Treatment of the First Acute Relapse Following Therapeutic Plasma Exchange in Formerly Glucocorticosteroid-Unresponsive Multiple Sclerosis Patients—A Multicenter Study to Evaluate Glucocorticosteroid Responsiveness

 , and
, and
Abstract
:
1. Introduction
2. Results
2.1. Baseline Characteristics and Magnetic Resonance Imaging Findings before the Initiation of Treatment for Relapse A
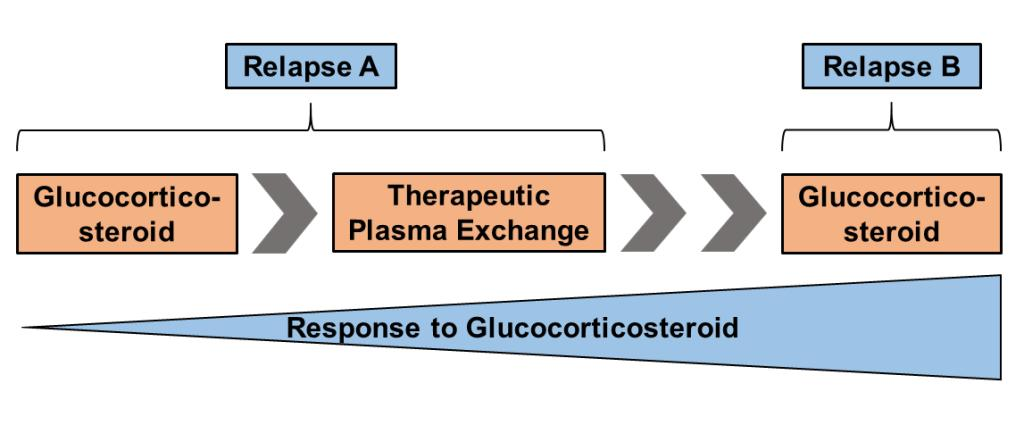
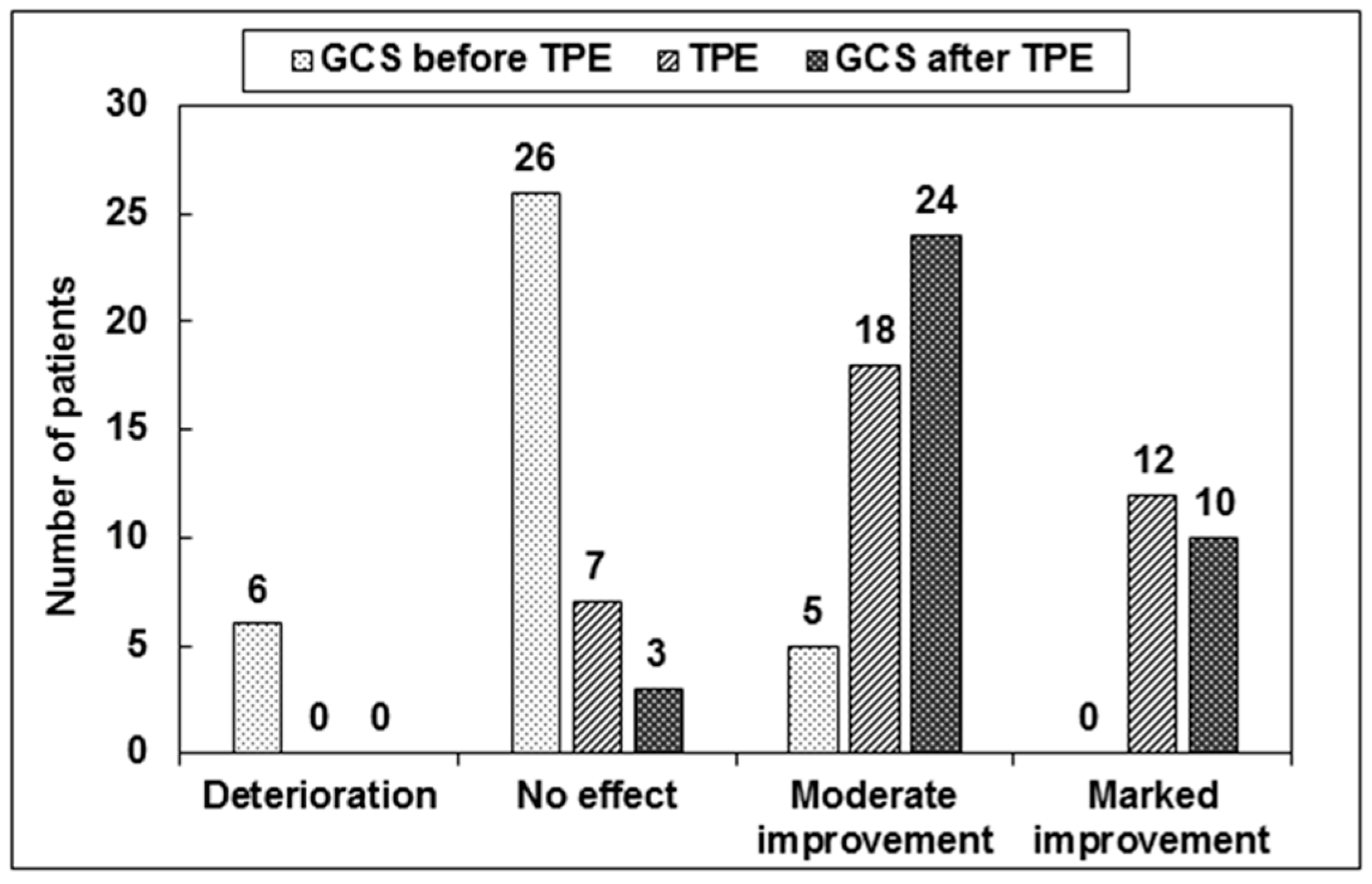
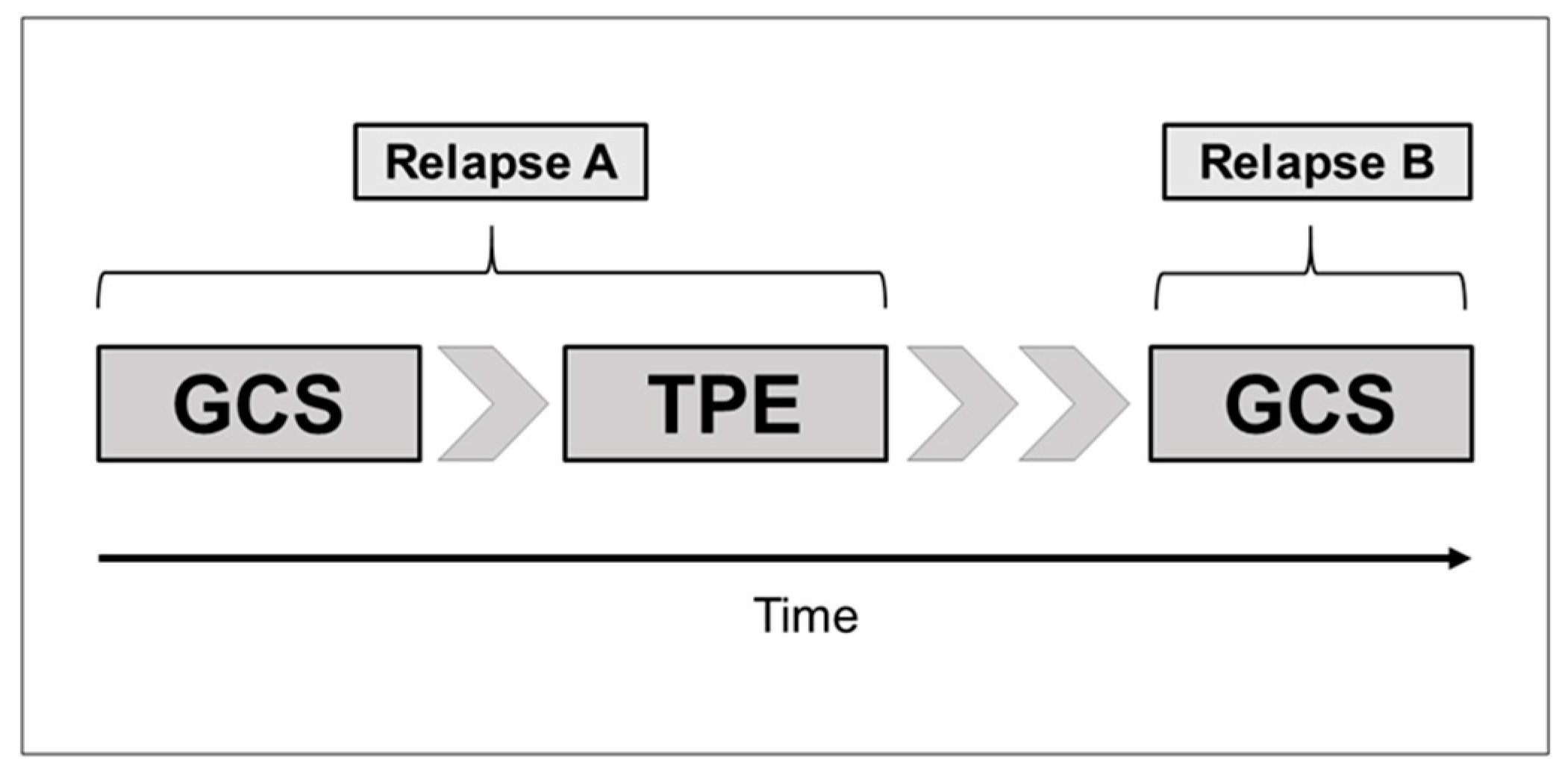
2.2. GCS Treatment for Relapse A
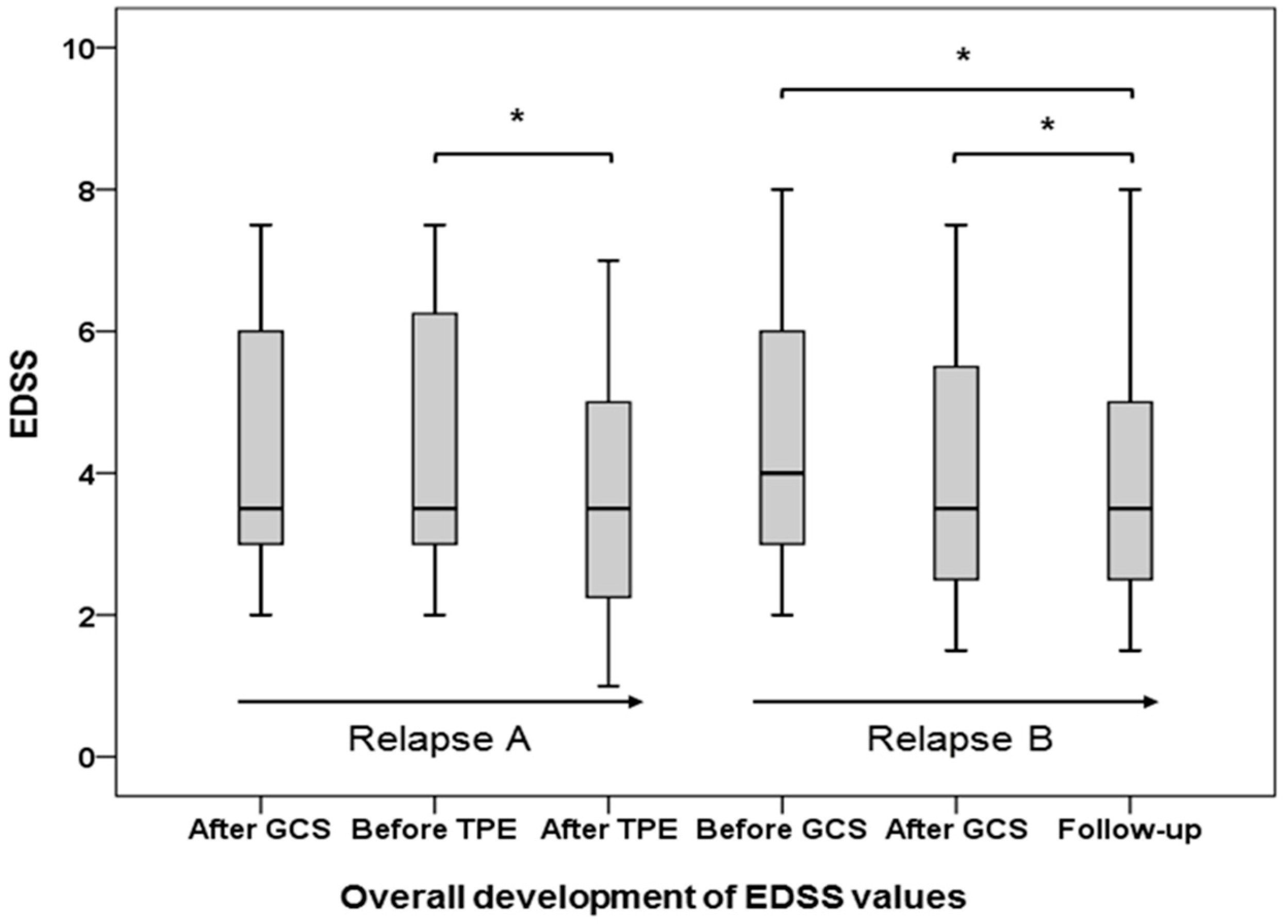
2.3. TPE for Relapse A
2.4. GCS Treatment for Relapse B
2.5. Follow-up Examination after GCS Treatment for Relapse B
3. Discussion
4. Materials and Methods
4.1. Study Participants and Inclusion Criteria
4.2. Outcome Measures
4.2.1. Primary Endpoint of the Response to GCS Treatment and TPE
4.2.2. Secondary Endpoint of the Response to GCS Treatment and TPE
4.3. Administration of GCS
4.4. TPE Procedures
4.5. Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| CIS | Clinically isolated syndrome |
| CNS | Central nervous system |
| CVA | Central venous access |
| DMD | Disease modifying drugs |
| EDSS | Expanded disability status scale |
| GCS | Glucocorticosteroid |
| MP | Methylprednisolone |
| MS | Multiple sclerosis |
| PP-MS | Primary-progressive multiple sclerosis |
| RR-MS | Relapsing-remitting multiple sclerosis |
| SP-MS | Secondary-progressive multiple sclerosis |
| TND | Target neurologic deficit |
| TPE | Therapeutic plasma exchange |
References
- Selmi, C.; Mix, E.; Zettl, U.K. A clear look at the neuroimmunology of multiple sclerosis and beyond. Autoimmun. Rev. 2012, 11, 159–162. [Google Scholar] [CrossRef] [PubMed]
- Weinshenker, B.G. The natural history of multiple sclerosis: Update 1998. Semin. Neurol. 1998, 18, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Hohlfeld, R.; Dornmair, K.; Meinl, E.; Wekerle, H. The search for the target antigens of multiple sclerosis, part 1: Autoreactive CD4+ T lymphocytes as pathogenic effectors and therapeutic targets. Lancet Neurol. 2016, 15, 198–209. [Google Scholar] [CrossRef]
- Hohlfeld, R.; Dornmair, K.; Meinl, E.; Wekerle, H. The search for the target antigens of multiple sclerosis, part 2: CD8+ T cells, B cells, and antibodies in the focus of reverse-translational research. Lancet Neurol. 2016, 15, 317–331. [Google Scholar] [CrossRef]
- Sorensen, P.S. New management algorithms in multiple sclerosis. Curr. Opin. Neurol. 2014, 27, 246–259. [Google Scholar] [CrossRef] [PubMed]
- Jokubaitis, V.G.; Spelman, T.; Kalincik, T.; Lorscheider, J.; Havrdova, E.; Horakova, D.; Duquette, P.; Girard, M.; Prat, A.; Izquierdo, G.; et al. Predictors of long-term disability accrual in relapse-onset multiple sclerosis. Ann. Neurol. 2016, 80, 89–100. [Google Scholar] [CrossRef] [PubMed]
- Bevan, C.; Gelfand, J.M. Therapeutic management of severe relapses in multiple sclerosis. Curr. Treat Options Neurol. 2015, 17, 345. [Google Scholar] [CrossRef] [PubMed]
- Rommer, P.S.; Zettl, U.K.; Kieseier, B.; Hartung, H.P.; Menge, T.; Frohman, E.; Greenberg, B.M.; Hemmer, B.; Stüve, O. Requirement for safety monitoring for approved multiple sclerosis therapies: An overview. Clin. Exp. Immunol. 2014, 175, 397–407. [Google Scholar] [CrossRef] [PubMed]
- Tumani, H. Corticosteroids and plasma exchange in multiple sclerosis. J. Neurol. 2008, 255, 36–42. [Google Scholar] [CrossRef] [PubMed]
- German Society of Neurology. Diagnosis and Therapy of Multiple Sclerosis. Available online: http://www.dgn.org/leitlinien/2333-ll-31-2012-diagnose-und-therapie-der-multiplen-sklerose (accessed on 31 March 2017).
- Berkovich, R.R. Acute multiple sclerosis relapse. Continuum (Minneap. Minn.) 2016, 22, 799–814. [Google Scholar] [CrossRef] [PubMed]
- Ross, A.P.; Ben-Zacharia, A.; Harris, C.; Smrtka, J. Multiple sclerosis, relapses, and the mechanism of action of adrenocorticotropic hormone. Front. Neurol. 2013, 4, 21. [Google Scholar] [CrossRef] [PubMed]
- Leussink, V.I.; Jung, S.; Merschdorf, U.; Toyka, K.V.; Gold, R. High-dose methylprednisolone therapy in multiple sclerosis induces apoptosis in peripheral blood leukocytes. Arch. Neurol. 2001, 58, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Khatri, B.O. Therapeutic apheresis in multiple sclerosis and other central nervous system disorders. Ther. Apher. 2000, 4, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Trebst, C.; Reising, A.; Kielstein, J.T.; Hafer, C.; Stangel, M. Plasma exchange therapy in steroid-unresponsive relapses in patients with multiple sclerosis. Blood Purif. 2009, 28, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Keegan, M.; König, F.; McClelland, R.; Brück, W.; Morales, Y.; Bitsch, A.; Panitch, H.; Lassmann, H.; Weinshenker, B.; Rodriguez, M.; et al. Relation between humoral pathological changes in multiple sclerosis and response to therapeutic plasma exchange. Lancet 2005, 366, 579–582. [Google Scholar] [CrossRef]
- Keegan, M.; Pineda, A.A.; McClelland, R.L.; Darby, C.H.; Rodriguez, M.; Weinshencker, B.G. Plasma exchange for severe attacks of CNS demyelination: Predictors of response. Neurology 2002, 58, 143–146. [Google Scholar] [CrossRef] [PubMed]
- Matzke, B.; Metze, C.; Winkelmann, A.; Grossmann, A.; Hartung, H.P.; Benecke, R.; Zettl, U.K. Severe relapse of multiple sclerosis during plasma exchange treatment. Mult. Scler. 2011, 17, 759–762. [Google Scholar] [CrossRef] [PubMed]
- Muchnik, S.; Jáuregui, W.O.; Mazía, C. Acute and reversible worsening of multiple sclerosis treated with plasmapheresis. A form of uhthoff symptom? Medicina (B Aires) 1985, 45, 207–208. [Google Scholar]
- Wirguin, I.; Shinar, E.; Abramsky, O. Relapse of multiple sclerosis following acute allergic reactions to plasma during plasmapheresis. J. Neurol. 1989, 236, 62–63. [Google Scholar] [CrossRef] [PubMed]
- Ehler, J.; Koball, S.; Sauer, M.; Hickstein, H.; Mitzner, S.; Benecke, R.; Zettl, U.K. Therapeutic plasma exchange in glucocorticosteroid–unresponsive patients with Clinically Isolated Syndrome. Ther. Apher. Dial. 2014, 18, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Lassmann, H.; Brück, W.; Lucchinetti, C.F. The immunopathology of multiple sclerosis: An overview. Brain Pathol. 2007, 17, 210–218. [Google Scholar] [CrossRef] [PubMed]
- Lucchinetti, C.; Brück, W.; Parisi, J.; Scheithauer, B.; Rodriguez, M.; Lassmann, H. Heterogeneity of multiple sclerosis lesions: Implications for the pathogenesis of demyelination. Ann. Neurol. 2000, 47, 707–717. [Google Scholar] [CrossRef]
- Metz, I.; Weigand, S.D.; Popescu, B.F.; Frischer, J.M.; Parisi, J.E.; Guo, Y.; Lassmann, H.; Brück, W.; Lucchinetti, C.F. Pathologic heterogeneity persists in early active multiple sclerosis lesions. Ann. Neurol. 2014, 75, 728–738. [Google Scholar] [CrossRef] [PubMed]
- Barnett, M.H.; Prineas, J.W. Relapsing and remitting multiple sclerosis: pathology of the newly forming lesion. Ann. Neurol. 2004, 55, 458–468. [Google Scholar] [CrossRef] [PubMed]
- Barnett, M.H.; Sutton, I. The pathology of multiple sclerosis: A paradigm shift. Curr. Opin. Neurol. 2006, 19, 242–247. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, A. Complications of apheresis. Semin. Dial. 2012, 25, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Bramlage, C.P.; Schröder, K.; Bramlage, P.; Ahrens, K.; Zapf, A.; Müller, G.A.; Koziolek, M.J. Predictors of complications in therapeutic plasma exchange. J. Clin. Apher. 2009, 24, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, H.C.; Hartung, H.P.; Hetzel, G.R.; Stüve, O.; Kieseier, B.C. Plasma exchange in neuroimmunological disorders: Part 1: Rationale and treatment of inflammatory central nervous system disorders. Arch. Neurol. 2006, 63, 930–935. [Google Scholar] [CrossRef] [PubMed]
- McLeod, B.C. Plasmapheresis in multiple sclerosis. J. Clin. Apher. 2003, 18, 72–74. [Google Scholar] [CrossRef] [PubMed]
- McDonald, W.I.; Compston, A.; Edan, G.; Goodkin, D.; Hartung, H.P.; Lublin, F.D.; McFarland, H.F.; Paty, D.W.; Polman, C.H.; Reingold, S.C.; et al. Recommended diagnostic criteria for multiple sclerosis: Guidelines from the international panel on the diagnosis of multiple sclerosis. Ann. Neurol. 2001, 50, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Ehler, J.; Koball, S.; Sauer, M.; Mitzner, S.; Hickstein, H.; Benecke, R.; Zettl, U.K. Response to therapeutic plasma exchange as a rescue treatment in clinically isolated syndromes and acute worsening of multiple sclerosis: A retrospective analysis of 90 patients. PLoS ONE 2015, 10, e0134583. [Google Scholar] [CrossRef] [PubMed]
- Weinshenker, B.G.; O’Brien, P.C.; Petterson, T.M.; Noseworthy, J.H.; Lucchinetti, C.F.; Dodick, D.W.; Pineda, A.A.; Stevens, L.N.; Rodriguez, M. A randomized trial of plasma exchange in acute central nervous system inflammatory demyelinating disease. Ann. Neurol. 1999, 46, 878–886. [Google Scholar] [CrossRef]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef] [PubMed]
- Sprenger, K.B.; Huber, K.; Kratz, W.; Henze, E. Nomograms for the prediction of patient’s plasma volume in plasma exchange therapy from height, weight, and hematocrit. J. Clin. Apher. 1987, 3, 185–190. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics before Relapse A | CIS | RR-MS | SP-MS | PP-MS | All Patients |
|---|---|---|---|---|---|
| No. of patients | 6 | 24 | 6 | 1 | 37 |
| Age (years) a | 34.5 (20–46) | 31.5 (15–52) | 34.5 (25–69) | 73.0 | 32.0 (15–73) |
| Disease duration (months) a | 1.0 (1–3) | 63.0 (1–273) | 101.0 (65–204) | 291.0 | 65.0 (1–291) |
| Disease-Modifying Drugs (DMD) (%) | 0.0 | 58.3 | 100.0 | 0 | 54.1 |
| Relapses ≤ 12 months a | 1.0 (1) | 2.0 (1–4) | 1.0 (1–3) | 1.0 | 2.0 (1–4) |
| T2-lesions in MRI (%) b | 6 (100) | 21 (100) | 3 (100) | 1 (100) | 31 (100) |
| Gd+ lesions in MRI (%) b | 6 (100) | 12 (57) | 2 (67) | 0 (0) | 20 (65) |
| MS Type at Relapse A | Marked Improvement (n) | Moderate Improvement (n) | No Effect (n) | Deterioration (n) |
|---|---|---|---|---|
| CIS (n = 6) | 0 | 2 | 4 | 0 |
| RR-MS (n = 24) | 0 | 3 | 17 | 4 |
| SP-MS (n = 6) | 0 | 0 | 4 | 2 |
| PP-MS (n = 1) | 0 | 0 | 1 | 0 |
| All patients (n = 37) | 0 | 5 | 26 | 6 |
| MS Type at Relapse A | Marked Improvement (n) | Moderate Improvement (n) | No Effect (n) | Deterioration (n) |
|---|---|---|---|---|
| CIS (n = 6) | 3 | 2 | 1 | 0 |
| RR-MS (n = 24) | 9 | 11 | 4 | 0 |
| SP-MS (n = 6) | 0 | 4 | 2 | 0 |
| PP-MS (n = 1) | 0 | 1 | 0 | 0 |
| All patients (n = 37) | 12 | 18 | 7 | 0 |
| Adverse event | n | Treatment |
|---|---|---|
| Allergic reaction to fresh frozen plasma | 1 | Antihistamines and prednisolone |
| Catheter-associated infection | 1 | Catheter removal and antibiotic treatment |
| Hypocalcaemia | 1 | 10% calcium gluconate |
| Dislocation of peripheral vascular access at end of treatment | 1 | Removal of vascular access |
| Nausea | 2 | No specific treatment needed |
| Coagulation imbalances | 2 | No specific treatment needed |
| Moderate arterial hypotension | 2 | Crystalloid infusion |
| MS Type at Relapse B | Marked Improvement (n) | Moderate Improvement (n) | No Effect (n) | Deterioration (n) |
|---|---|---|---|---|
| RR-MS (n = 29) | 9 | 17 | 3 | 0 |
| SP-MS (n = 7) | 1 | 6 | 0 | 0 |
| PP-MS (n = 1) | 0 | 1 | 0 | 0 |
| All patients (n = 37) | 10 | 24 | 3 | 0 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ehler, J.; Blechinger, S.; Rommer, P.S.; Koball, S.; Mitzner, S.; Hartung, H.-P.; Leutmezer, F.; Sauer, M.; Zettl, U.K. Treatment of the First Acute Relapse Following Therapeutic Plasma Exchange in Formerly Glucocorticosteroid-Unresponsive Multiple Sclerosis Patients—A Multicenter Study to Evaluate Glucocorticosteroid Responsiveness. Int. J. Mol. Sci. 2017, 18, 1749. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms18081749
Ehler J, Blechinger S, Rommer PS, Koball S, Mitzner S, Hartung H-P, Leutmezer F, Sauer M, Zettl UK. Treatment of the First Acute Relapse Following Therapeutic Plasma Exchange in Formerly Glucocorticosteroid-Unresponsive Multiple Sclerosis Patients—A Multicenter Study to Evaluate Glucocorticosteroid Responsiveness. International Journal of Molecular Sciences. 2017; 18(8):1749. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms18081749
Chicago/Turabian StyleEhler, Johannes, Stephan Blechinger, Paulus S. Rommer, Sebastian Koball, Steffen Mitzner, Hans-Peter Hartung, Fritz Leutmezer, Martin Sauer, and Uwe K. Zettl. 2017. "Treatment of the First Acute Relapse Following Therapeutic Plasma Exchange in Formerly Glucocorticosteroid-Unresponsive Multiple Sclerosis Patients—A Multicenter Study to Evaluate Glucocorticosteroid Responsiveness" International Journal of Molecular Sciences 18, no. 8: 1749. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms18081749