Hyaluronic Acid/Bone Substitute Complex Implanted on Chick Embryo Chorioallantoic Membrane Induces Osteoblastic Differentiation and Angiogenesis, but not Inflammation

 ,
,
Abstract
:1. Introduction
2. Results
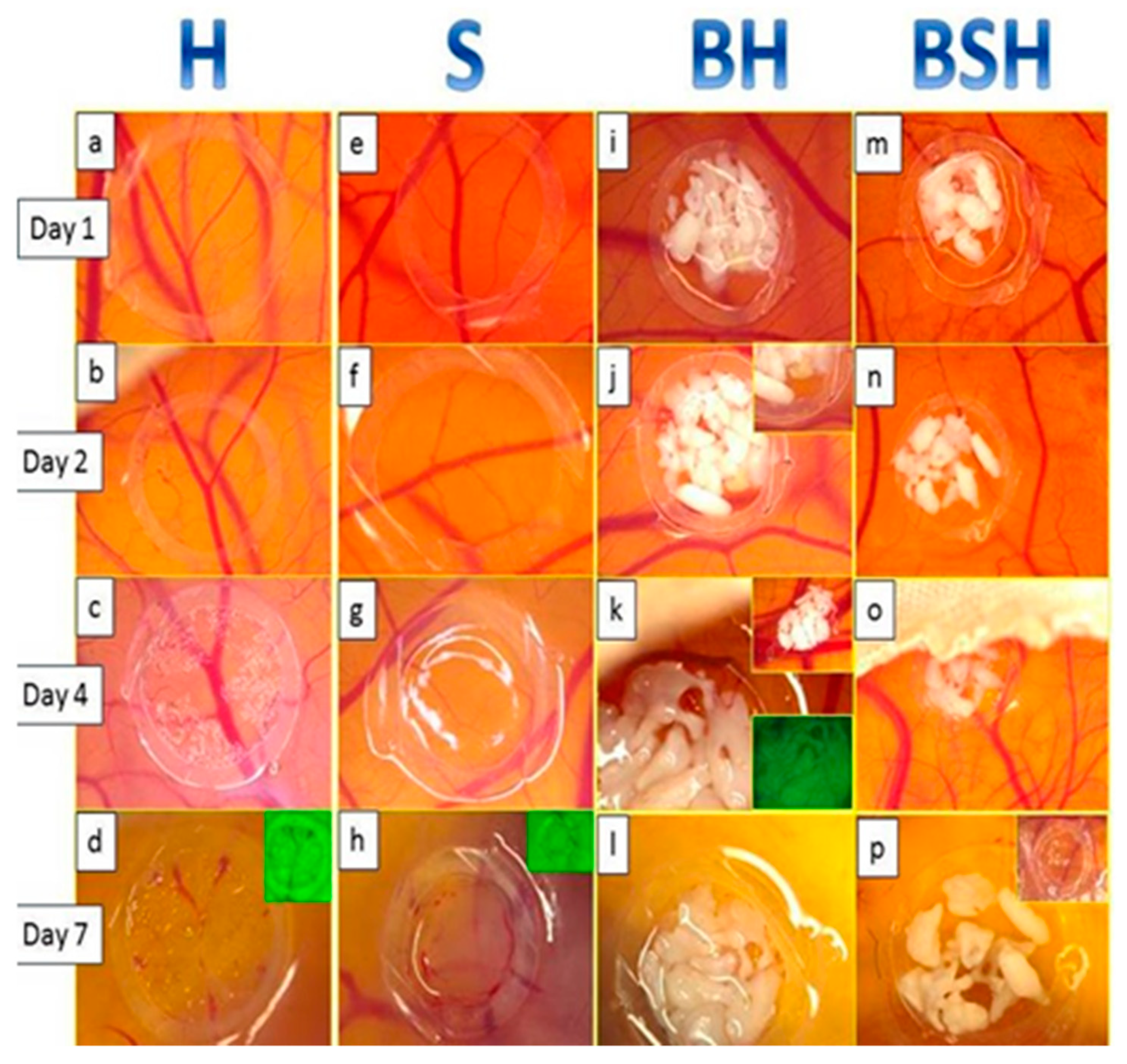
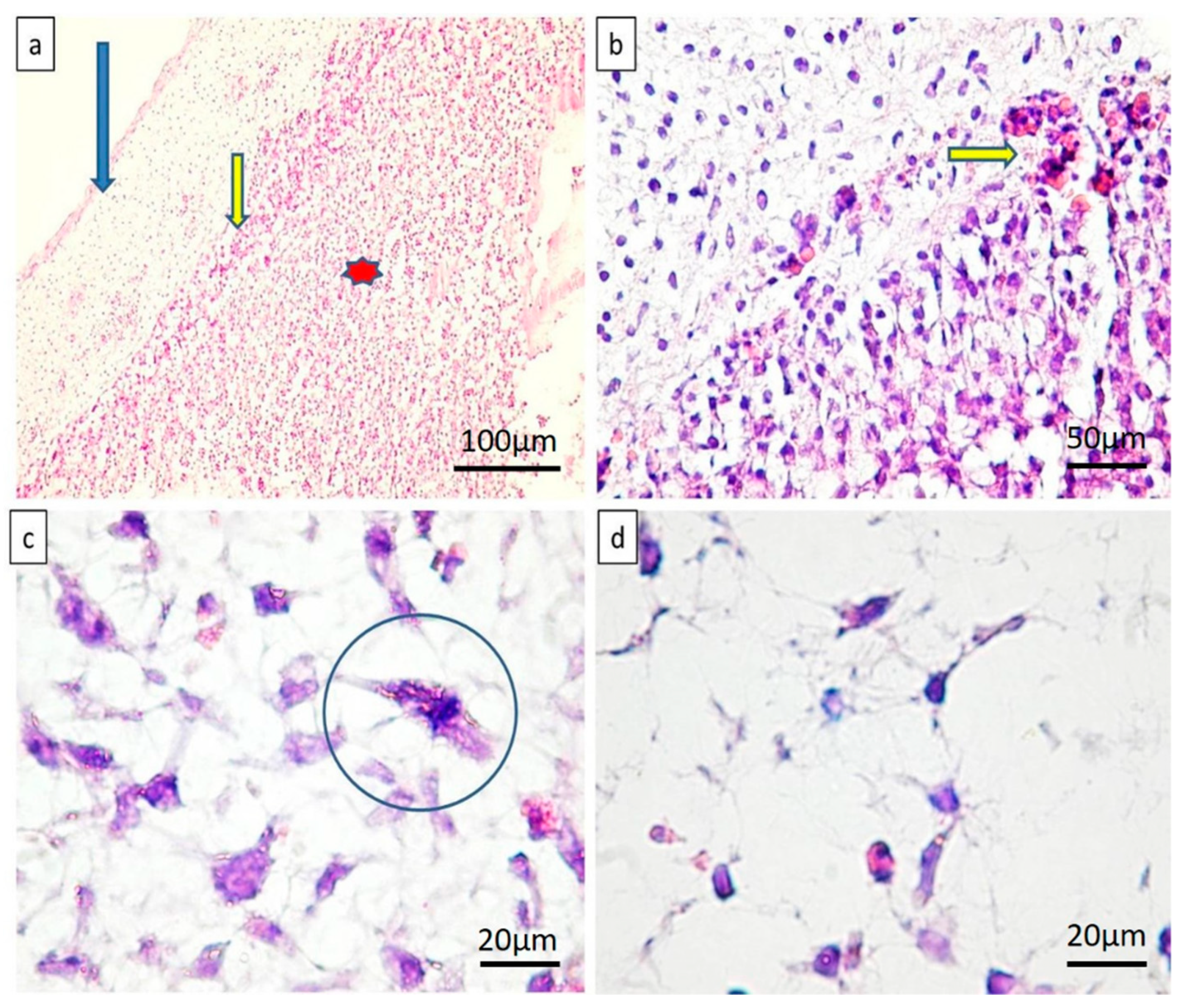
2.1. Microscopic Assessment
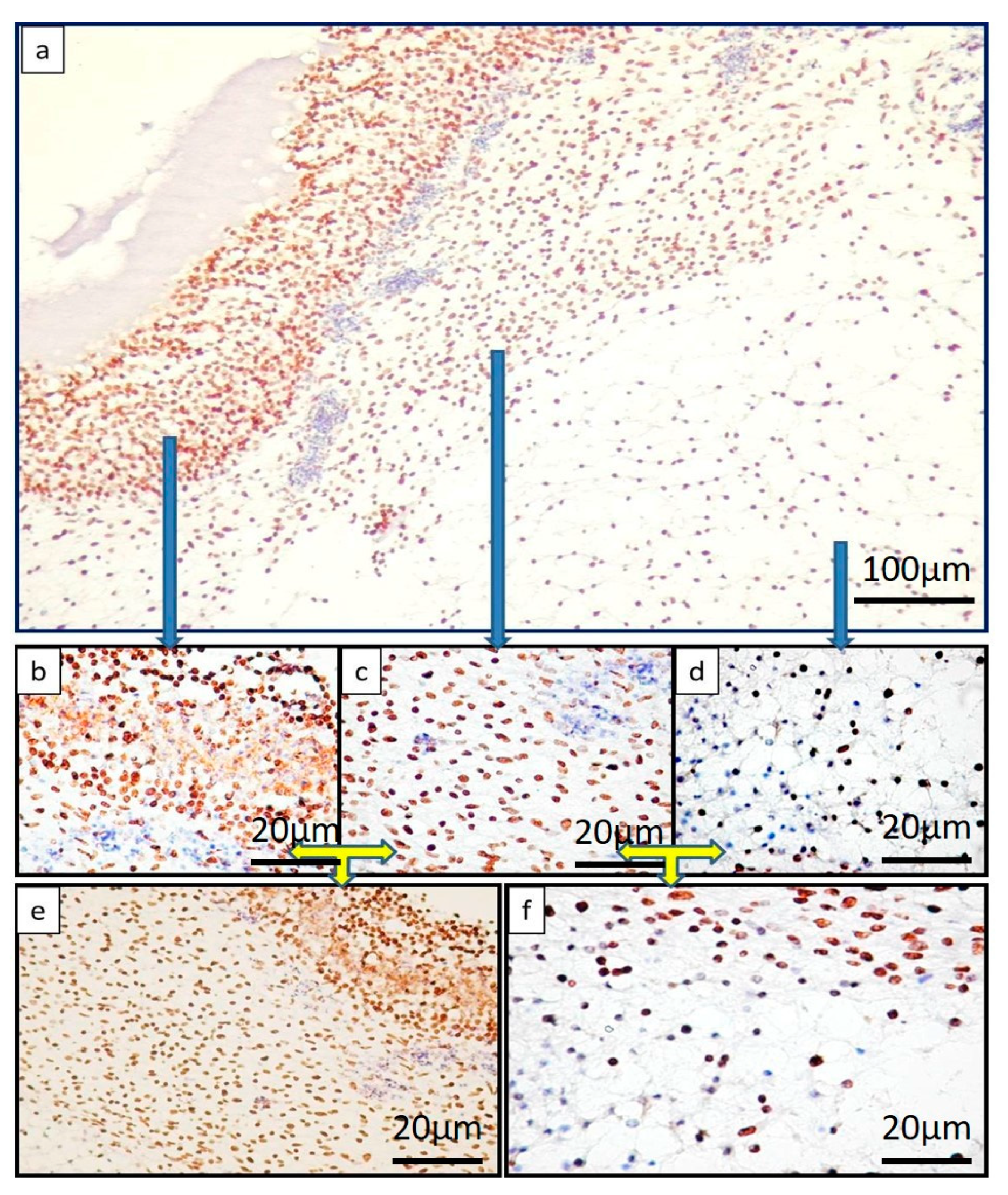
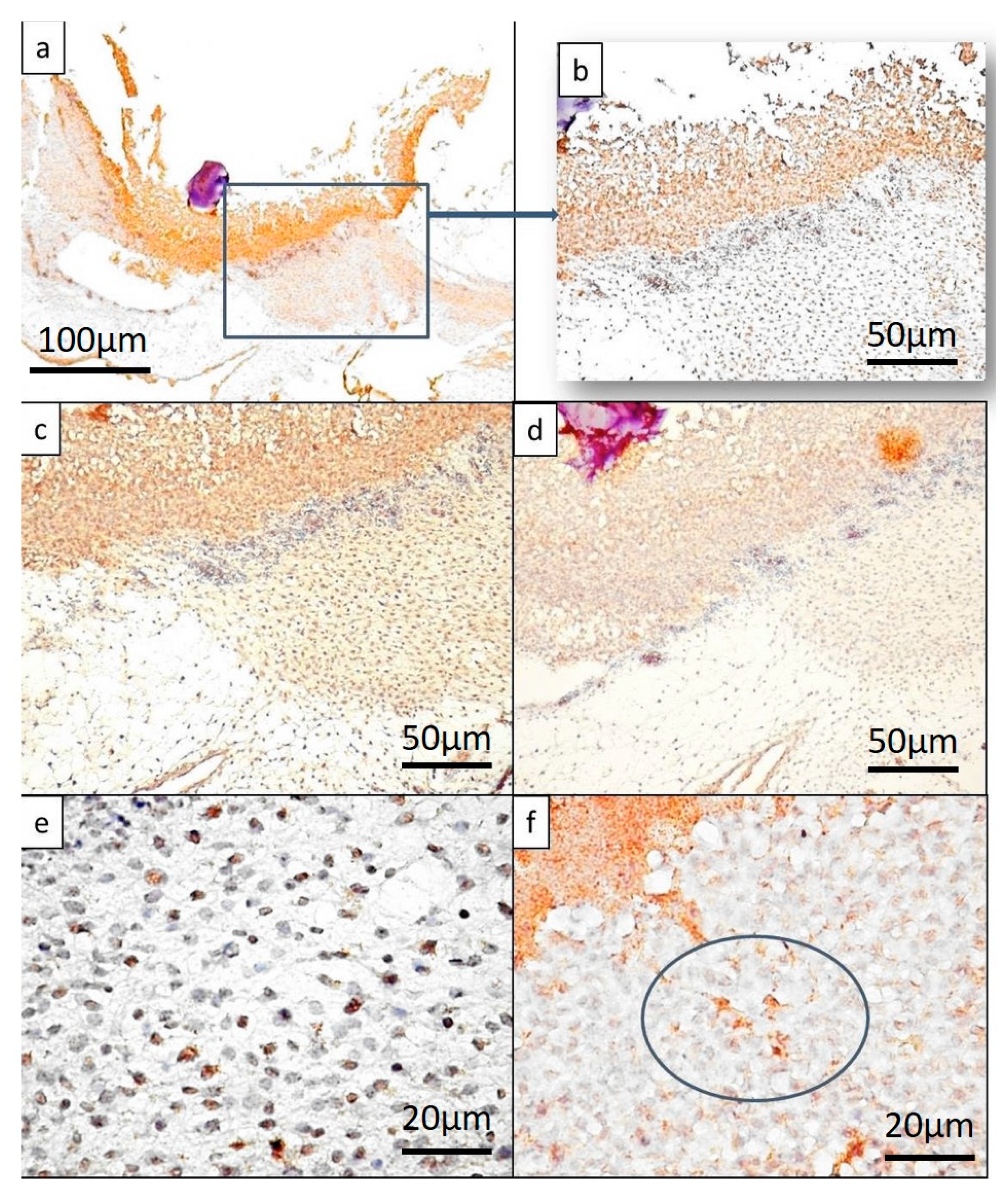
2.2. Immunohistochemistry Evaluation
3. Discussion
4. Materials and Methods
4.1. Bone Substitutes and Resuspension Media
4.2. Chick Embryo Chorioallantoic Membrane Experimental Model
4.3. CAM Harvesting and Primary Processing for Microscopy and Immunohistochemistry
4.4. Image Analysis and Data Acquisition
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Scheines, C.; Hokett, S.D.; Katancik, J.A. Recombinant Human Platelet-Derived Growth Factor-BB in Human Alveolar Ridge Augmentation: A Review of the Literature. Int. J. Oral Maxillofac. Implant. 2018, 33, 1047–1056. [Google Scholar] [CrossRef]
- Tirone, F.; Salzano, S. Esthetic treatment of alveolar ridge atrophy in the anterior maxilla via connective tissue graft performed simultaneously with implant placement: A three-case series. Quintessence Int. 2018, 49, 801–807. [Google Scholar]
- Parvini, P.; Sader, R.; Sahin, D.; Becker, J.; Schwarz, F. Radiographic outcomes following lateral alveolar ridge augmentation using autogenous tooth roots. Int. J. Implant Dent. 2018, 4, 31. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Júnior, I.R.; Souza, F.Á.; Figueiredo, A.A.S.; Poli, P.P.; Benetti, F.; Ferreira, S.; de Melo, W.M.; Rahal, S. Maxillary Alveolar Ridge Atrophy Reconstructed With Autogenous Bone Graft Harvested From the Proximal Ulna. J. Craniofac. Surg. 2018, 29, 1. [Google Scholar] [CrossRef] [PubMed]
- Strauss, F.J.; Stähli, A.; Gruber, R. The use of platelet-rich fibrin to enhance the outcomes of implant therapy: A systematic review. Clin. Oral Implant. Res. 2018, 29 (Suppl. 18), 6–19. [Google Scholar] [CrossRef] [PubMed]
- Rider, P.; Kačarević, Ž.P.; Alkildani, S.; Retnasingh, S.; Schnettler, R.; Barbeck, M. Additive Manufacturing for Guided Bone Regeneration: A Perspective for Alveolar Ridge Augmentation. Int. J. Mol. Sci. 2018, 19, 3308. [Google Scholar] [CrossRef]
- Perić Kačarević, Z.; Kavehei, F.; Houshmand, A.; Franke, J.; Smeets, R.; Rimashevskiy, D.; Wenisch, S.; Schnettler, R.; Jung, O.; Barbeck, M. Purification processes of xenogeneic bone substitutes and their impact on tissue reactions and regeneration. Int. J. Artif. Organs 2018, 41, 789–800. [Google Scholar] [CrossRef] [PubMed]
- Yamada, M.; Egusa, H. Current bone substitutes for implant dentistry. J. Prosthodont. Res. 2018, 62, 152–161. [Google Scholar] [CrossRef]
- Tang, Z.; Li, X.; Tan, Y.; Fan, H.; Zhang, X. The material and biological characteristics of osteoinductive calcium phosphate ceramics. Regen. Biomater. 2018, 5, 43–59. [Google Scholar] [CrossRef]
- Wei, J.; Qian, H.; Liu, Y.; Liu, J.; Zhao, R.; Yang, X.; Zhu, X.; Chen, R.; Zhang, X. Application of osteoinductive calcium phosphate ceramics in children’s endoscopic neurosurgery: REPORT of five cases. Regen. Biomater. 2018, 5, 221–227. [Google Scholar] [CrossRef]
- Kim, Y.J.; de Molon, R.S.; Horiguti, F.R.; Contador, G.P.; Coelho, M.A.; Mascarenhas, V.I.; de Souza Faloni, A.P.; Cirelli, J.A.; Sendyk, W.R. Vertical Bone Augmentation Using Deproteinized Bovine Bone Mineral, Absorbable Collagen Sponge, and Recombinant Human Bone Morphogenetic Protein-2: An In Vivo Study in Rabbits. Int. J. Oral Maxillofac. Implant. 2018, 33, 512–522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, Y.T.; Al-Hezaimi, K.; Galindo-Moreno, P.; O’Valle, F.; Al-Rasheed, A.; Wang, H.L. Effects of Recombinant Human Bone Morphogenetic Protein-2 on Vertical Bone Augmentation in a Canine Model. J. Periodontol. 2017, 88, 896–905. [Google Scholar] [CrossRef] [PubMed]
- Mangir, N.; Raza, A.; Haycock, J.W.; Chapple, C.; Macneil, S. An Improved In Vivo Methodology to Visualise Tumour Induced Changes in Vasculature Using the Chick Chorionic Allantoic Membrane Assay. In Vivo 2018, 32, 461–472. [Google Scholar] [PubMed]
- Deryugina, E.I. Chorioallantoic Membrane Microtumor Model to Study the Mechanisms of Tumor Angiogenesis, Vascular Permeability, and Tumor Cell Intravasation. Methods Mol. Biol. 2016, 1430, 283–298. [Google Scholar]
- Comşa, Ş.; Ceaușu, R.A.; Popescu, R.; Cîmpean, A.M.; Raica, M. The Human Mesenchymal Stem Cells and the Chick Embryo Chorioallantoic Membrane: The Key and the Lock in Revealing Vasculogenesis. In Vivo 2017, 31, 1139–1144. [Google Scholar] [PubMed]
- Comşa, Ş.; Popescu, R.; Avram, Ş.; Ceaușu, R.A.; Cîmpean, A.M.; Raica, M. Bevacizumab Modulation of the Interaction Between the MCF-7 Cell Line and the Chick Embryo Chorioallantoic Membrane. In Vivo 2017, 31, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Ribatti, D.; Tamma, R. The chick embryo chorioallantoic membrane as an in vivo experimental model to study human neuroblastoma. J. Cell Physiol. 2018, 234, 152–157. [Google Scholar] [CrossRef]
- Cimpean, A.M.; Ribatti, D.; Raica, M. The chick embryo chorioallantoic membrane as a model to study tumor metastasis. Angiogenesis 2008, 11, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Cimpean, A.M.; Lalošević, D.; Lalošević, V.; Banović, P.; Raica, M.; Mederle, O.A. Disodium Cromolyn and Anti-podoplanin Antibodies Strongly Inhibit Growth of BHK 21/C13-derived Fibrosarcoma in a Chick Embryo Chorioallantoic Membrane Model. In Vivo 2018, 32, 791–798. [Google Scholar] [CrossRef]
- Cimpean, A.M.; Raica, M. The Hidden Side of Disodium Cromolyn: FROM Mast Cell Stabilizer to an Angiogenic Factor and Antitumor Agent. Arch. Immunol. Ther. Exp. (Warsz) 2016, 64, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Jiménez, I.; Kanczler, J.M.; Hulsart-Billstrom, G.; Inglis, S.; Oreffo, R.O.C. The Chorioallantoic Membrane Assay for Biomaterial Testing in Tissue Engineering: A Short-Term In Vivo Preclinical Model. Tissue Eng. Part C Methods 2017, 23, 938–952. [Google Scholar] [CrossRef] [PubMed]
- Azzarello, J.; Ihnat, M.A.; Kropp, B.P.; Warnke, L.A.; Lin, H.K. Assessment of angiogenic properties of biomaterials using the chicken embryo chorioallantoic membrane assay. Biomed. Mater. 2007, 2, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Jiménez, I.; Hulsart-Billstrom, G.; Lanham, S.A. The chorioallantoic membrane (CAM) assay for the study of human bone regeneration: A refinement animal model for tissue engineering. Sci Rep. 2016, 6, 32168. [Google Scholar] [CrossRef]
- Moreno-Jiménez, I.; Lanham, S.A.; Kanczler, J.M.; Hulsart-Billstrom, G.; Evans, N.D.; Oreffo, R.O.C. Remodelling of human bone on the chorioallantoic membrane of the chicken egg: De novo bone formation and resorption. J. Tissue Eng. Regen. Med. 2018, 12, 1877–1890. [Google Scholar] [CrossRef]
- Burgio, F.; Rimmer, N.; Pieles, U.; Buschmann, J.; Beaufils-Hugot, M. Characterization and in ovo vascularisation of a 3D-printed hydroxyapatite scaffold with different extracellular matrix coatings under perfusion culture. Biol. Open 2018, 7, bio034488. [Google Scholar] [CrossRef] [PubMed]
- Freyre-Fonseca, V.; Medina-Reyes, E.I.; Téllez-Medina, D.I.; Paniagua-Contreras, G.L.; Monroy-Pérez, E.; Vaca-Paniagua, F.; Delgado-Buenrostro, N.L.; Flores-Flores, J.O.; López-Villegas, E.O.; Gutiérrez-López, G.F.; et al. Influence of shape and dispersion media of titanium dioxide nanostructures on microvessel network and ossification. Colloids Surf. B Biointerfaces 2018, 162, 193–201. [Google Scholar] [CrossRef]
- Bronckaers, A.; Hilkens, P.; Fanton, Y.; Struys, T.; Gervois, P.; Politis, C.; Martens, W.; Lambrichts, I. Angiogenic properties of human dental pulp stem cells. PLoS ONE 2013, 8, e71104. [Google Scholar] [CrossRef] [PubMed]
- Kauvar, A.S.; Thoma, D.S.; Carnes, D.L.; Cochran, D.L. In vivo angiogenic activity of enamel matrix derivative. J. Periodontol. 2010, 81, 1196–1201. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.S.; Hussain, A.N.; Sidra, L.; Sarfraz, Z.; Khalid, H.; Khan, M.; Manzoor, F.; Shahzadi, L.; Yar, M.; Rehman, I.U. Fabrication and in vivo evaluation of hydroxyapatite/carbon nanotube electrospun fibers for biomedical/dental application. Mater. Sci. Eng. C Mater. Biol. Appl. 2017, 80, 387–396. [Google Scholar] [CrossRef]
- Klueh, U.; Dorsky, D.I.; Moussy, F.; Kreutzer, D.L. Ex ovo chick chorioallantoic membrane as a novel model for evaluation of tissue responses to biomaterials and implants. J. Biomed. Mater. Res. A 2003, 67, 838–843. [Google Scholar] [CrossRef] [PubMed]
- Tatum, O.H. Maxillary and sinus implant reconstruction. Dent. Clin. N. Am. 1986, 30, 207–229. [Google Scholar] [PubMed]
- Boyne, P.J.; James, R.A. Grafting of the maxillary sinus floor with autogenous marrow and bone. J. Oral Surg. 1980, 38, 613–616. [Google Scholar] [PubMed]
- van den Bergh, J.P.; ten Bruggenkate, C.M.; Disch, F.J.; Tuinzing, D.B. Anatomical aspects of sinus floor elevations. Clin. Oral Implant. Res. 2000, 11, 256–265. [Google Scholar] [CrossRef]
- Garg, A.K. Augmentation grafting of the maxillary sinus for placement of dental implants: Anatomy, physiology, and procedures. Implant Dent. 1999, 8, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Klein, K.; Zamparo, E.; Kronen, P.W.; Kämpf, K.; Makara, M.; Steffen, T.; von Rechenberg, B. Bone augmentation for cancellous bone- development of a new animal model. BMC Musculoskelet. Disord. 2013, 14, 200. [Google Scholar] [CrossRef]
- Ramírez-Fernández, M.P.; Calvo-Guirado, J.L.; de-Val, J.E.; Delgado-Ruiz, R.A.; Negri, B.; Pardo-Zamora, G.; Peñarrocha, D.; Barona, C.; Granero, J.M.; Alcaraz-Baños, M. Melatonin promotes angiogenesis during repair of bone defects: A radiological and histomorphometric study in rabbit tibiae. Clin. Oral Investig. 2013, 17, 147–158. [Google Scholar] [CrossRef] [PubMed]
- Seo, J.P.; Tsuzuki, N.; Haneda, S.; Yamada, K.; Furuoka, H.; Tabata, Y.; Sasaki, N. Osteoinductivity of gelatin/β-tricalcium phosphate sponges loaded with different concentrations of mesenchymal stem cells and bone morphogenetic protein-2 in an equine bone defect model. Vet. Res. Commun. 2014, 38, 73–80. [Google Scholar] [CrossRef]
- Zecha, P.J.; Schortinghuis, J.; van der Wal, J.E.; Nagursky, H.; van den Broek, K.C.; Sauerbier, S.; Vissink, A.; Raghoebar, G.M. Applicability of equine hydroxyapatite collagen (eHAC) bone blocks for lateral augmentation of the alveolar crest. A histological and histomorphometric analysis in rats. Int. J. Oral Maxillofac. Surg. 2011, 40, 533–542. [Google Scholar] [CrossRef]
- Benlidayi, M.E.; Gaggl, A.; Buerger, H.; Kahraman, O.E.; Sencar, L.; Brandtner, C.; Kurkcu, M.; Polat, S.; Borumandi, F. Comparative study of the osseous healing process following three different techniques of bone augmentationin the mandible: An experimental study. Int. J. Oral Maxillofac. Surg. 2014, 43, 1404–1410. [Google Scholar] [CrossRef]
- Schwarz, F.; Ferrari, D.; Balic, E.; Buser, D.; Becker, J.; Sager, M. Lateral ridge augmentation using equine- and bovine-derived cancellous bone blocks: A feasibility study in dogs. Clin. Oral Implant. Res. 2010, 21, 904–912. [Google Scholar] [CrossRef]
- Ono, D.; Jimbo, R.; Kawachi, G.; Ioku, K.; Ikeda, T.; Sawase, T. Lateral bone augmentation with newly developed β-tricalcium phosphate block: An experimental study in the rabbit mandible. Clin. Oral Implant. Res. 2011, 22, 1366–1371. [Google Scholar] [CrossRef] [PubMed]
- Altuğ, H.A.; Aydintuğ, Y.S.; Sençimen, M.; Günhan, O.; Ortakoğlu, K.; Bayar, G.R.; Doğan, N. Histomorphometric analysis of different latency periods effect on new bone obtained by periosteal distraction: An experimental study in the rabbit model. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2011, 111, 539–546. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.I.; Chung, C.P.; Heo, M.S.; Park, Y.J.; Rhee, S.H. Periodontal regeneration capacity of equine particulate bone in canine alveolar bone defects. J. Periodontal Implant Sci. 2010, 40, 220–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holzmann, P.; Niculescu-Morzsa, E.; Zwickl, H.; Halbwirth, F.; Pichler, M.; Matzner, M.; Gottsauner-Wolf, F. Investigation of bone allografts representing different steps of the bone bank procedure using the CAM-model. ALTEX 2010, 27, 97–103. [Google Scholar] [CrossRef]
- Yabe, H.; Hanaoka, H. Investigation of the origin of the osteoclast by use of transplantation on chick chorioallantoic membrane. Clin. Orthop. Relat. Res. 1985, 197, 255–265. [Google Scholar] [CrossRef]
- Vargas, G.E.; Mesones, R.V.; Bretcanu, O.; López, J.M.; Boccaccini, A.R.; Gorustovich, A. Biocompatibility and bone mineralization potential of 45S5 Bioglass-derived glass-ceramic scaffolds in chick embryos. Acta Biomater. 2009, 5, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Piattelli, A.; Degidi, M.; Di Stefano, D.A.; Rubini, C.; Fioroni, M.; Strocchi, R. Microvessel density in alveolar ridge regeneration with autologous and alloplastic bone. Implant Dent. 2002, 11, 370–375. [Google Scholar] [CrossRef]
- Di Stefano, D.A.; Artese, L.; Iezzi, G.; Piattelli, A.; Pagnutti, S.; Piccirilli, M.; Perrotti, V. Alveolar ridge regeneration with equine spongy bone: A clinical, histological, and immunohistochemical case series. Clin. Implant Dent. Relat. Res. 2009, 11, 90–100. [Google Scholar] [CrossRef] [PubMed]
- Rachmiel, A.; Leiser, Y. The Molecular and Cellular Events That Take Place during Craniofacial Distraction Osteogenesis. Plast. Reconstr. Surg. Glob. Open 2014, 2, E98. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Substance/Sample | Angiogenic Response | Inflammation | RUNX2 | SPARC | BMP4 | Bone Particle Architecture |
|---|---|---|---|---|---|---|
| H | Present | No | Negative | Negative | Negative | - |
| S | No | Present | Negative | Negative | Negative | - |
| BH | Present, intense around implant | No | Positive with specific multilayered distribution. High density and intensity | Positive, respecting the layered distribution | Positive, heterogeneous distribution | Compact layer of interlaced bone lamellae, no resorption detected at the end of the experiment |
| BS | No | Present | +/−, inconsistent | Negative | Negative | Totally resorbed at the end of the experiment |
| BSH | Present, related to inflammation | Large inflammatory infiltrate | Positive | Positive in inflammatory cells, not in mesenchymal cells of CAM | Positive in inflammatory cells, not in mesenchymal cells of CAM | Dispersed arrangement of bone particles |
| Substance/Sample | BIO-GEN | Saline | Hyaluronic Barrier Gel | Saline + Hyaluronic |
|---|---|---|---|---|
| H | - | - | 0.1 μL | - |
| S | - | 0.1 μL | - | - |
| BH | 0.5 g | - | 0.5 mL | - |
| BSH | 0.5 g | 1 mL | 0.3 mL | 1 + 0.3 mL |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cirligeriu, L.; Cimpean, A.M.; Calniceanu, H.; Vladau, M.; Sarb, S.; Raica, M.; Nica, L. Hyaluronic Acid/Bone Substitute Complex Implanted on Chick Embryo Chorioallantoic Membrane Induces Osteoblastic Differentiation and Angiogenesis, but not Inflammation. Int. J. Mol. Sci. 2018, 19, 4119. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms19124119
Cirligeriu L, Cimpean AM, Calniceanu H, Vladau M, Sarb S, Raica M, Nica L. Hyaluronic Acid/Bone Substitute Complex Implanted on Chick Embryo Chorioallantoic Membrane Induces Osteoblastic Differentiation and Angiogenesis, but not Inflammation. International Journal of Molecular Sciences. 2018; 19(12):4119. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms19124119
Chicago/Turabian StyleCirligeriu, Laura, Anca Maria Cimpean, Horia Calniceanu, Mircea Vladau, Simona Sarb, Marius Raica, and Luminita Nica. 2018. "Hyaluronic Acid/Bone Substitute Complex Implanted on Chick Embryo Chorioallantoic Membrane Induces Osteoblastic Differentiation and Angiogenesis, but not Inflammation" International Journal of Molecular Sciences 19, no. 12: 4119. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms19124119