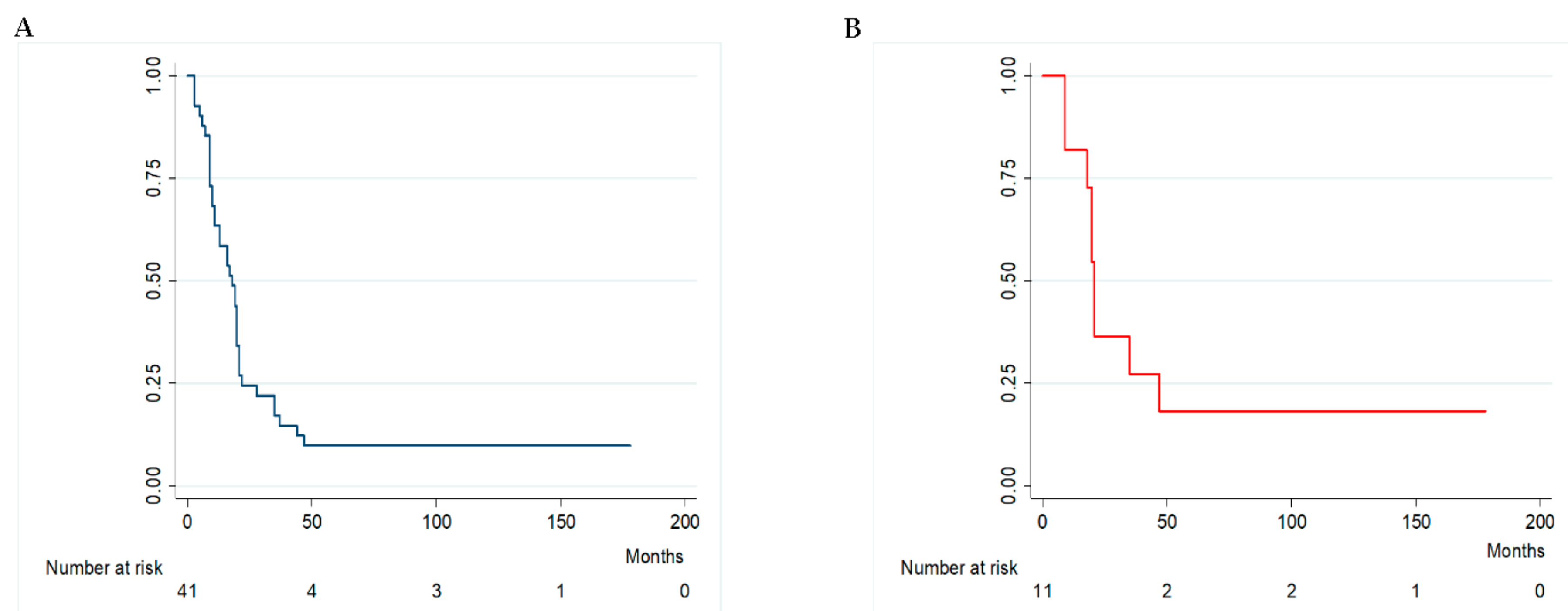
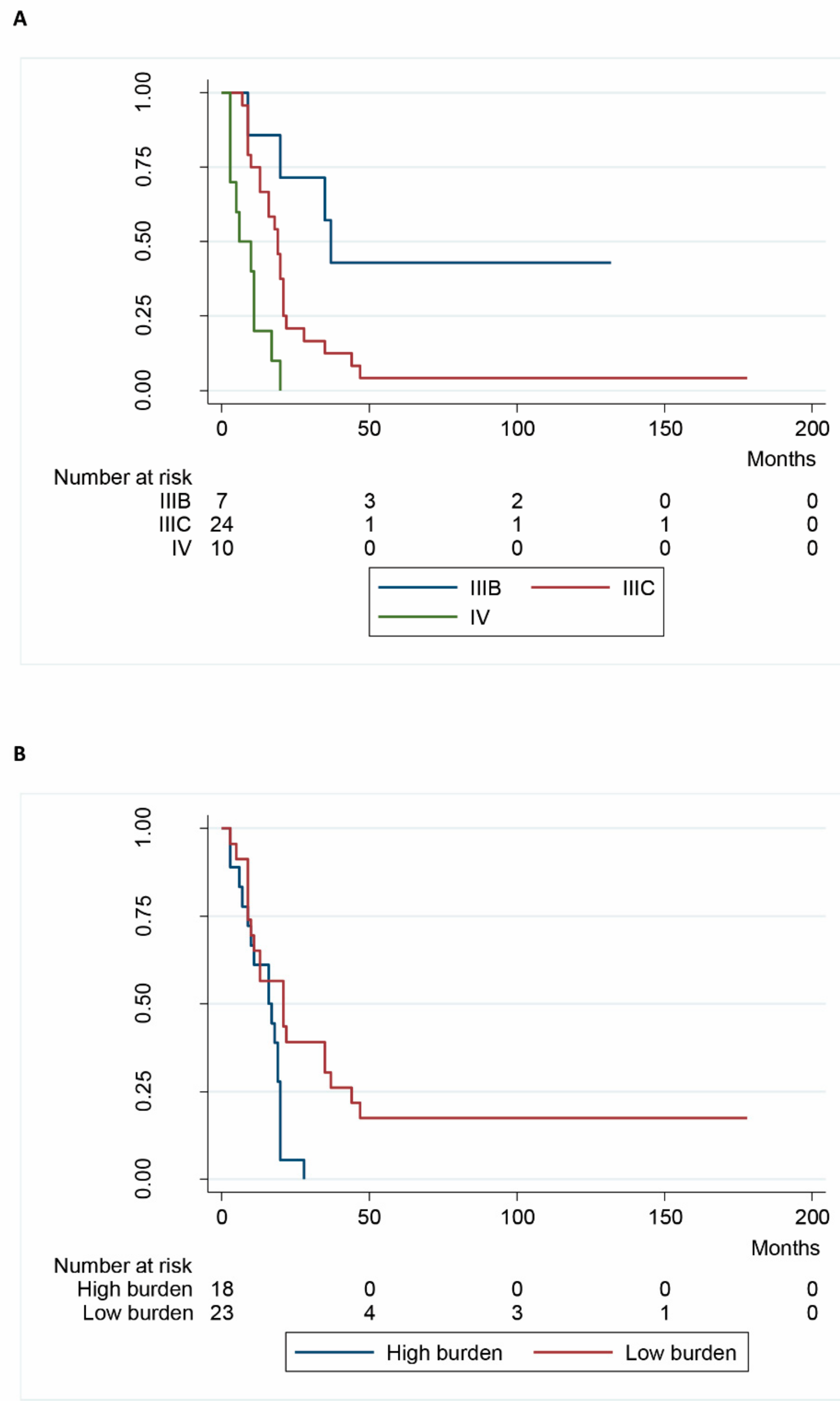
2.5. Survival
2.6. Follow-Up
3. Discussion
4. Patients and Methods
4.1. Patients
4.2. Histopathological and Molecular Evaluation
4.3. Treatment Protocol
4.4. Hypoxic Pelvic Perfusion Technique and Melphalan Regimen
4.5. Criteria for Responses and Adverse Events
4.6. Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| MST | median survival time |
| DOAJ | v-Raf murine sarcoma viral oncogene homolog B |
| FFPE | formalin fixed paraffin embedded |
| CAST | competitive allele specific technology |
| CT | Computerized tomography |
| MRI | Magnetic Resonance Imaging |
| PET | Position-emission Tomography |
| CTCAE | common Terminology Criteria for Adverse Events |
| SD | standard deviation |
| PFS | progression free survival |
| MAP | mitogen-activated protein |
| PD-1 | programmed cell death protein 1 |
| PD-L1 | programmed cell death-ligand protein 1 |
References
- Shain, A.H.; Bastian, B.C. From melanocytes to melanomas. Nat. Rev. Cancer 2016, 16, 345–358. [Google Scholar] [CrossRef] [PubMed]
- Kunz, M.; Hölzel, M. The impact of melanoma genetics on treatment response and resistance in clinical and experimental studies. Cancer Metastasis Rev. 2017, 36, 53–75. [Google Scholar] [CrossRef] [PubMed]
- Trout, A.T.; Rabinowitz, R.S.; Platt, J.F.; Elsayes, K.M. Melanoma metastases in the abdomen and pelvis: Frequency and patterns of spread. World J. Radiol. 2013, 5, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Guadagni, S.; Russo, F.; Rossi, C.R.; Pilati, P.L.; Miotto, D.; Fiorentini, G.; Deraco, M.; Santinami, M.; Palumbo, G.; Valenti, M.; et al. Deliberate hypoxic pelvic and limb chemoperfusion in the treatment of recurrent melanoma. Am. J. Surg. 2002, 83, 28–36. [Google Scholar] [CrossRef]
- Khushalani, N.I.; Sondak, V.K. Are we there yet? Prolonged MAPK inhibition in BRAF V600-mutant melanoma. Lancet Oncol. 2016, 17, 1178–1179. [Google Scholar] [CrossRef]
- Chan, M.M.; Haydu, L.E.; Menzies, A.M.; Azer, M.W.; Klein, O.; Lyle, M.; Clements, A.; Guminski, A.; Kefford, R.F.; Long, G.V. The nature and management of metastatic melanoma after progression on BRAF inhibitors: Effects of extended BRAF inhibition. Cancer 2014, 120, 3142–3153. [Google Scholar] [CrossRef] [PubMed]
- Topollian, S.L.; Sznol, M.; McDermott, D.F.; Kluger, H.M.; Carvajal, R.D.; Sharfman, W.H.; Brahmer, J.R.; Lawrence, D.P.; Atkins, M.B.; Powderly, J.D.; et al. Survival, durable tumor remission, and long-term safety in patients with advanced melanoma receiving nivolumab. J. Clin. Oncol. 2014, 32, 1020–1030. [Google Scholar] [CrossRef] [PubMed]
- Ribas, A.; Hamid, O.; Daud, A.; Hodi, F.S.; Wolchok, J.D.; Kefford, R.; Joshua, A.M.; Patnaik, A.; Hwu, W.J.; Weber, J.S.; et al. Association of pembrolizumab with tumor response and survival among patients with advanced melanoma. JAMA 2016, 315, 1600–1609. [Google Scholar] [CrossRef] [PubMed]
- Daud, A.; Nandoskar, P. Pembrolizumab for melanoma-safety profile and future trends. Expert Opin. Drug Saf. 2016, 15, 727–729. [Google Scholar] [CrossRef] [PubMed]
- Raigani, S.; Cohen, S.; Boland, G.M. The role of surgery for melanoma in an era of effective systemic therapy. Curr. Oncol. Rep. 2017, 19, 17. [Google Scholar] [CrossRef] [PubMed]
- Chapman, P.B.; Einhorn, L.H.; Meyers, M.L.; Saxman, S.; Destro, A.N.; Panageas, K.S.; Begg, C.B.; Agarwala, S.S.; Schuchter, L.M.; Ernstoff, M.S.; et al. Phase III multicenter randomized trial of the Dartmouth regimen versus dacarbazine in patients with metastatic melanoma. J. Clin. Oncol. 1999, 17, 2745–2751. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, S.; Tykodi, S.S.; Thompson, J.A. Treatment of metastatic melanoma: An overview. Oncology 2009, 23, 488–496. [Google Scholar] [PubMed]
- Stehlin, J.S.; Clark, R.L.; White, E.C.; Smith, J.L.; Griffin, A.C.; Jesse, R.H.; Healey, J.E. Regional chemotherapy for cancer: Experiences with 116 perfusions. Ann. Surg. 1960, 151, 605–619. [Google Scholar] [CrossRef] [PubMed]
- Guadagni, S.; Palumbo, G.; Fiorentini, G.; Clementi, M.; Marsili, L. Surgical versus percutaneous isolated pelvic perfusion (IPP) for advanced melanoma: Comparison in terms of melphalan pharmacokinetic pelvic bio-availability. BMC Res Notes 2017, 10. [Google Scholar] [CrossRef] [PubMed]
- Wanebo, H.J.; Chung, M.A.; Levy, A.I.; Turk, P.S.; Vezeridis, M.P.; Belliveau, J.F. Preoperative therapy for advanced pelvic malignancy by isolated pelvic perfusion with the balloon-occlusion technique. Ann. Surg. Oncol. 1996, 3, 295–303. [Google Scholar] [CrossRef] [PubMed]
- Bonvalot, S.; de Baere, T.; Mendiboure, J.; Paci, A.; Farace, F.; Drouard-Troalen, L.; Bonnet, L.; Hakime, A.; Bonniaud, G.; Raynard, B.; et al. Hyperthermic pelvic perfusion with tumor necrosis factor-α for locally advanced cancers. Encouraging results of a phase II study. Ann. Surg. 2012, 255, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Merlino, G.; Herlyn, M.; Fisher, D.E.; Bastian, B.C.; Flaherty, K.T.; Davies, M.A.; Wargo, J.A.; Curiel-Lewandrowski, C.; Weber, M.J.; Leachman, S.A.; et al. The state of melanoma: challenges and opportunities. Pigment Cell Melanoma Res. 2016, 29, 404–416. [Google Scholar] [CrossRef] [PubMed]
- Murali, R.; Shaw, H.M.; Lai, K.; McCarthy, S.W.; Quinn, M.J.; Stretch, J.R.; Thompson, J.F.; Scolyer, R.A. Prognostic factors in cutaneous Desmoplastic Melanoma: A study of 252 patients. Cancer 2010, 116, 4130–4138. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Kim, S.N.; Hahn, H.J.; Lee, Y.W.; Choe, Y.B.; Ahn, K.J. Metaanalysis of BRAF mutations and clinicopathologic characteristics in primary melanoma. J. Am. Acad. Dermatol. 2015, 72, 1036. [Google Scholar] [CrossRef] [PubMed]
- Pellegrini, C.; Di Nardo, L.; Cipolloni, G.; Martorelli, C.; de Padova, M.; Antonini, A.; Maturo, M.G.; del Regno, L.; Strafella, S.; Micantonio, T.; et al. Heterogeneity of Braf, Nras, and Tert-Promoter Mutational Status in Multiple Melanomas and association with Mc1r Genotype: Findings from Molecular and immunohistochemical analysis. J. Mol. Diagn. 2017. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.B.; Sullivan, R.J.; Menzies, A.M. Immune checkpoint inhibitors in challenging populations. Cancer 2017, 123, 1904–1911. [Google Scholar] [CrossRef] [PubMed]
- Pruijn, F.B.; van Daalen, M.; Holford, N.H. Mechanisms of enhancement of the antitumour activity of Melphalan by the tumour-blood-flow inhibitor 5,6-dimethylxanthenone-4-acetic acid. Cancer Chemother. Pharmacol. 1997, 39, 541–546. [Google Scholar] [CrossRef] [PubMed]
- Kroon, H.M.; Lin, D.Y.; Kam, P.C.A.; Thompson, J.F. Efficacy of repeat isolated limb infusion with melphalan and actinomycin D for recurrent melanoma. Cancer 2009, 115, 1932–1940. [Google Scholar] [CrossRef] [PubMed]
- Mangana, J.; Cheng, P.F.; Kaufmann, C. Multicenter, real-life experience with checkpoint inhibitors and targeted therapy agents in advanced melanoma patients in Switzerland. Melanoma Res. 2017, 27, 358–368. [Google Scholar] [CrossRef] [PubMed]
- Guadagni, S.; Fiorentini, G.; Clementi, M.; Palumbo, G.; Chiominto, A.; Cappelli, S.; Masedu, F.; Valenti, M. Melphalan hypoxic perfusion with hemofiltration for melanoma locoregional metastases in the pelvis. J. Surg. Res. 2017, 215, 114–124. [Google Scholar] [CrossRef] [PubMed]
- Ma, Q.; Zhao, Z.; Barber, B.L.; Shilkrut, M. Use patterns and costs of isolated limb perfusion and infusion in the treatment of regional metastatic melanoma: A retrospective database analysis. Adv. Ther. 2016, 33, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Balch, C.M.; Gershenwald, J.E.; Song, S.J.; Thompson, J.F.; Atkins, M.B.; Byrd, D.R.; Buzaid, A.C.; Cochran, A.J.; Coit, D.G.; Ding, S.; et al. Final version of 2009 AJCC melanoma staging and classification. J. Clin. Oncol. 2009, 27, 6199–6206. [Google Scholar] [CrossRef] [PubMed]
- Steinman, J.; Ariyan, C.; Rafferty, B.; Brady, M.S. Factors associated with response, survival, and limb salvage in patients undergoing isolated limb infusion. J. Surg. Oncol. 2014, 109, 405–409. [Google Scholar] [CrossRef] [PubMed]
- Didelot, A.; le Corre, D.; Luscan, A.; Cazes, A.; Pallier, K.; Emile, J.F.; Laurent-Puig, P.; Blons, H. Competitive allele specific TaqMan PCR for KRAS, BRAF and EGFR mutation detection in clinical formalin fixed paraffin embedded samples. Exp. Mol. Pathol. 2012, 92, 275–280. [Google Scholar] [CrossRef] [PubMed]
- Guadagni, S.; Santinami, M.; Patuzzo, R.; Pilati, P.L.; Miotto, D.; Deraco, M.; Rossi, C.R.; Fiorentini, G.; di Filippo, F.; Valenti, M.; et al. Hypoxic pelvic and limb perfusion with Melphalan and mitomycin C for recurrent limb melanoma: A pilot study. Melanoma Res. 2003, 13, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Varrassi, G.; Guadagni, S.; Ciccozzi, A.; Marinangeli, F.; Pozone, T.; Piroli, A.; Marsili, I.; Paladini, A. Hemodynamic variations during thoracic and abdominal stop-flow regional chemotherapy. Eur. J. Surg. Oncol. 2004, 30, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Guadagni, S.; Fiorentini, G.; Clementi, M.; Palumbo, G.; Masedu, F.; Deraco, M.; de Manzoni, G.; Chiominto, A.; Valenti, M.; Pellegrini, C. MGMT methylation correlates with melphalan pelvic perfusion survival in stage III melanoma patients: A pilot study. Melanoma Res. 2017, 27, 439–447. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J. New response valuation criteria in solid tumors: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Complications | Grade | n (%) |
| Seroma | 1 | 4 (2.3) |
| Persistent leakage of fluid from the incision | 2 | 14 (8.0) |
| Wound infection | 1 | 3 (1.7) |
| Inguinal hematoma | 1 | 7 (4.0) |
| Wound dehiscence | 2 | 7 (4.0) |
| Lymphangitis | 2 | 3 (1.7) |
| Scrotum edema | 1 | 6 (3.4) |
| Pelvic pain | 1 | 6 (3.4) |
| Toxicity | Grade | n (%) |
| Bone marrow hypocellularity | 1 | 25 (14.3) |
| 2 | 18 (10.3) | |
| 3 | 8 (4.6) | |
| Alopecia | 1 | 7 (4.0) |
| Nausea and vomiting | 1 | 26 (14.9) |
| Variables (Number of Patients) | MST (Months) | Log-Rank χ2 | p Value | Cox HR |
|---|---|---|---|---|
| Age | ||||
| <65 (n = 18) | 17 | |||
| ≥65 (n = 23) | 20 | 0.80 | 0.371 | |
| Gender | ||||
| Female (n = 28) | 19.5 | |||
| Male (n = 13) | 10 | 2.31 | 0.132 | |
| Stage | ||||
| IIIB (n = 7) | 37 | |||
| IIIC (n = 24) | 19 | |||
| IV (n = 10) | 8 | 21.44 | 0.001 | 4.03 [1.91–6.59] |
| BRAF status | ||||
| Wild-type (n = 22) | 20 | |||
| V600E Mutated (n = 19) | 13 | 0.36 | 0.551 | |
| Burden | ||||
| Low (n = 23) | 21 | |||
| High (n = 18) | 16.5 | 7.61 | 0.005 | 2.58 [1.26–5.58] |
| Mitosis | ||||
| <1 (n = 17) | 20 | |||
| ≥1 (n = 24) | 14.5 | 3.66 | 0.064 | |
| Associate Excision | ||||
| Yes (n = 35) | 18 | |||
| Not (n = 6) | 17.5 | 2.41 | 0.128 | |
| Melanin cellular pigmentation | ||||
| Yes (n = 15) | 20 | |||
| Not (n = 26) | 14.5 | 0.15 | 0.691 | |
| Number of treatments | ||||
| ≤2 (n = 7) | 5 | |||
| >2 (n = 34) | 19 | 1.58 | 0.203 |
| Characteristics of Patients | n (%) | |
| Gender | Males | 13 (31.7) |
| Females | 28 (68.3) | |
| Stage [27] | IIIB | 7 (17.1) |
| IIIC | 24 (58.5) | |
| IV | 10 (24.4) | |
| Burden [28] | Low Burden * | 23 (56.1) |
| High Burden ** | 18 (43.9) | |
| Patients with exclusion criteria for immune check-point therapy | Yes | 8 (19.5) |
| No | 33 (80.5) | |
| Characteristics of tumors | n (%) | |
| Anatomical site | Labia/vagina | 2 (4.9) |
| Anus | 2 (4.9) | |
| Anterior trunk | 2 (4.9) | |
| Back | 3 (9.7) | |
| Lower extremity | 31 (75.6) | |
| Melanin presence | Yes | 15 (36.6) |
| No | 26 (63.4) | |
| Mitotic rate | <1 mitosis per mm2 | 17 (41.5) |
| >1 mitosis per mm2 | 24 (58.5) | |
| BRAF status | wild-type | 22 (53.7) |
| V600E mutated | 19 (46.3) | |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guadagni, S.; Fiorentini, G.; Clementi, M.; Palumbo, G.; Palumbo, P.; Chiominto, A.; Baldoni, S.; Masedu, F.; Valenti, M.; Tommaso, A.D.; et al. Does Locoregional Chemotherapy Still Matter in the Treatment of Advanced Pelvic Melanoma? Int. J. Mol. Sci. 2017, 18, 2382. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms18112382
Guadagni S, Fiorentini G, Clementi M, Palumbo G, Palumbo P, Chiominto A, Baldoni S, Masedu F, Valenti M, Tommaso AD, et al. Does Locoregional Chemotherapy Still Matter in the Treatment of Advanced Pelvic Melanoma? International Journal of Molecular Sciences. 2017; 18(11):2382. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms18112382
Chicago/Turabian StyleGuadagni, Stefano, Giammaria Fiorentini, Marco Clementi, Giancarlo Palumbo, Paola Palumbo, Alessandro Chiominto, Stefano Baldoni, Francesco Masedu, Marco Valenti, Ambra Di Tommaso, and et al. 2017. "Does Locoregional Chemotherapy Still Matter in the Treatment of Advanced Pelvic Melanoma?" International Journal of Molecular Sciences 18, no. 11: 2382. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms18112382