Serum Biomarkers for Discrimination between Hepatitis C-Related Arthropathy and Early Rheumatoid Arthritis

 , , , , , ,
, , , , , ,  , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Clinical Characteristics of the Study Subjects
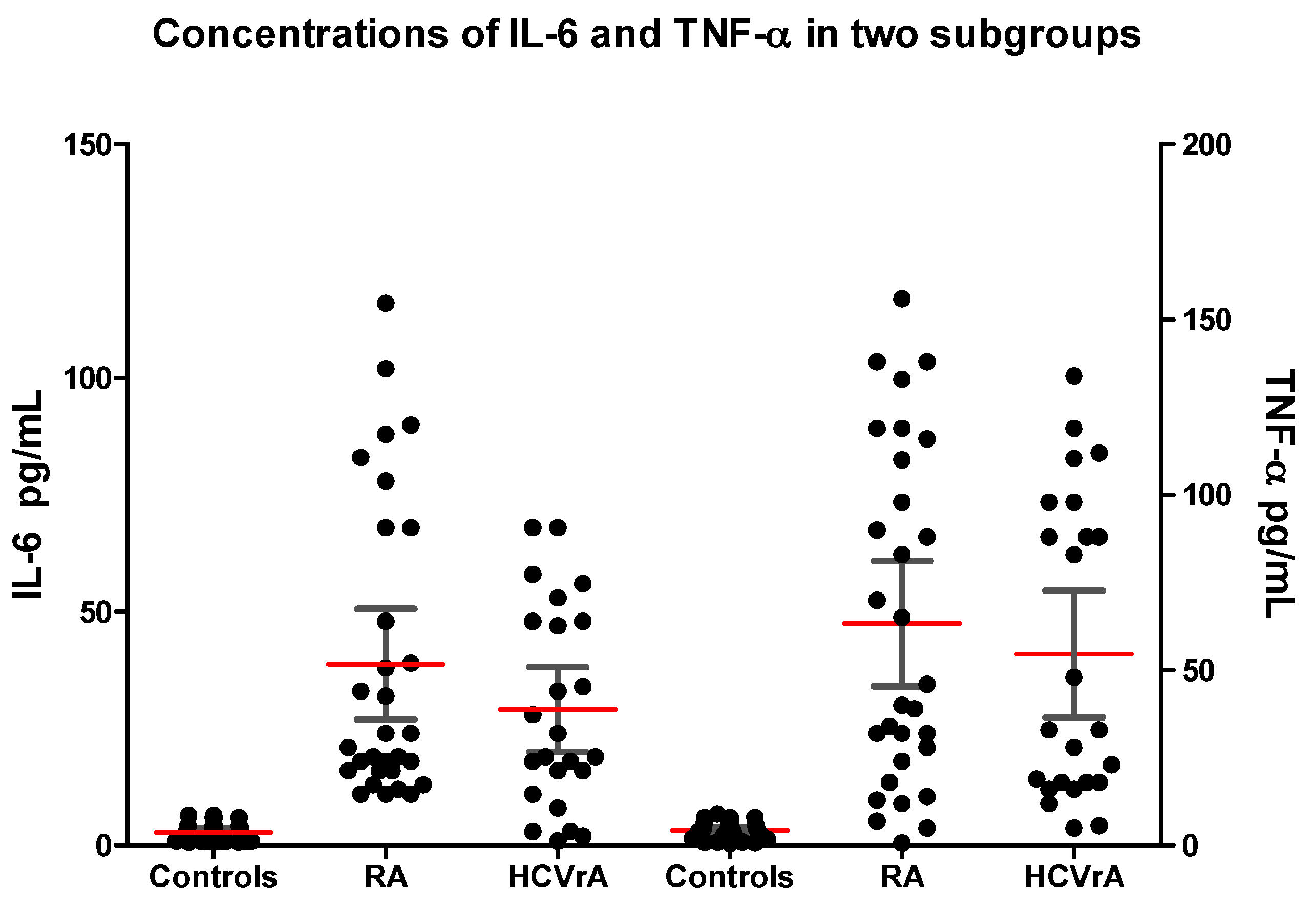
2.2. Cytokines Concentrations
2.3. Auto-Antibodies Concentrations
2.4. Correlations Between IL-6, TNF-α and Auto-Antibodies in eRA and HCVrA
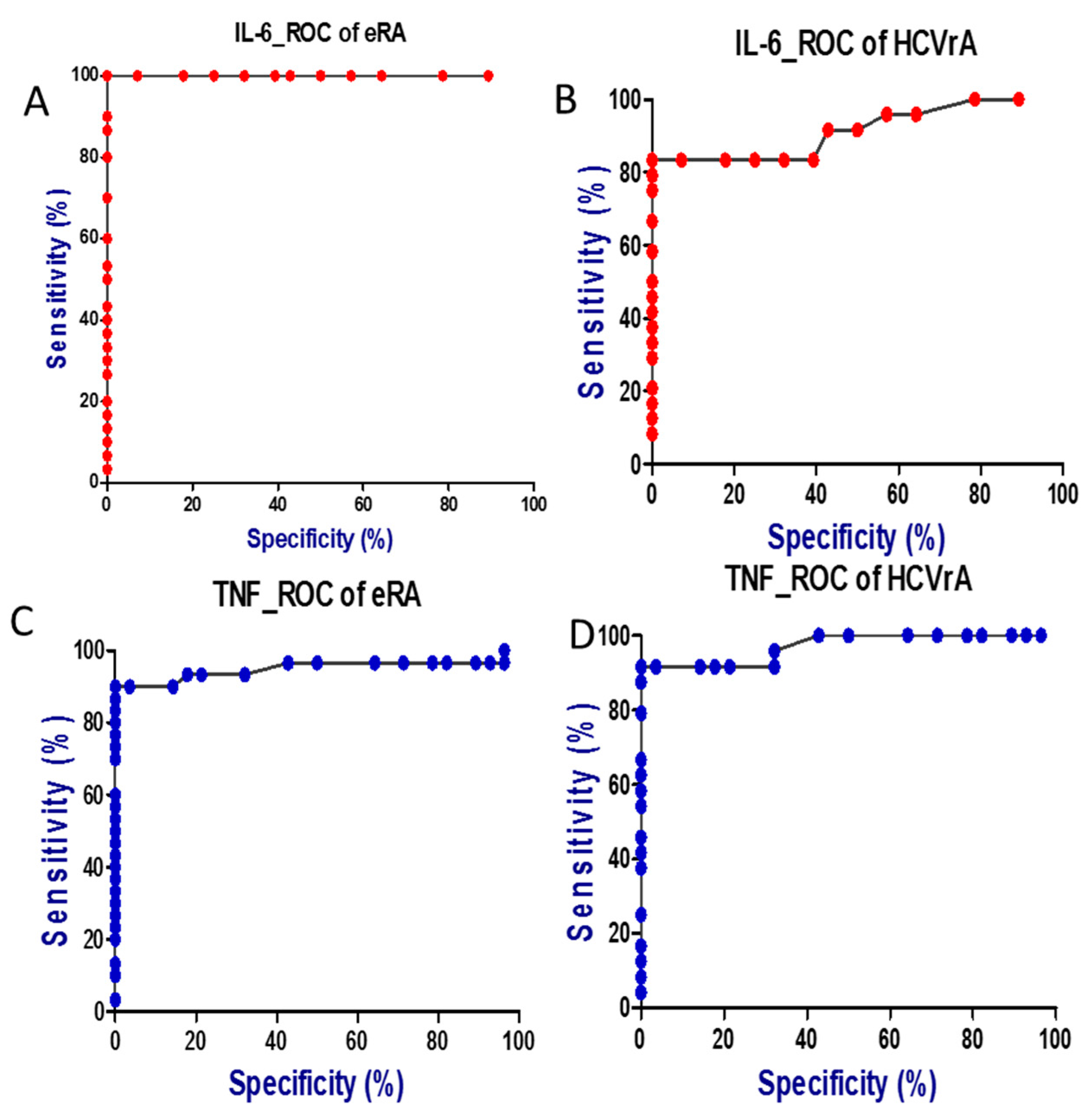
2.5. Diagnostic Performance of IL-6 and TNF-α as Disease Markers
3. Discussion
4. Materials and Methods
4.1. Subjects and Clinical Assessment
4.2. Samples Collection
4.3. Immunological Investigations
4.4. Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Houghton, M. The long and winding road leading to the identifcation of the hepatitis C virus. J. Hepatol. 2009, 51, 939–948. [Google Scholar] [CrossRef] [PubMed]
- Palazzi, C.; D’Amico, E.; D’Angelo, S.; Gilio, M.; Olivieri, I. Rheumatic manifestations of hepatitis C virus chronic infection: Indications for a correct diagnosis. World J. Gastroenterol. 2016, 22, 1405–1410. [Google Scholar] [CrossRef] [PubMed]
- Sayiner, Z.A.; Haque, U.; Malik, M.U.; Gurakar, A. Hepatitis C Virus Infection and Its Rheumatologic Implications. Gastroenterol. Hepatol. 2014, 10, 287–293. [Google Scholar]
- Zuckerman, E.; Yeshurun, D.; Rosner, I. Management of Hepatitis C Virus-Related Arthritis. BioDrugs 2001, 15, 573–584. [Google Scholar] [CrossRef] [PubMed]
- Poantă, L.; Albu., A. Chronic Hepatitis C with extrahepatic manifestations. Rom. J. Intern. Med. 2007, 45, 85–88. [Google Scholar]
- Yang, D.H.; Ho, L.J.; Lai, J.H. Useful biomarkers for assessment of Hepatitis C virus infection-associated autoimmune disorders. World J. Gastroenterol. 2014, 20, 2962–2970. [Google Scholar] [CrossRef] [PubMed]
- Lormeau, C.; Falgarone, G.; Roulot, D.; Boissier, M.C. Rheumatologic manifestations of chronic Hepatitis C infection. Jt. Bone Spine 2006, 73, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Ferri, C.; Sebastiani, M.; Antonelli, A.; Colaci, M.; Manfredi, A.; Giuggioli, D. Current treatment of Hepatitis C-associated rheumatic diseases. Arthritis Res. Ther. 2012, 14, 215. [Google Scholar] [CrossRef] [PubMed]
- Kemmer, N.M.; Sherman, K.E. Hepatitis C-related arthropathy: Diagnostic and treatment considerations. J. Musculoskelet. Med. 2010, 27, 351–354. [Google Scholar] [PubMed]
- Kaptanoğlu, E.; Nadir, I.; Bakici, Z.; Hayta, E.; Türkmen, M.; Sezer, H.; Hizmetli, S.; Elden, H. Differentiation of Rheumatoid Arthritis from HCV Infection: Rheumatoid Factor, Anti-Cyclic Citrullinated Peptide or Anti-Mutated Citrullinated Vimentin? Arch. Rheumatol. 2010, 25, 19–23. [Google Scholar] [CrossRef]
- Lutzky, V.; Hannawi, S.; Thomas, R. Cells of the synovium in rheumatoid arthritis. Dendritic cells. Arthritis Res. Ther. 2007, 9, 219. [Google Scholar] [CrossRef] [PubMed]
- Choy, E. Understanding the dynamics: Pathways involved in the pathogenesis of rheumatoid arthritis. Rheumatology 2012, 51, v3–v11. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.W.; Kang, E.H. Autoantibodies in rheumatoid arthritis: Rheumatoid factors and anticitrullinated protein antibodies. QJM 2010, 103, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Conca, P.; Tarantino, G. Hepatitis C virus lymphotropism and peculiar immunological phenotype: Effects on natural history and antiviral therapy. World J. Gastroenterol. 2009, 15, 2305–2308. [Google Scholar] [CrossRef] [PubMed]
- luo, J.C.; Hwang, S.J.; Li, C.P.; Lu, R.H.; Chan, C.Y.; Wu, J.C.; Chang, F.Y.; Lee, S.D. Clinical significance of serum auto-antibodies in Chinese patients with chronic Hepatitis C: Negative role of serum viral titre and genotype. J. Gastroenterol. Hepatol. 1998, 13, 475–479. [Google Scholar] [CrossRef] [PubMed]
- Buskila, D.; Shnaider, A.; Neumann, L.; Lorber, M.; Zilberman, D.; Hilzenrat, N.; Kuperman, O.J.; Sikuler, E. Musculoskeletal manifestations and autoantibody profile in 90 Hepatitis C virus infected Israeli patients. Semin Arthritis Rheum. 1998, 28, 107–113. [Google Scholar] [CrossRef]
- Narciso–Schiavon, J.L.; Freire, F.C.F.; Suarez, M.M.; Ferrari, M.V.O.; Scanhola, G.Q.; de Lucca Schiavon, L.; de Carvalho Filho, R.J.; Ferraz, M.L.G.; Silva, A.E.B. Antinuclear antibody positivity in patients with chronic hepatitis C: Clinically relevant or an epiphenomenon? Eur. J. Gastroenterol. Hepatol. 2009, 21, 440–446. [Google Scholar] [CrossRef] [PubMed]
- Mahler, M.; Hanly, J.G.; Fritzler, M.J. Importance of the dense fine speckled pattern on HEp-2 cells and anti-DFS70 antibodies for the diagnosis of systemic autoimmune diseases. Autoimmun. Rev. 2012, 11, 642–645. [Google Scholar] [CrossRef] [PubMed]
- Dalekos, G.N.; Kistis, K.G.; Boumba, D.S.; Voulgari, P.; Zervou, E.K.; Drosos, A.A.; Tsianos, E.V. Increased incidence of anti-cardiolipin antibodies in patients with hepatitis C is not associated with aetiopathogenetic link to anti-phospholipid syndrome. Eur. J. Gastroenterol. Hepatol. 2000, 12, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Rodríguez, F.J.; Tàssies, D.; Font, J.; Reverter, J.C.; Cervera, R.; Sánchez-Tapias, J.M.; Mazzara, R.; Ordinas, A.; Ingelmo, M. Prevalence of Hepatitis C virus infection in patients with antiphospholipid syndrome. J. Hepatol. 1999, 30, 770–773. [Google Scholar] [CrossRef]
- Abuaf, N.; Lunel, F.; Giral, P.; Borotto, E.; Laperche, S.; Poupon, R.; Opolon, P.; Huraux, J.M.; Homberg, J.C. Non-organ specific autoantibodies associated with chronic C virus hepatitis. J. Hepatol. 1993, 18, 359–364. [Google Scholar] [CrossRef]
- Prieto, J.; Yuste, J.R.; Beloqui, O.; Civeira, M.P.; Riezu, J.I.; Aguirre, B.; Sangro, B. Anticardiolipin antibodies in chronic hepatitis C. Implication of hepatitis C virus as the cause of the antiphospholipid syndrome. Hepatology 1996, 23, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Ordi–Ros, J.; Villarreal, J.; Monegal, F.; Sauleda, S.; Esteban, I.; Vilardell, M. Anticardiolipin Antibodies in Patients with Chronic Hepatitis C Virus Infection: Characterization in Relation to Antiphospholipid Syndrome. Clin. Diagn. Lab. Immunol. 2000, 7, 241–244. [Google Scholar] [PubMed]
- Palazzi, C.; Olivieri, I.; Cacciatore, P.; Pennese, E.; D'Amico, E. Difficulties in the differential diagnosis between primitive rheumatic diseases and hepatitis C virus-related disorders. Clin. Exp. Rheumatol. 2005, 23, 2–6. [Google Scholar] [PubMed]
- Ingegnoli, F.; Castelli., R.; Gualtierotti., R. Rheumatoid Factors: Clinical Applications. Dis. Markers 2013, 35, 727–734. [Google Scholar] [CrossRef] [PubMed]
- Deane, K.D.; O'Donnell, C.I.; Hueber, W.; Majka, D.S.; Lazar, A.A.; Derber, L.A.; Gilliland, W.R.; Edison, J.D.; Norris, J.M.; Robinson, W.H.; et al. The number of elevated cytokines and chemokines in preclinical seropositive rheumatoid arthritis predicts time to diagnosis in an agedependent manner. Arthritis Rheum. 2010, 62, 3161–3172. [Google Scholar] [CrossRef] [PubMed]
- Deane, K.D.; Norris, J.M.; Holers, V.M. Preclinical rheumatoid arthritis: Identification, evaluation, and future directions for investigation. Rheum. Dis. Clin. N. Am. 2010, 36, 213–241. [Google Scholar] [CrossRef] [PubMed]
- Al-Dahshan, M.A.; Al-Dahshan, T.A. Hepatitis C virus infection associated arthritis. J. Egypt Soc. Parasitol. 2012, 42, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Örge, E.; Cefle, A.; Gürel-Polat, N.; Hulagu, S. The positivity of rheumatoid factor and anti-cyclic citrullinated peptide antibody in nonarthritic patients with chronic hepatitis C infection. Rheumatol. Int. 2010, 30, 485–488. [Google Scholar] [CrossRef] [PubMed]
- Sene, D.; Ghillani-Dalbin, P.; Limal, N.; Thibault, V.; Van Boekel, T.; Piette, J.C.; Cacoub, P. Anti-cyclic citrullinated peptide antibodies in hepatitis C virus associated rheumatological manifestations and Sjogren’s syndrome. Ann. Rheum. Dis. 2006, 65, 394–397. [Google Scholar] [CrossRef] [PubMed]
- Shmerling, R.H.; Delbanco, T.L. How useful is the rheumatoid factor? An analysis of sensitivity, specificity, and predictive value. Arch. Intern. Med. 1992, 152, 2417–2420. [Google Scholar] [CrossRef] [PubMed]
- Clifford, B.D.; Donahue, D.; Smith, L.; Cable, E.; Luttig, B.; Manns, M.; Bonkovsky, H.L. High prevalence of serological markers of autoimmunity in patients with chronic hepatitis C. Hepatology 1995, 21, 613–619. [Google Scholar] [PubMed]
- Lienesch, D.; Morris, R.; Metzger, A.; Debuys, P.; Sherman, K. Absence of cyclic citrullinated peptide antibody in nonarthritic patients with chronic hepatitis C infection. J. Rheumatol. 2005, 32, 489–493. [Google Scholar] [PubMed]
- Wener, M.H.; Hutchinson, K.; Morishima, C.; Gretch, D.R. Absence of antibodies to cyclic citrullinated peptide in sera of patients with Hepatitis C virus infection and cryoglobulinemia. Arthritis Rheum. 2004, 50, 2305–2508. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, K.; Sugiyama, D.; Kogata, Y.; Tsuji, G.; Nakazawa, T.; Kawano, S.; Saigo, K.; Morinobu, A.; Koshiba, M.; Kuntz, K.M.; Kamae, I. Meta-analysis: Diagnostic accuracy of anti-cyclic citrullinated peptide antibody and rheumatoid factor for rheumatoid arthritis. Ann. Intern. Med. 2007, 146, 797–808. [Google Scholar] [CrossRef] [PubMed]
- Anzilotti, C.; Merlini, G.; Pratesi, F.; Tommasi, C.; Chimenti, D.; Migliorini, P. Antibodies to viral citrullinated peptide in rheumatoid arthritis. J. Rheumatol. 2006, 33, 647–651. [Google Scholar] [PubMed]
- Vander Cruyssen, B.; Hoffman, I.E.; Zmierczak, H.; Van den Berghe, M.; Kruithof, E.; De Rycke, L.; Mielants, H.; Veys, E.M.; Baeten, D.; de Keyser, F. Anti-citrullinated peptide antibodies may occur in patients with psoriatic arthritis. Ann. Rheum. Dis. 2005, 64, 1145–1149. [Google Scholar] [CrossRef] [PubMed]
- Gottenberg, J.E.; Mignot, S.; Nicaise-Rolland, P.; Cohen-Solal, J.; Aucouturier, F.; Goetz, J.; Labarre, C.; Meyer, O.; Sibilia, J.; Mariette, X. Prevalence of anti-cyclic citrullinated peptide and anti-keratin antibodies in patients with primary Sjogren’s syndrome. Ann. Rheum. Dis. 2005, 64, 114–117. [Google Scholar] [CrossRef] [PubMed]
- Bombardieri, M.; Alessandri, C.; Labbadia, G.; Iannuccelli, C.; Carlucci, F.; Riccieri, V.; Paoletti, V.; Valesini, G. Role of anti-cyclic citrullinated peptide antibodies in discriminating patients with rheumatoid arthritis from patients with chronic hepatitis C infection-associated polyarticular involvement. Arthritis Res. Ther. 2004, 6, R137–R141. [Google Scholar] [CrossRef] [PubMed]
- Caspi, D.; Anouk, M.; Golan, I.; Paran, D.; Kaufman, I.; Wigler, I.; Levartovsky, D.; Litinsky, I.; Elkayam, O. Synovial fluid levels of anti-cyclic citrullinated peptide antibodies and IgA rheumatoid factor in rheumatoid arthritis, psoriatic arthritis, and osteoarthritis. Arthritis Care Res. 2006, 55, 53–56. [Google Scholar] [CrossRef] [PubMed]
- Low, J.M.; Chauhan, A.K.; Kietz, D.A.; Daud, U.; Pepmueller, P.H.; Moore, T.L. Determination of anti-cyclic citrullinated peptide antibodies in the sera of patients with juvenile idiopathic arthritis. J. Rheumatol. 2004, 31, 1829–1833. [Google Scholar] [PubMed]
- Pinheiro, G.C.; Scheinberg, M.A.; Aparecida da Silva, M.; Maciel, S. Anti-cyclic citrullinated peptide antibodies in advanced rheumatoid arthritis. Ann. Intern. Med. 2003, 139, 234–235. [Google Scholar] [CrossRef] [PubMed]
- Antonelli, A.; Ferri, C.; Galeazzi, M.; Giannitti, C.; Manno, D.; Mieli-Vergani, G.; Menegatti, E.; Olivieri, I.; Puoti, M.; Palazzi, C.; et al. HCV infection: Pathogenesis, clinical manifestations and therapy. Clin. Exp. Rheumatol. 2008, 26, S39–S47. [Google Scholar] [PubMed]
- Riccio, A.; Postiglione, L.; La Dogana, P.; Spano, A.; Marzocchella, C.; Tarantino, G. Anti-cyclic citrullinated peptide antibodies in patients affected by HCV-related arthritis. J. Biol. Regul. Homeost Agents 2008, 22, 57–61. [Google Scholar] [PubMed]
- Antonelli, A.; Ferri, C.; Ferrari, S.M.; Colaci, M.; Fallahi, P. Immunopathogenesis of HCV-related endocrine manifestations in chronic hepatitis and mixed cryoglobulinemia. Autoimmun. Rev. 2008, 8, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Han, Z.Q.; Huang, T.; Deng, Y.Z.; Zhu, G.Z. Expression profile and kinetics of cytokines and chemokines in patients with chronic hepatitis C. Int. J. Clin. Exp. Med. 2015, 8, 17995–18003. [Google Scholar] [PubMed]
- Danis, V.A.; Franic, G.M.; Rathjen, D.A; Laurent, R.M.; Brooks, P.M. Circulating cytokine levels in patients with rheumatoid arthritis: Results of a double blind trial with sulphasalazine. Ann. Rheum. Dis. 1992, 51, 946–950. [Google Scholar] [CrossRef] [PubMed]
- Kishimoto, T. IL-6: From its discovery to clinical applications. Int. Immunol. 2010, 22, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Antonelli, A.; Ferri, C.; Ferrari, S.M.; Ghiri, E.; Marchi, S.; Colaci, M.; Bruschi, F.; Fallahi, P. High interleukin-6 and tumor necrosis factor-α serum levels in hepatitis C infection associated or not with mixed cryoglobulinemia. Clin. Rheumatol. 2009, 28, 1179–1185. [Google Scholar] [CrossRef] [PubMed]
- Riccio, A.; Postiglione, L.; Sabatini, P.; Linvelli, M.; Soriente, I.; Sangiolo, M.G.; Amato, P.; Tarantino, G. Similar serum levels of IL-6 and its soluble receptors in patients with HCV–related arthritis and rheumatoid arthritis: A pilot study. Int. J. Immunopathol. Pharmacol. 2012, 25, 281–285. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.J.; Kwon, Y.J.; Park, M.C.; Park, Y.B.; Lee, S.K. The correlation between increased serum concentrations of interleukin-6 family cytokines and disease activity in rheumatoid arthritis patients. Yonsei Med. J. 2011, 52, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Lapiński, T.W. The levels of IL-1β, IL-4 and IL-6 in the serum and the liver tissue of chronic HCV–infected patients. Arch. Immunol. Ther. Exp. 2001, 49, 311–316. [Google Scholar]
- Nelson, D.R.; Lim, H.L.; Marousis, C.G.; Fang, J.W.; Davis, G.L.; Shen, L.; Urdea, M.S.; Kolberg, J.A.; Lau, J.Y. Activation of tumor necrosis factor-α system in chronic hepatitis C virus infection. Dig. Dis. Sci. 1997, 42, 2487–2494. [Google Scholar] [CrossRef] [PubMed]
- Lam, J.; Takeshita, S.; Barker, J.E.; Kanagawa, O.; Ross, F.P.; Teitelbaum, S.L. TNF-α induces osteoclastogenesis by direct stimulation of macrophages exposed to permissive levels of RANK ligand. J. Clin. Investig. 2000, 106, 1481–1488. [Google Scholar] [CrossRef] [PubMed]
- Feldmann, M.; Brennan, F.M.; Williams, R.O.; Cope, A.P.; Gibbons, D.L.; Katsikis, P.D.; Maini, R.N. Evaluation of the role of cytokines in autoimmune disease: The importance of TNF-α in rheumatoid arthritis. Prog. Growth Factor Res. 1992, 4, 247–255. [Google Scholar] [CrossRef]
- Siloşi, I.; Boldeanu, M.V.; Cojocaru, M.; Biciuşcă, V.; Pădureanu, V.; Bogdan, M.; Badea, R.G.; Avramescu, C.; Petrescu, I.O.; Petrescu, F.; Siloşi, C.A. The Relationship of Cytokines IL-13 and IL-17 with Autoantibodies Profile in Early Rheumatoid Arthritis. J. Immunol. Res. 2016, 2016, 3109135. [Google Scholar] [CrossRef] [PubMed]
- Harrison, B.J.; Symmons, D.P.; Barrett, E.M.; Silman, A.J. The performance of the 1987 ARA classification criteria for rheumatoid arthritis in a population based cohort of patients with early inflammatory polyarthritis. American Rheumatism Association. J. Rheumatol. 1998, 25, 2324–2330. [Google Scholar] [PubMed]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O.; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; Combe, B. Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Ann. Rheum. Dis. 2010, 69, 1580–1588. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Character | eRA Subgroup 1 (n = 30) | HCVrA Subgroup 2 (n = 24) | p Value | Controls (n = 28) |
|---|---|---|---|---|
| Age (years) (mean ± stdv) | 55.77 ± 10.87 | 54.42 ± 7.49 | p = 0.342 | 52.36 ± 3.38 |
| Gender (female /male) | 24/6 (80%) | 14/10 (67%) | − | 22/6 (78.5%) |
| CRP (mg/dL) | 16.97 ± 5.14 | 16.27 ± 8.24 | p < 0.0001 | 4.75 ± 2.15 |
| ESR (mm/1st h) | 33.60 ± 12.35 | 15.71 ± 6.33 | p < 0.0001 | 11.68 ± 6.24 |
| Cryoglobulinemia | 13.33% | 28% |
| Parameter (Mean, 95% CI) | Levels in Subgroup 1 | Levels in Subgroup 2 | Levels in Subgroups | ||||||
|---|---|---|---|---|---|---|---|---|---|
| RA | Control | p | HCVrA | Control | p | RA | HCVrA | p | |
| IL-6 (pg/mL) | 38.77 (26.93–50.60) | 2.85 (2.08–3.62) | < 0.0001 | 29.13 (20.01–38.24) | 2.85 (2.08–3.62) | < 0.0001 | 38.77 (26.93–50.60) | 29.13 (20.01–38.24) | = 0.388 |
| TNF-α (pg/mL) | 63.32 (45.39–81.26) | 4.29 (3.33–5.25) | < 0.0001 | 54.63 (36.50–72.76) | 4.29 (3.33–5.25) | < 0.0001 | 63.32 (45.39–81.26) | 54.63 (36.50–72.76) | = 0.481 |
| ANA (U/mL) | 12.43 (9.35–15.52) | 4.55 (3.84–5.28) | < 0.0001 | 17.67 (15.76–19.58) | 4.55 (3.84–5.28) | < 0.0001 | 12.43 (9.35–15.52) | 17.67 (15.76–19.58) | = 0.006 |
| IgG anti-CCP (U/L) | 100.40 (69.45–131.30) | 5.75 (4.34–7.16) | < 0.0001 | 16.99 (14.92–19.07) | 5.75 (4.34–7.16) | < 0.0001 | 100.40 (69.45–131.30) | 16.99 (14.92–19.07) | < 0.0001 |
| IgM-RF (U/L) | 65.27 (45.71–84.83) | 5.07 (3.95–6.19) | < 0.0001 | 44.42 (31.88–56.96) | 5.07 (3.95–6.19) | < 0.0001 | 65.27 (45.71–84.83) | 44.42 (31.88–56.96) | = 0.276 |
| IgG anti-aCL (U/mL) | 13.97 (11.19–16.74) | 5.82 (4.41–7.24) | < 0.0001 | 16.12 (12.85–19.38) | 5.82 (4.41–7.24) | < 0.0001 | 13.97 (11.19–16.74) | 16.12 (12.85–19.38) | = 0.346 |
| CRP (mg/dL) | 16.97 (15.06–18.89) | 4.75 (3.92–5.59) | < 0.0001 | 16.27 (12.79–19.75) | 4.75 (3.92–5.59) | < 0.0001 | 16.97 (15.06–18.89) | 16.27 (12.79–19.75) | < 0.0001 |
| ESR (mm/1st h) | 33.60 (28.99–38.21) | 11.68 (9.47–14.31) | < 0.0001 | 15.71 (13.04–18.39) | 11.68 (9.47–14.31) | < 0.0001 | 33.60 (28.99–38.21) | 15.71 (13.04–18.39) | < 0.0001 |
| Parameter | ANA | IgG Anti-aCL | IgM-RF | IgG Anti-CCP | IL-6 | TNF-α | CRP | ESR |
|---|---|---|---|---|---|---|---|---|
| ANA | r = −0.069 p = 0.717 | r = 0.273 p = 0.145 | r = −0.157 p = 0.407 | r = −0.026 p = 0.890 | r = 0.076 p = 0.688 | r = 0.251 p = 0.181 | r = 0.089 p = 0.639 | |
| IgG anti-aCL | r = −0.320 p = 0.049 * | r = 0.052 p = 0.784 | r = 0.158 p = 0.460 | r = 0.349 p = 0.050 * | r = 0,129 p = 0.496 | r = 0.274 p = 0.142 | ||
| IgM-RF | r = 0.418 p = 0.022 * | r = −0.231 p = 0.219 | r = −0.131 p = 0.492 | r = 0.294 p = 0.115 | r = 0.071 p = 0.709 | |||
| IgG anti-CCP | r = 0.371 p = 0.044 * | r = −0.231 p = 0.219 | r = −0.039 p = 0.837 | r = −0.005 p = 0.979 | ||||
| IL-6 | r = 0.337 p = 0.049 * | r = 0.017 p = 0.928 | r = 0.029 p = 0.877 | |||||
| TNF-α | r = −0.404 p = 0.027 * | r = 0.112 p = 0.557 | ||||||
| CRP | r = −0.020 p = 0.916 |
| Parameter | ANA | IgG Anti-aCL | IgM-RF | IgG Anti-CCP | IL-6 | TNF-α | CRP | ESR |
|---|---|---|---|---|---|---|---|---|
| ANA | r = 0.649 p < 0.0001* | r = 0.077 p = 0.721 | r = 0.428 p = 0.037 * | r = −0.202 p = 0.345 | r = −0.160 p = 0.456 | r = −0.037 p = 0.864 | r = 0.303 p = 0.149 | |
| IgG anti-aCL | r = 0.070 p = 0.744 | r = 0.694 p < 0.0001 * | r = −0.056 p = 0.794 | r = −0.411 p = 0.046* | r = 0.140 p = 0.515 | r = −0.050 p = 0.817 | ||
| IgM-RF | r = −0.203 p = 0.498 | r = 0.578 p = 0.003* | r = −0.052 p = 0.809 | r = −0.269 p = 0.204 | r = 0.210 p = 0.325 | |||
| IgG anti-CCP | r = −0.054 p = 0.802 | r = −0.122 p = 0.571 | r = 0.185 p = 0.386 | r = −0.139 p = 0.516 | ||||
| IL-6 | r = −0.154 p = 0.471 | r = −0.101 p = 0.640 | r = 0.298 p = 0.158 | |||||
| THF-α | r = 0.050 p = 0.816 | r = 0.015 p = 0.944 | ||||||
| CRP | r = −0.342 p = 0.101 |
| Parameter | AUC Accuracy | Cut-off Value | p Value | Sensitivity % | Specificity % | Youden Index | |
|---|---|---|---|---|---|---|---|
| RA | IL-6 | 1.000 | 8.75 | <0.0001 | 100.00 | 100.00 | 1.000 |
| TNF-α | 0.950 | 10.50 | <0.0001 | 90.00 | 100.00 | 0.900 | |
| IgG anti-CCP | 0.982 | 11.50 | <0.0001 | 96.67 | 96.43 | 0.931 | |
| ANA | 0.798 | 9.00 | 0.0001 | 63.33 | 100.00 | 0.633 | |
| IgM-RF | 0.991 | 9.50 | <0.0001 | 100.00 | 96.43 | 0.964 | |
| IgG anti-aCL | 0.824 | 11.50 | <0.0001 | 60.00 | 92.86 | 0.529 | |
| HCVrA | IL-6 | 0.975 | 7.25 | <0.0001 | 100.00 | 96.43 | 0.964 |
| TNF-α | 0.971 | 10.50 | <0.0001 | 91.67 | 100.00 | 0.917 | |
| IgG anti-CCP | 0.914 | 7.25 | <0.0001 | 83.33 | 100.00 | 0.833 | |
| ANA | 1.000 | 9.20 | <0.0001 | 100.00 | 100.00 | 1.000 | |
| IgM-RF | 0.935 | 15.00 | <0.0001 | 87.50 | 96.43 | 0.839 | |
| IgG anti-aCL | 0.891 | 11.50 | <0.0001 | 79.17 | 92.86 | 0.720 | |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siloşi, I.; Boldeanu, L.; Biciuşcă, V.; Bogdan, M.; Avramescu, C.; Taisescu, C.; Padureanu, V.; Boldeanu, M.V.; Dricu, A.; Siloşi, C.A. Serum Biomarkers for Discrimination between Hepatitis C-Related Arthropathy and Early Rheumatoid Arthritis. Int. J. Mol. Sci. 2017, 18, 1304. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms18061304
Siloşi I, Boldeanu L, Biciuşcă V, Bogdan M, Avramescu C, Taisescu C, Padureanu V, Boldeanu MV, Dricu A, Siloşi CA. Serum Biomarkers for Discrimination between Hepatitis C-Related Arthropathy and Early Rheumatoid Arthritis. International Journal of Molecular Sciences. 2017; 18(6):1304. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms18061304
Chicago/Turabian StyleSiloşi, Isabela, Lidia Boldeanu, Viorel Biciuşcă, Maria Bogdan, Carmen Avramescu, Citto Taisescu, Vlad Padureanu, Mihail Virgil Boldeanu, Anica Dricu, and Cristian Adrian Siloşi. 2017. "Serum Biomarkers for Discrimination between Hepatitis C-Related Arthropathy and Early Rheumatoid Arthritis" International Journal of Molecular Sciences 18, no. 6: 1304. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms18061304