BNP as a Major Player in the Heart-Kidney Connection

1
Department of Cardiology and Nephrology, Mie University Graduate School of Medicine, 2-174 Edobashi, Tsu, Mie 514-8507, Japan
2
Department of Pathology and Matrix Biology, Mie University Graduate School of Medicine, 2-174 Edobashi, Tsu, Mie 514-8507, Japan
3
Department of Animal Genomics, Functional Genomics Institute, Mie University Life Science Research Center, 2-174 Edobashi, Tsu, Mie 514-8507, Japan
*
Author to whom correspondence should be addressed.
Int. J. Mol. Sci. 2019, 20(14), 3581; https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20143581
Submission received: 22 June 2019
/
Revised: 15 July 2019
/
Accepted: 17 July 2019
/
Published: 22 July 2019
(This article belongs to the Special Issue Molecular Basis of Cardiovascular Diseases: Implications of Natriuretic Peptides)
Abstract
:Brain natriuretic peptide (BNP) is an important biomarker for patients with heart failure, hypertension and cardiac hypertrophy. Although it is known that BNP levels are relatively higher in patients with chronic kidney disease and no heart disease, the mechanism remains unknown. Here, we review the functions and the roles of BNP in the heart-kidney interaction. In addition, we discuss the relevant molecular mechanisms that suggest BNP is protective against chronic kidney diseases and heart failure, especially in terms of the counterparts of the renin-angiotensin-aldosterone system (RAAS). The renal medulla has been reported to express depressor substances. The extract of the papillary tips from kidneys may induce the expression and secretion of BNP from cardiomyocytes. A better understanding of these processes will help accelerate pharmacological treatments for heart-kidney disease.
1. Introduction
The Brain natriuretic peptide (BNP), which is a component of the natriuretic peptide (NP) system and also known as B-type NP, is mainly secreted from the cardiomyocytes in response to cardiac stretch and ischemia, and plays an important role in cardiorenal protection [1,2,3,4]. The renoprotective effects of BNP include the inhibition of sodium reabsorption in the proximal tubule and the distal nephron, and the improvement of the glomerular filtration rate (GFR) and renal plasma flow (RPF) with respect to vasodilatation by inhibiting multiple plasma vasoconstrictors [5,6,7]. Furthermore, BNP infusion inhibits the cardiac and renal sympathetic tones [8] and the renin-angiotensin-aldosterone system (RAAS) [9], in addition to decreasing the endothelin release [10]. NPs mediate their functions through interactions with specific surface receptors on target cells. At present, there are three distinct natriuretic peptide receptors (NPR) that have been reported and which include NPR-A, NPR-B, and NPR-C. NPR-A and NPR-B stimulate guanylyl cyclase, mediating their effect via the activation of the second messenger, cyclic guanosine monophosphate (cGMP). In the kidney, NPs cause a relaxation of mesangial cells, which increases GFR and reduces fractional sodium reabsorption in the renal tubules [7,11,12,13].
Congestive heart failure (CHF) is a complex syndrome characterized by sodium and water retention through the activation of different neurohormonal systems, such as the RAAS and the sympathetic nervous system (SNS), and also importantly, the NP system. Several experimental and clinical studies have implicated BNP in the pathophysiology of the unbalanced cardiorenal axis in CHF. In CHF patients, BNP plasma levels are in excess of 100 pg/mL [14]. Due to BNP’s longer half-life, it has been shown to have greater stability and offer a better understanding of the disease progression diagnostically as compared to atrial NP (ANP) in terms of improving cardiovascular function [15,16,17,18]. BNP plasma levels are also elevated in chronic kidney disease (CKD) patients. Underlying causes include renal dysfunction, diminished neprilysin (NEP) activity in the kidney and associated cardiovascular pathophysiology. Previous studies reported finding markedly high plasma BNP levels in patients with renal impairments [19,20,21].
Growing evidence suggests that in CHF, coronary artery disease and/or left ventricular hypertrophy etc., are increasingly associated with CKD patients. More recently, the cardiorenal syndrome (CRS), which is a complex pathophysiological condition that involves an association between acute heart failure (AHF) or CHF and renal impairment, has received much more attention. However, this condition is more than just a simultaneous cardiac and renal disease [22]. A recent French prospective study on 507 AHF patients demonstrated that BNP and the BNP prohormone were higher in AHF patients with renal dysfunction (CRS patients) as compared to those with normal renal function [23].
BNP acts as a compensating agent in the early stages of disease progression by inducing natriuresis and dieresis, and reducing RAAS and SNS. Similar to that seen with severe disease states like HF or CRS and despite high levels, endogenous BNP becomes resistant and is no longer able to compensate for volume overload in such cases. Thus, the supportive role of BNP in counteracting the unwanted effects of activated RAAS and SNS in these diseases provides the rationale for using this peptide as a potential therapeutic agent [13,24]. As it has been reported that the renal medulla expresses depressor substances, an extract of the papillary tips from kidneys might be able to induce the expression and secretion of endogenous BNP from cardiomyocytes [25]. A better understanding of these processes could potentially accelerate pharmacological treatments for CRS. Here, we review the functions and the roles of BNP in the heart-kidney interaction. In addition, we discuss the relevant molecular mechanisms for the protective effect of BNP against CKD and HF, especially in terms of the counterparts of the RAA system.
2. Biochemical Characteristics of BNP
Human BNP mRNA is translated to preproBNP of 134 amino acids, from which proBNP of 108 amino acids is processed and cleaved by the serine proteases corin and/or furin, yielding a biological inactive amino-terminal fragment, 76-amino acid proBNP (NT-proBNP) and an active carboxy-terminal fragment, 32-amino acid BNP [6,26]. It has been considered that, after maturation, both NT-proBNP and BNP are secreted at a 1:1 molar ratio from the heart. However, recent studies have shown that a certain amount of proBNP is also secreted without its cleavage from the heart [27]. Therefore, we should take into consideration the possibility that the increase in NT-proBNP is partly due to the elevation of proBNP when we see patients with an elevation of NT-proBNP. In contrast, BNP is increased without additional cardiac stress in patients treated with angiotensin-receptor/Neprilysin inhibitor (ARNi) due to its inhibitory effects of BNP degradation. In this review, we will not discuss them in detail here. Both NT-proBNP and BNP are equally useful in the differential diagnosis of heart failure [28,29], although the NT-proBNP and BNP assay allows for complementary information during ARNi treatments [30]. The gene structure and the post-translational processing of BNP and the diversity of circulating BNP-related peptides have been reviewed in detail [2,6,31].
3. The Function of BNP in Kidneys
It has been well established that BNP plays important roles in the kidneys, and provides multiple beneficial effects involving renal function [3]. Abnormalities or alterations of this system may contribute to renal impairment including tubular damage as a consequence of other CV disorders [32]. On the other hand, BNP plasma levels are affected by renal function, although the mechanism remains unclear. Thus, during renal failure, these are not considered to be an ideal choice as hemodynamic biomarkers [33,34]. The elevated levels of BNP may be the result of an increased cardiac release in CKD patients. In CKD patients, the increase in circulatory blood volume, the elevation in BP due to volume overload and arterial stiffness, and the cardiac hypertrophy and HF etc., can contribute to the elevation in BNP. The elevation of BNP in CKD patients is partly due to the impaired clearance of BNP from the kidneys.
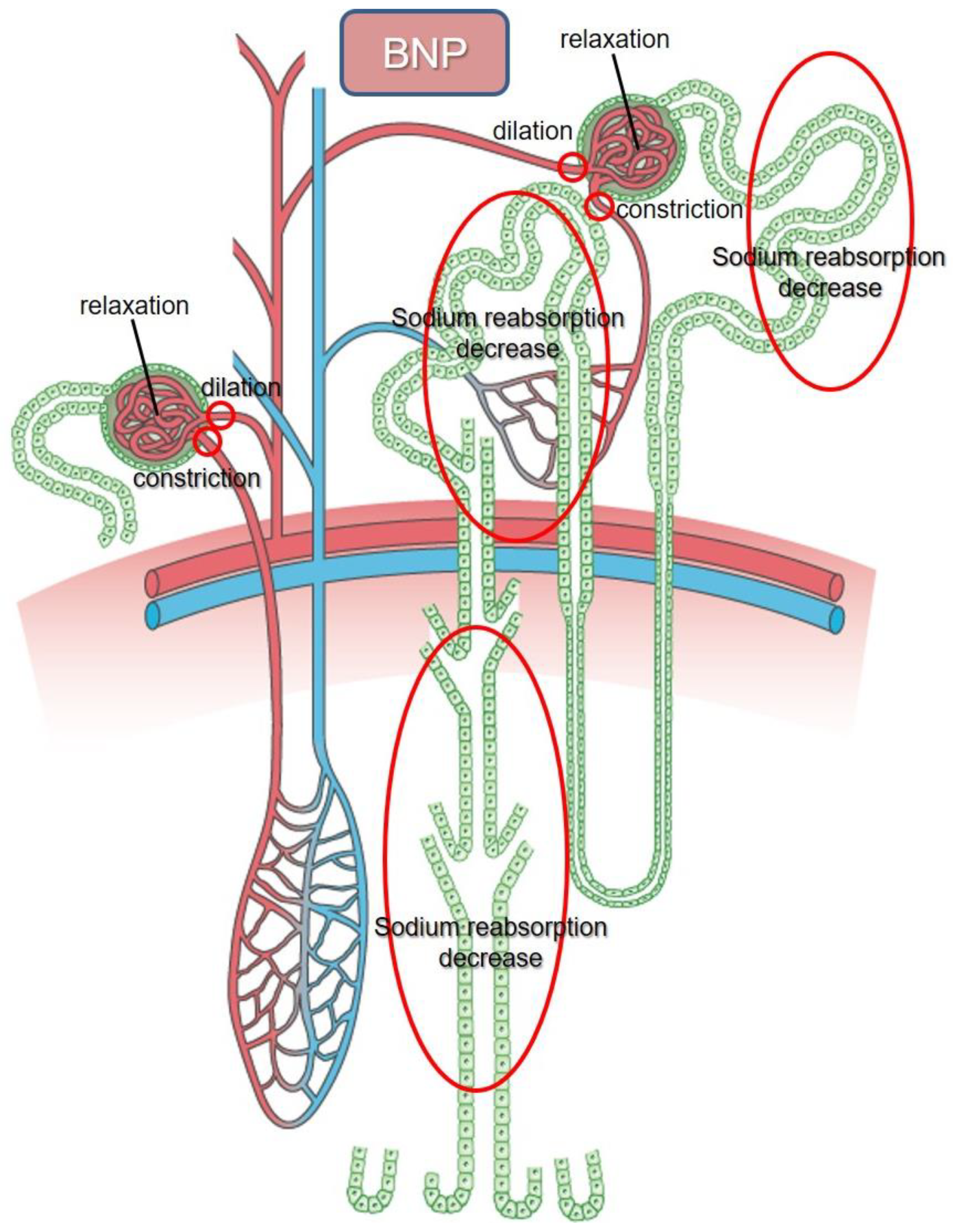
The functions of NPs are mediated by their interactions with specific surface receptors on the target cells. In the kidney, BNP increases GFR by relaxing the mesangial cells and inhibits the tubular fractional reabsorption of sodium [7,35] (Figure 1). BNP also decreases vascular resistance by relaxing vascular smooth muscle cells, while it has no effect on vascular permeability, unlike ANP.
Table 1 shows a sequence of pioneer studies that examined the injection of BNP in humans [5,9,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52]. Among them, Jensen et al. performed a well-organized study of BNP infusion in healthy men in 1998 [35]. The maximum concentration in the plasma that was reached was 199 pmol/L (688.6 pg/mL) after a dose of 4 pmol/kg/min for 60 min. The authors observed that there was an increase in the urinary flow rate and GFR (about +60% and +5% respectively) and that there was inhibition of the renin secretion (−24%). In addition, the fractional excretion of sodium was increased (+140%). The fractional reabsorption of sodium was decreased under the infusion (30 to 60 min after the start of infusion). The measurement of the clearance using lithium, which is assumed to only be reabsorbed in the proximal tubule and to the same degree as sodium and water, demonstrated that the tubular site of action occurred both in the proximal tubules (−7%) and distal nephron (−5%). There were no changes in the blood pressure, heart rate and aldosterone concentration. There was a decrease in the ANF concentration (−16%). These results suggest that the infusion of BNP within the physiological range, which can be observed in patients with HF, induces an increase in the GFR and the inhibition of sodium excretion, which leads to an increase in both the urine volume and the sodium excretion without affecting the blood pressure and heart rate in healthy subjects. These results are similar to other studies in terms of urination and sodium excretion irrespective of the minor differences in the protocol and the results (Table 1). Sodium reabsorption appears to decrease in the distal nephron earlier than that observed in the proximal tubule [41]. Interestingly, a trial of BNP infusion (2 pmol/kg/min for 60 min) in patients with heart failure and reduced ejection fraction (HFrEF) due to previous myocardial infarction or dilated cardiomyopathy showed that the impaired natriuretic response due to the reduced responsiveness in the distal nephron in patients with HFrEF was comparable to that found in healthy control subjects [5] and the results reported in another previous study [41]. This finding may be of interest, as this is in line with another previous report that found that a reduced reabsorption of sodium occurs in the distal nephron earlier than in the proximal tubules in patients with mild CKD [53]. In the distal nephron, the inner medullary collecting duct is the most prominent target of ANP [13]. It has been reported that BNP is colocalized with ANP in the distal tubules, while CNP is observed in the proximal tubules in human kidneys [54]. Thus, the adaptive recovery from impaired reabsorption of sodium in the distal nephron and feasibility for lowering the blood pressure suggest these can be therapeutic targets if we can determine the range of nesiritide in patients with CHF or/and CKD [55,56]. Moreover, as the NPRs are predominantly expressed in the distal part of the renal tubules [57], this can be another possible reason for their impaired natriuretic effect in advanced HF in which the proximal reabsorption of sodium is greatly enhanced [58]. In an experimental CHF model, BNP enhances the renal diuretic and natriuretic actions of loop diuretics while at the same time it also reduces the diuretic-induced aldosterone production [59].
BNP infusion may play an important role in preventing the development of CKD. McKie et al. recently examined BNP’s role in the pathophysiology of cardiorenal dysfunction and found that in asymptomatic systolic HF patients, chronic subcutaneous BNP therapy for 12 weeks improved renal function along with favourable hemodynamic effects in response to volume expansion [60]. A recent study also investigated the prophylactic effects of early BNP administration on contrast-induced nephropathy (CIN) in CKD patients undergoing elective percutaneous coronary intervention or coronary angiography [61]. BNP effectively decreased the incidence of CIN in patients with CKD, as was shown by the improved estimated GFR, cystatin C, and serum creatinine compared to the control group. In addition, the BNP group showed a faster recovery. Thus, exogenous BNP served as a prophylactic agent for attenuating the CIN incidence in CKD patients [61]. A retrospective study analyzed the effect of nesiritide on renal function and its clinical safety in 328 patients with decompensated HFpEF (dHFpEF) and concluded that nesiritide can be safely administered without negatively impacting the long-term renal function in these patients [56]. The GFR and creatinine remained stable at 1-month post-nesiritide infusion, whereas there was a significant deterioration of kidney function (GFR and creatinine) observed in the control subjects. In addition, their multivariate analysis showed that nesiritide was an important predictor of renal function at 1 month [56].
The vascular effects of NPs are site-specific [62]. Importantly, in the kidney’s vasculature, while NPs relax the afferent arterioles by acting as vasodilators, they act as vasoconstrictive agents on the efferent arterioles, thereby causing the GFR to be increased [63]. Therefore, since it is presumed that the renal blood flow may increase or decrease or even remain unchanged in response to exogenous NPs, it can be accompanied by a similar discrepant result regarding the renal plasma flow [13].
In CKD patients, impaired renal function restricts the use of NPs, as plasma BNP levels are elevated to ~200 pg/mL in CKD patients without HF. Whether these elevated BNP levels in CKD promote the activation of the NP system and have an effect on the target organ still remains unclear. Downregulation of NPR-A and upregulation of NPR-C expression in the renal medulla and renal cortex, respectively, may be responsible for the resistance of NPs including BNP in CKD, thereby resulting in its limited use in treating CKD patients with HF [64,65].
4. BNP Clearance from Kidneys
BNP clearance is associated with two major pathways. The first involves binding to the NPR-C receptor, while the second one is involved with the degradation by neprilysin (NEP), a zinc metallopeptidase. NPR-C, which is devoid of any guanylyl cyclase activity and coupled to the adenylyl cyclase inhibition [66], plays an important role as a clearance receptor for BNP in addition to ANP and CNP. In humans, it has been demonstrated that NPR-C mRNA is expressed in a variety of tissues such as the atria, kidney, lung, mesentery, placenta, adrenal, heart, cerebral cortex, cerebellum and aortic smooth muscle and endothelial cells [67,68]. ANP has been shown to be degraded mainly in the lung, liver and kidney. The binding ability of BNP with NPR-C in these organs is much weaker than ANP and CNP [69], which suggests a diminished removal of BNP by NPR-C-mediated internalization, and a long half-life due to the smaller amount of degradation. BNP is also degraded by a neutral endopeptidase known as NEP, which is mainly expressed at high levels at the luminal side of the renal proximal tubules in the kidneys [70] in addition to other tissues such as the heart, lungs, liver and vascular smooth muscle and endothelial cells. NEP extensively degrades BNP in the rat renal membrane in collaboration with a renal protease. In the human renal membrane, however, not all BNPs are degraded by NEP [71]. Moreover, the NEP mediated degradation of BNP is slower [72]. These results suggest that it is difficult to clear BNP from the kidneys in humans. Despite the fact that BNP degradation is mediated by both the NPR-C and NEP pathways, the precise role of each process with regard to the BNP concentrations remains undetermined [72]. In addition to NEP, BNP has also been reported to be degraded by dipeptidyl peptidase-4 and insulin-degrading enzyme [73,74]. In CHF patients, a marked decrease in urinary excretion of NPs was observed in conjunction with elevated plasma levels [75]. However, another report showed that there was an increase of NT-proBNP in fresh urine from HF patients [76].
5. BNP System vs. RAA System
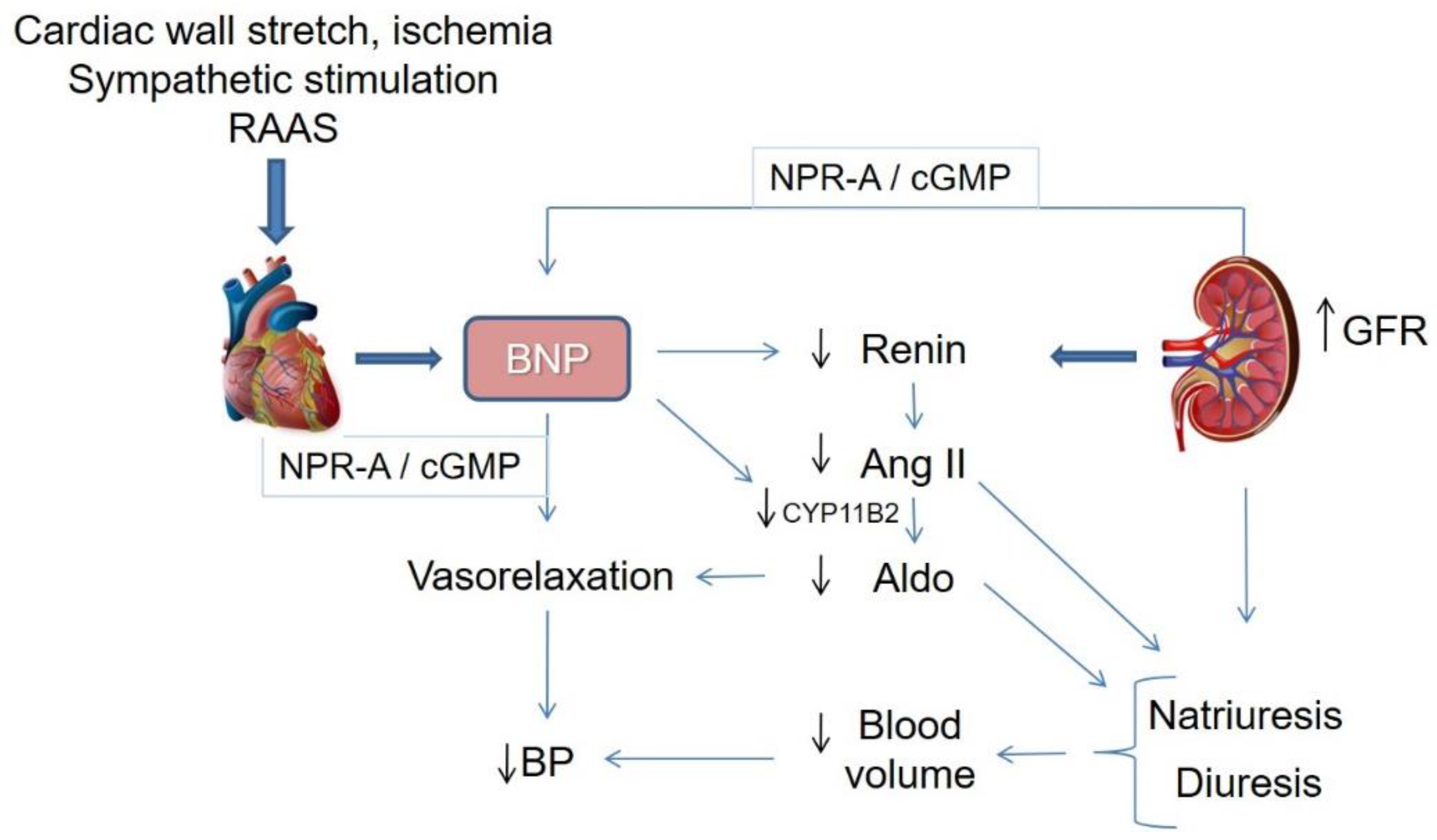
Sympathetic stimulation activates the RAAS, including the augmentation of angiotensin II (Ang II) and aldosterone production, as a result of the elevation of vasopressin and norepinephrine plasma levels, as well as the secretion of renin. SNS and RAAS augment the cardiac output by increasing heart rate, contractibility, preload and afterload at the expense of increased oxygen consumption [77]. Inhibiting the SNS through beta-blockers and antagonizing the RAAS through the angiotensin-converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs), and mineralocorticoid receptor antagonists, may be insufficient for certain neurohormonal abnormalities [78]. As a response to volume overload or cardiac stretching, secretion of BNP from the cardiac chambers manifests the heart as one of the endocrine organs in order to maintain the salt balance by interacting with the RAAS, SNS and the kidneys (Figure 2). Continual or excessive activation of the RAAS and SNS leads to the development of CHF. Furthermore, BNP is also activated in order to resist the actions attributed to the diuretic, natriuretic and vasorelaxant effects of BNP. As a result, this counterbalances the neurohormonal activation in CHF or hypertension leading to beneficial effects, such as natriuresis, vasodilation, and anti-cardiac remodelling (Figure 2) [79,80,81].
BNP has been shown to directly inhibit renin production from the kidney before affecting RBF or GFR [82], similar to ANP [83]. This result indicates that BNP directly inhibits the tubuloglomerular feedback response that is activated by salt over intake.
Experimental studies using rat cardiomyocytes reported that both endogenous and exogenous BNP reduced aldosterone synthase (CYP11B2) mRNA expression, which may lead to the inhibition of the RAAS and attenuation of cardiac hypertrophy and fibrosis [84]. Furthermore, in cultured primary human adrenocortical cells, it has been reported that BNP opposed the Ang II-stimulated biosynthesis of aldosterone due to decreased expression of both CYP11B2 and CYP11B1, which are the most important synthetic enzymes of aldosterone [85]. In contrast, BNP failed to directly inhibit the production of catecholamine and the synthesis of tyrosine hydroxylase, a dopamine synthetic enzyme, in rat adrenal pheochromocytoma cells [86]. Infusion of BNP induced a sympatho-inhibitory effect in normal subjects and inhibited renal sympathetic nervous activity in patients with CHF but not in healthy subjects [8]. However, the findings of another study that found that there were reductions in systemic and right-sided cardiac pressures in HF patients infused with BNP without any changes in the renin, aldosterone and norepinephrine plasma levels suggests that there is a RAAS or SNS independent direct vasorelaxant effect of BNP [47]. Both systems appear to influence each other, with BNP counteracting RAAS by inhibiting the renin secretion and CYP11B2 expression through cGMP, while the RAAS blockade, in turn, activates BNP. This suggests these may exert a synergistic effect in HF [87]. Thus, NP clearly interacts with the RAAS, and is inversely correlated with the plasma Ang II levels in certain physiologic conditions [88]. Furthermore, since the plasma levels of both hormonal systems are augmented in HF, this suggests that they counterbalance each other [89].
6. NPs Augmentation Combined with RAAS Blockade: Dual-Acting Angiotensin-Receptor/Neprilysin Inhibitors (ARNi)
Although BNP is progressively activated in HF, its response may often be insufficient to counteract the sodium retention and vascular constriction due to activation of RAAS and SNS. Therefore, more thorough approaches were undertaken both experimentally and clinically in an attempt to minimize the dysregulation of these neurohormonal systems. Ongoing strategies in promoting NP include synthesis or using agonists to increase its bioactivity and inhibition of NEP to reduce its catabolism [90,91]. Nesiritide, a recombinant BNP approved by the US Food and Drug Administration (FDA) in 2001, has been shown to promote clinical improvements in the management of CHF [92]. However, it has been reported to worsen renal function and increase the mortality rate in a meta-analysis [93]. Moreover, the severe hypotension and short half-life made these agents, including nesiritide, carperitide and ularitide, clinically imperfect. NEP inhibitors (NEPi) alone leads to activation of RAAS and attenuated Ang II degradation. Again the NEPi and ACE inhibitor combination predisposes a high risk of angioedema [94]. Therefore, the use of an ARB would be the optimal method of RAAS inhibition for use with NEPi. The first angiotensin receptor–neprilysin inhibitor (ARNI, LCZ696), developed by combining an ARB (Valsartan) with a NEPi (Sacubitril), was a major advance in the therapies for HF [95,96]. The combination of sacubitril and valsartan augments the beneficial effects of NPs and inhibits the harmful effects of Ang II. It preserves the ACE mechanism for bradykinin degradation and protects from angioedema formation [97]. Animal studies have shown that the NEPi and RAAS inhibitor combination reduced proteinuria and prevented kidney damage [98], also improved cardiac remodelling, fibrosis, and hypertrophy [99]. The recent UK HARP-III (United Kingdom Heart and Renal Protection-III), study on 414 CKD patients with an eGFR 20 to 60 mL/min/1.73 m2 has demonstrated that over 12 months, the combination of sacubitril and valsartan was well tolerated and had similar effects on kidney function and albuminuria compared to ARB irbesartan, with a BP and cardiac biomarker lowering effect, suggested that this combination could have the potential for reducing cardiovascular risk in CKD [100].
LCZ696 lowered BP more effectively than valsartan in hypertensive patients [101]. The PARAMOUNT (Prospective comparison of ARNI with ARB on Management Of heart failUre with preserved ejectioN fracTion, HFpEF) trial demonstrated that compared to valsartan, LCZ696 improved the overall clinical status and decreased atrial pressure and elevated GFR as well [102]. In HF patients with reduced ejection fraction (HFrEF), LCZ696 was reported to be more effective than enalapril in reducing hospitalization and cardiovascular and sudden death, preventing HF progression and improving renal function, as well as quality of life, in the Prospective comparison of ARNI with the ACE inhibitor to Determine Impact on Global Mortality and Morbidity in Heart Failure (PARADIGM-HF) trial [103,104,105,106]. Based on the myriads of favourable results of this trial, LCZ696 has been approved by the FDA in 2015 for treating HFrEF. ARNI has been shown in several studies including the PARADIGM-HF trial, to improve kidney function compared with RAAS inhibitor in HF [102,106,107]. Recently, an experimental study using a mouse myocardial infarction (MI) model and an in vitro mouse peritoneal macrophage, demonstrated that LCZ696 was associated with a better balance between the RAA and NP systems, and attenuated cardiac rupture following MI, suggesting that LCZ696 by its dual regulating mechanisms inhibited the inflammation and degradation response of macrophages and that early treatment with LCZ696 might have a cardioprotective effect after MI [108].
In spite of having numerous benefits of ARNi so far, however, some concerns raised that limits its clinical use, such as the elevation of bradykinin levels with ARB, the development of angioedema [109], and the chance of inducing Alzheimer disease by blocking the breakdown of amyloid-β [110]. Importantly, since sacubitril is predominantly excreted in the kidney in patients with renal impairment, it may accumulate and induce the development of hypotension particularly in patients with borderline BP [74].
7. Vasopressor and Vasodepressor Derived from Kidneys
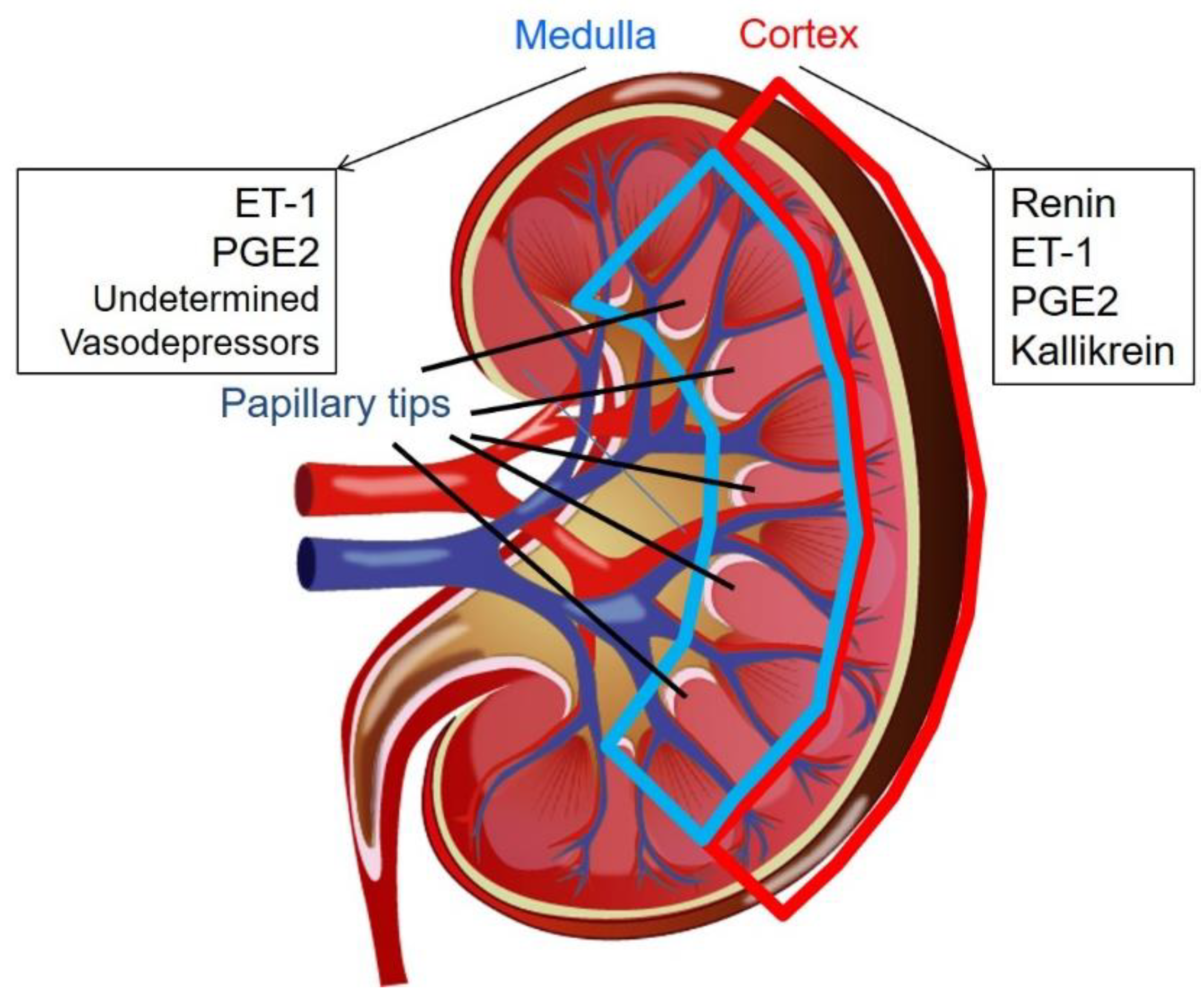
Kidneys play an important role in regulating blood pressure. In addition to volume control via urination with balanced water and electrolytes excretion, the kidneys possess several substances that are used to control blood pressure [111] (Figure 3). The most well-known substance is derived from the renal cortex. Tigerstedt and Bergman demonstrated that the injection of cortical extracts from rabbit kidneys caused a blood pressure elevation in the recipient rabbits, which led to the subsequent discovery of renin, a powerful vasopressor [112].
Endothelin-1 (ET-1), a 21 amino acid vasoconstrictor, is also produced by the endothelial cells, tubular cells and inner medullary collecting duct cells [113]. In physiological states, increased salt intake induces the tubular production of ET-1, which inhibits epithelial sodium channels and causes a reduced sodium reabsorption rate that leads to natriuresis. However, in pathophysiological states, ET-1 has been considered to be a vasopressor due to the development of glomerular and interstitial kidney and vascular diseases [114].
Prostaglandin (PG) is a lipid mediator involved in a variety of physiological and pathological processes in the kidneys [115]. PGE2 is the most abundant renal arachidonic acid metabolite. PGE2 is produced by the microsomal PGE synthase in the macula densa, distal convoluted tubule, collecting duct and renal medullary interstitial cells (RMIC) [116]. Although there are still conflicting conclusions, PGE2 is generally considered to be a vasodepressor due to its diuretic effect [117].
Tissue kallikrein is mainly expressed in the submandibular gland, pancreas and kidneys. Kallikreins are primarily produced in the distal convoluted tubule [118,119], the cortical collecting tubule [119,120], and possibly in the collecting tubule in the inner medulla [120]. Tissue kallikrein releases kinins from low and high molecular-weight kininogen. Kinins are inactivated kininases and the best-known kininase is the angiotensin-converting enzyme (ACE). In humans, tissue kallikrein releases Lys-bradykinin (kallidin). The kallikrein-kinin system increases the renal blood flow leading to more urination, water and sodium excretion [121] in collaboration with its direct effect on the distal nephron [122]. It has been reported that a reduced urinary kallikrein is associated with the development of hypertension [123,124,125]. Thus, kallikrein is considered to be a vasodepressor.
It has been reported by several independent groups that the renal medulla possesses a depressor substance that acts as a counterpart to RAAS [126,127]. This depressor agent is produced from RMICs. RMICs contain intracellular endocrine granules, which are reduced in size in proportion to blood pressure and renal blood flow [128]. Although the inclusions have not been correctly identified, electron microscopy studies have revealed that the contents consist of free fatty acids and PGs. However, the depressor substance does not seem to be a PG, nitric oxide or a platelet-activating factor [126,129]. The renal papillary RMICs have abundant granules when a kidney is clipped, and they have been shown to degranulate after unclipping in a one-kidney and one-clip hypertensive rat model [130]. It remains unknown whether the renal papillary tip contains the same substance the researchers have been trying to identify in the renal medulla, as most researchers did not distinguish between the papillary tip and the entire inner medulla.
8. Renal Papillary Tip May Contribute to the Expression of BNP in Cardiomyocytes
We recently developed a BNP reporter mouse carrying tdTomato under the mouse promoter of the 1136-bp fragment of the mouse NPPB gene from −1000 to +136 and demonstrated that this promoter was specifically activated in the papillary tips of the kidneys and was not accompanied by the BNP mRNA expression [25]. No evidence has been found that shows the existence of BNP isoforms or other nucleotide expressions apart from BNP and tdTomato. After the treatment with the extract from the renal papillary tip, both the expression and the secretion of BNP unexpectedly increased in the primary cultured neonatal cardiomyocytes. Although it is possible that artefacts due to contamination could occur, we found that there was no change in the expression of Ang II, ET-1, and type A, B and C NPs between the papillary tip and other portions of the kidneys. Even though its mechanism remains unknown, we initially evaluated elderly female mice as ageing and the female sex contribute to the expression of BNP in both normal subjects and patients with CHF [131,132,133,134]. However, we observed a similar activation of the BNP promoter in the papillary tips from young adults and/or male adult mice, although this was not recognized in neonatal mice [25].
The pBNP-tdTomato-positive cells were interstitial cells and were not proliferative. The papillary medulla has been reported to possess the ability to decrease blood pressure due to its vasodilatory activity [126,127]. To evaluate this activity of the papillary medulla from the kidneys, we injected an extract of the papillary tip intraperitoneally into stroke-prone spontaneously hypertensive rats (SHR-SPs). Intraperitoneal injection of the papillary extract reduced blood pressure from 210 mmHg to 165 mmHg and this was accompanied by an increase in serum BNP and urinary cGMP production in SHR-SP rats. Furthermore, the treatment with the papillary extract from rats with heart failure due to myocardial infarction significantly induced BNP expression in cardiomyocytes [25].
9. Conclusions
BNP plays an important role as a major player in the heart-kidney connection via its inhibitory effect on the RAAS, especially in the heart and the kidneys. Kidneys possess several substances involved in regulating the blood pressure in addition to volume control via urination. Furthermore, the papillary tips may play important roles in regulating the BNP expression from cardiomyocytes. Additional investigations will need to be undertaken in order to determine the relationship between the renal depressor system and BNP regulation, especially in terms of cardiovascular diseases, such as heart failure, hypertension and CKD.
Funding
This work is supported in part by Grants-in-Aid for Scientific Research from the Ministry of Education, Culture, Sports, Science and Technology, Japan (No. 19K08578 to R.O.) and the Okasan-Kato Foundation (to R.O.).
Acknowledgments
We thank Rie Ito and Miho Hisamura for their excellent technical assistance. The Department of Cardiology and Nephrology, Mie University Graduate School of Medicine, received research grants from Bristol-Myers Squibb, MSD K.K., Pfizer Japan Inc., Takeda Pharmaceutical Co., Ltd., Astellas Pharma Inc., Daiichi Sankyo Pharmaceutical Co., Ltd., Genzyme Japan, Shionogi & Co., Ltd., Sumitomo Dainippon Pharma Co., Ltd., Mitsubishi Tanabe Corporation, Otsuka Pharmaceutical Co., Ltd., Bayer Yakuhin, Ltd., AstraZeneca K.K., and Boehringer Ingelheim Co., Ltd. Masaaki Ito received lecture fees from Daiichi Sankyo Co. Pharmaceutical Co., Ltd., Mitsubishi Tanabe Corporation, Bayer Yakuhin, Ltd. and Takeda Pharmaceutical Co., Ltd.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| ANP | atrial natriuretic peptide |
| BNP | brain natriuretic peptide |
| cGMP | cyclic guanosine monophosphate |
| CHF | congestive heart failure |
| CKD | chronic kidney disease |
| CRS | cardiorenal syndrome |
| GFR | glomerular filtration rate |
| NP | natriuretic peptide |
| NPR | natriuretic peptide receptor |
| RAAS | renin-angiotensin-aldosterone system |
| RMIC | renal medullary interstitial cell |
| RPF | renal plasma flow |
| SNS | sympathetic nervous system |
References
- Sudoh, T.; Kangawa, K.; Minamino, N.; Matsuo, H. A new natriuretic peptide in porcine brain. Nature 1988, 332, 78–81. [Google Scholar] [CrossRef] [PubMed]
- LaPointe, M.C. Molecular regulation of the brain natriuretic peptide gene. Peptides 2005, 26, 944–956. [Google Scholar] [CrossRef] [PubMed]
- Volpe, M. Natriuretic peptides and cardio-renal disease. Int. J. Cardiol. 2014, 176, 630–639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabatine, M.S.; Morrow, D.A.; de Lemos, J.A.; Omland, T.; Desai, M.Y.; Tanasijevic, M.; Hall, C.; McCabe, C.H.; Braunwald, E. Acute changes in circulating natriuretic peptide levels in relation to myocardial ischemia. J. Am. Coll. Cardiol. 2004, 44, 1988–1995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, K.T.; Eiskjaer, H.; Carstens, J.; Pedersen, E.B. Renal effects of brain natriuretic peptide in patients with congestive heart failure. Clin. Sci. 1999, 96, 5–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishikimi, T.; Kuwahara, K.; Nakao, K. Current biochemistry, molecular biology, and clinical relevance of natriuretic peptides. J. Cardiol. 2011, 57, 131–140. [Google Scholar] [CrossRef] [Green Version]
- Levin, E.R.; Gardner, D.G.; Samson, W.K. Natriuretic peptides. N. Engl. J. Med. 1998, 339, 321–328. [Google Scholar]
- Brunner-La Rocca, H.P.; Kaye, D.M.; Woods, R.L.; Hastings, J.; Esler, M.D. Effects of intravenous brain natriuretic peptide on regional sympathetic activity in patients with chronic heart failure as compared with healthy control subjects. J. Am. Coll. Cardiol. 2001, 37, 1221–1227. [Google Scholar] [CrossRef] [Green Version]
- Holmes, S.J.; Espiner, E.A.; Richards, A.M.; Yandle, T.G.; Frampton, C. Renal, endocrine, and hemodynamic effects of human brain natriuretic peptide in normal man. J. Clin. Endocrinol. Metab. 1993, 76, 91–96. [Google Scholar]
- Kohno, M.; Yokokawa, K.; Horio, T.; Yasunari, K.; Murakawa, K.; Takeda, T. Atrial and brain natriuretic peptides inhibit the endothelin-1 secretory response to angiotensin II in porcine aorta. Circ. Res. 1992, 70, 241–247. [Google Scholar] [CrossRef]
- De Arriba, G.; Barrio, V.; Olivera, A.; Rodriguez-Puyol, D.; Lopez-Novoa, J.M. Atrial natriuretic peptide inhibits angiotensin II-induced contraction of isolated glomeruli and cultured glomerular mesangial cells of rats: The role of calcium. J. Lab. Clin. Med. 1988, 111, 466–474. [Google Scholar] [PubMed]
- Ballermann, B.J.; Hoover, R.L.; Karnovsky, M.J.; Brenner, B.M. Physiologic regulation of atrial natriuretic peptide receptors in rat renal glomeruli. J. Clin. Investig. 1985, 76, 2049–2056. [Google Scholar] [CrossRef] [PubMed]
- Houben, A.J.; van der Zander, K.; de Leeuw, P.W. Vascular and renal actions of brain natriuretic peptide in man: Physiology and pharmacology. Fundam. Clin. Pharmacol. 2005, 19, 411–419. [Google Scholar] [CrossRef] [PubMed]
- Doust, J.; Lehman, R.; Glasziou, P. The role of BNP testing in heart failure. Am. Fam. Physician 2006, 74, 1893–1898. [Google Scholar] [PubMed]
- Brenner, B.M.; Ballermann, B.J.; Gunning, M.E.; Zeidel, M.L. Diverse biological actions of atrial natriuretic peptide. Physiol. Rev. 1990, 70, 665–699. [Google Scholar] [CrossRef] [PubMed]
- Rademaker, M.T.; Richards, A.M. Cardiac natriuretic peptides for cardiac health. Clin. Sci. 2005, 108, 23–36. [Google Scholar] [CrossRef] [PubMed]
- Semenov, A.G.; Katrukha, A.G. Analytical Issues with Natriuretic Peptides—Has this been Overly Simplified? EJIFCC 2016, 27, 189–207. [Google Scholar]
- Kitakaze, M.; Asakura, M.; Kim, J.; Shintani, Y.; Asanuma, H.; Hamasaki, T.; Seguchi, O.; Myoishi, M.; Minamino, T.; Ohara, T.; et al. Human atrial natriuretic peptide and nicorandil as adjuncts to reperfusion treatment for acute myocardial infarction (J-WIND): Two randomised trials. Lancet 2007, 370, 1483–1493. [Google Scholar] [CrossRef]
- Spanaus, K.S.; Kronenberg, F.; Ritz, E.; Schlapbach, R.; Fliser, D.; Hersberger, M.; Kollerits, B.; Konig, P.; von Eckardstein, A. B-type natriuretic peptide concentrations predict the progression of nondiabetic chronic kidney disease: The Mild-to-Moderate Kidney Disease Study. Clin. Chem. 2007, 53, 1264–1272. [Google Scholar] [CrossRef]
- Van Kimmenade, R.R.; Januzzi, J.L., Jr.; Bakker, J.A.; Houben, A.J.; Rennenberg, R.; Kroon, A.A.; Crijns, H.J.; van Dieijen-Visser, M.P.; de Leeuw, P.W.; Pinto, Y.M. Renal clearance of B-type natriuretic peptide and amino terminal pro-B-type natriuretic peptide a mechanistic study in hypertensive subjects. J. Am. Coll. Cardiol. 2009, 53, 884–890. [Google Scholar] [CrossRef]
- Takase, H.; Dohi, Y. Kidney function crucially affects B-type natriuretic peptide (BNP), N-terminal proBNP and their relationship. Eur. J. Clin. Investig. 2014, 44, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Niizuma, S.; Iwanaga, Y.; Yahata, T.; Miyazaki, S. Renocardiovascular Biomarkers: From the Perspective of Managing Chronic Kidney Disease and Cardiovascular Disease. Front. Cardiovasc. Med. 2017, 4, 10. [Google Scholar] [CrossRef] [PubMed]
- Dos Reis, D.; Fraticelli, L.; Bassand, A.; Manzo-Silberman, S.; Peschanski, N.; Charpentier, S.; Elbaz, M.; Savary, D.; Bonnefoy-Cudraz, E.; Laribi, S.; et al. Impact of renal dysfunction on the management and outcome of acute heart failure: Results from the French prospective, multicentre, DeFSSICA survey. BMJ Open 2019, 9, e022776. [Google Scholar] [CrossRef] [PubMed]
- Volpe, M.; Carnovali, M.; Mastromarino, V. The natriuretic peptides system in the pathophysiology of heart failure: From molecular basis to treatment. Clin. Sci. 2016, 130, 57–77. [Google Scholar] [CrossRef] [PubMed]
- Goto, I.; Okamoto, R.; Hashizume, R.; Suzuki, N.; Ito, R.; Yamanaka, K.; Saito, H.; Kiyonari, H.; Tawara, I.; Kageyama, Y.; et al. Renal papillary tip extract stimulates BNP production and excretion from cardiomyocytes. PLoS ONE 2018, 13, e0197078. [Google Scholar] [CrossRef] [PubMed]
- Clerico, A.; Passino, C.; Franzini, M.; Emdin, M. Cardiac biomarker testing in the clinical laboratory: Where do we stand? General overview of the methodology with special emphasis on natriuretic peptides. Clin. Chim. Acta 2015, 443, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Waldo, S.W.; Beede, J.; Isakson, S.; Villard-Saussine, S.; Fareh, J.; Clopton, P.; Fitzgerald, R.L.; Maisel, A.S. Pro-B-type natriuretic peptide levels in acute decompensated heart failure. J. Am. Coll. Cardiol. 2008, 51, 1874–1882. [Google Scholar] [CrossRef]
- Santaguida, P.L.; Don-Wauchope, A.C.; Oremus, M.; McKelvie, R.; Ali, U.; Hill, S.A.; Balion, C.; Booth, R.A.; Brown, J.A.; Bustamam, A.; et al. BNP and NT-proBNP as prognostic markers in persons with acute decompensated heart failure: A systematic review. Heart Fail. Rev. 2014, 19, 453–470. [Google Scholar] [CrossRef]
- Mueller, T.; Gegenhuber, A.; Poelz, W.; Haltmayer, M. Head-to-head comparison of the diagnostic utility of BNP and NT-proBNP in symptomatic and asymptomatic structural heart disease. Clin. Chim. Acta 2004, 341, 41–48. [Google Scholar] [CrossRef]
- Clerico, A.; Zaninotto, M.; Passino, C.; Plebani, M. New issues on measurement of B-type natriuretic peptides. Clin. Chem. Lab. Med. 2017, 56, 32–39. [Google Scholar] [CrossRef] [Green Version]
- Kuwahara, K.; Nakagawa, Y.; Nishikimi, T. Cutting Edge of Brain Natriuretic Peptide (BNP) Research- The Diversity of BNP Immunoreactivity and Its Clinical Relevance. Circ. J. 2018, 82, 2455–2461. [Google Scholar] [CrossRef] [PubMed]
- Rubattu, S.; Forte, M.; Marchitti, S.; Volpe, M. Molecular Implications of Natriuretic Peptides in the Protection from Hypertension and Target Organ Damage Development. Int. J. Mol. Sci. 2019, 20, 798. [Google Scholar] [CrossRef] [PubMed]
- Santos-Araujo, C.; Leite-Moreira, A.; Pestana, M. Clinical value of natriuretic peptides in chronic kidney disease. Nefrologia 2015, 35, 227–233. [Google Scholar] [CrossRef] [Green Version]
- Vanderheyden, M.; Bartunek, J.; Filippatos, G.; Goethals, M.; Vlem, B.V.; Maisel, A. Cardiovascular disease in patients with chronic renal impairment: Role of natriuretic peptides. Congest. Heart Fail. 2008, 14, 38–42. [Google Scholar] [CrossRef]
- Jensen, K.T.; Carstens, J.; Pedersen, E.B. Effect of BNP on renal hemodynamics, tubular function and vasoactive hormones in humans. Am. J. Physiol. 1998, 274, F63–F72. [Google Scholar] [CrossRef] [PubMed]
- McGregor, A.; Richards, M.; Espiner, E.; Yandle, T.; Ikram, H. Brain natriuretic peptide administered to man: Actions and metabolism. J. Clin. Endocrinol. Metab. 1990, 70, 1103–1107. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, M.; Yasue, H.; Morita, E.; Sakaino, N.; Jougasaki, M.; Kurose, M.; Mukoyama, M.; Saito, Y.; Nakao, K.; Imura, H. Hemodynamic, renal, and hormonal responses to brain natriuretic peptide infusion in patients with congestive heart failure. Circulation 1991, 84, 1581–1588. [Google Scholar] [CrossRef]
- Cheung, B.M.; Dickerson, J.E.; Ashby, M.J.; Brown, M.J.; Brown, J. Effects of physiological increments in human alpha-atrial natriuretic peptide and human brain natriuretic peptide in normal male subjects. Clin. Sci. 1994, 86, 723–730. [Google Scholar] [CrossRef]
- Florkowski, C.M.; Richards, A.M.; Espiner, E.A.; Yandle, T.G.; Frampton, C. Renal, endocrine, and hemodynamic interactions of atrial and brain natriuretic peptides in normal men. Am. J. Physiol. 1994, 266, R1244–R1250. [Google Scholar] [CrossRef]
- La Villa, G.; Fronzaroli, C.; Lazzeri, C.; Porciani, C.; Bandinelli, R.; Vena, S.; Messeri, G.; Franchi, F. Cardiovascular and renal effects of low dose brain natriuretic peptide infusion in man. J. Clin. Endocrinol. Metab. 1994, 78, 1166–1171. [Google Scholar]
- La Villa, G.; Stefani, L.; Lazzeri, C.; Zurli, C.; Guerra, C.T.; Barletta, G.; Bandinelli, R.; Strazzulla, G.; Franchi, F. Acute effects of physiological increments of brain natriuretic peptide in humans. Hypertension 1995, 26, 628–633. [Google Scholar] [CrossRef] [PubMed]
- Lazzeri, C.; La Villa, G.; Bisi, G.; Boddi, V.; Messeri, G.; Strazzulla, G.; Franchi, F. Cardiovascular function during brain natriuretic peptide infusion in man. Cardiology 1995, 86, 396–401. [Google Scholar] [CrossRef] [PubMed]
- Hunt, P.J.; Espiner, E.A.; Nicholls, M.G.; Richards, A.M.; Yandle, T.G. Differing biological effects of equimolar atrial and brain natriuretic peptide infusions in normal man. J. Clin. Endocrinol. Metab. 1996, 81, 3871–3876. [Google Scholar] [PubMed]
- Yasue, H.; Yoshimura, M. Natriuretic peptides in the treatment of heart failure. J. Card. Fail. 1996, 2, S277–S285. [Google Scholar] [CrossRef]
- Van der Zander, K.; Houben, A.J.; Hofstra, L.; Kroon, A.A.; de Leeuw, P.W. Hemodynamic and renal effects of low-dose brain natriuretic peptide infusion in humans: A randomized, placebo-controlled crossover study. Am. J. Physiol. Heart Circ. Physiol. 2003, 285, H1206–H1212. [Google Scholar] [CrossRef] [PubMed]
- Marcus, L.S.; Hart, D.; Packer, M.; Yushak, M.; Medina, N.; Danziger, R.S.; Heitjan, D.F.; Katz, S.D. Hemodynamic and renal excretory effects of human brain natriuretic peptide infusion in patients with congestive heart failure. A double-blind, placebo-controlled, randomized crossover trial. Circulation 1996, 94, 3184–3189. [Google Scholar] [CrossRef] [PubMed]
- Lainchbury, J.G.; Richards, A.M.; Nicholls, M.G.; Hunt, P.J.; Ikram, H.; Espiner, E.A.; Yandle, T.G.; Begg, E. The effects of pathophysiological increments in brain natriuretic peptide in left ventricular systolic dysfunction. Hypertension 1997, 30, 398–404. [Google Scholar] [CrossRef]
- Abraham, W.T.; Lowes, B.D.; Ferguson, D.A.; Odom, J.; Kim, J.K.; Robertson, A.D.; Bristow, M.R.; Schrier, R.W. Systemic hemodynamic, neurohormonal, and renal effects of a steady-state infusion of human brain natriuretic peptide in patients with hemodynamically decompensated heart failure. J. Card. Fail. 1998, 4, 37–44. [Google Scholar] [CrossRef]
- Wang, Y.; Gu, X.; Fan, W.; Fan, Y.; Li, W.; Fu, X. Effects of recombinant human brain natriuretic peptide on renal function in patients with acute heart failure following myocardial infarction. Am. J. Transl. Res. 2016, 8, 239–245. [Google Scholar]
- Richards, A.M.; Crozier, I.G.; Holmes, S.J.; Espiner, E.A.; Yandle, T.G.; Frampton, C. Brain natriuretic peptide: Natriuretic and endocrine effects in essential hypertension. J. Hypertens. 1993, 11, 163–170. [Google Scholar] [CrossRef]
- Lazzeri, C.; Franchi, F.; Porciani, C.; Fronzaroli, C.; Casini Raggi, V.; De Feo, M.L.; Mannelli, M.; Cersosimo, R.M.; La Villa, G. Systemic hemodynamics and renal function during brain natriuretic peptide infusion in patients with essential hypertension. Am. J. Hypertens. 1995, 8, 799–807. [Google Scholar] [CrossRef]
- Pidgeon, G.B.; Richards, A.M.; Nicholls, M.G.; Espiner, E.A.; Yandle, T.G.; Frampton, C. Differing metabolism and bioactivity of atrial and brain natriuretic peptides in essential hypertension. Hypertension 1996, 27, 906–913. [Google Scholar] [CrossRef] [PubMed]
- Kamper, A.L.; Holstein-Rathlou, N.H.; Leyssac, P.P.; Strandgaard, S. Lithium clearance in chronic nephropathy. Clin. Sci. 1989, 77, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Totsune, K.; Takahashi, K.; Murakami, O.; Satoh, F.; Sone, M.; Saito, T.; Sasano, H.; Mouri, T.; Abe, K. Natriuretic peptides in the human kidney. Hypertension 1994, 24, 758–762. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, S.S.; Stebbins, A.; Voors, A.A.; Hasselblad, V.; Ezekowitz, J.A.; Califf, R.M.; O’Connor, C.M.; Starling, R.C.; Hernandez, A.F. Effects of nesiritide and predictors of urine output in acute decompensated heart failure: Results from ASCEND-HF (acute study of clinical effectiveness of nesiritide and decompensated heart failure). J. Am. Coll. Cardiol. 2013, 62, 1177–1183. [Google Scholar] [CrossRef] [PubMed]
- Kelesidis, I.; Mazurek, J.; Khullar, P.; Saeed, W.; Vittorio, T.; Zolty, R. The effect of nesiritide on renal function and other clinical parameters in patients with decompensated heart failure and preserved ejection fraction. Congest. Heart Fail. 2012, 18, 158–164. [Google Scholar] [CrossRef] [PubMed]
- Fontoura, B.M.; Nussenzveig, D.R.; Pelton, K.M.; Maack, T. Atrial natriuretic factor receptors in cultured renomedullary interstitial cells. Am. J. Physiol. 1990, 258, C692–C699. [Google Scholar] [CrossRef] [PubMed]
- Verbrugge, F.H.; Dupont, M.; Steels, P.; Grieten, L.; Swennen, Q.; Tang, W.H.; Mullens, W. The kidney in congestive heart failure: ‘Are natriuresis, sodium, and diuretics really the good, the bad and the ugly?’. Eur. J. Heart Fail. 2014, 16, 133–142. [Google Scholar] [CrossRef]
- Cataliotti, A.; Boerrigter, G.; Costello-Boerrigter, L.C.; Schirger, J.A.; Tsuruda, T.; Heublein, D.M.; Chen, H.H.; Malatino, L.S.; Burnett, J.C., Jr. Brain natriuretic peptide enhances renal actions of furosemide and suppresses furosemide-induced aldosterone activation in experimental heart failure. Circulation 2004, 109, 1680–1685. [Google Scholar] [CrossRef]
- McKie, P.M.; Schirger, J.A.; Benike, S.L.; Harstad, L.K.; Slusser, J.P.; Hodge, D.O.; Redfield, M.M.; Burnett, J.C., Jr.; Chen, H.H. Chronic subcutaneous brain natriuretic peptide therapy in asymptomatic systolic heart failure. Eur. J. Heart Fail. 2016, 18, 433–441. [Google Scholar] [CrossRef]
- Liu, J.; Xie, Y.; He, F.; Gao, Z.; Hao, Y.; Zu, X.; Chang, L.; Li, Y. Recombinant Brain Natriuretic Peptide for the Prevention of Contrast-Induced Nephropathy in Patients with Chronic Kidney Disease Undergoing Nonemergent Percutaneous Coronary Intervention or Coronary Angiography: A Randomized Controlled Trial. Biomed Res. Int. 2016, 2016, 5985327. [Google Scholar] [CrossRef] [PubMed]
- Woods, R.L.; Jones, M.J. Atrial, B-type, and C-type natriuretic peptides cause mesenteric vasoconstriction in conscious dogs. Am. J. Physiol. 1999, 276, R1443–R1452. [Google Scholar] [CrossRef] [PubMed]
- Marin-Grez, M.; Fleming, J.T.; Steinhausen, M. Atrial natriuretic peptide causes pre-glomerular vasodilatation and post-glomerular vasoconstriction in rat kidney. Nature 1986, 324, 473–476. [Google Scholar] [CrossRef] [PubMed]
- Santos-Araujo, C.; Roncon-Albuquerque, R., Jr.; Moreira-Rodrigues, M.; Henriques-Coelho, T.; Quelhas-Santos, J.; Faria, B.; Sampaio-Maia, B.; Leite-Moreira, A.F.; Pestana, M. Local modulation of the natriuretic peptide system in the rat remnant kidney. Nephrol. Dial. Transplant. 2009, 24, 1774–1782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sackner-Bernstein, J.D.; Skopicki, H.A.; Aaronson, K.D. Risk of worsening renal function with nesiritide in patients with acutely decompensated heart failure. Circulation 2005, 111, 1487–1491. [Google Scholar] [CrossRef] [PubMed]
- Anand-Srivastava, M.B. Natriuretic peptide receptor-C signaling and regulation. Peptides 2005, 26, 1044–1059. [Google Scholar] [CrossRef] [PubMed]
- Porter, J.G.; Arfsten, A.; Fuller, F.; Miller, J.A.; Gregory, L.C.; Lewicki, J.A. Isolation and functional expression of the human atrial natriuretic peptide clearance receptor cDNA. Biochem. Biophys. Res. Commun. 1990, 171, 796–803. [Google Scholar] [CrossRef]
- Wilcox, J.N.; Augustine, A.; Goeddel, D.V.; Lowe, D.G. Differential regional expression of three natriuretic peptide receptor genes within primate tissues. Mol. Cell. Biol. 1991, 11, 3454–3462. [Google Scholar] [CrossRef]
- He, X.; Chow, D.; Martick, M.M.; Garcia, K.C. Allosteric activation of a spring-loaded natriuretic peptide receptor dimer by hormone. Science 2001, 293, 1657–1662. [Google Scholar] [CrossRef]
- Jalal, F.; Dehbi, M.; Berteloot, A.; Crine, P. Biosynthesis and polarized distribution of neutral endopeptidase in primary cultures of kidney proximal tubule cells. Biochem. J. 1994, 302, 669–674. [Google Scholar] [CrossRef] [Green Version]
- Dickey, D.M.; Potter, L.R. Human B-type natriuretic peptide is not degraded by meprin A. Biochem. Pharmacol. 2010, 80, 1007–1011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, M.W.; Espiner, E.A.; Yandle, T.G.; Charles, C.J.; Richards, A.M. Delayed metabolism of human brain natriuretic peptide reflects resistance to neutral endopeptidase. J. Endocrinol. 2000, 167, 239–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ralat, L.A.; Guo, Q.; Ren, M.; Funke, T.; Dickey, D.M.; Potter, L.R.; Tang, W.J. Insulin-degrading enzyme modulates the natriuretic peptide-mediated signaling response. J. Biol. Chem. 2011, 286, 4670–4679. [Google Scholar] [CrossRef] [PubMed]
- Fu, S.; Ping, P.; Wang, F.; Luo, L. Synthesis, secretion, function, metabolism and application of natriuretic peptides in heart failure. J. Biol. Eng. 2018, 12, 2. [Google Scholar] [CrossRef] [PubMed]
- Linssen, G.C.; Damman, K.; Hillege, H.L.; Navis, G.; van Veldhuisen, D.J.; Voors, A.A. Urinary N-terminal prohormone brain natriuretic peptide excretion in patients with chronic heart failure. Circulation 2009, 120, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Jungbauer, C.G.; Buchner, S.; Birner, C.; Resch, M.; Heinicke, N.; Debl, K.; Buesing, M.; Biermeier, D.; Schmitz, G.; Riegger, G.; et al. N-terminal pro-brain natriuretic peptide from fresh urine for the biochemical detection of heart failure and left ventricular dysfunction. Eur. J. Heart Fail. 2010, 12, 331–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, P.C.; Guo, J.; Zhang, A. The renal and cardiovascular effects of natriuretic peptides. Adv. Physiol. Educ. 2017, 41, 179–185. [Google Scholar] [CrossRef] [Green Version]
- Volpe, M.; Battistoni, A.; Mastromarino, V. Natriuretic peptides and volume handling in heart failure: The paradigm of a new treatment. Eur. J. Heart Fail. 2016, 18, 442–444. [Google Scholar] [CrossRef]
- Von Lueder, T.G.; Sangaralingham, S.J.; Wang, B.H.; Kompa, A.R.; Atar, D.; Burnett, J.C., Jr.; Krum, H. Renin-angiotensin blockade combined with natriuretic peptide system augmentation: Novel therapeutic concepts to combat heart failure. Circ. Heart Fail. 2013, 6, 594–605. [Google Scholar] [CrossRef]
- Corti, R.; Burnett, J.C., Jr.; Rouleau, J.L.; Ruschitzka, F.; Luscher, T.F. Vasopeptidase inhibitors: A new therapeutic concept in cardiovascular disease? Circulation 2001, 104, 1856–1862. [Google Scholar] [CrossRef]
- Tokudome, T.; Kishimoto, I.; Horio, T.; Arai, Y.; Schwenke, D.O.; Hino, J.; Okano, I.; Kawano, Y.; Kohno, M.; Miyazato, M.; et al. Regulator of G-protein signaling subtype 4 mediates antihypertrophic effect of locally secreted natriuretic peptides in the heart. Circulation 2008, 117, 2329–2339. [Google Scholar] [CrossRef] [PubMed]
- Akabane, S.; Matsushima, Y.; Matsuo, H.; Kawamura, M.; Imanishi, M.; Omae, T. Effects of brain natriuretic peptide on renin secretion in normal and hypertonic saline-infused kidney. Eur. J. Pharmacol. 1991, 198, 143–148. [Google Scholar] [CrossRef]
- Kurtz, A.; Della Bruna, R.; Pfeilschifter, J.; Taugner, R.; Bauer, C. Atrial natriuretic peptide inhibits renin release from juxtaglomerular cells by a cGMP-mediated process. Proc. Natl. Acad. Sci. USA 1986, 83, 4769–4773. [Google Scholar] [CrossRef] [PubMed]
- Ito, T.; Yoshimura, M.; Nakamura, S.; Nakayama, M.; Shimasaki, Y.; Harada, E.; Mizuno, Y.; Yamamuro, M.; Harada, M.; Saito, Y.; et al. Inhibitory effect of natriuretic peptides on aldosterone synthase gene expression in cultured neonatal rat cardiocytes. Circulation 2003, 107, 807–810. [Google Scholar] [CrossRef] [PubMed]
- Liang, F.; Kapoun, A.M.; Lam, A.; Damm, D.L.; Quan, D.; O’Connell, M.; Protter, A.A. B-Type natriuretic peptide inhibited angiotensin II-stimulated cholesterol biosynthesis, cholesterol transfer, and steroidogenesis in primary human adrenocortical cells. Endocrinology 2007, 148, 3722–3729. [Google Scholar] [CrossRef] [PubMed]
- Takekoshi, K.; Ishii, K.; Isobe, K.; Nomura, F.; Nammoku, T.; Nakai, T. Effects of natriuretic peptides (ANP, BNP, CNP) on catecholamine synthesis and TH mRNA levels in PC12 cells. Life Sci. 2000, 66, PL303–PL311. [Google Scholar] [CrossRef]
- Han, B.; Hasin, Y. Cardiovascular effects of natriuretic peptides and their interrelation with endothelin-1. Cardiovasc. Drugs Ther. 2003, 17, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Johnston, C.I.; Hodsman, P.G.; Kohzuki, M.; Casley, D.J.; Fabris, B.; Phillips, P.A. Interaction between atrial natriuretic peptide and the renin angiotensin aldosterone system. Endogenous antagonists. Am. J. Med. 1989, 87, 24S–28S. [Google Scholar] [PubMed]
- Rossi, F.; Mascolo, A.; Mollace, V. The pathophysiological role of natriuretic peptide-RAAS cross talk in heart failure. Int. J. Cardiol. 2017, 226, 121–125. [Google Scholar] [CrossRef] [PubMed]
- Filippatos, G.; Farmakis, D.; Parissis, J.; Lekakis, J. Drug therapy for patients with systolic heart failure after the PARADIGM-HF trial: In need of a new paradigm of LCZ696 implementation in clinical practice. BMC Med. 2015, 13, 35. [Google Scholar] [CrossRef] [PubMed]
- Bayes-Genis, A.; Barallat, J.; Galan, A.; de Antonio, M.; Domingo, M.; Zamora, E.; Urrutia, A.; Lupon, J. Soluble neprilysin is predictive of cardiovascular death and heart failure hospitalization in heart failure patients. J. Am. Coll. Cardiol. 2015, 65, 657–665. [Google Scholar] [CrossRef] [PubMed]
- Colucci, W.S.; Elkayam, U.; Horton, D.P.; Abraham, W.T.; Bourge, R.C.; Johnson, A.D.; Wagoner, L.E.; Givertz, M.M.; Liang, C.S.; Neibaur, M.; et al. Intravenous nesiritide, a natriuretic peptide, in the treatment of decompensated congestive heart failure. Nesiritide Study Group. N. Engl. J. Med. 2000, 343, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Partovian, C.; Li, S.X.; Xu, X.; Lin, H.; Strait, K.M.; Hwa, J.; Krumholz, H.M. Patterns of change in nesiritide use in patients with heart failure: How hospitals react to new information. JACC Heart Fail. 2013, 1, 318–324. [Google Scholar] [CrossRef]
- Kostis, J.B.; Packer, M.; Black, H.R.; Schmieder, R.; Henry, D.; Levy, E. Omapatrilat and enalapril in patients with hypertension: The Omapatrilat Cardiovascular Treatment vs. Enalapril (OCTAVE) trial. Am. J. Hypertens. 2004, 17, 103–111. [Google Scholar] [CrossRef] [PubMed]
- McCormack, P.L. Sacubitril/Valsartan: A Review in Chronic Heart Failure with Reduced Ejection Fraction. Drugs 2016, 76, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Volpe, M.; Rubattu, S.; Battistoni, A. ARNi: A Novel Approach to Counteract Cardiovascular Diseases. Int. J. Mol. Sci. 2019, 20, 2092. [Google Scholar] [CrossRef] [PubMed]
- Braunwald, E. The path to an angiotensin receptor antagonist-neprilysin inhibitor in the treatment of heart failure. J. Am. Coll. Cardiol. 2015, 65, 1029–1041. [Google Scholar] [CrossRef]
- Roksnoer, L.C.; van Veghel, R.; van Groningen, M.C.; de Vries, R.; Garrelds, I.M.; Bhaggoe, U.M.; van Gool, J.M.; Friesema, E.C.; Leijten, F.P.; Hoorn, E.J.; et al. Blood pressure-independent renoprotection in diabetic rats treated with AT1 receptor-neprilysin inhibition compared with AT1 receptor blockade alone. Clin. Sci. 2016, 130, 1209–1220. [Google Scholar] [CrossRef]
- Von Lueder, T.G.; Wang, B.H.; Kompa, A.R.; Huang, L.; Webb, R.; Jordaan, P.; Atar, D.; Krum, H. Angiotensin receptor neprilysin inhibitor LCZ696 attenuates cardiac remodeling and dysfunction after myocardial infarction by reducing cardiac fibrosis and hypertrophy. Circ. Heart Fail. 2015, 8, 71–78. [Google Scholar] [CrossRef]
- Haynes, R.; Judge, P.K.; Staplin, N.; Herrington, W.G.; Storey, B.C.; Bethel, A.; Bowman, L.; Brunskill, N.; Cockwell, P.; Hill, M.; et al. Effects of Sacubitril/Valsartan Versus Irbesartan in Patients With Chronic Kidney Disease. Circulation 2018, 138, 1505–1514. [Google Scholar] [CrossRef]
- Ruilope, L.M.; Dukat, A.; Bohm, M.; Lacourciere, Y.; Gong, J.; Lefkowitz, M.P. Blood-pressure reduction with LCZ696, a novel dual-acting inhibitor of the angiotensin II receptor and neprilysin: A randomised, double-blind, placebo-controlled, active comparator study. Lancet 2010, 375, 1255–1266. [Google Scholar] [CrossRef]
- Solomon, S.D.; Zile, M.; Pieske, B.; Voors, A.; Shah, A.; Kraigher-Krainer, E.; Shi, V.; Bransford, T.; Takeuchi, M.; Gong, J.; et al. The angiotensin receptor neprilysin inhibitor LCZ696 in heart failure with preserved ejection fraction: A phase 2 double-blind randomised controlled trial. Lancet 2012, 380, 1387–1395. [Google Scholar] [CrossRef]
- McMurray, J.J.; Packer, M.; Desai, A.S.; Gong, J.; Lefkowitz, M.P.; Rizkala, A.R.; Rouleau, J.L.; Shi, V.C.; Solomon, S.D.; Swedberg, K.; et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N. Engl. J. Med. 2014, 371, 993–1004. [Google Scholar] [CrossRef] [PubMed]
- Vardeny, O.; Miller, R.; Solomon, S.D. Combined neprilysin and renin-angiotensin system inhibition for the treatment of heart failure. JACC Heart Fail. 2014, 2, 663–670. [Google Scholar] [CrossRef] [PubMed]
- Desai, A.S.; McMurray, J.J.; Packer, M.; Swedberg, K.; Rouleau, J.L.; Chen, F.; Gong, J.; Rizkala, A.R.; Brahimi, A.; Claggett, B.; et al. Effect of the angiotensin-receptor-neprilysin inhibitor LCZ696 compared with enalapril on mode of death in heart failure patients. Eur. Heart J. 2015, 36, 1990–1997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Packer, M.; McMurray, J.J.; Desai, A.S.; Gong, J.; Lefkowitz, M.P.; Rizkala, A.R.; Rouleau, J.L.; Shi, V.C.; Solomon, S.D.; Swedberg, K.; et al. Angiotensin receptor neprilysin inhibition compared with enalapril on the risk of clinical progression in surviving patients with heart failure. Circulation 2015, 131, 54–61. [Google Scholar] [CrossRef]
- Voors, A.A.; Gori, M.; Liu, L.C.; Claggett, B.; Zile, M.R.; Pieske, B.; McMurray, J.J.; Packer, M.; Shi, V.; Lefkowitz, M.P.; et al. Renal effects of the angiotensin receptor neprilysin inhibitor LCZ696 in patients with heart failure and preserved ejection fraction. Eur. J. Heart Fail. 2015, 17, 510–517. [Google Scholar] [CrossRef] [Green Version]
- Ishii, M.; Kaikita, K.; Sato, K.; Sueta, D.; Fujisue, K.; Arima, Y.; Oimatsu, Y.; Mitsuse, T.; Onoue, Y.; Araki, S.; et al. Cardioprotective Effects of LCZ696 (Sacubitril/Valsartan) After Experimental Acute Myocardial Infarction. JACC Basic Transl. Sci. 2017, 2, 655–668. [Google Scholar] [CrossRef]
- Campbell, D.J.; Krum, H.; Esler, M.D. Losartan increases bradykinin levels in hypertensive humans. Circulation 2005, 111, 315–320. [Google Scholar] [CrossRef]
- Grimm, M.O.; Mett, J.; Stahlmann, C.P.; Haupenthal, V.J.; Zimmer, V.C.; Hartmann, T. Neprilysin and Abeta Clearance: Impact of the APP Intracellular Domain in NEP Regulation and Implications in Alzheimer’s Disease. Front. Aging Neurosci. 2013, 5, 98. [Google Scholar] [CrossRef]
- Kuwahara, M.; Marumo, F. Biosynthesis of hormones in renal tubular and interstitial cells. Nihon Rinsho 1995, 53, 1873–1878. [Google Scholar] [PubMed]
- Marks, L.S.; Maxwell, M.H. Tigerstedt and the discovery of renin. An historical note. Hypertension 1979, 1, 384–388. [Google Scholar] [CrossRef] [PubMed]
- De Miguel, C.; Speed, J.S.; Kasztan, M.; Gohar, E.Y.; Pollock, D.M. Endothelin-1 and the kidney: New perspectives and recent findings. Curr. Opin. Nephrol. Hypertens. 2016, 25, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Boesen, E.I. Endothelin receptors, renal effects and blood pressure. Curr. Opin. Pharmacol. 2015, 21, 25–34. [Google Scholar] [CrossRef]
- Nasrallah, R.; Hassouneh, R.; Hebert, R.L. PGE2, Kidney Disease, and Cardiovascular Risk: Beyond Hypertension and Diabetes. J. Am. Soc. Nephrol. 2016, 27, 666–676. [Google Scholar] [CrossRef]
- Li, Y.; Xia, W.; Zhao, F.; Wen, Z.; Zhang, A.; Huang, S.; Jia, Z.; Zhang, Y. Prostaglandins in the pathogenesis of kidney diseases. Oncotarget 2018, 9, 26586–26602. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Wei, Y.; Zheng, F.; Guan, Y.; Zhang, X. Prostaglandin E2 in the Regulation of Water Transport in Renal Collecting Ducts. Int. J. Mol. Sci. 2017, 18, 2539. [Google Scholar] [CrossRef]
- Tomita, K.; Endou, H.; Sakai, F. Localization of kallikrein-like activity along a single nephron in rabbits. Pflug. Arch. 1981, 389, 91–95. [Google Scholar] [CrossRef]
- Omata, K.; Carretero, O.A.; Scicli, A.G.; Jackson, B.A. Localization of active and inactive kallikrein (kininogenase activity) in the microdissected rabbit nephron. Kidney Int. 1982, 22, 602–607. [Google Scholar] [CrossRef] [Green Version]
- Proud, D.; Perkins, M.; Pierce, J.V.; Yates, K.N.; Highet, P.F.; Herring, P.L.; Mangkornkanok/Mark, M.; Bahu, R.; Carone, F.; Pisano, J.J. Characterization and localization of human renal kininogen. J. Biol. Chem. 1981, 256, 10634–10639. [Google Scholar]
- Rhaleb, N.E.; Yang, X.P.; Carretero, O.A. The kallikrein-kinin system as a regulator of cardiovascular and renal function. Compr. Physiol. 2011, 1, 971–993. [Google Scholar] [PubMed]
- Kauker, M.L. Bradykinin action on the efflux of luminal 22Na in the rat nephron. J. Pharmacol. Exp. Ther. 1980, 214, 119–123. [Google Scholar] [PubMed]
- Sinaiko, A.R.; Glasser, R.J.; Gillum, R.F.; Prineas, R.J. Urinary kallikrein excretion in grade school children with high and low blood pressure. J. Pediatr. 1982, 100, 938–940. [Google Scholar] [CrossRef]
- Sharma, J.N.; Narayanan, P. The kallikrein-kinin pathways in hypertension and diabetes. Prog. Drug Res. 2014, 69, 15–36. [Google Scholar] [PubMed]
- Wollheim, E.; Peterknecht, S.; Dees, C.; Wiener, A.; Wollheim, C.B. Defect in the excretion of a vasoactive polypeptide fraction A possible genetic marker of primary hypertension. Hypertension 1981, 3, 574–579. [Google Scholar] [CrossRef] [PubMed]
- Thomas, C.J.; Woods, R.L.; Evans, R.G.; Alcorn, D.; Christy, I.J.; Anderson, W.P. Evidence for a renomedullary vasodepressor hormone. Clin. Exp. Pharmacol. Physiol. 1996, 23, 777–785. [Google Scholar] [CrossRef] [PubMed]
- Muirhead, E.E. Renal vasodepressor mechanisms: The medullipin system. J. Hypertens. Suppl. 1993, 11, S53–S58. [Google Scholar] [CrossRef] [PubMed]
- Maric, C.; Harris, P.J.; Alcorn, D. Changes in mean arterial pressure predict degranulation of renomedullary interstitial cells. Clin. Exp. Pharmacol. Physiol. 2002, 29, 1055–1059. [Google Scholar] [CrossRef]
- Glodny, B.; Pauli, G.F. The vasodepressor function of the kidney: Prostaglandin E2 is not the principal vasodepressor lipid of the renal medulla. Acta Physiol. 2006, 187, 419–430. [Google Scholar] [CrossRef]
- Pitcock, J.A.; Brown, P.S.; Byers, W.; Brooks, B.; Muirhead, E.E. Degranulation of renomedullary interstitial cells during reversal of hypertension. Hypertension 1981, 3, II-75. [Google Scholar] [CrossRef]
- Wang, T.J.; Larson, M.G.; Levy, D.; Leip, E.P.; Benjamin, E.J.; Wilson, P.W.; Sutherland, P.; Omland, T.; Vasan, R.S. Impact of age and sex on plasma natriuretic peptide levels in healthy adults. Am. J. Cardiol. 2002, 90, 254–258. [Google Scholar] [CrossRef]
- Redfield, M.M.; Rodeheffer, R.J.; Jacobsen, S.J.; Mahoney, D.W.; Bailey, K.R.; Burnett, J.C., Jr. Plasma brain natriuretic peptide concentration: Impact of age and gender. J. Am. Coll. Cardiol. 2002, 40, 976–982. [Google Scholar] [CrossRef]
- Sayama, H.; Nakamura, Y.; Saito, N.; Kinoshita, M. Why is the concentration of plasma brain natriuretic peptide in elderly inpatients greater than normal? Coron. Artery Dis. 1999, 10, 537–540. [Google Scholar] [CrossRef] [PubMed]
- Sobhani, K.; Nieves Castro, D.K.; Fu, Q.; Gottlieb, R.A.; Van Eyk, J.E.; Merz, C.N.B. Sex differences in ischemic heart disease and heart failure biomarkers. Biol. Sex Differ. 2018, 9, 43. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The interaction site of BNP in the nephron. BNP: brain natriuretic peptide.

Figure 2.
BNP as a counterregulatory system of the renin angiotensin II aldosterone system (RAAS). Aldo, aldosterone; Ang II, angiotensin II; BP, blood pressure; BNP, brain natriuretic peptide; CYP11B2, cytochrome P450 family 11 subfamily B member 2 (aldosterone synthase); cGMP, cyclic guanosine monophosphate; GFR, glomerular filtration rate; NPR-A, natriuretic peptide receptor A.
Figure 2.
BNP as a counterregulatory system of the renin angiotensin II aldosterone system (RAAS). Aldo, aldosterone; Ang II, angiotensin II; BP, blood pressure; BNP, brain natriuretic peptide; CYP11B2, cytochrome P450 family 11 subfamily B member 2 (aldosterone synthase); cGMP, cyclic guanosine monophosphate; GFR, glomerular filtration rate; NPR-A, natriuretic peptide receptor A.

Figure 3.
The vasopressors and vasodepressors derived from the kidneys. ET-1, endothelin 1; PGE2, prostaglandin E2.
Figure 3.
The vasopressors and vasodepressors derived from the kidneys. ET-1, endothelin 1; PGE2, prostaglandin E2.


{kind=link}
{kind=link}
{kind=link}
Table 1.
The effects of brain natriuretic peptide (BNP) infusion on renal function, the renin angiotensin II aldosterone system and hemodynamics in normal subjects and patients with heart failure and hypertension.
Table 1.
The effects of brain natriuretic peptide (BNP) infusion on renal function, the renin angiotensin II aldosterone system and hemodynamics in normal subjects and patients with heart failure and hypertension.
| Study/Reference | Dosage of BNP pmol/kg/min | GFR | RPF | Urine Volume | Urine Na | Urine cGMP | Urine Aldo | Plasma cGMP | PRA | AngII | Plasma Aldo | MAP | HR | CO | SVR | PCWP |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Normal Subjects | ||||||||||||||||
| McGregor. J. Clin. Endocrinol. Metab. 1990 [36] | 2 | ↑↔ * | ↑ | ↓ | ↓ | ↔ | ↔ | |||||||||
| Yoshimura. Circulation. 1991 [37] | 30 | ↑ | ↑ | ↑ | ↔ | ↓ | ↓ | ↑ | ↑ | ↓ | ↓ | |||||
| Holmes. J. Clin. Endocrinol. Metab. 1993 [9] | 2 | ↔ | ↑ | ↑ | ↑ | ↓↔ * | ↓ | ↔ | ↑ | |||||||
| Cheung. Clin. Sci. 1994 [38] | 0.4 | ↔ | ↔ | ↑ | ↔ | ↔ | ||||||||||
| Florkowski. Am. J. Physiol. 1994 [39] | 2(+ANP(2)) ** | ↔ | ↑ | ↑ | ↑ | ↔ | ↔ | ↔ | ↓ | ↔ | ||||||
| La Villa. J. Clin. Endocrinol. Metab. 1994 [40] | 4 | ↑ | ↑ | ↑ | ↑ | ↑ | ↔ | ↔ | ↔ | ↔ | ↔ | ↔ | ||||
| La Villa. Hypertension. 1995 [41] | 0.25 and 0.5 | ↔ | ↔ | ↔ | ↑ | ↑ | ↓ | ↓ | ↔ | ↔ | ||||||
| Lazzeri. Cardiology. 1995 [42] | 4, 8, 10, 12 | ↑ | ↔ | ↔ | ↑ | ↔ | ↔ | |||||||||
| Hunt. J Clin. Endocrinol. Metab. 1996 [43] | 2 | ↔ | ↑ | ↑ | ↑ | ↓↔ * | ↓ | ↓ | ↔ | ↑ | ||||||
| Yasue. J Card. Fail. 1996 [44] | 30 | ↑ | ↑ | ↑ | ↑ | ↓ | ↑ | ↓ | ↓ | |||||||
| Jensen. Am. J. Phy.1998 [35] | 1, 2 and 4 | ↑ | ↓ | ↑ | ↑ | ↑ | ↑ | ↓ | ↔ | ↔ | ↔ | ↔ | ||||
| Jensen. Clin. Sci. 1999 [5] | 2 | ↑ | ↓ *** | ↔ | ↑ | ↑ | ↑ | ↓ | ↔ | ↔ | ↑ | ↔ | ||||
| van der Zander. Am. J. Physiol. 2003 [45] | 4 | ↑ | ↔ | ↑ | ↑ | ↑ | ↔ | ↔ | ↓↔ * | ↔ | ||||||
| Summarized | ↑ | ↔ | ↑ | ↑ | ↑ | ↑ | ↓↔ | ↔ | ↓ | ↔ | ↔ | ↔ | ↔ | ↓ | ||
| Patients with Heart Failure | ||||||||||||||||
| Yoshimura. Circulation. 1991 [37] | 30 | ↑ | ↑ | ↑ | ↔ | ↓ | ↓ | ↑ | ↑ | ↓ | ↓ | |||||
| Marcus. Circulation. 1996 [46] | 1 to 30 | ↔ | ↑ | ↑ | ↑ | ↓ | ↓ | ↑ | ↓ | ↓ | ||||||
| Yasue. J. Card. Fail. 1996 [44] | 30 | ↔ | ↑ | ↑ | ↑ | ↔ | ↔ | ↓ | ↓ | |||||||
| Lainchbury. HTN 1997 [47] | 3.3 | ↔ | ↔ | ↑ | ↔ | ↔ | ↓ | ↔ | ↔ | ↓ | ↓ | |||||
| Abraham. J. Cardiac. fail. 1998 [48] | 7.5, 15 | ↔ | ↔ | ↔ | ↔ | ↑ | ↔ | ↓ | ↓ | ↔ | ↑ | ↓ | ↓ | |||
| Jensen. Clin. Sci. 1999 [5] | 2 | ↔ | ↔ | ↔ | ↑ | ↑ | ↑ | ↓ | ↔ | ↔ | ↑ | ↔ | ||||
| Wang. Am. J. Trans. Res. 2016 [49] | A bolus followed by 2 to 6 for 72 h | ↓ | ↓ | |||||||||||||
| Summarized | ↔ | ↔ | ↑ | ↑ | ↑ | ↑ | ↔ | ↔ | ↓ | ↓ | ↔ | ↑ | ↓ | ↓ | ||
| Patients with Hypertension | ||||||||||||||||
| Richards. J. Hypertension. 1993 [50] | 2 | ↔ | ↑ | ↑ | ↔ | ↑ | ↔ # | ↓ | ↔ | ↔ | ||||||
| Lazzeri. Am. J. Hypertension. 1995 [51] | 4 | ↑ | ↑ | ↑ | ↑ | ↔ | ↔ | ↔ | ↔ | ↔ | ||||||
| Pidgeon. Hypertension. 1996 [52] | 2 | ↑ | ↑ | ↔ | ↑ | ↓ | ↓ | ↓ | ↑ | |||||||
| Summarized | ↑ | ↑ | ↑ | ↑ | ↔ | ↓ | ↔ | ↔ |
ANP, atrial natriuretic peptide; cGMP, cyclic guanosine monophosphate; CO, cardiac output; GFR, glomerular filtration rate; HR, heart rate; MAP, mean arterial pressure; PCWP, pulmonary capillary wedge pressure; PRA, plasma renin activity; RPF, renal plasma flow; SVR, systemic vascular resistance. * marginal significance. ** BNP(2)+ANP(2) vs ANP(2) alone. *** after the infusion. # Plasma renin concentration.
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Okamoto, R.; Ali, Y.; Hashizume, R.; Suzuki, N.; Ito, M. BNP as a Major Player in the Heart-Kidney Connection. Int. J. Mol. Sci. 2019, 20, 3581. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20143581
AMA Style
Okamoto R, Ali Y, Hashizume R, Suzuki N, Ito M. BNP as a Major Player in the Heart-Kidney Connection. International Journal of Molecular Sciences. 2019; 20(14):3581. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20143581
Chicago/Turabian StyleOkamoto, Ryuji, Yusuf Ali, Ryotaro Hashizume, Noboru Suzuki, and Masaaki Ito. 2019. "BNP as a Major Player in the Heart-Kidney Connection" International Journal of Molecular Sciences 20, no. 14: 3581. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20143581
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.