
Clinical Outcomes of 217 Patients with Acute Erythroleukemia According to Treatment Type and Line: A Retrospective Multinational Study

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Total Acute Erythroleukemia (AEL) Cohort (n = 217)
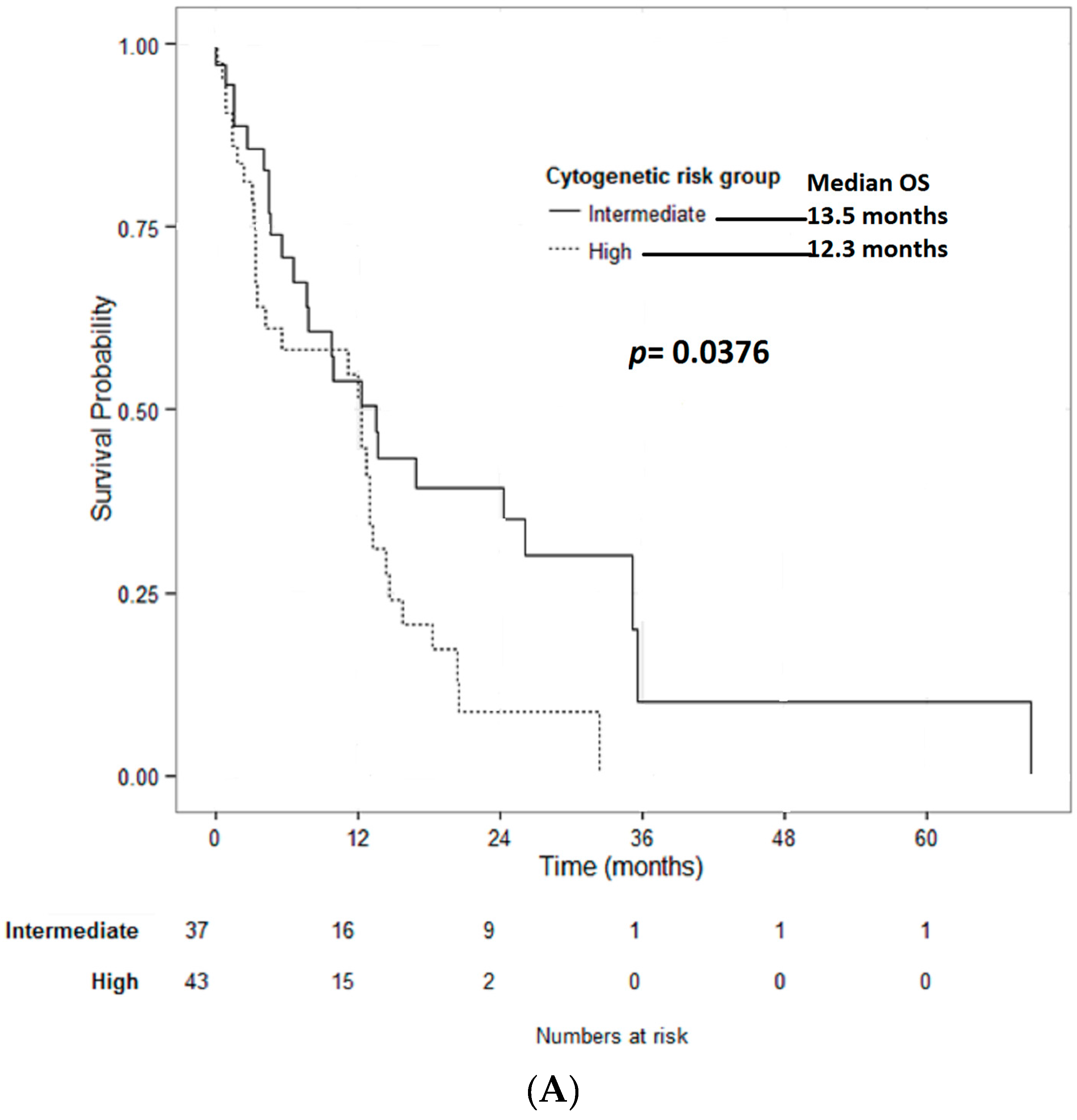
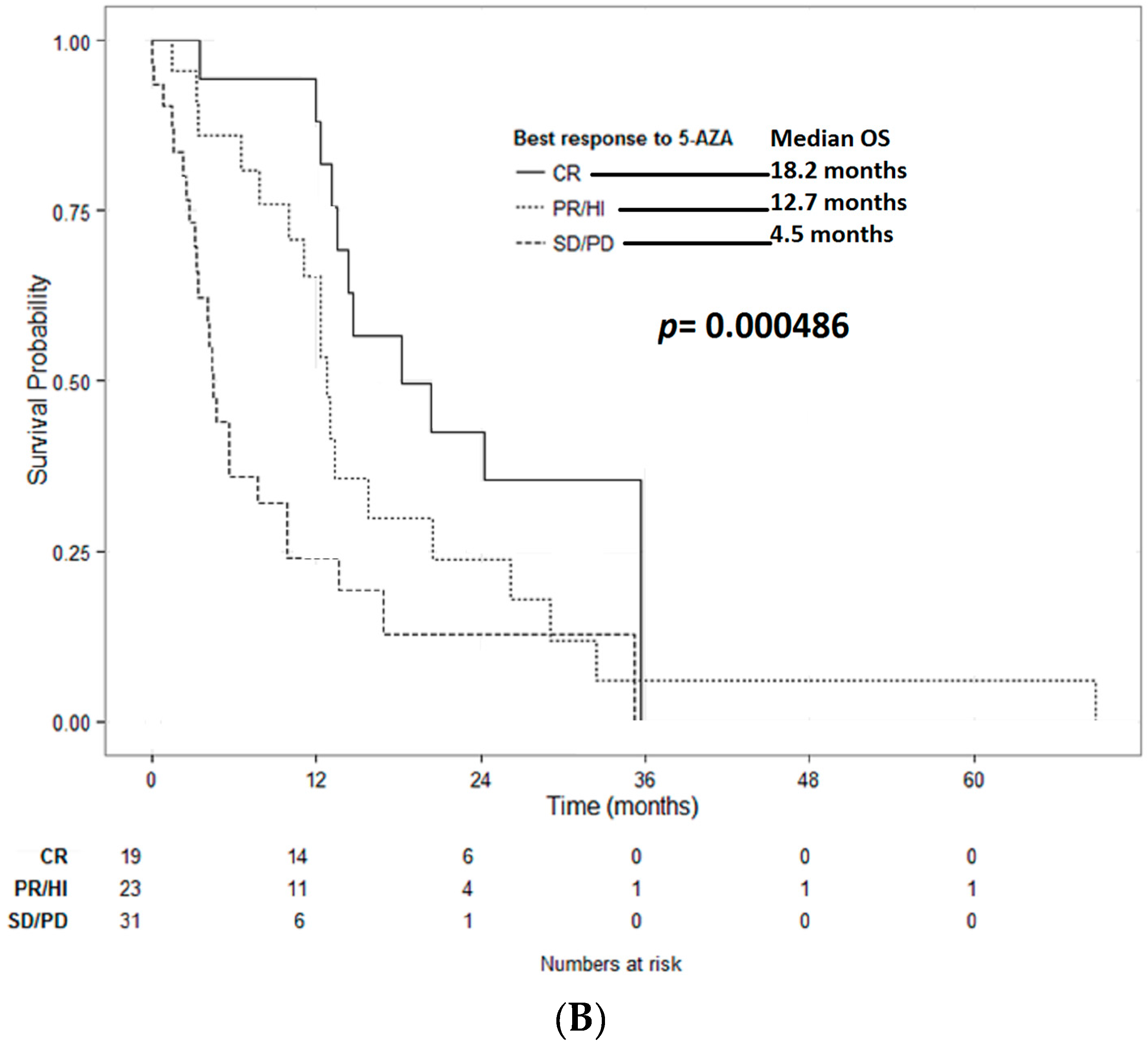
2.2. AEL Treated with HMA (n = 88)
2.3. AEL Treated with ICT (n = 122)
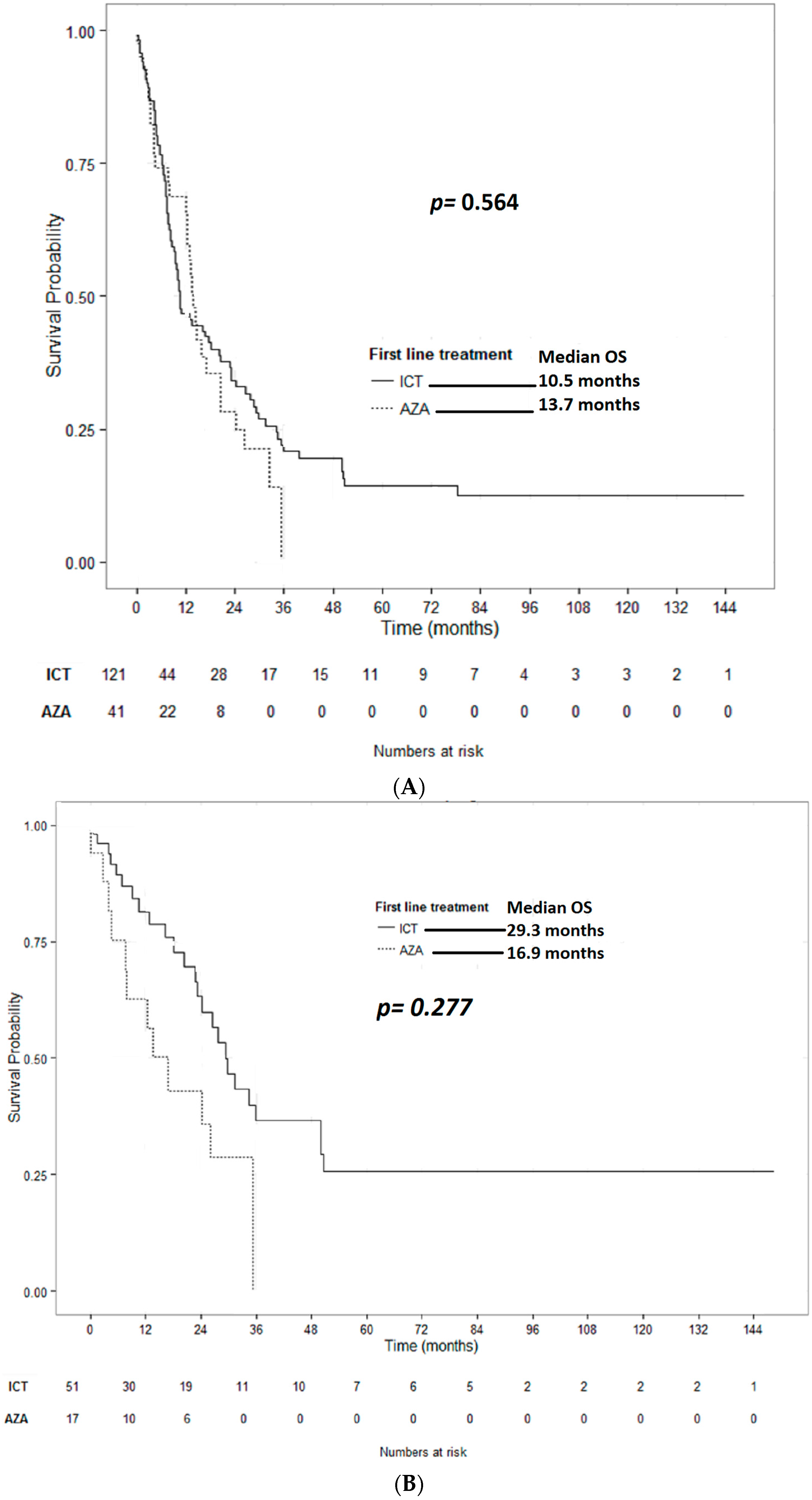
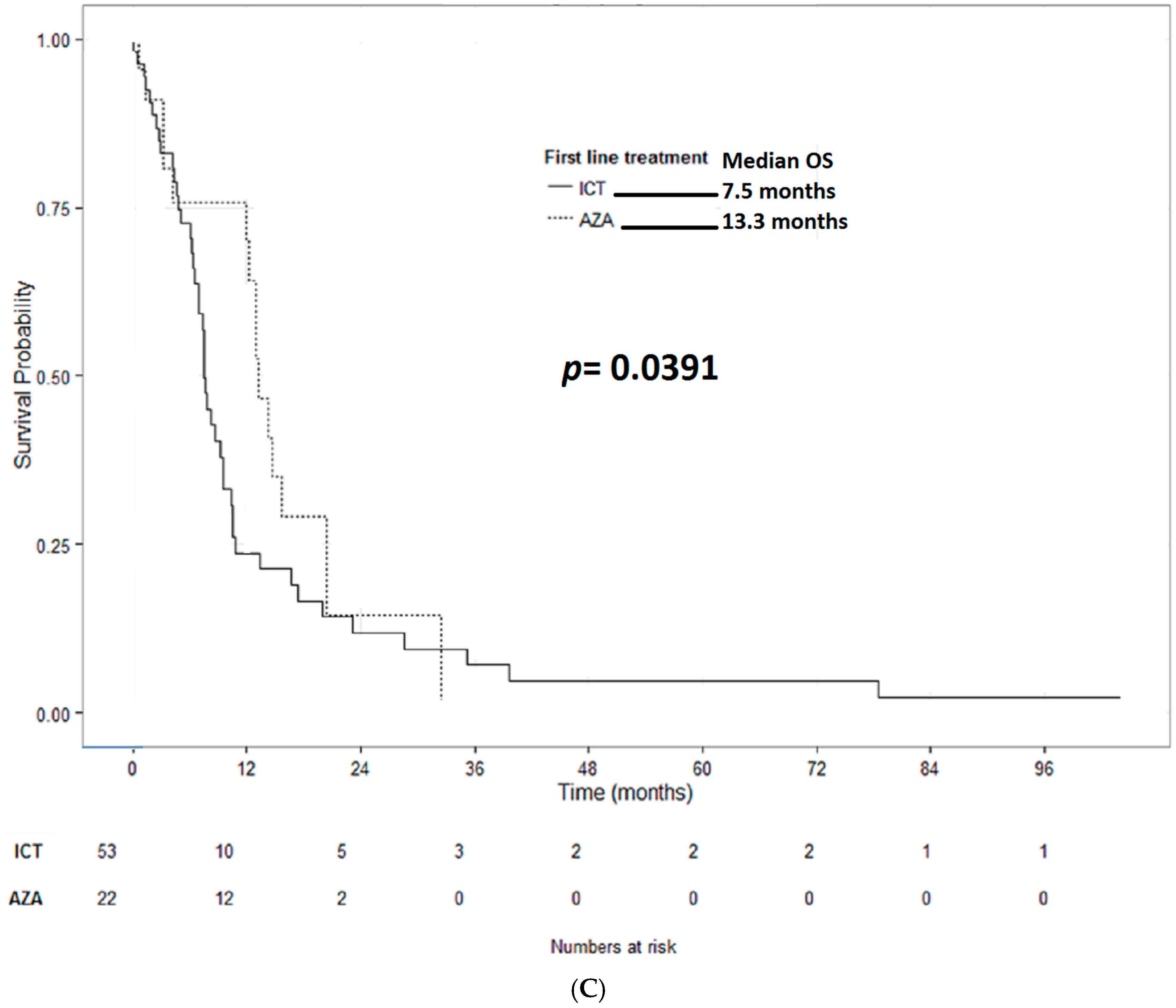
2.4. Comparison of AEL Treated with ICT vs. HMA
3. Discussion
4. Methods
4.1. Patient Population
4.2. Definition of Endpoints
4.3. Statistics
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Santos, F.P.; Bueso-Ramos, C.E.; Ravandi, F. Acute erythroleukemia: Diagnosis and management. Expert Rev. Hematol. 2010, 3, 705–718. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Hasserjian, R.P.; Hu, Y.; Zhang, L.; Miranda, R.N.; Medeiros, L.J.; Wang, S.A. Pure erythroid leukemia: A reassessment of the entity using the 2008 World Health Organization classification. Mod. Pathol. 2011, 24, 375–383. [Google Scholar] [CrossRef] [PubMed]
- Zuo, Z.; Polski, J.M.; Kasyan, A.; Medeiros, L.J. Acute erythroid leukemia. Arch. Pathol. Lab. Med. 2010, 134, 1261–1270. [Google Scholar] [PubMed]
- Kasyan, A.; Medeiros, L.J.; Zuo, Z.; Santos, F.P.; Ravandi-Kashani, F.; Miranda, R.; Vadhan-Raj, S.; Koeppen, H.; Bueso-Ramos, C.E. Acute erythroid leukemia as defined in the World Health Organization classification is a rare and pathogenetically heterogeneous disease. Mod. Pathol. 2010, 23, 1113–1126. [Google Scholar] [CrossRef] [PubMed]
- Selby, D.M.; Valdez, R.; Schnitzer, B.; Ross, C.W.; Finn, W.G. Diagnostic criteria for acute erythroleukemia. Blood 2003, 101, 2895–2896. [Google Scholar] [CrossRef] [PubMed]
- Arber, D.A.; Orazi, A.; Hasserjian, R.; Thiele, J.; Borowitz, M.J.; Le Beau, M.M.; Bloomfield, C.D.; Cazzola, M.; Vardiman, J.W. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood 2016, 127, 2391–2405. [Google Scholar] [CrossRef] [PubMed]
- Arenillas, L.; Calvo, X.; Luno, E.; Senent, L.; Alonso, E.; Ramos, F.; Ardanaz, M.T.; Pedro, C.; Tormo, M.; Marco, V.; et al. Considering Bone Marrow Blasts From Nonerythroid Cellularity Improves the Prognostic Evaluation of Myelodysplastic Syndromes. J. Clin. Oncol. 2016, 34, 3284–3292. [Google Scholar] [CrossRef] [PubMed]
- Calvo, X.; Arenillas, L.; Luno, E.; Senent, L.; Arnan, M.; Ramos, F.; Ardanaz, M.T.; Pedro, C.; Tormo, M.; Montoro, J.; et al. Erythroleukemia shares biological features and outcome with myelodysplastic syndromes with excess blasts: A rationale for its inclusion into future classifications of myelodysplastic syndromes. Mod. Pathol. 2016, 29, 1541–1551. [Google Scholar] [CrossRef] [PubMed]
- Jogai, S.; Varma, N.; Garewal, G.; Das, R.; Varma, S. Acute erythroleukemia (AML-M6)—A study of clinicohematological, morphological and dysplastic features in 10 cases. Indian J. Cancer 2001, 38, 143–148. [Google Scholar] [PubMed]
- Olopade, O.I.; Thangavelu, M.; Larson, R.A.; Mick, R.; Kowal-Vern, A.; Schumacher, H.R.; Le Beau, M.M.; Vardiman, J.W.; Rowley, J.D. Clinical, morphologic, and cytogenetic characteristics of 26 patients with acute erythroblastic leukemia. Blood 1992, 80, 2873–2882. [Google Scholar] [PubMed]
- Domingo-Claros, A.; Larriba, I.; Rozman, M.; Irriguible, D.; Vallespi, T.; Aventin, A.; Ayats, R.; Milla, F.; Sole, F.; Florensa, L.; et al. Acute erythroid neoplastic proliferations. A biological study based on 62 patients. Haematologica 2002, 87, 148–153. [Google Scholar] [PubMed]
- Lessard, M.; Struski, S.; Leymarie, V.; Flandrin, G.; Lafage-Pochitaloff, M.; Mozziconacci, M.J.; Talmant, P.; Bastard, C.; Charrin, C.; Baranger, L.; et al. Cytogenetic study of 75 erythroleukemias. Cancer Genet. Cytogenet. 2005, 163, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Mazzella, F.M.; Kowal-Vern, A.; Shrit, M.A.; Rector, J.T.; Cotelingam, J.D.; Schumacher, H.R. Effects of multidrug resistance gene expression in acute erythroleukemia. Mod. Pathol. 2000, 13, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Grossmann, V.; Bacher, U.; Haferlach, C.; Schnittger, S.; Potzinger, F.; Weissmann, S.; Roller, A.; Eder, C.; Fasan, A.; Zenger, M.; et al. Acute erythroid leukemia (AEL) can be separated into distinct prognostic subsets based on cytogenetic and molecular genetic characteristics. Leukemia 2013, 27, 1940–1943. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, J.; Hrisinko, M.A.; Weil, S.C. Erythroleukemia: A review of 15 cases meeting 1985 FAB criteria and survey of the literature. Blood Rev. 1992, 6, 204–214. [Google Scholar] [CrossRef]
- Micci, F.; Thorsen, J.; Panagopoulos, I.; Nyquist, K.B.; Zeller, B.; Tierens, A.; Heim, S. High-throughput sequencing identifies an NFIA/CBFA2T3 fusion gene in acute erythroid leukemia with t(1;16)(p31;q24). Leukemia 2013, 27, 980–982. [Google Scholar] [CrossRef] [PubMed]
- Srinivas, U.; Kumar, R.; Pati, H.P.; Saxena, R.; Tyagi, S. Sub classification and clinico-hematological correlation of 40 cases of acute erythroleukemia—Can proerythroblast/myeloblast and proerythroblast/total erythroid cell ratios help subclassify? Hematology 2007, 12, 381–385. [Google Scholar] [CrossRef] [PubMed]
- Mazzella, F.M.; Kowal-Vern, A.; Shrit, M.A.; Wibowo, A.L.; Rector, J.T.; Cotelingam, J.D.; Collier, J.; Mikhael, A.; Cualing, H.; Schumacher, H.R. Acute erythroleukemia: Evaluation of 48 cases with reference to classification, cell proliferation, cytogenetics, and prognosis. Am. J. Clin. Pathol. 1998, 110, 590–598. [Google Scholar] [CrossRef] [PubMed]
- Kowal-Vern, A.; Mazzella, F.M.; Cotelingam, J.D.; Shrit, M.A.; Rector, J.T.; Schumacher, H.R. Diagnosis and characterization of acute erythroleukemia subsets by determining the percentages of myeloblasts and proerythroblasts in 69 cases. Am. J. Hematol. 2000, 65, 5–13. [Google Scholar] [CrossRef]
- Santos, F.P.; Faderl, S.; Garcia-Manero, G.; Koller, C.; Beran, M.; O‘Brien, S.; Pierce, S.; Freireich, E.J.; Huang, X.; Borthakur, G.; et al. Adult acute erythroleukemia: An analysis of 91 patients treated at a single institution. Leukemia 2009, 23, 2275–2280. [Google Scholar] [CrossRef] [PubMed]
- Pierdomenico, F.; Almeida, A. Treatment of acute erythroleukemia with Azacitidine: A case series. Leuk. Res. Rep. 2013, 2, 41–43. [Google Scholar] [CrossRef] [PubMed]
- Colita, A.; Belhabri, A.; Chelghoum, Y.; Charrin, C.; Fiere, D.; Thomas, X. Prognostic factors and treatment effects on survival in acute myeloid leukemia of M6 subtype: A retrospective study of 54 cases. Ann. Oncol. 2001, 12, 451–455. [Google Scholar] [CrossRef] [PubMed]
- Fenaux, P.; Mufti, G.J.; Hellstrom-Lindberg, E.; Santini, V.; Finelli, C.; Giagounidis, A.; Schoch, R.; Gattermann, N.; Sanz, G.; List, A.; et al. Efficacy of azacitidine compared with that of conventional care regimens in the treatment of higher-risk myelodysplastic syndromes: A randomised, open-label, phase III study. Lancet Oncol. 2009, 10, 223–232. [Google Scholar] [CrossRef]
- Garcia-Manero, G.; Jabbour, E.; Borthakur, G.; Faderl, S.; Estrov, Z.; Yang, H.; Maddipoti, S.; Godley, L.A.; Gabrail, N.; Berdeja, J.G.; et al. Randomized open-label phase II study of decitabine in patients with low- or intermediate-risk myelodysplastic syndromes. J. Clin. Oncol. 2013, 31, 2548–2553. [Google Scholar] [CrossRef] [PubMed]
- Pleyer, L.; Germing, U.; Sperr, W.R.; Linkesch, W.; Burgstaller, S.; Stauder, R.; Girschikofsky, M.; Schreder, M.; Pfeilstocker, M.; Lang, A.; et al. Azacitidine in CMML: Matched-pair analyses of daily-life patients reveal modest effects on clinical course and survival. Leuk. Res. 2014, 38, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Thorpe, M.; Montalvao, A.; Pierdomenico, F.; Moita, F.; Almeida, A. Treatment of chronic myelomonocytic leukemia with 5-Azacitidine: A case series and literature review. Leuk. Res. 2012, 36, 1071–1073. [Google Scholar] [CrossRef] [PubMed]
- Fianchi, L.; Criscuolo, M.; Breccia, M.; Maurillo, L.; Salvi, F.; Musto, P.; Mansueto, G.; Gaidano, G.; Finelli, C.; Aloe-Spiriti, A.; et al. High rate of remissions in chronic myelomonocytic leukemia treated with 5-azacytidine: Results of an Italian retrospective study. Leuk. Lymphoma 2013, 54, 658–661. [Google Scholar] [CrossRef] [PubMed]
- Fenaux, P.; Mufti, G.J.; Hellstrom-Lindberg, E.; Santini, V.; Gattermann, N.; Germing, U.; Sanz, G.; List, A.F.; Gore, S.; Seymour, J.F.; et al. Azacitidine prolongs overall survival compared with conventional care regimens in elderly patients with low bone marrow blast count acute myeloid leukemia. J. Clin. Oncol. 2010, 28, 562–569. [Google Scholar] [CrossRef] [PubMed]
- Dombret, H.; Seymour, J.F.; Butrym, A.; Wierzbowska, A.; Selleslag, D.; Jang, J.H.; Kumar, R.; Cavenagh, J.; Schuh, A.C.; Candoni, A.; et al. International phase 3 study of azacitidine vs. conventional care regimens in older patients with newly diagnosed AML with >30% blasts. Blood 2015, 126, 291–299. [Google Scholar] [CrossRef] [PubMed]
- Kantarjian, H.M.; Thomas, X.G.; Dmoszynska, A.; Wierzbowska, A.; Mazur, G.; Mayer, J.; Gau, J.P.; Chou, W.C.; Buckstein, R.; Cermak, J.; et al. Multicenter, randomized, open-label, phase III trial of decitabine versus patient choice, with physician advice, of either supportive care or low-dose cytarabine for the treatment of older patients with newly diagnosed acute myeloid leukemia. J. Clin. Oncol. 2012, 30, 2670–2677. [Google Scholar] [CrossRef] [PubMed]
- Thepot, S.; Itzykson, R.; Seegers, V.; Recher, C.; Raffoux, E.; Quesnel, B.; Delaunay, J.; Cluzeau, T.; Marfaing Koka, A.; Stamatoullas, A.; et al. Azacitidine in untreated acute myeloid leukemia: A report on 149 patients. Am. J. Hematol. 2014, 89, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Pleyer, L.; Burgstaller, S.; Girschikofsky, M.; Linkesch, W.; Stauder, R.; Pfeilstocker, M.; Schreder, M.; Tinchon, C.; Sliwa, T.; Lang, A.; et al. Azacitidine in 302 patients with WHO-defined acute myeloid leukemia: Results from the Austrian Azacitidine Registry of the AGMT-Study Group. Ann. Hematol. 2014, 93, 1825–1838. [Google Scholar] [CrossRef] [PubMed]
- Falantes, J.; Thepot, S.; Pleyer, L.; Maurillo, L.; Martínez-Robles, V.; Itzykson, R.; Bargay, J.; Stauder, R.; Venditti, A.; Martínez, M.P.; Seegers, V.; et al. Azacitidine in older patients with acute myeloid leukemia (AML). Results from the expanded international E-ALMA series (E-ALMA+) according to the MRC risk index score. Blood 2015, 126, 2554. [Google Scholar]
- Pleyer, L.; Stauder, R.; Burgstaller, S.; Schreder, M.; Tinchon, C.; Pfeilstocker, M.; Steinkirchner, S.; Melchardt, T.; Mitrovic, M.; Girschikofsky, M.; et al. Azacitidine in patients with WHO-defined AML—Results of 155 patients from the Austrian Azacitidine Registry of the AGMT-Study Group. J. Hematol. Oncol. 2013, 6, 32. [Google Scholar] [CrossRef] [PubMed]
- Maurillo, L.; Venditti, A.; Spagnoli, A.; Gaidano, G.; Ferrero, D.; Oliva, E.; Lunghi, M.; D’Arco, A.M.; Levis, A.; Pastore, D.; et al. Azacitidine for the treatment of patients with acute myeloid leukemia: Report of 82 patients enrolled in an Italian Compassionate Program. Cancer 2012, 118, 1014–1022. [Google Scholar] [CrossRef] [PubMed]
- Pleyer, L.; Burgstaller, S.; Stauder, R.; Girschikofsky, M.; Sill, H.; Schlick, K.; Thaler, J.; Halter, B.; Machherndl-Spandl, S.; Zebisch, A.; et al. Azacitidine front-line in 339 patients with myelodysplastic syndromes and acute myeloid leukaemia: Comparison of French-American-British and World Health Organization classifications. J. Hematol. Oncol. 2016, 9, 39. [Google Scholar] [CrossRef] [PubMed]
- Kadia, T.M.; Thomas, X.G.; Dmoszynska, A.; Wierzbowska, A.; Minden, M.; Arthur, C.; Delaunay, J.; Ravandi, F.; Kantarjian, H. Decitabine improves outcomes in older patients with acute myeloid leukemia and higher blast counts. Am. J. Hematol. 2015, 90, E139–E141. [Google Scholar] [CrossRef] [PubMed]
- Mayer, J.; Arthur, C.; Delaunay, J.; Mazur, G.; Thomas, X.G.; Wierzbowska, A.; Ravandi, F.; Berrak, E.; Jones, M.; Li, Y.; et al. Multivariate and subgroup analyses of a randomized, multinational, phase 3 trial of decitabine vs. treatment choice of supportive care or cytarabine in older patients with newly diagnosed acute myeloid leukemia and poor- or intermediate-risk cytogenetics. BMC Cancer 2014, 14, 69. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Miller, A.; Gandhi, S.; Ford, L.A.; Vigil, C.E.; Griffiths, E.A.; Thompson, J.E.; Wetzler, M.; Wang, E.S. Comparison of epigenetic versus standard induction chemotherapy for newly diagnosed acute myeloid leukemia patients ≥60 years old. Am. J. Hematol. 2015, 90, 639–646. [Google Scholar] [CrossRef] [PubMed]
- Lao, Z.; Yiu, R.; Wong, G.C.; Ho, A. Treatment of elderly patients with acute myeloid leukemia with azacitidine results in fewer hospitalization days and infective complications but similar survival compared with intensive chemotherapy. Asia Pac. J. Clin. Oncol. 2015, 11, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Van der Helm, L.H.; Scheepers, E.R.; Veeger, N.J.; Daenen, S.M.; Mulder, A.B.; van den Berg, E.; Vellenga, E.; Huls, G. Azacitidine might be beneficial in a subgroup of older AML patients compared to intensive chemotherapy: A single centre retrospective study of 227 consecutive patients. J. Hematol. Oncol. 2013, 6, 29. [Google Scholar] [CrossRef] [PubMed]
- Jabbour, E.; Mathisen, M.S.; Garcia-Manero, G.; Champlin, R.; Popat, U.; Khouri, I.; Giralt, S.; Kadia, T.; Chen, J.; Pierce, S.; et al. Allogeneic hematopoietic stem cell transplantation versus hypomethylating agents in patients with myelodysplastic syndrome: A retrospective case-control study. Am. J. Hematol. 2013, 88, 198–200. [Google Scholar] [CrossRef] [PubMed]
- Ravandi, F.; Issa, J.P.; Garcia-Manero, G.; O’Brien, S.; Pierce, S.; Shan, J.; Borthakur, G.; Verstovsek, S.; Faderl, S.; Cortes, J.; et al. Superior outcome with hypomethylating therapy in patients with acute myeloid leukemia and high-risk myelodysplastic syndrome and chromosome 5 and 7 abnormalities. Cancer 2009, 115, 5746–5751. [Google Scholar] [CrossRef] [PubMed]
- Almeida, A.; Ferreira, A.R.; Costa, M.J.; Silva, S.; Alnajjar, K.; Bogalho, I.; Pierdomenico, F.; Esteves, S.; Alpoim, M.; Braz, G.; et al. Clinical outcomes of AML patients treated with Azacitidine in Portugal: A retrospective multicenter study. Leuk. Res. Rep. 2017, 7, 6–10. [Google Scholar] [CrossRef] [PubMed]
- Hansen, S.B.; Dufva, I.H.; Kjeldsen, L. Durable complete remission after azacitidine treatment in a patient with erythroleukaemia. Eur. J. Haematol. 2012, 89, 369–370. [Google Scholar] [CrossRef] [PubMed]
- Hangai, S.; Nakamura, F.; Kamikubo, Y.; Honda, A.; Arai, S.; Nakagawa, M.; Ichikawa, M.; Kurokawa, M. Erythroleukemia showing early erythroid and cytogenetic responses to azacitidine therapy. Ann. Hematol. 2013, 92, 707–709. [Google Scholar] [CrossRef] [PubMed]
- Vigil, C.E.; Cortes, J.; Kantarjian, H.; Garcia-Manero, G.; Lancet, J.; List, A. Hypomethylating Therapy for the Treatment of Acute Erythroleukemia Patients. Blood 2009, 114, 2069. [Google Scholar]
- King, R.J.; Crouch, A.; Radojcic, V.; Marini, B.L.; Perissinotti, A.J.; Bixby, D. Therapeutic Outcomes of Patients with Acute Erythroid Leukemia Treated with Hypomethylating Agents. Blood 2016, 128, 5203. [Google Scholar]
- Uchida, T.; Hagihara, M.; Hua, J.; Inoue, M. The effects of azacitidine on the response and prognosis of myelodysplastic syndrome and acute myeloid leukemia involving a bone marrow erythroblast frequency of >50. Leuk. Res. 2016, 53, 35–38. [Google Scholar] [CrossRef] [PubMed]
- Steger, G.G.; Dittrich, C.; Chott, A.; Derfler, K.; Schwarzmeier, J.D. Long-term remission in a patient with erythroleukemia following interferon-α treatment. J. Biol. Response Modif. 1989, 8, 351–354. [Google Scholar]
- Camera, A.; Volpicelli, M.; Villa, M.R.; Risitano, A.M.; Rossi, M.; Rotoli, B. Complete remission induced by high dose erythropoietin and granulocyte colony stimulating factor in acute erythroleukemia (AML-M6 with maturation). Haematologica 2002, 87, 1225–1227. [Google Scholar] [PubMed]
- Creusot, F.; Acs, G.; Christman, J.K. Inhibition of DNA methyltransferase and induction of Friend erythroleukemia cell differentiation by 5-azacytidine and 5-aza-2’-deoxycytidine. J. Biol. Chem. 1982, 257, 2041–2048. [Google Scholar] [PubMed]
- Gambari, R.; del Senno, L.; Barbieri, R.; Viola, L.; Tripodi, M.; Raschella, G.; Fantoni, A. Human leukemia K-562 cells: Induction of erythroid differentiation by 5-azacytidine. Cell Differ. 1984, 14, 87–97. [Google Scholar] [CrossRef]
- Zucker, R.M.; Decal, D.L.; Whittington, K.B. 5-Azacytidine increases the synthesis of embryonic hemoglobin (E2) in murine erythroleukemic cells. FEBS Lett. 1983, 162, 436–441. [Google Scholar] [CrossRef]
- Ando, T.; Nishimura, M.; Oka, Y. Decitabine (5-Aza-2′-deoxycytidine) decreased DNA methylation and expression of MDR-1 gene in K562/ADM cells. Leukemia 2000, 14, 1915–1920. [Google Scholar] [CrossRef] [PubMed]
- Efferth, T.; Futscher, B.W.; Osieka, R. 5-Azacytidine modulates the response of sensitive and multidrug-resistant K562 leukemic cells to cytostatic drugs. Blood Cells Mol. Dis. 2001, 27, 637–648. [Google Scholar] [CrossRef] [PubMed]
- Pleyer, L.; Greil, R. Digging deep into “dirty” drugs—Modulation of the methylation machinery. Drug Metab. Rev. 2015, 47, 252–279. [Google Scholar] [CrossRef] [PubMed]
- Damaj, G.; Duhamel, A.; Robin, M.; Beguin, Y.; Michallet, M.; Mohty, M.; Vigouroux, S.; Bories, P.; Garnier, A.; El Cheikh, J.; et al. Impact of azacitidine before allogeneic stem-cell transplantation for myelodysplastic syndromes: A study by the Societe Francaise de Greffe de Moelle et de Therapie-Cellulaire and the Groupe-Francophone des Myelodysplasies. J. Clin. Oncol. 2012, 30, 4533–4540. [Google Scholar] [CrossRef] [PubMed]
- Figueroa, M.E.; Skrabanek, L.; Li, Y.; Jiemjit, A.; Fandy, T.E.; Paietta, E.; Fernandez, H.; Tallman, M.S.; Greally, J.M.; Carraway, H.; et al. MDS and secondary AML display unique patterns and abundance of aberrant DNA methylation. Blood 2009, 114, 3448–3458. [Google Scholar] [CrossRef]
- Papaemmanuil, E.; Gerstung, M.; Bullinger, L.; Gaidzik, V.I.; Paschka, P.; Roberts, N.D.; Potter, N.E.; Heuser, M.; Thol, F.; Bolli, N.; et al. Genomic Classification and Prognosis in Acute Myeloid Leukemia. N. Engl. J. Med. 2016, 374, 2209–2221. [Google Scholar] [CrossRef] [PubMed]
- Dohner, H.; Estey, E.H.; Amadori, S.; Appelbaum, F.R.; Buchner, T.; Burnett, A.K.; Dombret, H.; Fenaux, P.; Grimwade, D.; Larson, R.A.; et al. Diagnosis and management of acute myeloid leukemia in adults: Recommendations from an international expert panel, on behalf of the European LeukemiaNet. Blood 2010, 115, 453–474. [Google Scholar] [CrossRef] [PubMed]
- Cheson, B.D.; Greenberg, P.L.; Bennett, J.M.; Lowenberg, B.; Wijermans, P.W.; Nimer, S.D.; Pinto, A.; Beran, M.; de Witte, T.M.; Stone, R.M.; et al. Clinical application and proposal for modification of the International Working Group (IWG) response criteria in myelodysplasia. Blood 2006, 108, 419–425. [Google Scholar] [CrossRef] [PubMed]
- R: The R Project for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 12 April 2017).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | HMA All Lines (n = 88) | First-Line HMA (n = 41) | First-Line ICT (n = 122) | p-Value First-Line HMA vs. ICT |
|---|---|---|---|---|
| Median age at diagnosis, years | 69 | 73 | 60 | 0.1698 |
| (min–max) | (28–88) | (44–88) | (20–86) | |
| Male gender, n (%) | 54 (61) | 26 (63) | 88 (72) | 0.3919 |
| BM blasts at start of treatment | ||||
| Median | 22 | 22 | 24 | 0.8576 |
| Mean (Standard Deviation) | 25.8 (17.2) | 25.8 (15.9) | 27.1 (15.8) | |
| Unknown, n (%) | 12 (14) | 2 (5) | 6 (5) | |
| Hemoglobin at start of treatment, n (%) | ||||
| ≤10 g/dL | 55 (63) | 32 (78) | 32/64 (50) | 1.00 |
| Pts. with unknown hemoglobin | 3 (3) | 0 (0) | 71 (58) | |
| Median WBC count at start of treatment, ×109/L (min–max) | 2.35 | 2.42 | 1.81 | 0.7294 |
| (0.1–32.3) | (0.6–24.0) | (0.2–23.9) | ||
| Neutrophil count at start of treatment, n (%) | ||||
| ≤ 0.5 × 109/L | 34 (39) | 18 (44) | 18/57 (31) | 0.7326 |
| Pts. with unknown neutrophil count | 5 (6) | 1 (2) | 79 (65) | |
| Platelet count at start of treatment, n (%) | ||||
| ≤50 × 109/L | 54 (61) | 24 (69) | 62 (51) | 0.8673 |
| Unknown | 3 (3) | 0 (0) | 10 (8) | |
| AML subtype, n (%) | ||||
| Primary | 66 (75) | 35 (85) | 81 (66) | 0.4373 |
| Secondary | 11 (13) | 4 (10) | 17 (14) | |
| Unknown | 11 (13) | 2 (5) | 24 (20) | |
| MRC cytogenetic risk group, n (%) | ||||
| Good risk | 1 (1) | 0 (0) | 0 (0) | 0.6943 |
| Intermediate risk | 39 (44) | 17 (42) | 51 (42) | |
| Poor risk | 45 (51) | 22 (54) | 53 (43) | |
| Unknown | 3 (3) | 2 (5) | 18 (15) |
| HMA All Lines (n = 75) 1 | HMA 1st Line (n = 39) 2 | HMA ≥ 2nd Line (n = 34) 3 | ICT 1st Line (n = 119) 4 | |
|---|---|---|---|---|
| Overall response acc. to ELN, n (%) | 30 (40.0) | 18 (46.2) | 10 (29.4) | 86 (72.3) |
| Complete | 20 (26.7) | 12 (30.8) | 7 (20.6) | 79 (66.4) |
| Partial | 10 (13.3) | 6 (15.4) | 3 (8.8) | 7 (5.9) |
| Overall response including HI, n (%) | 44 (58.7) | 25 (64.1) | 17 (50.0) | ND |
| HI without marrow response | 14 (18.7) | 7 (17.9) | 7 (20.6) | ND |
| ANC | 9 (12.0) | 6 (15.4) | 3 (8.8) | |
| RBC | 7 (9.3) | 5 (12.8) | 2 (5.9) | |
| PLT | 9 (12.0) | 5 (12.8) | 4 (11.8) | |
| Transfusion independence, n/n (%) 5 | ||||
| RBC-TI | 19/55 (35) | 13/32 (40.6) | 6/21 (28.6) | ND |
| PLT-TI | 8/28 (29) | 3/14 (21.4) | 4/12 (33.3) | |
| Stable disease | 26 (34.7) | 11 (28.2) | 15 (44.1) | 16 (13.4) |
| Primary disease progression | 5 (6.7) | 3 (7.7) | 2 (5.9) | 17 (14.3) |
| Time to first response, days 6 | ND | |||
| Median (min–max) | 79 (18–822) 7 | 66 (18–233) | 85 (30–822) | |
| Time to best response, days 8 | ||||
| Median (min–max) | 120 (20–1150) 7 | 143 (20–353) | 89.5 (30–1150) | ND |
| Outcomes | First-Line ICT | First-Line HMA | p-Value |
|---|---|---|---|
| Overall response acc. to ELN, % | 72.3 | 46.2 | 0.016 |
| Complete response | 64.4 | 30.8 | <0.001 |
| Partial response | 5.9 | 15.4 | 0.101 |
| Stable disease, % | 13.4 | 28.2 | 0.001 |
| Primary disease progression, % | 14.3 | 7.7 | 0.004 |
| Median time to best response, months | NA 1 | 89.5 | NA 1 |
| Median PFS, months | 8.0 | 9.4 | 0.107 |
| MRC intermediate cytogenetic risk | 22.7 | 5.9 | 0.004 |
| MRC high cytogenetic risk | 6.5 | 11.3 | 0.279 |
| 1-year PFS, % | 41.8 | 40.6 | 0.896 |
| Median OS total cohort, months | 10.5 | 13.7 | 0.564 |
| MRC intermediate cytogenetic risk | 16.9 | 29.3 | 0.277 |
| MRC high cytogenetic risk | 7.5 | 13.3 | 0.039 |
| 1-year OS total cohort, % | 46.7 | 65.8 | 0.072 |
| PFS Comparison | Hazard Ratio | 95% CI | p-Value |
|---|---|---|---|
| First line AZA vs. ICT | 0.90 | 0.54–1.51 | 0.6907 |
| Cytogenetic risk group: | |||
| High vs. Intermediate | 1.86 | 1.19–2.90 | 0.0064 |
| Age | |||
| Per additional year | 1.03 | 1.01–1.05 | 0.0118 |
| OS Comparison | Hazard Ratio | 95% CI | p-Value |
| First line AZA vs. ICT | 0.75 | 0.45–1.23 | 0.2489 |
| Cytogenetic risk group | |||
| High vs. Intermediate | 2.40 | 1.54–3.69 | <0.0001 |
| Age | |||
| Per additional year | 1.03 | 1.01–1.05 | 0.0032 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almeida, A.M.; Prebet, T.; Itzykson, R.; Ramos, F.; Al-Ali, H.; Shammo, J.; Pinto, R.; Maurillo, L.; Wetzel, J.; Musto, P.; et al. Clinical Outcomes of 217 Patients with Acute Erythroleukemia According to Treatment Type and Line: A Retrospective Multinational Study. Int. J. Mol. Sci. 2017, 18, 837. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms18040837
Almeida AM, Prebet T, Itzykson R, Ramos F, Al-Ali H, Shammo J, Pinto R, Maurillo L, Wetzel J, Musto P, et al. Clinical Outcomes of 217 Patients with Acute Erythroleukemia According to Treatment Type and Line: A Retrospective Multinational Study. International Journal of Molecular Sciences. 2017; 18(4):837. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms18040837
Chicago/Turabian StyleAlmeida, Antonio M., Thomas Prebet, Raphael Itzykson, Fernando Ramos, Haifa Al-Ali, Jamile Shammo, Ricardo Pinto, Luca Maurillo, Jaime Wetzel, Pellegrino Musto, and et al. 2017. "Clinical Outcomes of 217 Patients with Acute Erythroleukemia According to Treatment Type and Line: A Retrospective Multinational Study" International Journal of Molecular Sciences 18, no. 4: 837. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms18040837