MiR-371a-3p Serum Levels Are Increased in Recurrence of Testicular Germ Cell Tumor Patients

 , ,
, ,
Abstract
:1. Introduction
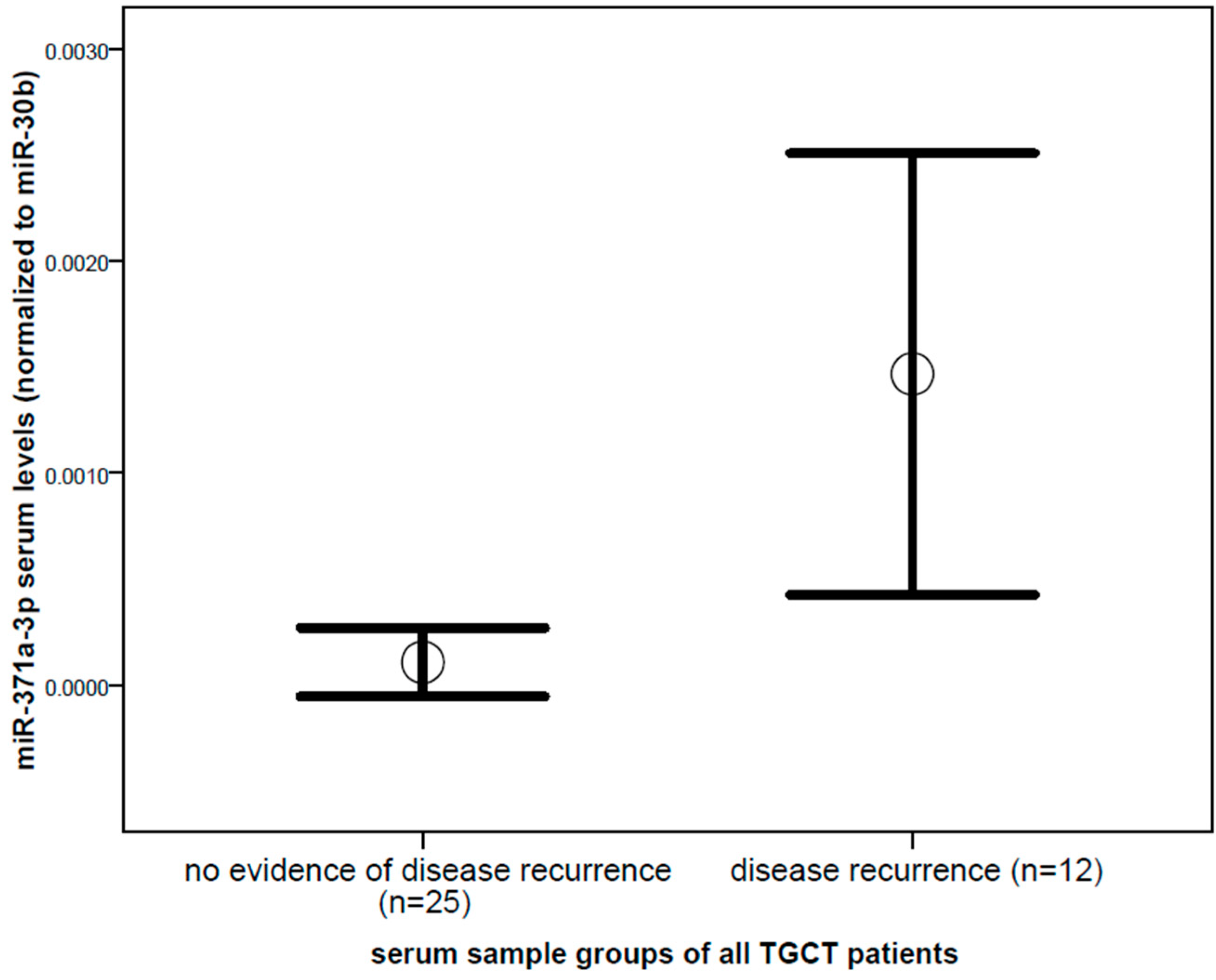
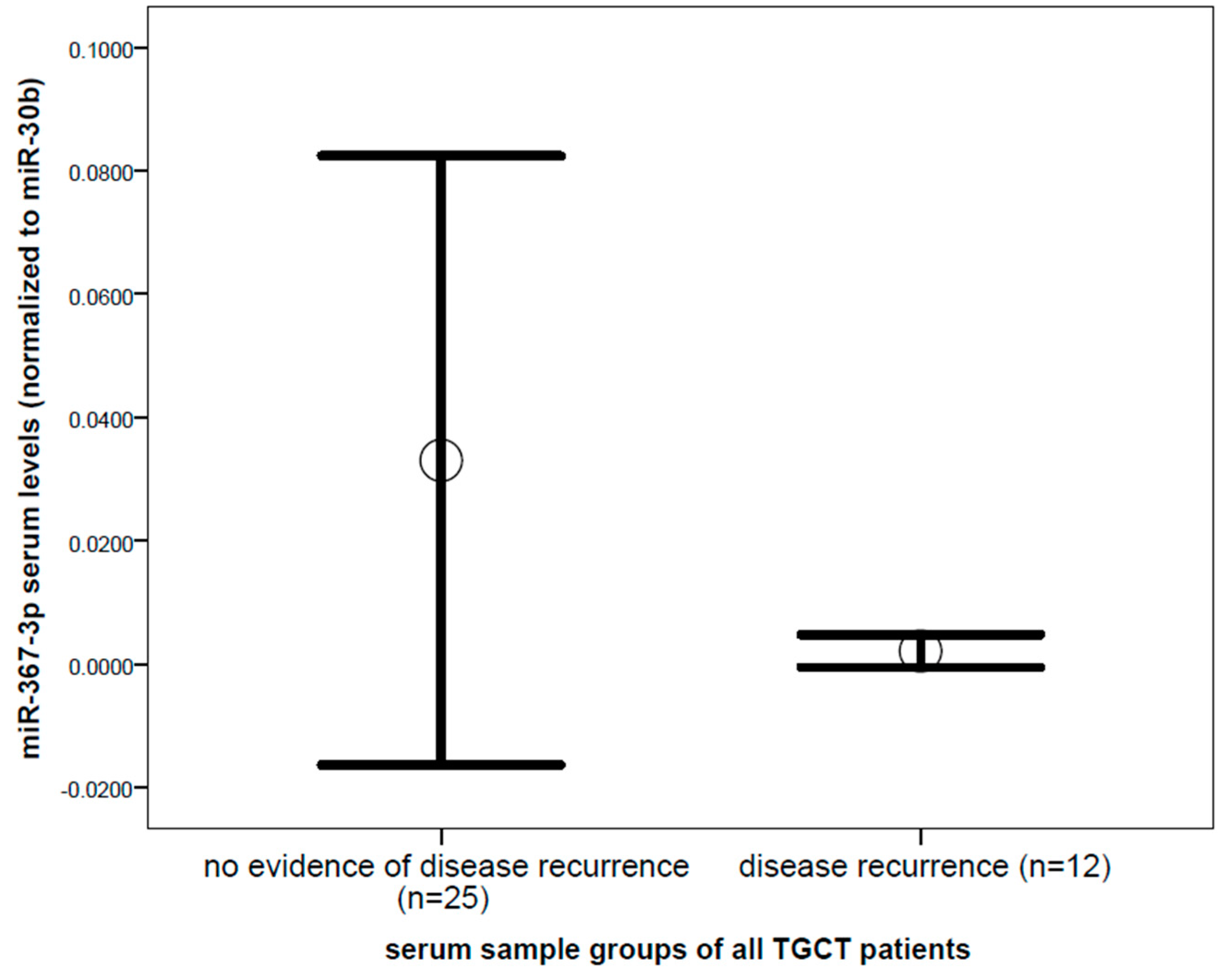
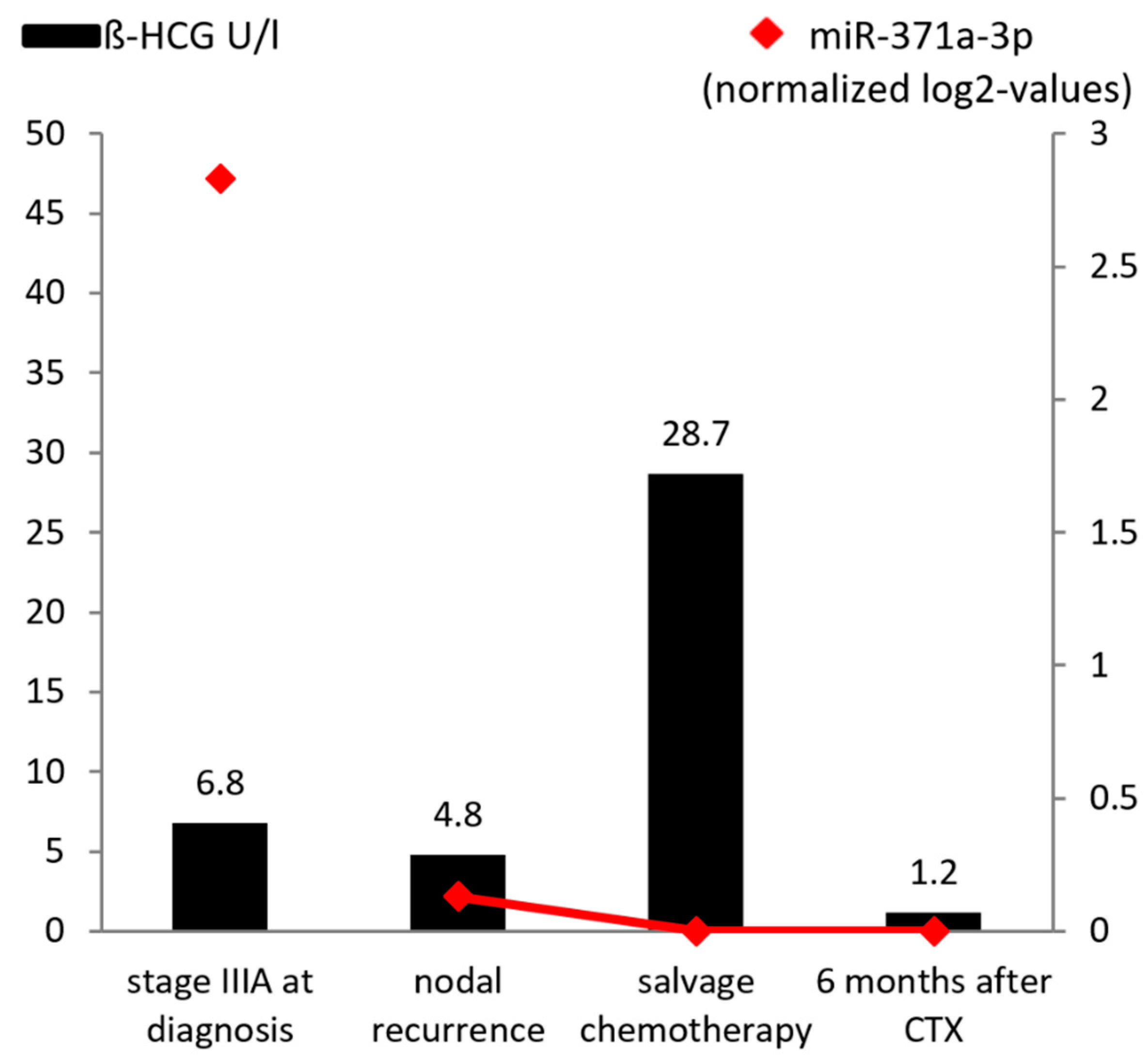
2. Results
3. Discussion
4. Materials and Methods
MiRNA Isolation, cDNA Synthesis, and Quantitative RT PCR (qRT-PCR)
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2018. CA Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef] [PubMed]
- International germ cell consensus classification: A prognostic factor-based staging system for metastatic germ cell cancers. International germ cell cancer collaborative group. J. Clin. Oncol. 1997, 15, 594–603. [CrossRef] [PubMed]
- Albers, P.; Albrecht, W.; Algaba, F.; Bokemeyer, C.; Cohn-Cedermark, G.; Fizazi, K.; Horwich, A.; Laguna, M.P.; Nicolai, N.; Oldenburg, J.; et al. Guidelines on testicular cancer: 2015 update. Eur. Urol. 2015, 68, 1054–1068. [Google Scholar] [CrossRef] [PubMed]
- Dieckmann, K.P.; Spiekermann, M.; Balks, T.; Flor, I.; Loning, T.; Bullerdiek, J.; Belge, G. Micrornas mir-371-3 in serum as diagnostic tools in the management of testicular germ cell tumours. Br. J. cancer 2012, 107, 1754–1760. [Google Scholar] [CrossRef] [PubMed]
- Albers, P.; Albrecht, W.; Algaba, F.; Bokemeyer, C.; Cohn-Cedermark, G.; Fizazi, K.; Horwich, A.; Laguna, M.P. EAU guidelines on testicular cancer: 2011 update. Eur. Urol. 2011, 60, 304–319. [Google Scholar] [CrossRef] [PubMed]
- Smolle, M.A.; Calin, H.N.; Pichler, M.; Calin, G.A. Noncoding rnas and immune checkpoints-clinical implications as cancer therapeutics. FEBS J. 2017, 284, 1952–1966. [Google Scholar] [CrossRef] [PubMed]
- Ling, H.; Vincent, K.; Pichler, M.; Fodde, R.; Berindan-Neagoe, I.; Slack, F.J.; Calin, G.A. Junk DNA and the long non-coding rna twist in cancer genetics. Oncogene 2015, 34, 5003–5011. [Google Scholar] [CrossRef] [PubMed]
- Pichler, M.; Calin, G.A. Micrornas in cancer: From developmental genes in worms to their clinical application in patients. Br. J. Cancer 2015, 113, 569–573. [Google Scholar] [CrossRef] [PubMed]
- Croce, C.M.; Calin, G.A. Mirnas, cancer, and stem cell division. Cell 2005, 122, 6–7. [Google Scholar] [CrossRef] [PubMed]
- Eini, R.; Dorssers, L.C.; Looijenga, L.H. Role of stem cell proteins and micrornas in embryogenesis and germ cell cancer. Int. J. Dev. Biol. 2013, 57, 319–332. [Google Scholar] [CrossRef] [PubMed]
- Stiegelbauer, V.; Vychytilova-Faltejskova, P.; Karbiener, M.; Pehserl, A.M.; Reicher, A.; Resel, M.; Heitzer, E.; Ivan, C.; Bullock, M.; Ling, H.; et al. Mir-196b-5p regulates colorectal cancer cell migration and metastases through interaction with hoxb7 and galnt5. Clin. Cancer Res. 2017, 23, 5255–5266. [Google Scholar] [CrossRef] [PubMed]
- Posch, F.; Leitner, L.; Bergovec, M.; Bezan, A.; Stotz, M.; Gerger, A.; Pichler, M.; Stoger, H.; Liegl-Atzwanger, B.; Leithner, A.; et al. Can multistate modeling of local recurrence, distant metastasis, and death improve the prediction of outcome in patients with soft tissue sarcomas? Clin. Orthop. Relat. Res. 2017, 475, 1427–1435. [Google Scholar] [CrossRef] [PubMed]
- Huppi, K.; Volfovsky, N.; Mackiewicz, M.; Runfola, T.; Jones, T.L.; Martin, S.E.; Stephens, R.; Caplen, N.J. Micrornas and genomic instability. Semin. Cancer Biol. 2007, 17, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Ress, A.L.; Perakis, S.; Pichler, M. Micrornas and colorectal cancer. Adv. Exp. Med. Biol. 2015, 889, 89–103. [Google Scholar] [PubMed]
- Al-Ali, B.M.; Ress, A.L.; Gerger, A.; Pichler, M. Micrornas in renal cell carcinoma: Implications for pathogenesis, diagnosis, prognosis and therapy. Anticancer Res. 2012, 32, 3727–3732. [Google Scholar] [PubMed]
- Mayr, C.; Beyreis, M.; Wagner, A.; Pichler, M.; Neureiter, D.; Kiesslich, T. Deregulated micrornas in biliary tract cancer: Functional targets and potential biomarkers. Biomed. Res. Int. 2016, 2016, 4805270. [Google Scholar] [CrossRef] [PubMed]
- Romero-Cordoba, S.L.; Salido-Guadarrama, I.; Rodriguez-Dorantes, M.; Hidalgo-Miranda, A. Mirna biogenesis: Biological impact in the development of cancer. Cancer Biol. Ther. 2014, 15, 1444–1455. [Google Scholar] [CrossRef] [PubMed]
- Smolle, M.A.; Leithner, A.; Posch, F.; Szkandera, J.; Liegl-Atzwanger, B.; Pichler, M. Micrornas in different histologies of soft tissue sarcoma: A comprehensive review. Int. J. Mol. Sci. 2017, 18, 1960. [Google Scholar] [CrossRef] [PubMed]
- Dieckmann, K.P.; Radtke, A.; Spiekermann, M.; Balks, T.; Matthies, C.; Becker, P.; Ruf, C.; Oing, C.; Oechsle, K.; Bokemeyer, C.; et al. Serum levels of microrna mir-371a-3p: A sensitive and specific new biomarker for germ cell tumours. Eur. Urol. 2017, 71, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Bezan, A.; Gerger, A.; Pichler, M. Micrornas in testicular cancer: Implications for pathogenesis, diagnosis, prognosis and therapy. Anticancer Res. 2014, 34, 2709–2713. [Google Scholar] [PubMed]
- Gillis, A.J.; Rijlaarsdam, M.A.; Eini, R.; Dorssers, L.C.; Biermann, K.; Murray, M.J.; Nicholson, J.C.; Coleman, N.; Dieckmann, K.P.; Belge, G.; et al. Targeted serum mirna (tsmir) test for diagnosis and follow-up of (testicular) germ cell cancer patients: A proof of principle. Mol. Oncol. 2013, 7, 1083–1092. [Google Scholar] [CrossRef] [PubMed]
- Spiekermann, M.; Belge, G.; Winter, N.; Ikogho, R.; Balks, T.; Bullerdiek, J.; Dieckmann, K.P. Microrna mir-371a-3p in serum of patients with germ cell tumours: Evaluations for establishing a serum biomarker. Andrology 2015, 3, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Terbuch, A.; Posch, F.; Partl, R.; Zurl, B.; Bauernhofer, T.; Pichler, M.; Szkandera, J.; Hutterer, G.C.; Pummer, K.; Kapp, K.S.; et al. Risk stratification for febrile neutropenia in patients with testicular germ cell tumors. Cancer Med. 2018, 7, 508–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Agthoven, T.; Eijkenboom, W.M.H.; Looijenga, L.H.J. Microrna-371a-3p as informative biomarker for the follow-up of testicular germ cell cancer patients. Cell. Oncol. 2017, 40, 379–388. [Google Scholar] [CrossRef] [PubMed]
- Murray, M.J.; Halsall, D.J.; Hook, C.E.; Williams, D.M.; Nicholson, J.C.; Coleman, N. Identification of micrornas from the mir-371~373 and mir-302 clusters as potential serum biomarkers of malignant germ cell tumors. Am. J. Clin. Pathol. 2011, 135, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Vilela-Salgueiro, B.; Barros-Silva, D.; Lobo, J.; Costa, A.L.; Guimaraes, R.; Cantante, M.; Lopes, P.; Braga, I.; Oliveira, J.; Henrique, R.; et al. Germ cell tumour subtypes display differential expression of microrna371a-3p. Philos. Trans. R. Soc. Lond. B. Biol. Sci. 2018, 373. [Google Scholar] [CrossRef] [PubMed]
- Syring, I.; Bartels, J.; Holdenrieder, S.; Kristiansen, G.; Muller, S.C.; Ellinger, J. Circulating serum mirna (mir-367-3p, mir-371a-3p, mir-372-3p and mir-373-3p) as biomarkers in patients with testicular germ cell cancer. J. Urol. 2015, 193, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Belge, G.; Dieckmann, K.P.; Spiekermann, M.; Balks, T.; Bullerdiek, J. Serum levels of micrornas mir-371-3: A novel class of serum biomarkers for testicular germ cell tumors? Eur. Urol. 2012, 61, 1068–1069. [Google Scholar] [CrossRef] [PubMed]
- Anheuser, P.; Radtke, A.; Wulfing, C.; Kranz, J.; Belge, G.; Dieckmann, K.P. Serum levels of microrna371a-3p: A highly sensitive tool for diagnosing and staging testicular germ cell tumours: A clinical case series. Urol. Int. 2017, 99, 98–103. [Google Scholar] [CrossRef] [PubMed]
- van Agthoven, T.; Looijenga, L.H.J. Accurate primary germ cell cancer diagnosis using serum based microrna detection (amptsmir test). Oncotarget 2017, 8, 58037–58049. [Google Scholar] [CrossRef] [PubMed]
- Leao, R.; van Agthoven, T.; Figueiredo, A.; Jewett, M.A.S.; Fadaak, K.; Sweet, J.; Ahmad, A.E.; Anson-Cartwright, L.; Chung, P.; Hansen, A.; et al. Serum mirna predicts viable disease after chemotherapy in patients with testicular nonseminoma germ cell tumor. J. Urol. 2018, 200, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Bezan, A.; Posch, F.; Ploner, F.; Bauernhofer, T.; Pichler, M.; Szkandera, J.; Hutterer, G.C.; Pummer, K.; Gary, T.; Samonigg, H.; et al. Risk stratification for venous thromboembolism in patients with testicular germ cell tumors. PLoS ONE 2017, 12, e0176283. [Google Scholar] [CrossRef] [PubMed]
- Terbuch, A.; Posch, F.; Annerer, L.M.; Bauernhofer, T.; Pichler, M.; Szkandera, J.; Hutterer, G.C.; Pummer, K.; Partl, R.; Kapp, K.S.; et al. Long-term cardiovascular complications in stage i seminoma patients. Clin. Transl. Oncol. 2017, 19, 1400–1408. [Google Scholar] [CrossRef] [PubMed]
- Schmoll, H.J.; Souchon, R.; Krege, S.; Albers, P.; Beyer, J.; Kollmannsberger, C.; Fossa, S.D.; Skakkebaek, N.E.; de Wit, R.; Fizazi, K.; et al. European consensus on diagnosis and treatment of germ cell cancer: A report of the european germ cell cancer consensus group (egcccg). Ann. Oncol. 2004, 15, 1377–1399. [Google Scholar] [CrossRef] [PubMed]
- Cathomas, R.; Helbling, D.; Stenner, F.; Rothermundt, C.; Rentsch, C.; Shahin, O.; Seifert, H.H.; Zaugg, K.; Lorch, A.; Mayer, F.; et al. Interdisciplinary evidence-based recommendations for the follow-up of testicular cancer patients: A joint effort. Swiss. Med. Wkly. 2010, 140, 356–369. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Age * | Histol. | Primary Stage | MFS | Site of Relapse | CSO | β-HCG (0–5 U/L) ** | AFP (0–15 ng/mL) ** | LDH (120–240 U/L) ** | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| REC | CTX | FU | REC | CTX | FU | REC | CTX | FU | |||||||
| 1 | 38 | NS | IIIC | 2 | LN retrop | D | <1.2 | <1.2 | <1.2 | 210 | 229 | 14 | 156 | 262 | 175 |
| 2 | 45 | NS | IIIC | 72 | LN med | D | <1.2 | NA | NA | 9.5 | NA | NA | 192 | NA | NA |
| 3 | 70 | S | IIB | 2 | LN retrop | D | <1.2 | <1.2 | <1.2 | 3.4 | 3.3 | 3.6 | 163 | 162 | 163 |
| 4 | 27 | NS | IIIC | 22 | brain | D | NA | NA | 5 | NA | NA | 3.7 | NA | NA | 135 |
| 5 | 39 | S | IIB | 3 | LN retrop | CR | 4.8 | 28.7 | <1.2 | 1.6 | 2.0 | 2.2 | 235 | 243 | 370 |
| 6 | 45 | S | IIA | 11 | LN med | CR | 1.7 | <1.2 | <1.2 | 5.8 | 4.7 | 4.3 | 295 | 196 | 188 |
| 7 | 29 | S | IIB | 5 | lung | D | 2.4 | NA | NA | 2.0 | NA | NA | 199 | NA | NA |
| 8 | 42 | NS | IIIC | 2 | liver | D | <1.2 | NA | NA | 1652.3 | NA | NA | 191 | NA | NA |
| 9 | 30 | NS | IIB | 18 | LN retrop | CR | NA | NA | <1.2 | NA | NA | 4.2 | NA | NA | 189 |
| 10 | 48 | NS | IIA | 1 | markers | CR | <1.2 | <1.2 | <1.2 | 244.6 | 151.1 | 110.7 | 174 | 174 | 153 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Terbuch, A.; Adiprasito, J.B.; Stiegelbauer, V.; Seles, M.; Klec, C.; Pichler, G.P.; Resel, M.; Posch, F.; Lembeck, A.L.; Stöger, H.; et al. MiR-371a-3p Serum Levels Are Increased in Recurrence of Testicular Germ Cell Tumor Patients. Int. J. Mol. Sci. 2018, 19, 3130. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms19103130
Terbuch A, Adiprasito JB, Stiegelbauer V, Seles M, Klec C, Pichler GP, Resel M, Posch F, Lembeck AL, Stöger H, et al. MiR-371a-3p Serum Levels Are Increased in Recurrence of Testicular Germ Cell Tumor Patients. International Journal of Molecular Sciences. 2018; 19(10):3130. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms19103130
Chicago/Turabian StyleTerbuch, Angelika, Jan B. Adiprasito, Verena Stiegelbauer, Maximilian Seles, Christiane Klec, Georg P. Pichler, Margit Resel, Florian Posch, Anna L. Lembeck, Herbert Stöger, and et al. 2018. "MiR-371a-3p Serum Levels Are Increased in Recurrence of Testicular Germ Cell Tumor Patients" International Journal of Molecular Sciences 19, no. 10: 3130. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms19103130