The Prognostic Significance of Histone Demethylase UTX in Esophageal Squamous Cell Carcinoma

Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
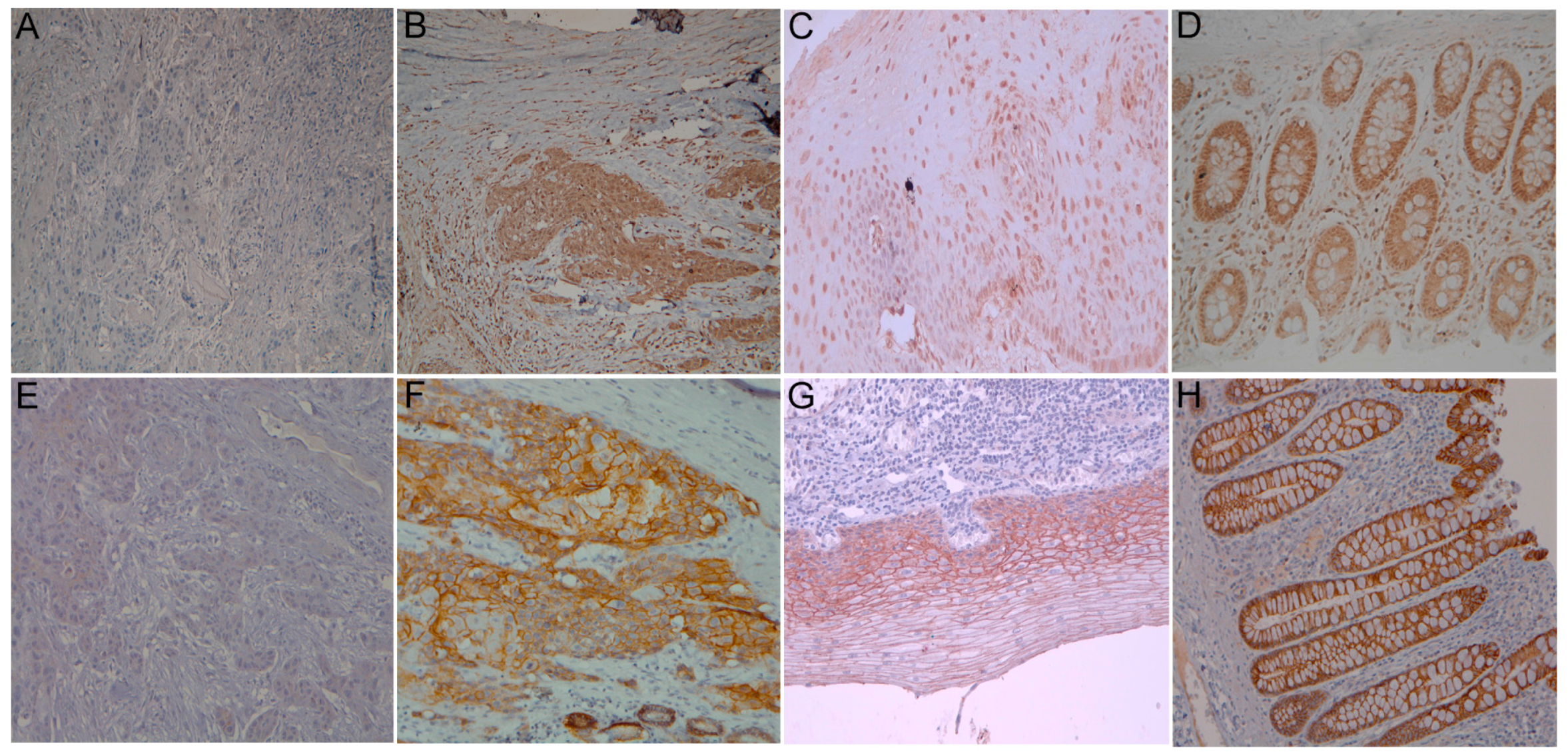
2.2. Correlation between Clinicopathologic Parameters and UTX Expression
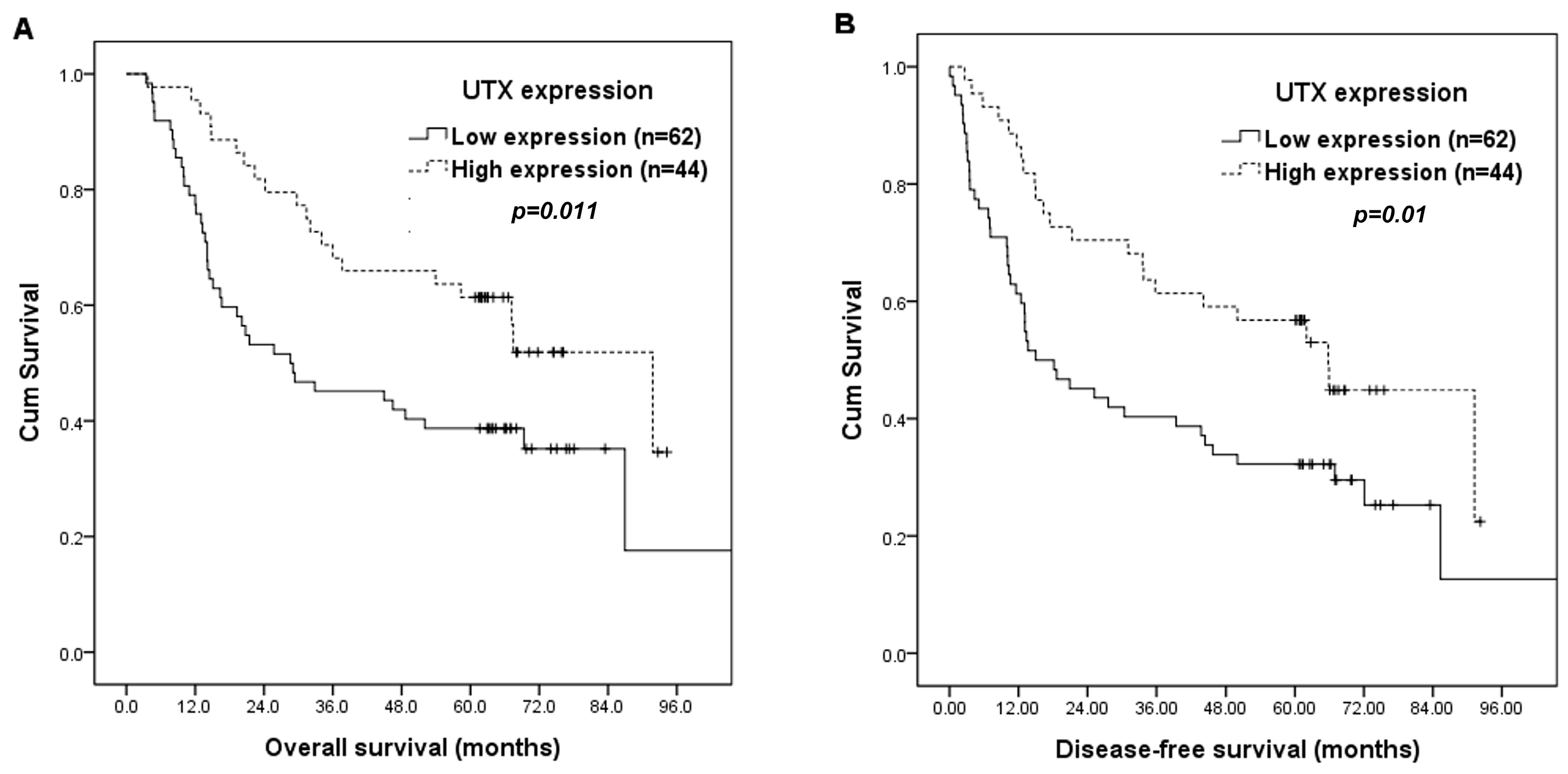
2.3. Survival Analyses
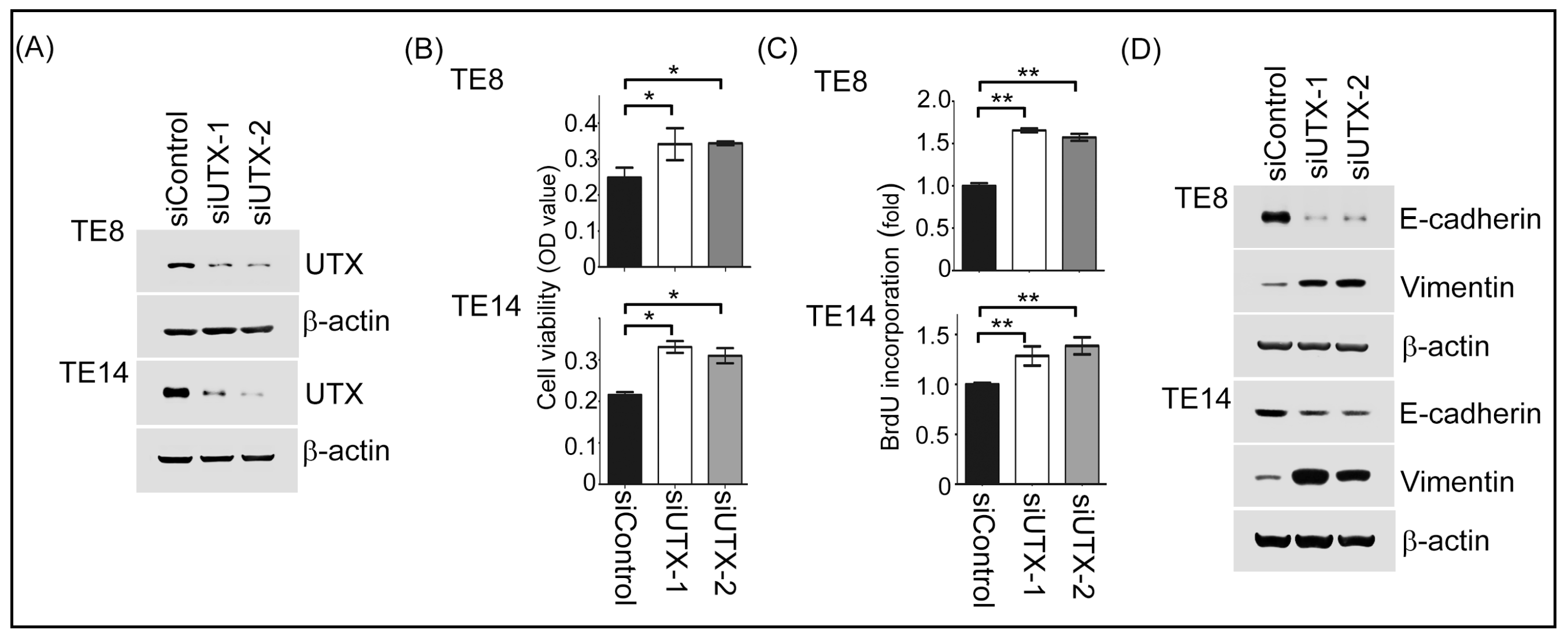
2.4. Inhibition of UTX Promoted ESCC Cells Proliferation and Epithelial-Mesenchymal Transition Process
3. Discussion
4. Materials and Methods
4.1. Patient Population
4.2. Immunohistochemistry
4.3. Cell Lines and siRNA Transfection
4.4. Western Blotting Assay
4.5. MTT and BrdU Assay
4.6. Statistical Analysis
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| UTX | ubiquitouslytranscribed TPR gene on the X chromosome |
| ESCC | Directory of open access journals |
| H3K27me2/3 | lysine 27 of histone H3 |
| TCGA | The Cancer Genome Atlas |
| bHLH | basic helix–loop–helix |
| DFS | Disease-free survival |
References
- Chen, Y.H.; Lu, H.I.; Wang, Y.M.; Lo, C.M.; Chou, S.Y.; Huang, C.H.; Shih, L.H.; Chen, S.W.; Li, S.H. The prognostic significance of celiac lymph node metastasis in patients with locally advanced esophageal squamous cell carcinoma receiving curative concurrent chemoradiotherapy. Oncotarget 2017, 8, 96190–96202. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Xie, X.; Zhou, C.; Peng, S.; Rao, D.; Fu, J. Which factors are associated with actual 5-year survival of oesophageal squamous cell carcinoma? Eur. J. Cardiothorac. Surg. 2012, 41, e7–e11. [Google Scholar] [CrossRef] [PubMed]
- Li, S.H.; Lu, H.I.; Chang, A.Y.; Huang, W.T.; Lin, W.C.; Lee, C.C.; Tien, W.Y.; Lan, Y.C.; Tsai, H.T.; Chen, C.H. Angiotensin II type I receptor (AT1R) is an independent prognosticator of esophageal squamous cell carcinoma and promotes cells proliferation via mTOR activation. Oncotarget 2016, 7, 67150–67165. [Google Scholar] [CrossRef] [PubMed]
- Li, S.H.; Chen, C.H.; Lu, H.I.; Huang, W.T.; Tien, W.Y.; Lan, Y.C.; Lee, C.C.; Chen, Y.H.; Huang, H.Y.; Chang, A.Y.; et al. Phosphorylated p70S6K expression is an independent prognosticator for patients with esophageal squamous cell carcinoma. Surgery 2015, 157, 570–580. [Google Scholar] [CrossRef] [PubMed]
- Estes, N.C.; Stauffer, J.; Romberg, M.; Thomas, J.H.; Jewell, W.R.; Hermreck, A. Squamous cell carcinoma of the esophagus. Am. Surg. 1996, 62, 573–576. [Google Scholar] [PubMed]
- Rada-Iglesias, A.; Wysocka, J. Epigenomics of human embryonic stem cells and induced pluripotent stem cells: Insights into pluripotency and implications for disease. Genome Med. 2011, 3, 36. [Google Scholar] [CrossRef] [PubMed]
- Shpargel, K.B.; Sengoku, T.; Yokoyama, S.; Magnuson, T. UTX and UTY demonstrate histone demethylase-independent function in mouse embryonic development. PLoS Genet. 2012, 8, e1002964. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.; Zhang, H.S.; Liu, Y.; Zhang, Z.G.; Du, G.Y.; Li, H.; Yu, X.Y.; Huang, Y.H. Loss of TET1 facilitates DLD1 colon cancer cell migration via H3K27me3-mediated down-regulation of E-cadherin. J. Cell. Physiol. 2018, 233, 1359–1369. [Google Scholar] [CrossRef] [PubMed]
- Nickerson, M.L.; Dancik, G.M.; Im, K.M.; Edwards, M.G.; Turan, S.; Brown, J.; Ruiz-Rodriguez, C.; Owens, C.; Costello, J.C.; Guo, G.; et al. Concurrent alterations in TERT, KDM6A, and the BRCA pathway in bladder cancer. Clin. Cancer Res. 2014, 20, 4935–4948. [Google Scholar] [CrossRef] [PubMed]
- Suva, M.L.; Riggi, N.; Bernstein, B.E. Epigenetic reprogramming in cancer. Science 2013, 339, 1567–1570. [Google Scholar] [CrossRef] [PubMed]
- Van Haaften, G.; Dalgliesh, G.L.; Davies, H.; Chen, L.; Bignell, G.; Greenman, C.; Edkins, S.; Hardy, C.; O’Meara, S.; Teague, J.; et al. Somatic mutations of the histone H3K27 demethylase gene UTX in human cancer. Nat. Genet. 2009, 41, 521–523. [Google Scholar] [CrossRef] [PubMed]
- Miyake, N.; Mizuno, S.; Okamoto, N.; Ohashi, H.; Shiina, M.; Ogata, K.; Tsurusaki, Y.; Nakashima, M.; Saitsu, H.; Niikawa, N.; et al. KDM6A point mutations cause Kabuki syndrome. Hum. Mutat. 2013, 34, 108–110. [Google Scholar] [CrossRef] [PubMed]
- Banka, S.; Lederer, D.; Benoit, V.; Jenkins, E.; Howard, E.; Bunstone, S.; Kerr, B.; McKee, S.; Lloyd, I.C.; Shears, D.; et al. Novel KDM6A (UTX) mutations and a clinical and molecular review of the X-linked Kabuki syndrome (KS2). Clin. Genet. 2015, 87, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Shpargel, K.B.; Starmer, J.; Wang, C.; Ge, K.; Magnuson, T. UTX-guided neural crest function underlies craniofacial features of Kabuki syndrome. Proc. Natl. Acad. Sci. USA 2017, 114, E9046–E9055. [Google Scholar] [CrossRef] [PubMed]
- Kandoth, C.; McLellan, M.D.; Vandin, F.; Ye, K.; Niu, B.; Lu, C.; Xie, M.; Zhang, Q.; McMichael, J.F.; Wyczalkowski, M.A.; et al. Mutational landscape and significance across 12 major cancer types. Nature 2013, 502, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Ezponda, T.; Dupere-Richer, D.; Will, C.M.; Small, E.C.; Varghese, N.; Patel, T.; Nabet, B.; Popovic, R.; Oyer, J.; Bulic, M.; et al. UTX/KDM6A Loss Enhances the Malignant Phenotype of Multiple Myeloma and Sensitizes Cells to EZH2 inhibition. Cell Rep. 2017, 21, 628–640. [Google Scholar] [CrossRef] [PubMed]
- Benyoucef, A.; Palii, C.G.; Wang, C.; Porter, C.J.; Chu, A.; Dai, F.; Tremblay, V.; Rakopoulos, P.; Singh, K.; Huang, S.; et al. UTX inhibition as selective epigenetic therapy against TAL1-driven T-cell acute lymphoblastic leukemia. Genes Dev. 2016, 30, 508–521. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Sharma, A.; Dhar, S.S.; Lee, S.H.; Gu, B.; Chan, C.H.; Lin, H.K.; Lee, M.G. UTX and MLL4 coordinately regulate transcriptional programs for cell proliferation and invasiveness in breast cancer cells. Cancer Res. 2014, 74, 1705–1717. [Google Scholar] [CrossRef] [PubMed]
- Gameiro, S.F.; Kolendowski, B.; Zhang, A.; Barrett, J.W.; Nichols, A.C.; Torchia, J.; Mymryk, J.S. Human papillomavirus dysregulates the cellular apparatus controlling the methylation status of H3K27 in different human cancers to consistently alter gene expression regardless of tissue of origin. Oncotarget 2017, 8, 72564–72576. [Google Scholar] [CrossRef] [PubMed]
- Van der Meulen, J.; Speleman, F.; Van Vlierberghe, P. The H3K27me3 demethylase UTX in normal development and disease. Epigenetics 2014, 9, 658–668. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.K.; Tsai, M.C.; Poulin, G.; Adler, A.S.; Chen, S.; Liu, H.; Shi, Y.; Chang, H.Y. The histone demethylase UTX enables RB-dependent cell fate control. Genes Dev. 2010, 24, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Curtis, C.; Shah, S.P.; Chin, S.F.; Turashvili, G.; Rueda, O.M.; Dunning, M.J.; Speed, D.; Lynch, A.G.; Samarajiwa, S.; Yuan, Y.; et al. The genomic and transcriptomic architecture of 2000 breast tumours reveals novel subgroups. Nature 2012, 486, 346–352. [Google Scholar] [PubMed]
- Liu, J.; Mercher, T.; Scholl, C.; Brumme, K.; Gilliland, D.G.; Zhu, N. A functional role for the histone demethylase UTX in normal and malignant hematopoietic cells. Exp. Hematol. 2012, 40, 487–498. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.L.; Ling, Z.Q.; Chen, S.Z.; Li, B.; Ji, W.H.; Mao, W.M. The impact of E-cadherin expression on the prognosis of esophageal cancer: A meta-analysis. Dis. Esophagus 2014, 27, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Zha, L.; Cao, Q.; Cui, X.; Li, F.; Liang, H.; Xue, B.; Shi, H. Epigenetic regulation of E-cadherin expression by the histone demethylase UTX in colon cancer cells. Med. Oncol. 2016, 33, 21. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.J.; Park, J.H.; Park, M.; Won, H.Y.; Joo, H.S.; Lee, C.H.; Lee, J.Y.; Kong, G. UTX inhibits EMT-induced breast CSC properties by epigenetic repression of EMT genes in cooperation with LSD1 and HDAC1. EMBO Rep. 2015, 16, 1288–1298. [Google Scholar] [CrossRef] [PubMed]
- Edge, S.B.; Compton, C.C.; Fritz, A.G.; Greene, F.L.; Trotti, A. (Eds.) Esophagus and esophagogastric junction. In AJCC Cancer Satging Manual, 7th ed.; Springer: New York, NY, USA, 2010; pp. 103–111. [Google Scholar]
- Bouvier, C.; Macagno, N.; Nguyen, Q.; Loundou, A.; Jiguet-Jiglaire, C.; Gentet, J.C.; Jouve, J.L.; Rochwerger, A.; Mattei, J.C.; Bouvard, D.; et al. Prognostic value of the Hippo pathway transcriptional coactivators YAP/TAZ and beta1-integrin in conventional osteosarcoma. Oncotarget 2016, 7, 64702–64710. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Age (years) | Parameters | No. of Cases (%) |
|---|---|---|
| median | 55 | |
| mean | 56 | |
| range | 29–80 | |
| Sex | ||
| male | 101 (95%) | |
| female | 5 (5%) | |
| Primary tumor location | ||
| Upper | 19 (18%) | |
| Middle | 36 (34%) | |
| Lower | 51 (48%) | |
| T classification | ||
| T1 | 42 (40%) | |
| T2 | 28 (26%) | |
| T3 | 26 (25%) | |
| T4 | 10 (9%) | |
| N classification | ||
| N0 | 70 (66%) | |
| N1 | 25 (24%) | |
| N2 | 9 (8%) | |
| N3 | 2 (2%) | |
| 7th AJCC Stage | ||
| IA | 5 (5%) | |
| IB | 33 (31%) | |
| IIA | 17 (16%) | |
| IIB | 26 (24%) | |
| IIIA | 11 (10%) | |
| IIIB | 3 (3%) | |
| IIIC | 9 (9%) | |
| IV | 2 (2%) | |
| Histological grading | ||
| Grade 1 | 10 (9%) | |
| Grade 2 | 70 (66%) | |
| Grade 3 | 26 (25%) | |
| Surgical margin | ||
| Negative | 91 (86%) | |
| Positive | 15 (14%) | |
| UTX expression | ||
| Low expression | 62 (58%) | |
| High expression | 44 (42%) | |
| E-cadherin | ||
| Low expression | 50 (47%) | |
| High expression | 56 (53%) |
| Parameters | UTX Expression | E-Cadherin Expression | |||||
|---|---|---|---|---|---|---|---|
| Low | High | p Value | Low | High | p Value | ||
| Age (years) | <55 | 29 | 23 | 0.58 | 25 | 27 | 0.85 |
| ≥55 | 33 | 21 | 25 | 29 | |||
| Primary tumor location | U + M | 30 | 25 | 0.39 | 22 | 33 | 0.13 |
| L | 32 | 19 | 28 | 23 | |||
| T classification | T1 + T2 | 38 | 32 | 0.22 | 26 | 44 | 0.004 * |
| T3 + T4 | 24 | 12 | 24 | 12 | |||
| N classification | N0 | 37 | 33 | 0.10 | 25 | 45 | 0.001 * |
| N1 + 2 + 3 | 25 | 11 | 25 | 11 | |||
| 7th AJCC Stage | I | 20 | 18 | 0.36 | 12 | 26 | 0.016 * |
| II + III + IV | 42 | 26 | 38 | 30 | |||
| Histological grading | Grade 1 + 2 | 44 | 36 | 0.20 | 34 | 46 | 0.091 |
| Grade 3 | 18 | 8 | 16 | 10 | |||
| Surgical margin | Negative | 50 | 41 | 0.068 | 40 | 51 | 0.10 |
| Positive | 12 | 3 | 10 | 5 | |||
| E-cadherin expression | Low | 36 | 14 | 0.008 * | - | - | - |
| High | 26 | 30 | - | - | - | ||
| Factors | No. of Patients | Overall Survival (OS) | Disease-Free Survival (DFS) | ||
|---|---|---|---|---|---|
| 5-year OS (%) | p Value | 5-year DFS (%) | p Value | ||
| Age (years) | |||||
| <55 | 52 | 56% | 0.32 | 52% | 0.17 |
| ≥55 | 54 | 41% | 33% | ||
| Location | |||||
| U + M | 55 | 55% | 0.20 | 46% | 0.42 |
| L | 51 | 41% | 39% | ||
| T classification | |||||
| T1 + 2 | 70 | 56% | 0.013 * | 49% | 0.022 * |
| T3 + 4 | 36 | 33% | 31% | ||
| N classification | |||||
| N0 | 70 | 63% | <0.001 * | 54% | <0.001 * |
| N1 + 2 + 3 | 36 | 19% | 19% | ||
| 7th AJCC stage | |||||
| I | 38 | 63% | 0.008 * | 58% | 0.002 * |
| II + III + IV | 68 | 40% | 34% | ||
| Histological grading | |||||
| Grade 1 + 2 | 80 | 50% | 0.33 | 43% | 0.62 |
| Grade 3 | 26 | 42% | 42% | ||
| Surgical margin | |||||
| Negative | 91 | 52% | 0.015 * | 45% | 0.11 |
| Positive | 15 | 27% | 27% | ||
| UTX expression | |||||
| Low expression | 62 | 39% | 0.011 * | 32% | 0.01 * |
| High expression | 44 | 61% | 57% | ||
| E-cadherin expression | |||||
| Low expression | 50 | 38% | 0.026 * | 28% | 0.005 * |
| High expression | 56 | 57% | 55% | ||
| Low UTX/E-cadherin expression | |||||
| Presence | 36 | 31% | 0.001 * | 22% | <0.001 * |
| Absence | 70 | 57% | 53% | ||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, S.-H.; Lu, H.-I.; Huang, W.-T.; Tien, W.-Y.; Lan, Y.-C.; Lin, W.-C.; Tsai, H.-T.; Chen, C.-H. The Prognostic Significance of Histone Demethylase UTX in Esophageal Squamous Cell Carcinoma. Int. J. Mol. Sci. 2018, 19, 297. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms19010297
Li S-H, Lu H-I, Huang W-T, Tien W-Y, Lan Y-C, Lin W-C, Tsai H-T, Chen C-H. The Prognostic Significance of Histone Demethylase UTX in Esophageal Squamous Cell Carcinoma. International Journal of Molecular Sciences. 2018; 19(1):297. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms19010297
Chicago/Turabian StyleLi, Shau-Hsuan, Hung-I Lu, Wan-Ting Huang, Wan-Yu Tien, Ya-Chun Lan, Wei-Che Lin, Hsin-Ting Tsai, and Chang-Han Chen. 2018. "The Prognostic Significance of Histone Demethylase UTX in Esophageal Squamous Cell Carcinoma" International Journal of Molecular Sciences 19, no. 1: 297. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms19010297