Comparison between Slow Freezing and Vitrification for Human Ovarian Tissue Cryopreservation and Xenotransplantation


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
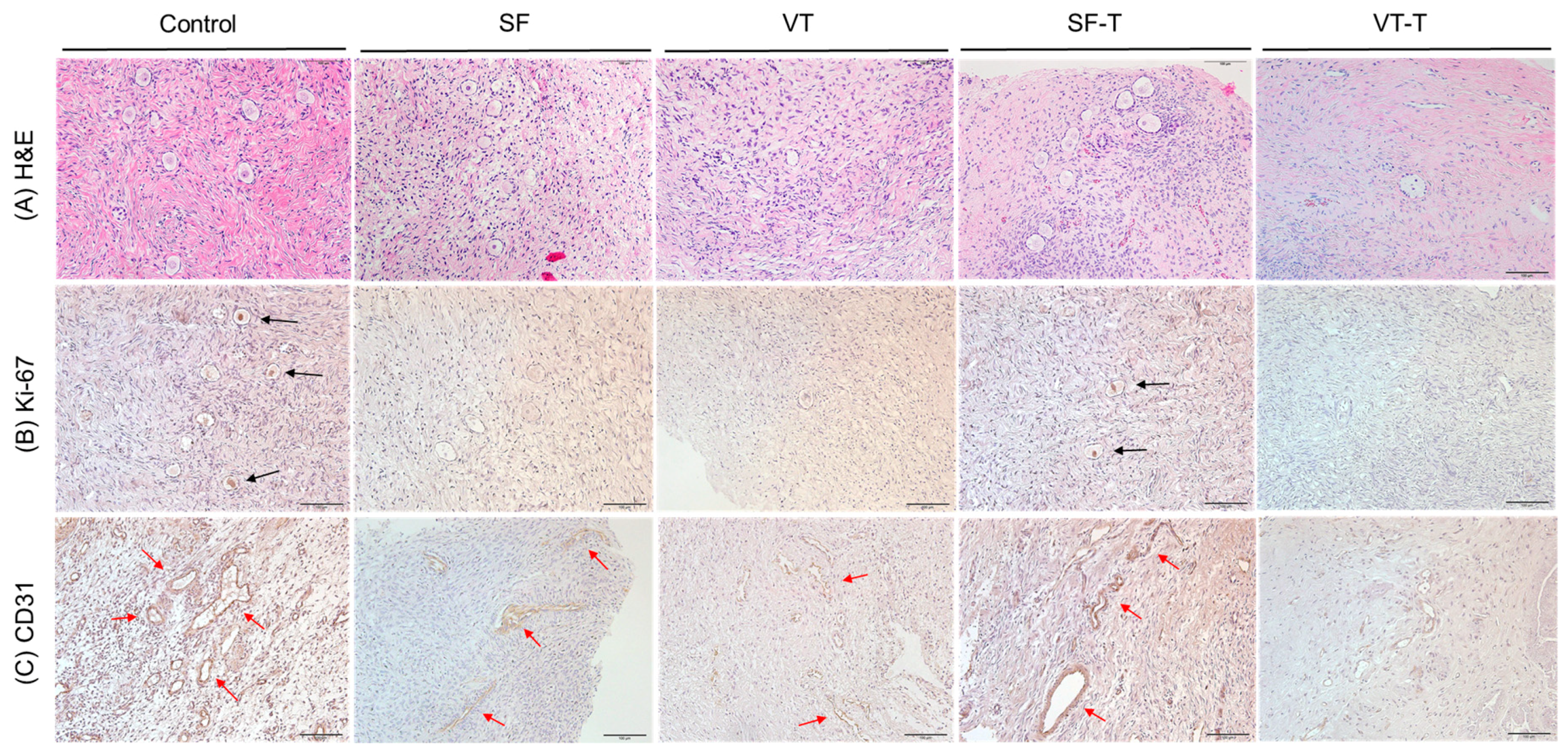
2.1. Histologic Evaluation and Primordial Follicular Counts
2.2. Follicular Cell Proliferation and Neo-Vascularization
2.3. Gonadotropin Receptors
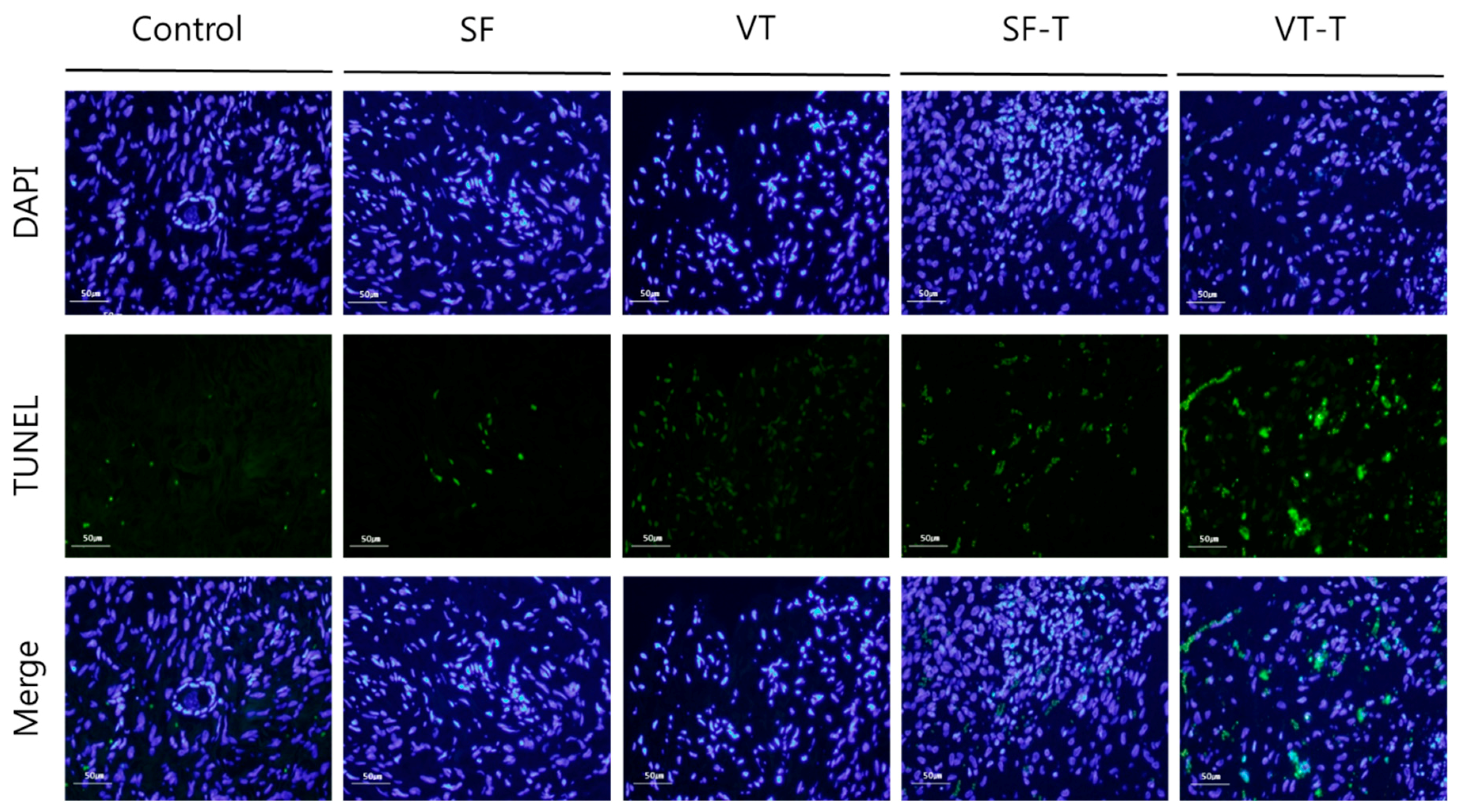
2.4. DNA Damage
2.5. Western Blot Analysis
2.6. Fine Structural Evaluation by Transmission Electron Microscopy (TEM)
3. Discussion
4. Materials and Methods
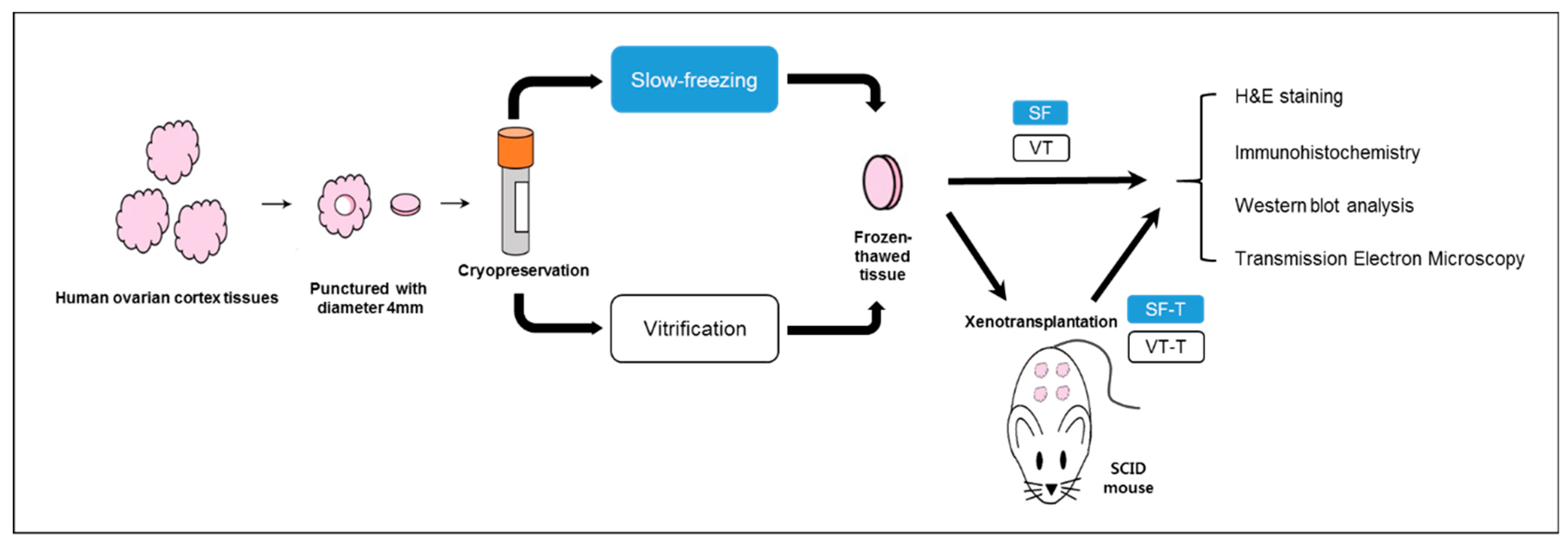
4.1. Study Design
4.2. Slow Freezing Protocol
4.3. Vitrification Protocol
4.4. Slow Freezing-Thawing Protocol
4.5. Vitrification-Thawing Protocol
4.6. Xenotransplantation into SCID Mice
4.7. Histologic Evaluation
4.8. Immunohistochemistry Evaluation
4.9. Immunofluorescence Staining Evaluation
4.10. TUNEL Assay
4.11. Western Blot
4.12. TEM
4.13. Statistical Analyses
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| SCID | severe combined immunodeficient |
| DMSO | dimethyl sulfoxide |
| TUNEL | terminal deoxynucleotidyl transferase-mediated dUTP nick-end labeling |
| TEM | transmission electron microscopy |
| AMH | anti-Müllerian hormone |
References
- Tiong, V.; Rozita, A.M.; Taib, N.A.; Yip, C.H.; Ng, C.H. Incidence of chemotherapy-induced ovarian failure in premenopausal women undergoing chemotherapy for breast cancer. World J. Surg. 2014, 38, 2288–2296. [Google Scholar] [CrossRef] [PubMed]
- Howell, S.; Shalet, S. Gonadal damage from chemotherapy and radiotherapy. Endocrinol. Metab. Clin. N. Am. 1998, 27, 927–943. [Google Scholar] [CrossRef]
- Rosen, A.; Rodriguez-Wallberg, K.A.; Rosenzweig, L. Psychosocial distress in young cancer survivors. Semin. Oncol. Nurs. 2009, 25, 268–277. [Google Scholar] [CrossRef] [PubMed]
- Vehmanen, L.; Saarto, T.; Elomaa, I.; Makela, P.; Valimaki, M.; Blomqvist, C. Long-term impact of chemotherapy-induced ovarian failure on bone mineral density (BMD) in premenopausal breast cancer patients. The effect of adjuvant clodronate treatment. Eur. J. Cancer 2001, 37, 2373–2378. [Google Scholar] [CrossRef]
- Lee, S.; Heytens, E.; Moy, F.; Ozkavukcu, S.; Oktay, K. Determinants of access to fertility preservation in women with breast cancer. Fertil. Steril. 2011, 95, 1932–1936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.; Ozkavukcu, S.; Heytens, E.; Moy, F.; Oktay, K. Value of early referral to fertility preservation in young women with breast cancer. J. Clin. Oncol. 2010, 28, 4683–4686. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Oktay, K.; Gracia, C.; Lee, S.; Morse, C.; Mersereau, J.E. Which patients pursue fertility preservation treatments? A multicenter analysis of the predictors of fertility preservation in women with breast cancer. Fertil. Steril. 2012, 97, 671–676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oktay, K.; Harvey, B.E.; Partridge, A.H.; Quinn, G.P.; Reinecke, J.; Taylor, H.S.; Wallace, W.H.; Wang, E.T.; Loren, A.W. Fertility preservation in patients with cancer: ASCO Clinical Practice Guideline Update. J. Clin. Oncol. 2018, 36, 1994–2001. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Kim, S.K.; Hwang, K.J.; Kim, T.; Kim, S.H. Fertility preservation for patients with gynecologic malignancies: The Korean Society for Fertility Preservation clinical guidelines. Clin. Exp. Reprod. Med. 2017, 44, 175–180. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.; Oktay, K. Does higher starting dose of FSH stimulation with letrozole improve fertility preservation outcomes in women with breast cancer? Fertil. Steril. 2012, 98, 961–964. [Google Scholar] [CrossRef]
- Campos, A.L.; Guedes Jde, S.; Rodrigues, J.K.; Pace, W.A.; Fontoura, R.R.; Caetano, J.P.; Marinho, R.M. Comparison between slow freezing and vitrification in terms of ovarian tissue viability in a bovine model. Rev. Bras. Ginecol. Obstet. 2016, 38, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Lee, Y.; Lee, S.; Kim, T. Ovarian tissue cryopreservation and transplantation in patients with cancer. Obstet. Gynecol. Sci. 2018, 61, 431–442. [Google Scholar] [CrossRef] [PubMed]
- Oktay, K.; Karlikaya, G. Ovarian function after transplantation of frozen, banked autologous ovarian tissue. N. Engl. J. Med. 2000, 342, 1919. [Google Scholar] [CrossRef] [PubMed]
- Donnez, J.; Dolmans, M.M.; Demylle, D.; Jadoul, P.; Pirard, C.; Squifflet, J.; Martinez-Madrid, B.; van Langendonckt, A. Livebirth after orthotopic transplantation of cryopreserved ovarian tissue. Lancet 2004, 364, 1405–1410. [Google Scholar] [CrossRef]
- Seli, E.; Tangir, J. Fertility preservation options for female patients with malignancies. Curr. Opin. Obstet. Gynecol. 2005, 17, 299–308. [Google Scholar] [CrossRef] [PubMed]
- Practice Committee of American Society for Reproductive Medicine. Ovarian tissue cryopreservation: A committee opinion. Fertil. Steril. 2014, 101, 1237–1243. [Google Scholar] [CrossRef]
- Silber, S. Ovarian tissue cryopreservation and transplantation: Scientific implications. J. Assist. Reprod. Genet. 2016, 33, 1595–1603. [Google Scholar] [CrossRef]
- Diaz-Garcia, C.; Domingo, J.; Garcia-Velasco, J.A.; Herraiz, S.; Mirabet, V.; Iniesta, I.; Cobo, A.; Remohi, J.; Pellicer, A. Oocyte vitrification versus ovarian cortex transplantation in fertility preservation for adult women undergoing gonadotoxic treatments: A prospective cohort study. Fertil. Steril. 2018, 109, 478–485. [Google Scholar] [CrossRef]
- Donnez, J.; Dolmans, M.M. Fertility Preservation in Women. N. Engl. J. Med. 2017, 377, 1657–1665. [Google Scholar] [CrossRef]
- Mazur, P. Equilibrium, quasi-equilibrium, and nonequilibrium freezing of mammalian embryos. Cell Biophys. 1990, 17, 53–92. [Google Scholar] [CrossRef]
- Vajta, G.; Nagy, Z.P. Are programmable freezers still needed in the embryo laboratory? Review on vitrification. Reprod. Biomed. Online 2006, 12, 779–796. [Google Scholar] [CrossRef]
- Gandolfi, F.; Paffoni, A.; Papasso Brambilla, E.; Bonetti, S.; Brevini, T.A.; Ragni, G. Efficiency of equilibrium cooling and vitrification procedures for the cryopreservation of ovarian tissue: Comparative analysis between human and animal models. Fertil. Steril. 2006, 85 (Suppl. 1), 1150–1156. [Google Scholar] [CrossRef]
- Jensen, A.K.; Macklon, K.T.; Fedder, J.; Ernst, E.; Humaidan, P.; Andersen, C.Y. 86 successful births and 9 ongoing pregnancies worldwide in women transplanted with frozen-thawed ovarian tissue: Focus on birth and perinatal outcome in 40 of these children. J. Assist. Reprod. Genet. 2017, 34, 325–336. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, N.; Yoshioka, N.; Takae, S.; Sugishita, Y.; Tamura, M.; Hashimoto, S.; Morimoto, Y.; Kawamura, K. Successful fertility preservation following ovarian tissue vitrification in patients with primary ovarian insufficiency. Hum. Reprod. 2015, 30, 608–615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amorim, C.A.; Curaba, M.; Van Langendonckt, A.; Dolmans, M.M.; Donnez, J. Vitrification as an alternative means of cryopreserving ovarian tissue. Reprod. Biomed. Online 2011, 23, 160–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.; Song, J.Y.; Ku, S.Y.; Kim, S.H.; Kim, T. Fertility preservation in women with cancer. Clin. Exp. Reprod. Med. 2012, 39, 46–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, X.H.; Zhang, D.; Shi, J.; Wu, Y.J. Comparison of vitrification and conventional slow freezing for cryopreservation of ovarian tissue with respect to the number of intact primordial follicles: A meta-analysis. Medicine 2016, 95, e4095. [Google Scholar] [CrossRef] [PubMed]
- Oktem, O.; Alper, E.; Balaban, B.; Palaoglu, E.; Peker, K.; Karakaya, C.; Urman, B. Vitrified human ovaries have fewer primordial follicles and produce less antimullerian hormone than slow-frozen ovaries. Fertil. Steril. 2011, 95, 2661–2664. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Z.; Wang, Y.; Li, L.L.; Li, S.W. In vitro culture thawed human ovarian tissue: NIV versus slow freezing method. Cryo Lett. 2013, 34, 520–526. [Google Scholar] [PubMed]
- Shi, Q.; Xie, Y.; Wang, Y.; Li, S. Vitrification versus slow freezing for human ovarian tissue cryopreservation: A systematic review and meta-analysis. Sci. Rep. 2017, 7, 8538. [Google Scholar] [CrossRef]
- Liu, J.; Van der Elst, J.; Van den Broecke, R.; Dhont, M. Early massive follicle loss and apoptosis in heterotopically grafted newborn mouse ovaries. Hum. Reprod. 2002, 17, 605–611. [Google Scholar] [CrossRef]
- Youm, H.W.; Lee, J.; Kim, E.J.; Kong, H.S.; Lee, J.R.; Suh, C.S.; Kim, S.H. Effects of angiopoietin-2 on transplanted mouse ovarian tissue. PLoS ONE 2016, 11, e0166782. [Google Scholar] [CrossRef]
- Choi, W.J.; Lee, J.H.; Park, M.H.; Choi, I.Y.; Park, J.K.; Shin, J.K.; Lee, S.A.; Paik, W.Y.; Lee, J.H. Influence of the vitrification solution on the angiogenic factors in vitrificated mouse ovarian tissue. Obstet. Gynecol. Sci. 2013, 56, 382–388. [Google Scholar] [CrossRef]
- Donnez, J.; Dolmans, M.M.; Pellicer, A.; Diaz-Garcia, C.; Sanchez Serrano, M.; Schmidt, K.T.; Ernst, E.; Luyckx, V.; Andersen, C.Y. Restoration of ovarian activity and pregnancy after transplantation of cryopreserved ovarian tissue: A review of 60 cases of reimplantation. Fertil. Steril. 2013, 99, 1503–1513. [Google Scholar] [CrossRef]
- Herraiz, S.; Novella-Maestre, E.; Rodriguez, B.; Diaz, C.; Sanchez-Serrano, M.; Mirabet, V.; Pellicer, A. Improving ovarian tissue cryopreservation for oncologic patients: Slow freezing versus vitrification, effect of different procedures and devices. Fertil. Steril. 2014, 101, 775–784. [Google Scholar] [CrossRef]
- Amorim, C.A.; Dolmans, M.M.; David, A.; Jaeger, J.; Vanacker, J.; Camboni, A.; Donnez, J.; Van Langendonckt, A. Vitrification and xenografting of human ovarian tissue. Fertil. Steril. 2012, 98, 1291–1298. [Google Scholar] [CrossRef]
- Rahimi, G.; Isachenko, V.; Kreienberg, R.; Sauer, H.; Todorov, P.; Tawadros, S.; Mallmann, P.; Nawroth, F.; Isachenko, E. Re-vascularisation in human ovarian tissue after conventional freezing or vitrification and xenotransplantation. Eur. J. Obstet. Gynecol. Reprod. Biol. 2010, 149, 63–67. [Google Scholar] [CrossRef]
- Rahimi, G.; Isachenko, V.; Todorov, P.; Tawadros, S.; Mallmann, P.; Nawaroth, F.; Isachenko, E. Apoptosis in human ovarian tissue after conventional freezing or vitrification and xenotransplantation. Cryo Lett. 2009, 30, 300–309. [Google Scholar]
- Shams Mofarahe, Z.; Ghaffari Novin, M.; Jafarabadi, M.; Salehnia, M.; Noroozian, M.; Ghorbanmehr, N. Effect of human ovarian tissue vitrification/warming on the expression of genes related to folliculogenesis. Iran. Biomed. J. 2015, 19, 220–225. [Google Scholar]
- Van Eyck, A.S.; Bouzin, C.; Feron, O.; Romeu, L.; Van Langendonckt, A.; Donnez, J.; Dolmans, M.M. Both host and graft vessels contribute to revascularization of xenografted human ovarian tissue in a murine model. Fertil. Steril. 2010, 93, 1676–1685. [Google Scholar] [CrossRef]
- Oktay, K.; Economos, K.; Kan, M.; Rucinski, J.; Veeck, L.; Rosenwaks, Z. Endocrine function and oocyte retrieval after autologous transplantation of ovarian cortical strips to the forearm. JAMA 2001, 286, 1490–1493. [Google Scholar] [CrossRef]
- Kim, Y.Y.; Kim, Y.J.; Cho, K.M.; Kim, S.H.; Park, K.E.; Kang, B.C.; Jung, K.C.; Kim, M.S.; Ku, S.Y. The expression profile of angiotensin system on thawed murine ovaries. Tissue Eng. Regen. Med. 2016, 17, 724–731. [Google Scholar] [CrossRef]
- Oktay, K.; Karlikaya, G.G.; Aydin, B.A. Ovarian cryopreservation and transplantation: Basic aspects. Mol. Cell. Endocrinol. 2000, 169, 105–108. [Google Scholar] [CrossRef]
- Kagawa, N.; Silber, S.; Kuwayama, M. Successful vitrification of bovine and human ovarian tissue. Reprod. Biomed. Online 2009, 18, 568–577. [Google Scholar] [CrossRef]
- Myers, M.; Britt, K.L.; Wreford, N.G.; Ebling, F.J.; Kerr, J.B. Methods for quantifying follicular numbers within the mouse ovary. Reproduction 2004, 127, 569–580. [Google Scholar] [CrossRef]








© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.; Ryu, K.-J.; Kim, B.; Kang, D.; Kim, Y.Y.; Kim, T. Comparison between Slow Freezing and Vitrification for Human Ovarian Tissue Cryopreservation and Xenotransplantation. Int. J. Mol. Sci. 2019, 20, 3346. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20133346
Lee S, Ryu K-J, Kim B, Kang D, Kim YY, Kim T. Comparison between Slow Freezing and Vitrification for Human Ovarian Tissue Cryopreservation and Xenotransplantation. International Journal of Molecular Sciences. 2019; 20(13):3346. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20133346
Chicago/Turabian StyleLee, Sanghoon, Ki-Jin Ryu, Boram Kim, Dahyeon Kang, Yoon Young Kim, and Tak Kim. 2019. "Comparison between Slow Freezing and Vitrification for Human Ovarian Tissue Cryopreservation and Xenotransplantation" International Journal of Molecular Sciences 20, no. 13: 3346. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20133346