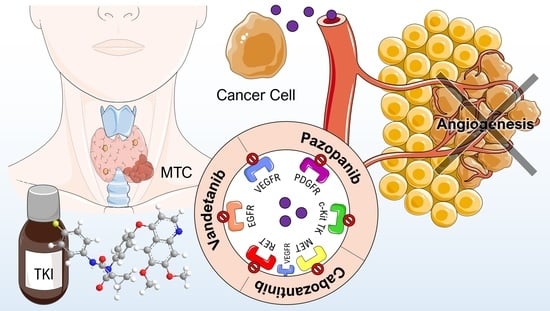
Pazopanib, Cabozantinib, and Vandetanib in the Treatment of Progressive Medullary Thyroid Cancer with a Special Focus on the Adverse Effects on Hypertension


 ,
,
Abstract
:
1. Introduction
2. Thyroid Cancer
3. Tyrosine Kinase Inhibitors
3.1. Adverse Effects
3.2. Efficacy of Cancer Drug Treatment
3.3. Management of Drug-Induced Hypertension
3.4. Ongoing Clinical Trials
4. Discussion
5. Methods
Author Contributions
Acknowledgments
Conflicts of Interest
Abbreviations
| AE(s) | Adverse effect(s) |
| AKT | Protein kinase |
| APWV | Aortic pulse wave velocity |
| ATC | Anaplastic thyroid cancer |
| BAD | BCL2 associated agonist of cell death |
| CAIx | Central aortic augmentation index |
| c-Kit | Stem cell growth factor receptor |
| CV | Cardiovascular |
| CYP3A4 | Cytochrome P4503A4 |
| DBP | Diastolic blood pressure |
| DTC | Differentiated thyroid cancer |
| EGF | Epidermal growth factor |
| ERA | Endothelin receptor antagonist |
| ERK | Extracelluar regulated kinase |
| FC | Follicular cell |
| FGF | Fibroblast growth factor |
| FMTC | Familial medullary thyroid cancer |
| FTC | follicular thyroid cancer |
| GF | Growth factors |
| HGF | Hepatocyte growth factor |
| MAPK | Mitogen activated protein kinase |
| MEK | Methyl ethyl ketone |
| MET | Methionine |
| MDM2 | Mouse double minute 2 |
| MTC | Medullary thyroid cancer |
| mTOR | Mammalian rarget of rapamycin |
| NF-kB | Nuclear factor kappa B |
| OS | Overall survival |
| PDGF | Platelet derived growth factor |
| PDGFR | Platelet derived growth factor receptor |
| PDTC | Poorly differentiated thyroid cancer |
| PFS | Progression free survival |
| PI3K | Phosphoinositide 3 kinases |
| PR | Partial response |
| PTC | Papillary thyroid cancer |
| RAF | Rapidly accelerated fibrosarcoma |
| RAS | Rat sarcoma |
| RECIST | Response Evaluation Criteria in Solid Tumors |
| RET | Rearranged during Transfection |
| RTK | Receptor tyrosine kinase |
| SBP | Systolic blood pressure |
| STAT | Signal transducers and activators of transcription |
| TK | Tyrosine kinase |
| TKI | Tyrosine kinase inhibitor(s) |
| VEGF | Vascular endothelial growth factor |
| VEGFR | Vascular endothelial growth factor receptor |
References
- Griebeler, M.L.; Gharib, H.; Thompson, G.B. Medullary thyroid carcinoma. Endocr. Pract. 2013, 19, 703–711. [Google Scholar] [CrossRef] [PubMed]
- Priya, S.R.; Dravid, C.S.; Digumarti, R.; Dandekar, M. Targeted therapy for medullary thyroid cancer: A review. Front. Oncol. 2017, 7, 238. [Google Scholar] [CrossRef] [PubMed]
- Kandula, P.; Agarwal, R. Proteinuria and hypertension with tyrosine kinase inhibitors. Kidney Int. 2011, 80, 1271–1277. [Google Scholar] [CrossRef] [PubMed]
- Cheah, W.K. Thyroid cancer: Diagnosis and management. Singap. Med. J. 2007, 48, 107–112. [Google Scholar] [PubMed]
- Patel, K.N.; Shaha, A.R. Poorly differentiated and anaplastic thyroid cancer. Cancer Control 2006, 13, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Howlader, N.; Noone, A.M.; Krapcho, M.; Miller, D.; Bishop, K.; Altekruse, S.F.; Kosary, C.L.; Yu, M.; Ruhl, J.; Tatalovich, Z.; et al. Seer Cancer Statistics Review, 1975–2013. National Cancer Institute: Bethesda, MD, USA. Available online: https://seer.Cancer.Gov/csr/1975_2013/ (accessed on 31 August 2018).
- Blomberg, M.; Feldt-Rasmussen, U.; Andersen, K.K.; Kjaer, S.K. Thyroid cancer in Denmark 1943–2008, before and after iodine supplementation. Int. J. Cancer 2012, 131, 2360–2366. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, C.V.; Siqueira, D.R.; Ceolin, L.; Maia, A.L. Advanced medullary thyroid cancer: Pathophysiology and management. Cancer Manag. Res. 2013, 5, 57–66. [Google Scholar] [PubMed]
- Elisei, R.; Cosci, B.; Romei, C.; Bottici, V.; Renzini, G.; Molinaro, E.; Agate, L.; Vivaldi, A.; Faviana, P.; Basolo, F.; et al. Prognostic significance of somatic ret oncogene mutations in sporadic medullary thyroid cancer: A 10-year follow-up study. J. Clin. Endocrinol. Metab. 2008, 93, 682–687. [Google Scholar] [CrossRef] [PubMed]
- Quayle, F.J.; Moley, J.F. Medullary thyroid carcinoma: Management of lymph node metastases. Curr. Treat. Opt. Oncol. 2005, 6, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Modigliani, E.; Cohen, R.; Campos, J.M.; Conte-Devolx, B.; Maes, B.; Boneu, A.; Schlumberger, M.; Bigorgne, J.C.; Dumontier, P.; Leclerc, L.; et al. Prognostic factors for survival and for biochemical cure in medullary thyroid carcinoma: Results in 899 patients. The getc study group. Groupe d’etude des tumeurs a calcitonine. Clin. Endocrinol. 1998, 48, 265–273. [Google Scholar] [CrossRef]
- Roman, S.; Lin, R.; Sosa, J.A. Prognosis of medullary thyroid carcinoma: Demographic, clinical, and pathologic predictors of survival in 1252 cases. Cancer 2006, 107, 2134–2142. [Google Scholar] [CrossRef] [PubMed]
- Massicotte, M.H.; Brassard, M.; Claude-Desroches, M.; Borget, I.; Bonichon, F.; Giraudet, A.L.; Do Cao, C.; Chougnet, C.N.; Leboulleux, S.; Baudin, E.; et al. Tyrosine kinase inhibitor treatments in patients with metastatic thyroid carcinomas: A retrospective study of the tuthyref network. Eur. J. Endocrinol. 2014, 170, 575–582. [Google Scholar] [CrossRef] [PubMed]
- Schlessinger, J. Cell signaling by receptor tyrosine kinases. Cell 2000, 103, 211–225. [Google Scholar] [CrossRef]
- Arora, A.; Scholar, E.M. Role of tyrosine kinase inhibitors in cancer therapy. J. Pharmacol. Exp. Ther. 2005, 315, 971–979. [Google Scholar] [CrossRef] [PubMed]
- Dvorak, H.F. Angiogenesis: Update 2005. J. Thromb. Haemost. 2005, 3, 1835–1842. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, N. Vascular endothelial growth factor: Basic science and clinical progress. Endocr. Rev. 2004, 25, 581–611. [Google Scholar] [CrossRef] [PubMed]
- Kowanetz, M.; Ferrara, N. Vascular endothelial growth factor signaling pathways: Therapeutic perspective. Clin. Cancer Res. 2006, 12, 5018–5022. [Google Scholar] [CrossRef] [PubMed]
- Presta, L.G.; Chen, H.; O’Connor, S.J.; Chisholm, V.; Meng, Y.G.; Krummen, L.; Winkler, M.; Ferrara, N. Humanization of an anti-vascular endothelial growth factor monoclonal antibody for the therapy of solid tumors and other disorders. Cancer Res. 1997, 57, 4593–4599. [Google Scholar] [PubMed]
- Yakes, F.M.; Chen, J.; Tan, J.; Yamaguchi, K.; Shi, Y.; Yu, P.; Qian, F.; Chu, F.; Bentzien, F.; Cancilla, B.; et al. Cabozantinib (xl184), a novel met and vegfr2 inhibitor, simultaneously suppresses metastasis, angiogenesis, and tumor growth. Mol. Cancer Ther. 2011, 10, 2298–2308. [Google Scholar] [CrossRef] [PubMed]
- Kurzrock, R.; Sherman, S.I.; Ball, D.W.; Forastiere, A.A.; Cohen, R.B.; Mehra, R.; Pfister, D.G.; Cohen, E.E.; Janisch, L.; Nauling, F.; et al. Activity of xl184 (cabozantinib), an oral tyrosine kinase inhibitor, in patients with medullary thyroid cancer. J. Clin. Oncol. 2011, 29, 2660–2666. [Google Scholar] [CrossRef] [PubMed]
- Bible, K.C.; Suman, V.J.; Molina, J.R.; Smallridge, R.C.; Maples, W.J.; Menefee, M.E.; Rubin, J.; Karlin, N.; Sideras, K.; Morris, I.I.I.J.C.; et al. A multicenter phase 2 trial of pazopanib in metastatic and progressive medullary thyroid carcinoma: Mc057h. J. Clin. Endocrinol. Metab. 2014, 99, 1687–1693. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Knick, V.B.; Rudolph, S.K.; Johnson, J.H.; Crosby, R.M.; Crouthamel, M.C.; Hopper, T.M.; Miller, C.G.; Harrington, L.E.; Onori, J.A.; et al. Pharmacokinetic-pharmacodynamic correlation from mouse to human with pazopanib, a multikinase angiogenesis inhibitor with potent antitumor and antiangiogenic activity. Mol. Cancer Ther. 2007, 6, 2012–2021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karras, S.; Pontikides, N.; Krassas, G.E. Pharmacokinetic evaluation of cabozantinib for the treatment of thyroid cancer. Expert Opin. Drug Metab. Toxicol. 2013, 9, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Verheijen, R.B.; Beijnen, J.H.; Schellens, J.H.M.; Huitema, A.D.R.; Steeghs, N. Clinical Pharmacokinetics and Pharmacodynamics of Pazopanib: Towards Optimized Dosing. Clin. Pharmacokinet. 2017, 56, 987–997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carlomagno, F.; Vitagliano, D.; Guida, T.; Ciardiello, F.; Tortora, G.; Vecchio, G.; Ryan, A.J.; Fontanini, G.; Fusco, A.; Santoro, M. Zd6474, an orally available inhibitor of kdr tyrosine kinase activity, efficiently blocks oncogenic ret kinases. Cancer Res. 2002, 62, 7284–7290. [Google Scholar] [PubMed]
- Wedge, S.R.; Ogilvie, D.J.; Dukes, M.; Kendrew, J.; Chester, R.; Jackson, J.A.; Boffey, S.J.; Valentine, P.J.; Curwen, J.O.; Musgrove, H.L.; et al. Zd6474 inhibits vascular endothelial growth factor signaling, angiogenesis, and tumor growth following oral administration. Cancer Res. 2002, 62, 4645–4655. [Google Scholar] [PubMed]
- Wells, S.A., Jr.; Gosnell, J.E.; Gagel, R.F.; Moley, J.; Pfister, D.; Sosa, J.A.; Skinner, M.; Krebs, A.; Vasselli, J.; Schlumberger, M. Vandetanib for the treatment of patients with locally advanced or metastatic hereditary medullary thyroid cancer. J. Clin. Oncol. 2010, 28, 767–772. [Google Scholar] [CrossRef] [PubMed]
- Robinson, B.G.; Paz-Ares, L.; Krebs, A.; Vasselli, J.; Haddad, R. Vandetanib (100 mg) in patients with locally advanced or metastatic hereditary medullary thyroid cancer. J. Clin. Endocrinol. Metab. 2010, 95, 2664–2671. [Google Scholar] [CrossRef] [PubMed]
- Wells, S.A., Jr.; Robinson, B.G.; Gagel, R.F.; Dralle, H.; Fagin, J.A.; Santoro, M.; Baudin, E.; Elisei, R.; Jarzab, B.; Vasselli, J.R.; et al. Vandetanib in patients with locally advanced or metastatic medullary thyroid cancer: A randomized, double-blind phase iii trial. J. Clin. Oncol. 2012, 30, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Fox, E.; Widemann, B.C.; Chuk, M.K.; Marcus, L.; Aikin, A.; Whitcomb, P.O.; Merino, M.J.; Lodish, M.; Dombi, E.; Steinberg, S.M.; et al. Vandetanib in children and adolescents with multiple endocrine neoplasia type 2b associated medullary thyroid carcinoma. Clin. Cancer Res. 2013, 19, 4239–4248. [Google Scholar] [CrossRef] [PubMed]
- Frampton, J.E. Vandetanib: In medullary thyroid cancer. Drugs 2012, 72, 1423–1436. [Google Scholar] [CrossRef] [PubMed]
- Resteghini, C.; Cavalieri, S.; Galbiati, D.; Granata, R.; Alfieri, S.; Bergamini, C.; Bossi, P.; Licitra, L.; Locati, L.D. Management of tyrosine kinase inhibitors (tki) side effects in differentiated and medullary thyroid cancer patients. Best Pract. Res. Clin. Endocrinol. Metab. 2017, 31, 349–361. [Google Scholar] [CrossRef] [PubMed]
- Elisei, R.; Schlumberger, M.J.; Müller, S.P.; Schöffski, P.; Brose, M.S.; Shah, M.H.; Licitra, L.; Jarzab, B.; Medvedev, V.; Kreissl, M.C.; et al. Cabozantinib in progressive medullary thyroid cancer. J. Clin. Oncol. 2013, 31, 3639–3646. [Google Scholar] [CrossRef] [PubMed]
- Cabanillas, M.E.; Hu, M.I.; Durand, J.B.; Busaidy, N.L. Challenges associated with tyrosine kinase inhibitor therapy for metastatic thyroid cancer. J. Thyroid Res. 2011, 2011, 985780. [Google Scholar] [CrossRef] [PubMed]
- Hoy, S.M. Cabozantinib: A review of its use in patients with medullary thyroid cancer. Drugs 2014, 74, 1435–1444. [Google Scholar] [CrossRef] [PubMed]
- Facemire, C.S.; Nixon, A.B.; Griffiths, R.; Hurwitz, H.; Coffman, T.M. Vascular endothelial growth factor receptor 2 controls blood pressure by regulating nitric oxide synthase expression. Hypertension 2009, 54, 652–658. [Google Scholar] [CrossRef] [PubMed]
- Horowitz, J.R.; Rivard, A.; van der Zee, R.; Hariawala, M.; Sheriff, D.D.; Esakof, D.D.; Chaudhry, G.M.; Symes, J.F.; Isner, J.M. Vascular endothelial growth factor/vascular permeability factor produces nitric oxide-dependent hypotension. Evidence for a maintenance role in quiescent adult endothelium. Arterioscler. Thromb. Vasc. Biol. 1997, 17, 2793–2800. [Google Scholar] [CrossRef] [PubMed]
- Steeghs, N.; Gelderblom, H.; Roodt, J.O.; Christensen, O.; Rajagopalan, P.; Hovens, M.; Putter, H.; Rabelink, T.J.; de Koning, E. Hypertension and rarefaction during treatment with telatinib, a small molecule angiogenesis inhibitor. Clin. Cancer Res. 2008, 14, 3470–3476. [Google Scholar] [CrossRef] [PubMed]
- Matsuura, A.; Yamochi, W.; Hirata, K.; Kawashima, S.; Yokoyama, M. Stimulatory interaction between vascular endothelial growth factor and endothelin-1 on each gene expression. Hypertension 1998, 32, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Veronese, M.L.; Mosenkis, A.; Flaherty, K.T.; Gallagher, M.; Stevenson, J.P.; Townsend, R.R.; O’Dwyer, P.J. Mechanisms of hypertension associated with bay 43-9006. J. Clin. Oncol. 2006, 24, 1363–1369. [Google Scholar] [CrossRef] [PubMed]
- Schlumberger, M.; Elisei, R.; Müller, S.; Schöffski, P.; Brose, M.; Shah, M.; Licitra, L.; Krajewska, J.; Kreissl, M.C.; Niederle, B.; et al. Overall survival analysis of exam, a phase iii trial of cabozantinib in patients with radiographically progressive medullary thyroid carcinoma. Ann. Oncol. 2017, 28, 2813–2819. [Google Scholar] [CrossRef] [PubMed]
- Rapsomaniki, E.; Timmis, A.; George, J.; Pujades-Rodriguez, M.; Shah, A.D.; Denaxas, S.; White, I.R.; Caulfield, M.J.; Deanfield, J.E.; Smeeth, L.; et al. Blood pressure and incidence of twelve cardiovascular diseases: Lifetime risks, healthy life-years lost, and age-specific associations in 1·25 million people. Lancet 2014, 383, 1899–1911. [Google Scholar] [CrossRef]
- Nguyen, L.; Holland, J.; Miles, D.; Engel, C.; Benrimoh, N.; O’Reilly, T.; Lacy, S. Pharmacokinetic (pk) drug interaction studies of cabozantinib: Effect of cyp3a inducer rifampin and inhibitor ketoconazole on cabozantinib plasma pk and effect of cabozantinib on cyp2c8 probe substrate rosiglitazone plasma pk. J. Clin. Pharmacol. 2015, 55, 1012–1023. [Google Scholar] [CrossRef] [PubMed]
- Tan, A.R.; Gibbon, D.G.; Stein, M.N.; Lindquist, D.; Edenfield, J.W.; Martin, J.C.; Gregory, C.; Suttle, A.B.; Tada, H.; Botbyl, J.; et al. Effects of ketoconazole and esomeprazole on the pharmacokinetics of pazopanib in patients with solid tumors. Cancer Chemother. Pharmacol. 2013, 71, 1635–1643. [Google Scholar] [CrossRef] [PubMed]
- Kruzliak, P.; Kovacova, G.; Pechanova, O. Therapeutic potential of nitric oxide donors in the prevention and treatment of angiogenesis-inhibitor-induced hypertension. Angiogenesis 2013, 16, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Dirix, L.Y.; Maes, H.; Sweldens, C. Treatment of arterial hypertension (aht) associated with angiogenesis inhibitors. Ann. Oncol. 2007, 18, 1121–1122. [Google Scholar] [CrossRef] [PubMed]
- Kružliak, P.; Novák, J.; Novák, M. Vascular endothelial growth factor inhibitor–induced hypertension: From pathophysiology to prevention and treatment based on long-acting nitric oxide donors. Am. J. Hypertens. 2014, 27, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Miyagawa, K.; Emoto, N. Current state of endothelin receptor antagonism in hypertension and pulmonary hypertension. Ther. Adv. Cardiovasc. Dis. 2014, 8, 202–216. [Google Scholar] [CrossRef] [PubMed]
- Laffin, L.J.; Bakris, G.L. Endothelin antagonism and hypertension: An evolving target. Semin. Nephrol. 2015, 35, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Zamorano, J.L.; Lancellotti, P.; Rodriguez Muñoz, D.; Aboyans, V.; Asteggiano, R.; Galderisi, M.; Habib, G.; Lenihan, D.J.; Lip, G.Y.H.; Lyon, A.R.; et al. 2016 esc position paper on cancer treatments and cardiovascular toxicity developed under the auspices of the esc committee for practice guidelines the task force for cancer treatments and cardiovascular toxicity of the european society of cardiology (esc). Eur. Heart J. 2016, 37, 2768–2801. [Google Scholar] [CrossRef] [PubMed]
- ClinicalTrials.gov Is a Database of Privately and Publicly Funded Clinical Studies Conducted around the World. Available online: http://www.clinicaltrials.gov (accessed on 31 August 2018).
- Bible, K.C.; Suman, V.J.; Molina, J.R.; Smallridge, R.C.; Maples, W.J.; Menefee, M.E.; Rubin, J.; Sideras, K.; Morris, J.C., 3rd; McIver, B.; et al. Efficacy of pazopanib in progressive, radioiodine-refractory, metastatic differentiated thyroid cancers: Results of a phase 2 consortium study. Lancet Oncol. 2010, 11, 962–972. [Google Scholar] [CrossRef]
- Hamnvik, O.P.; Choueiri, T.K.; Turchin, A.; McKay, R.R.; Goyal, L.; Davis, M.; Kaymakcalan, M.D.; Williams, J.S. Clinical risk factors for the development of hypertension in patients treated with inhibitors of the vegf signaling pathway. Cancer 2015, 121, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Maitland, M.L.; Bakris, G.L.; Black, H.R.; Chen, H.X.; Durand, J.B.; Elliott, W.J.; Ivy, S.P.; Leier, C.V.; Lindenfeld, J.; Liu, G.; et al. Initial assessment, surveillance, and management of blood pressure in patients receiving vascular endothelial growth factor signaling pathway inhibitors. J. Natl. Cancer Inst. 2010, 102, 596–604. [Google Scholar] [CrossRef] [PubMed]
- Sherman, S.I.; Clary, Clary, D.O.; Elisei, R.; Schlumberger, M.J.; Cohen, E.E.; Schöffski, P.; Wirth, L.J.; Mangeshkar, M.; Aftab, D.T.; Brose, M.S. Correlative analyses of RET and RAS mutations in a phase 3 trial of cabozantinib in patients with progressive, metastatic medullary thyroid cancer. Cancer 2016, 122, 3856–3864. [Google Scholar] [PubMed]
- Spring, B.Q.; Bryan Sears, R.; Zheng, L.Z.; Mai, Z.; Watanabe, R.; Sherwood, M.E.; Schoenfeld, D.A.; Pogue, B.W.; Pereira, S.P.; Villa, E.; et al. A photoactivable multi-inhibitor nanoliposome for tumour control and simultaneous inhibition of treatment escape pathways. Nat. Nanotechnol. 2016, 11, 378–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tailor, T.D.; Hanna, G.; Yarmolenko, P.S.; Dreher, M.R.; Betof, A.S.; Nixon, A.B.; Spasojevic, I.; Dewhirst, M.W. Effect of pazopanib on tumor microenvironment and liposome delivery. Mol. Cancer Ther. 2010, 9, 1798–1808. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| VEGFR | VEGF |
|---|---|
| VEGFR-1 | VEGF-A, VEGF-B and placental growth factors (PGF) |
| VEGFR-2 | VEGF-A and proteolytically cleaved forms of VEGF-C and VEGF-D |
| VEGFR-3 | VEGF-C and VEGF-D |
| Drug | Most Common Adverse Events (Any Grade) | Dose Reductions | Discontinuations Due to Aes |
|---|---|---|---|
| Cabozantinib [34] | Diarrhea (63%; 135/214) Hand-foot syndrome (50%; 107/214) Nausea (43%; 92/214) Fatigue (41%; 87/214) Hypertension (33%; 70/214) | 79%; 169/214 | 16%; 35/214 |
| Pazopanib [22] | Diarrhea (77%; 27/35) Fatigue (63%; 22/35) Hypertension (52%; 18/35) Nausea (52%; 18/35) Anorexia (46%; 16/35) | 40%; 14/35 | 8.6%; 3/35 |
| Vandetanib [28] | Diarrhea (56%; 130/231) Rash (45%; 104/231) Nausea (33%; 77/231) Hypertension (32%; 73/231) Headache (25%; 59/231) | 35%; 81/231 | 12%; 28/231 |
| Drug | Title | Design | Objective | Status | Results |
|---|---|---|---|---|---|
| Pazopanib | A Phase II Study of GW 786034 (Pazopanib) in Advanced Thyroid Cancer NCT00625846 | Interventional Open label | To establish safety and efficacy of pazopanib in Differentiated thyroid cancer (DTC), Medullary thyroid cancer (MTC), and Anaplastic thyroid cancer (ATC), how the drug impacts VEGF plasma levels and the changes is thyroglobulin and its relationship with tumor response. | Active, Not recruiting | The study found positive partial response rates in DTC, but has no overall survival (OS) measure. Adverse effects (AEs) occurred in 43% but generally mild. It showed to be a positive treatment option [53]. |
| Cabozantinib | A Randomized, Double-blind Study To Evaluate the Efficacy and Safety of Cabozantinib (XL184) at 60 mg/Day Compared to a 140 mg/Day in Progressive, Metastatic Medullary Thyroid Cancer Patients NCT01896479 | Interventional Double-blind Randomized | To study the efficacy and safety of cabozantinib when comparing to different doses: 60 mg and 140 mg with placebo. Efficacy measures are progression free survival and overall response rate. Safety measures is a comparison between fewer adverse effects and the efficacy measures. | Recruiting | − |
| An Open-Label, Expanded Access Study of Cabozantinib (XL184) in Subjects With Unresectable, Locally Advanced, or Metastatic Medullary Thyroid Cancer NCT01683110 | Expanded access Open Label | Provide access to cabozantinib | Approved for marketing | − | |
| An International, Randomized, Double-Blinded, Phase 3 Efficacy Study of XL184 Versus Placebo in Subjects With Unresectable, Locally Advanced, or Metastatic Medullary Thyroid Cancer NCT00704730 | Interventional Double-blind Randomized | This study is comparing efficacy measures such as progression-free survival, overall survival and objective response rate between patients receiving cabozantinib and placebo. | Unknown, has results | The study found a statistically significant increase in Progression free survival (PFS) using cabozantinib compared to placebo, an objective response rate of 28% (higher for RET M918T positive subgroup) and an improved OS, although not significantly better than placebo [42,43]. | |
| A Phase 1 Dose-Escalation Study of the Safety and Pharmacokinetics of XL184 Administered Orally to Subjects With Advanced Malignancies NCT00215605 | Interventional Open label | This study is evaluating the safety, tolerability, maximum tolerated dose and dose-limiting toxicity of cabozantinib. It also evaluates plasma pharmacokinetics and renal elimination. Measurements include progression-free survival and tumor response. | Completed | 49% of patients with MTC showed tumor shrinkage and 68% of these showed stable disease for over 6 months. Of all patients included, 90% experienced AEs, but 43% were of grade 1 or 2. The drug was considered to have a satisfactory safety profile [34] | |
| A Phase 1 Study of XL184 (Cabozantinib) in Children and Adolescents With Recurrent or Refractory Solid Tumors, Including CNS Tumors NCT01709435 | Interventional Open label | It is evaluating maximum tolerated dose and recommended phase II dose of cabozantinib in children with solid tumors incl. childhood thyroid gland medullary carcinomas. They also describe toxicities, pharmacokinetics and evaluate overall survival. | Active, Not recruiting | − | |
| Phase 2 Trial of XL184 (Cabozantinib) an Oral Small-Molecule Inhibitor of Multiple Kinases, in Children and Young Adults With Refractory Sarcomas, Wilms Tumor, and Other Rare Tumors NCT02867592 | Interventional, Open label | Determine the objective response rate, toxicities, and pharmacokinetics of cabozantinib in children and young adults with rare tumors. | Recruiting | ||
| Vandetanib | European, Observational, Prospective Study to Evaluate the Benefit/Risk of Vandetanib in RET Mutation Negative and Positive Patients With Symptomatic, Aggressive, Sporadic, Unresectable, Locally Advanced/Metastatic Medullary Thyroid Cancer NCT01945762 | Observational | Assessment of the risk/benefit of 300 mg/d vandetanibin RET positive and RET negative patients with MTC. | Recruiting | |
| Phase I/II Trial of Vandetanib (ZD6474, ZACTIMA) in Children and Adolescents With Hereditary Medullary Thyroid Carcinoma NCT00514046 | Interventional | Investigation of activity of vandetanib in children and adolescents with MTC caused by multiple endocrine neoplasia genetic disorder. Assessment of safety, tolerability, and survival in the study group. | Active, not recruiting | ||
| A Randomized, Int., Open-Label Phase III Study to Assess the Effect of a Patient Outreach Program on the Percentage of Time Patients With Locally Advanced or Metastatic MTC Experience Grade 2 or Higher AEs in the First 12 Months of Treatment With Vandetanib NCT01298323 | Randomized, Open label | Determine if contacting patients with MTC more frequently results in earlier detection and treatment of signs and symptoms of AEs during the first 12 months on vandetanib treatment. | Active, not recruiting | ||
| An International, Randomised, Double-Blind, Two-Arm Study To Evaluate The Safety And Efficacy Of Vandetanib 150 And 300mg/Day In Patients With Unresectable Locally Advanced Or Metastatic Medullary Thyroid Carcinoma With Progressive Or Symptomatic Disease NCT01496313 | Interventional, Randomized, Double-blind | Comparison of safety and efficacy of 150 and 300 mg/d vandetanib in patients with MTC. | Active, not recruiting |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Milling, R.V.; Grimm, D.; Krüger, M.; Grosse, J.; Kopp, S.; Bauer, J.; Infanger, M.; Wehland, M. Pazopanib, Cabozantinib, and Vandetanib in the Treatment of Progressive Medullary Thyroid Cancer with a Special Focus on the Adverse Effects on Hypertension. Int. J. Mol. Sci. 2018, 19, 3258. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms19103258
Milling RV, Grimm D, Krüger M, Grosse J, Kopp S, Bauer J, Infanger M, Wehland M. Pazopanib, Cabozantinib, and Vandetanib in the Treatment of Progressive Medullary Thyroid Cancer with a Special Focus on the Adverse Effects on Hypertension. International Journal of Molecular Sciences. 2018; 19(10):3258. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms19103258
Chicago/Turabian StyleMilling, Rikke Vilsbøll, Daniela Grimm, Marcus Krüger, Jirka Grosse, Sascha Kopp, Johann Bauer, Manfred Infanger, and Markus Wehland. 2018. "Pazopanib, Cabozantinib, and Vandetanib in the Treatment of Progressive Medullary Thyroid Cancer with a Special Focus on the Adverse Effects on Hypertension" International Journal of Molecular Sciences 19, no. 10: 3258. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms19103258