Infusing Mesenchymal Stromal Cells into Porcine Kidneys during Normothermic Machine Perfusion: Intact MSCs Can Be Traced and Localised to Glomeruli

 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
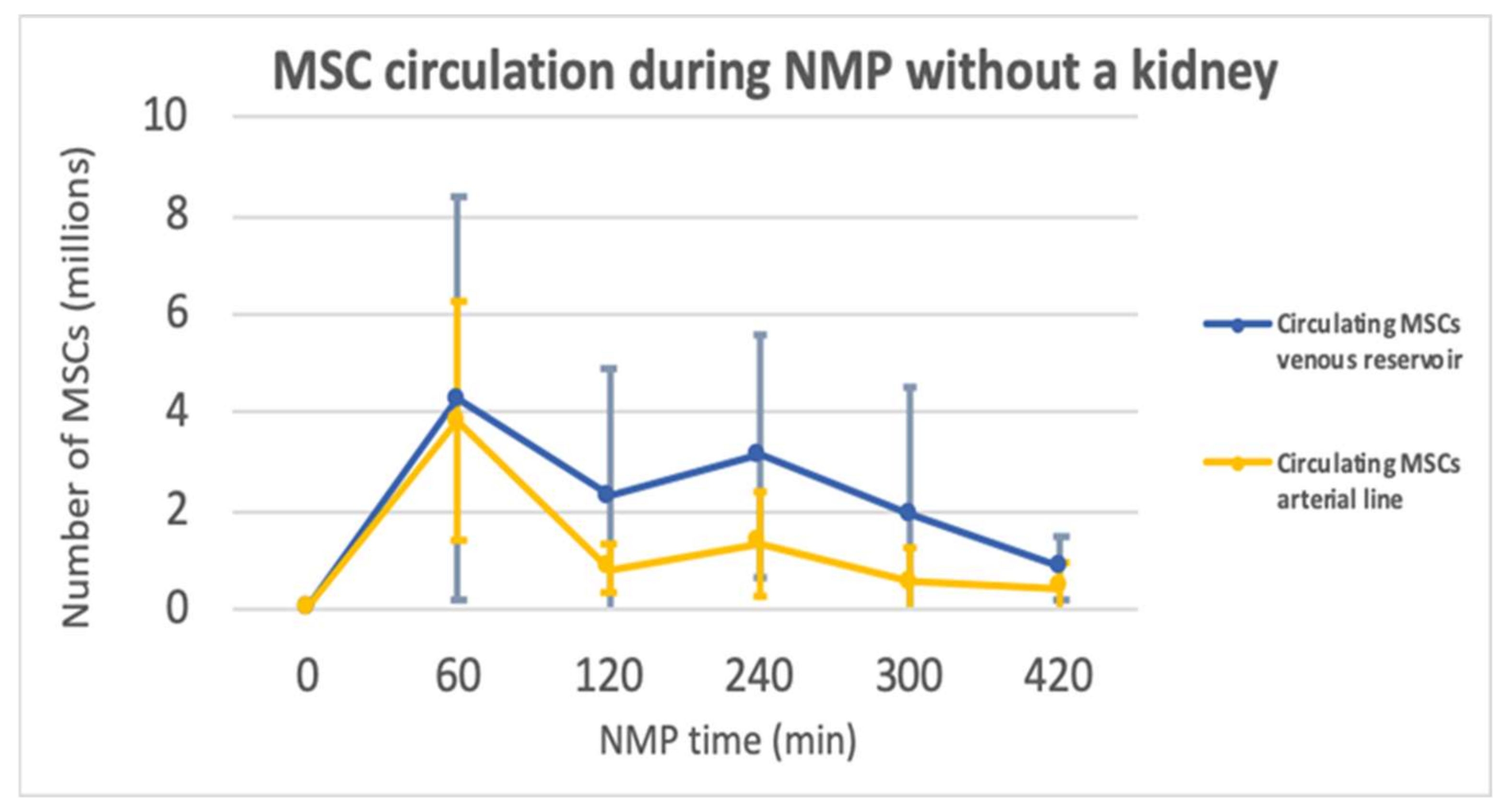
2.1. Normothermic Machine Perfusion
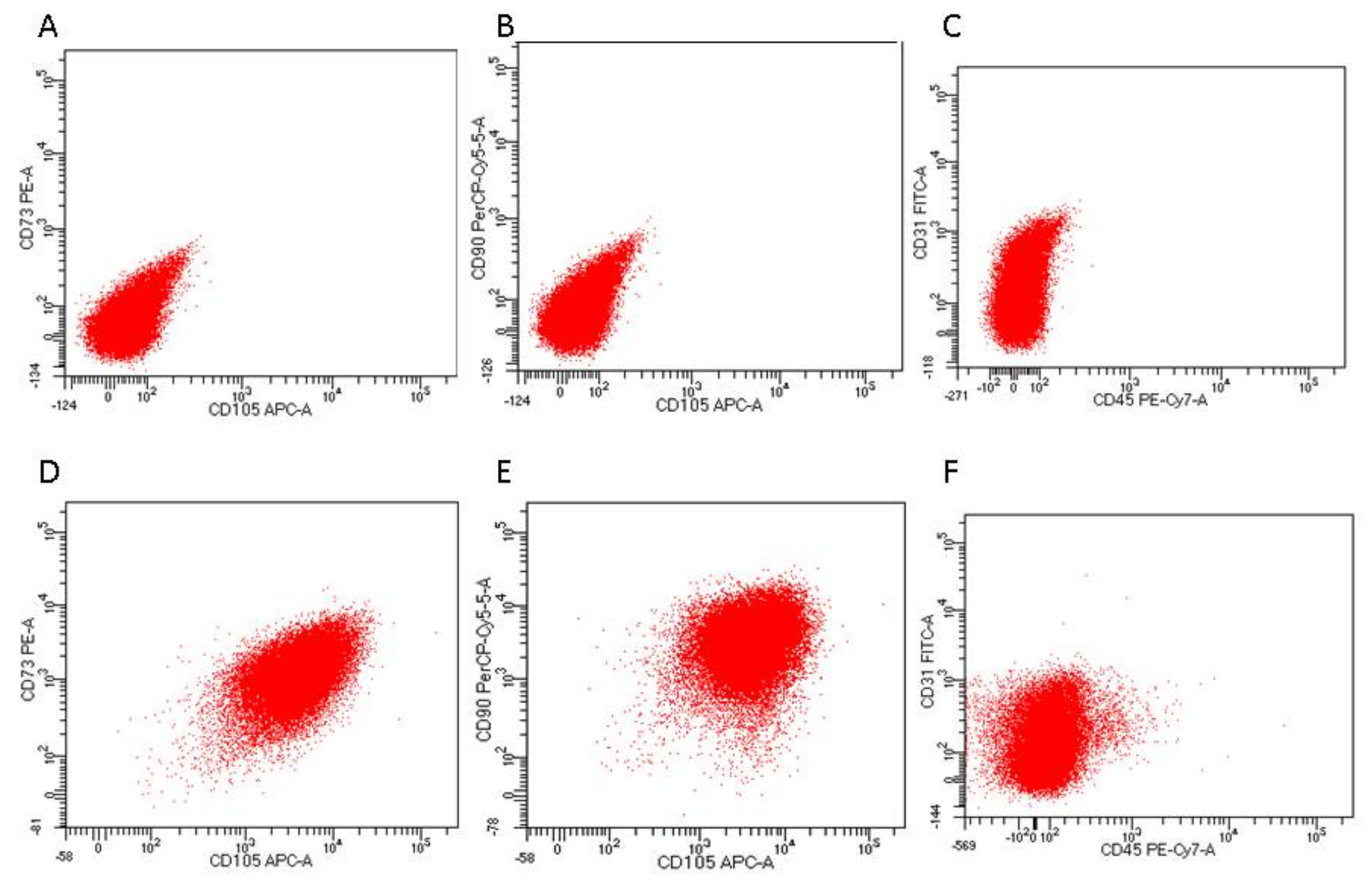
2.2. Characterisation of MSCs Using Fluorescence-Activated Cell Sorting (FACS)
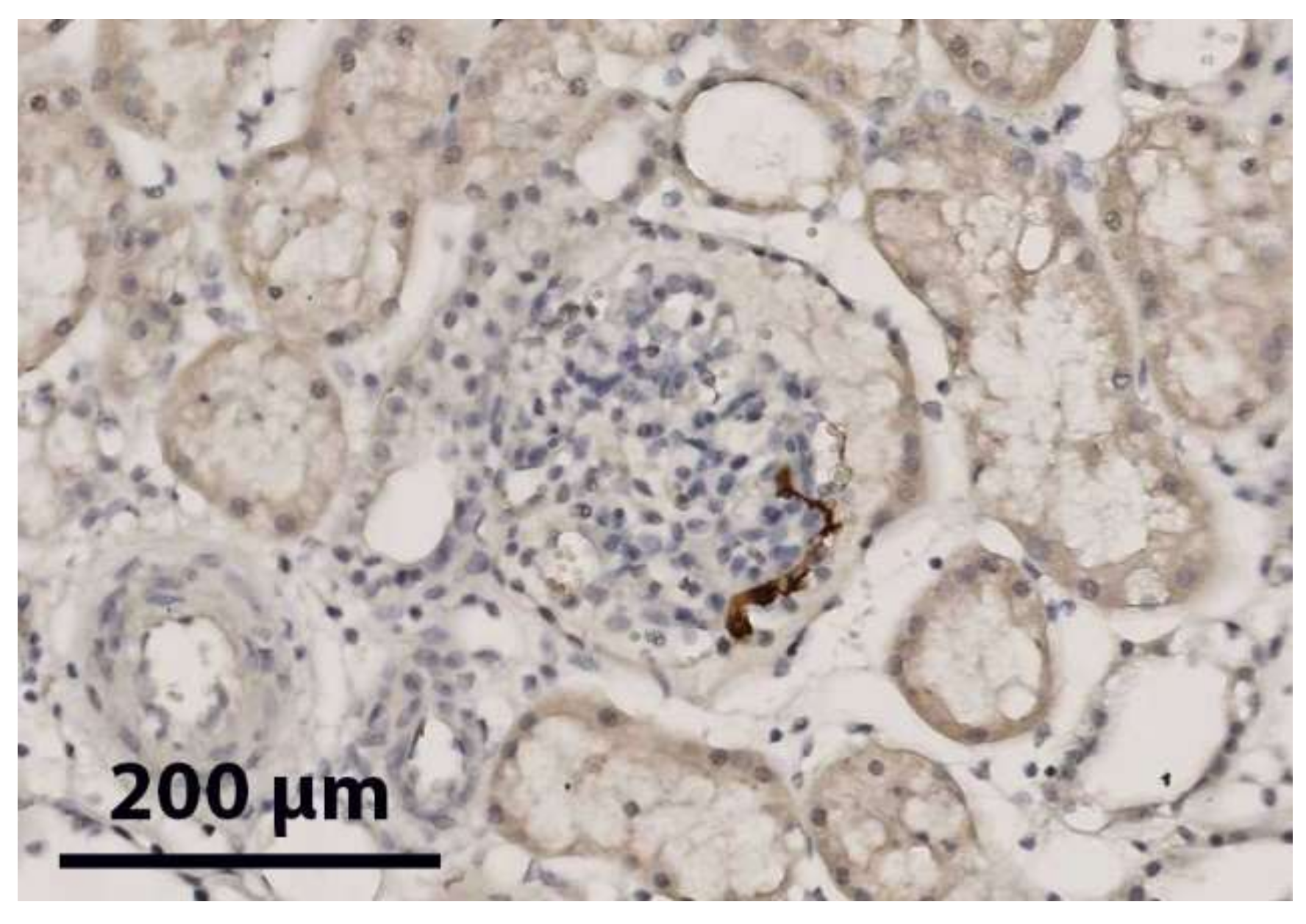
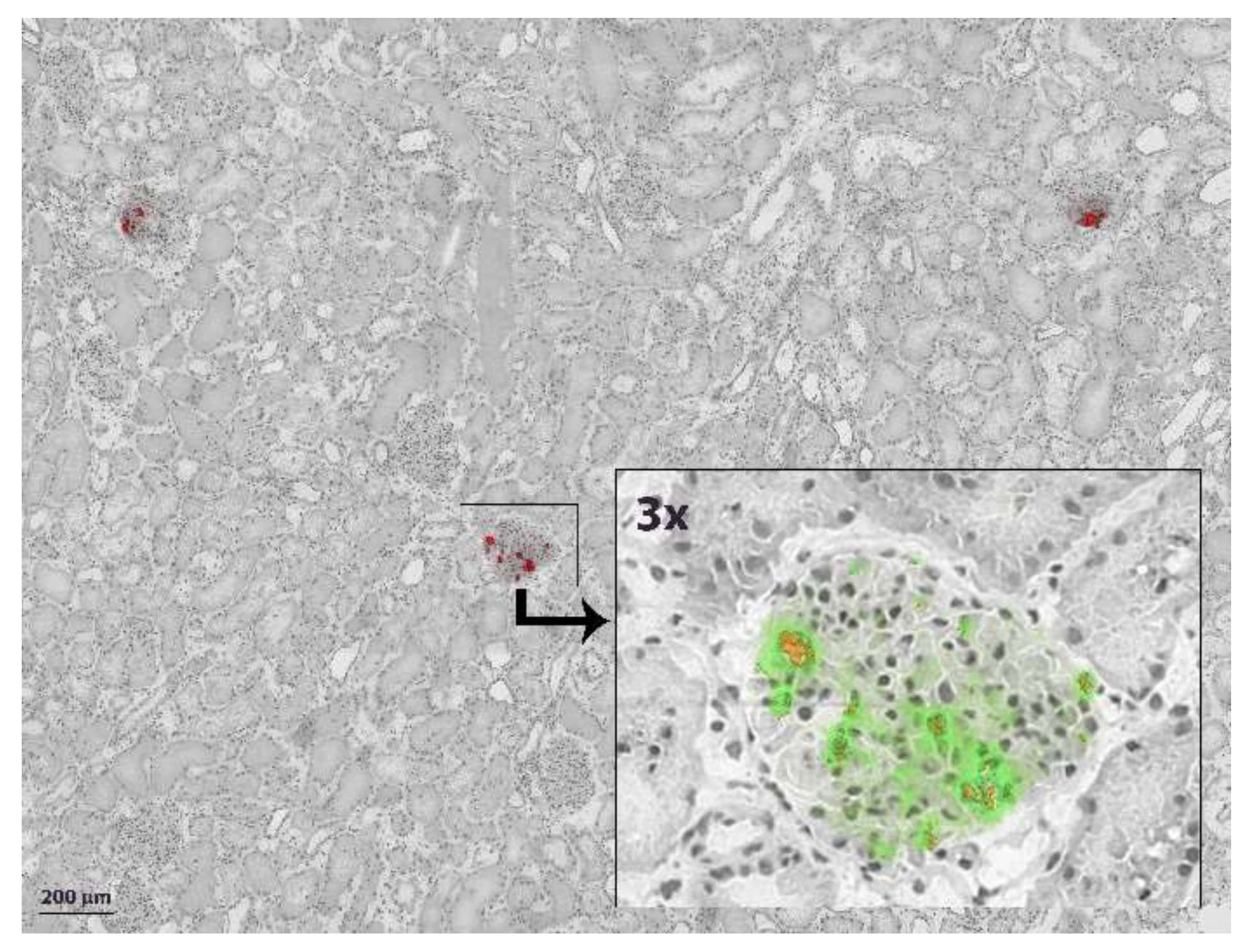
2.3. Renal Immunohistochemistry
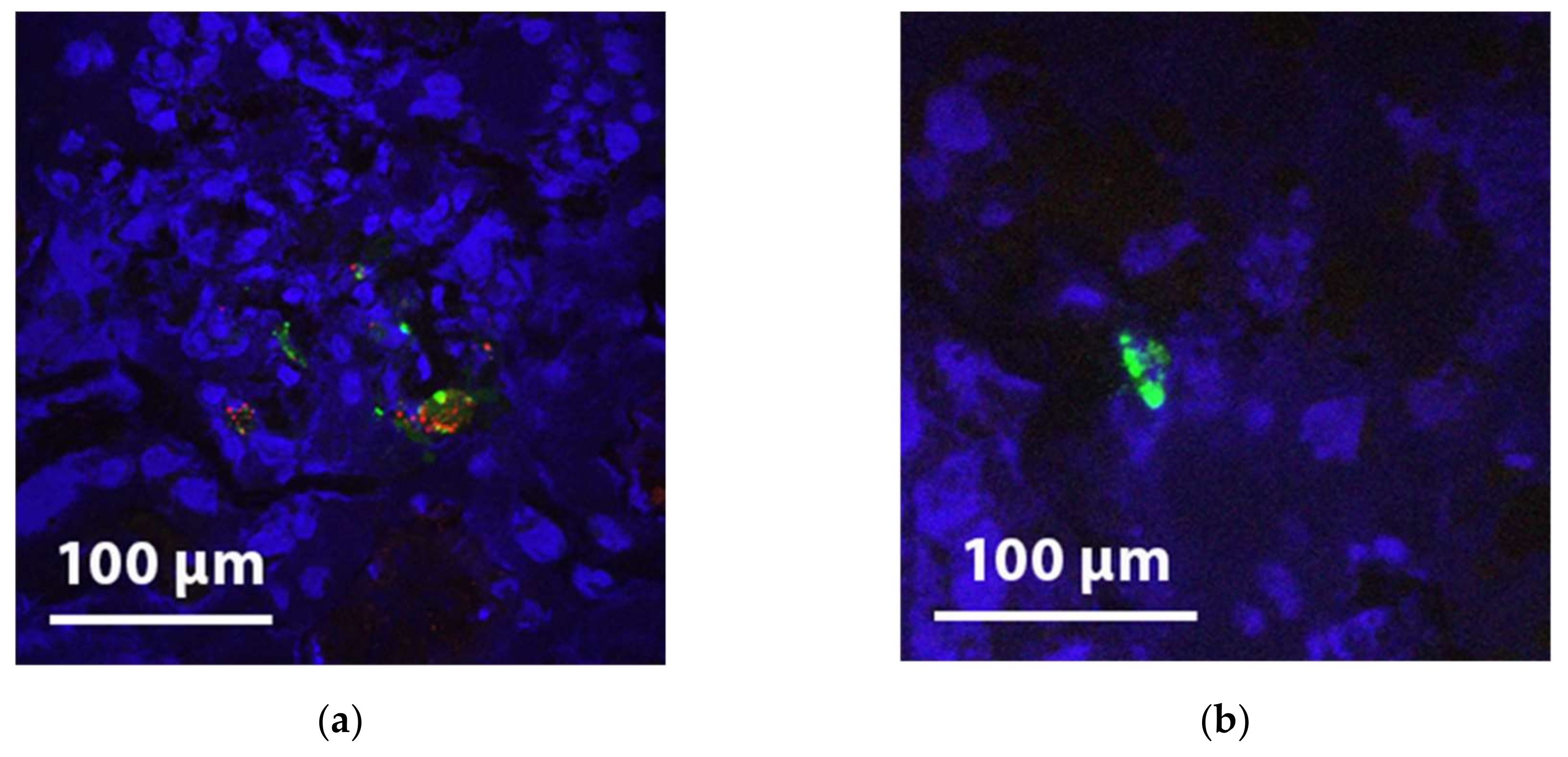
2.4. Fluorescence Microscopy in the Experiments with Pre-labelled MSCs
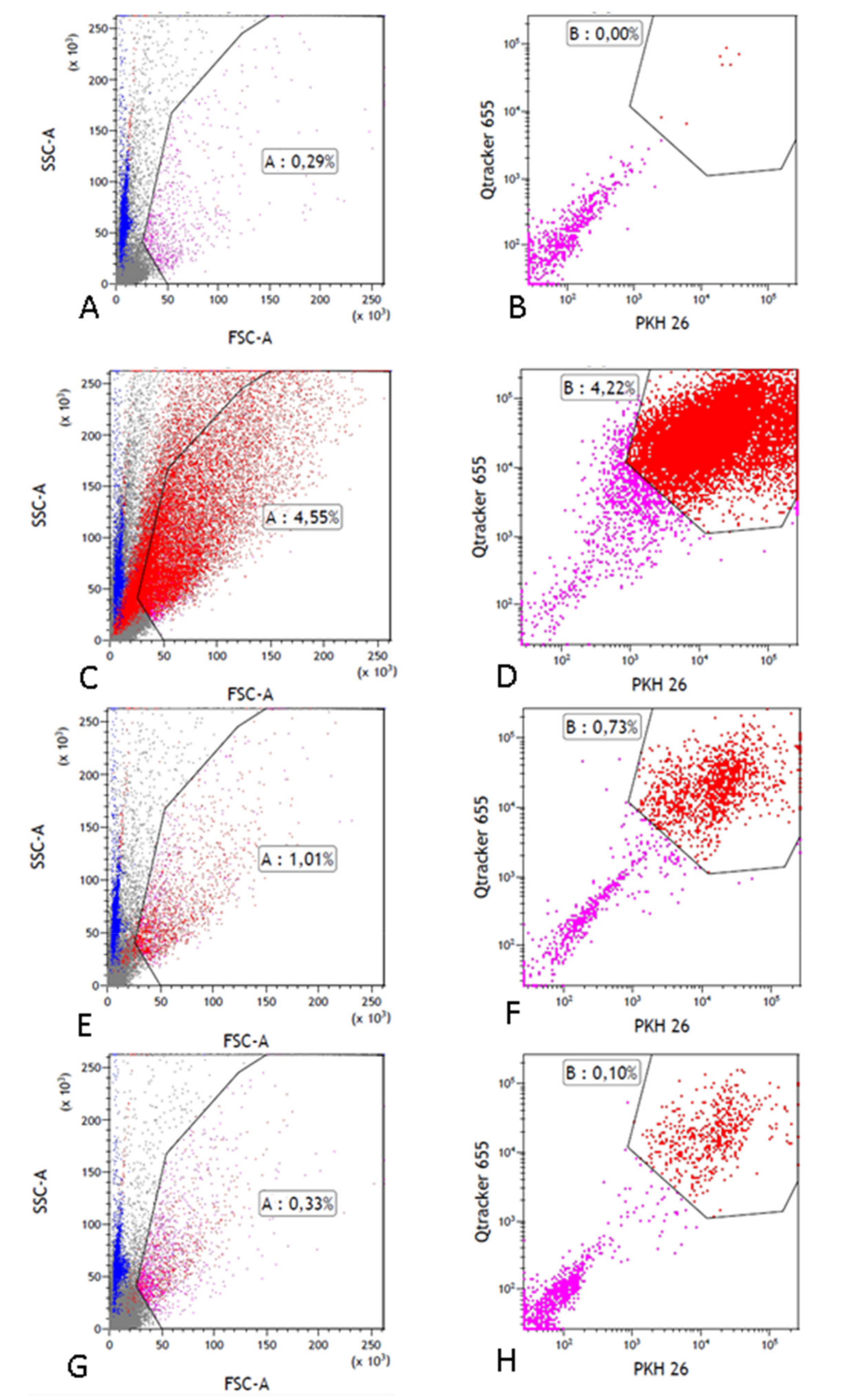
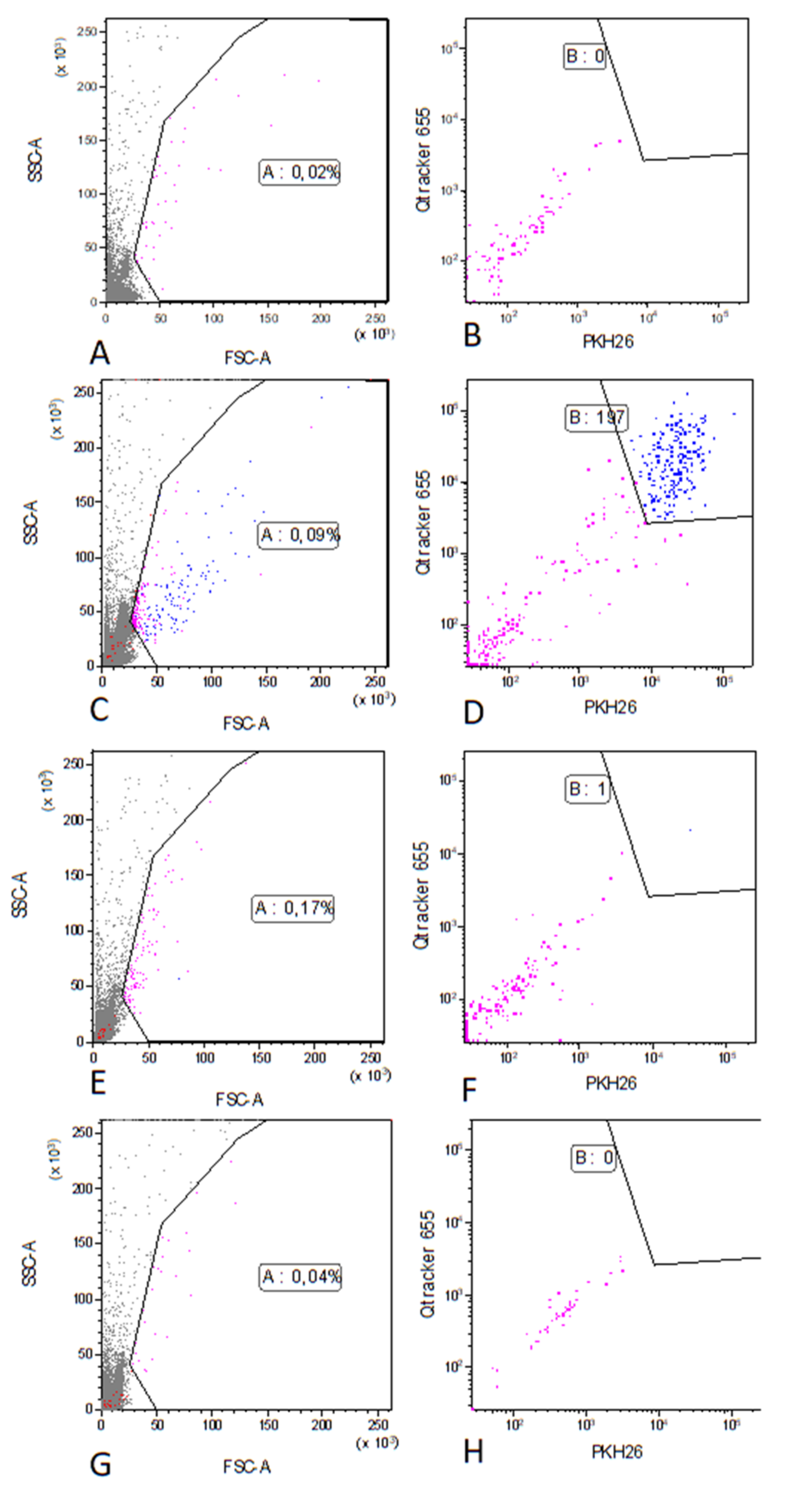
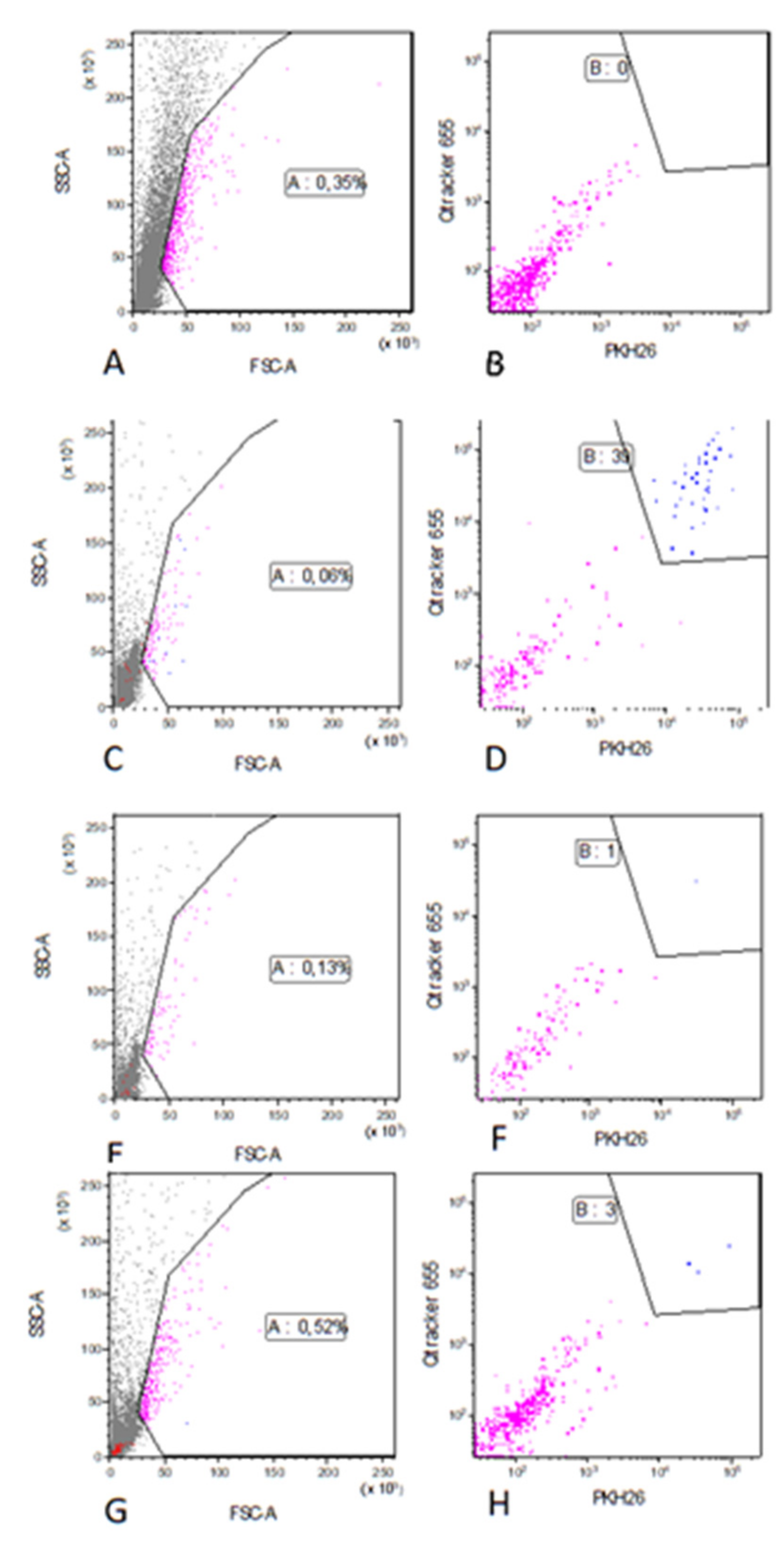
2.5. Detection of MSCs Using Flow Cytometry in the Experiments with Pre-labelled MSCs
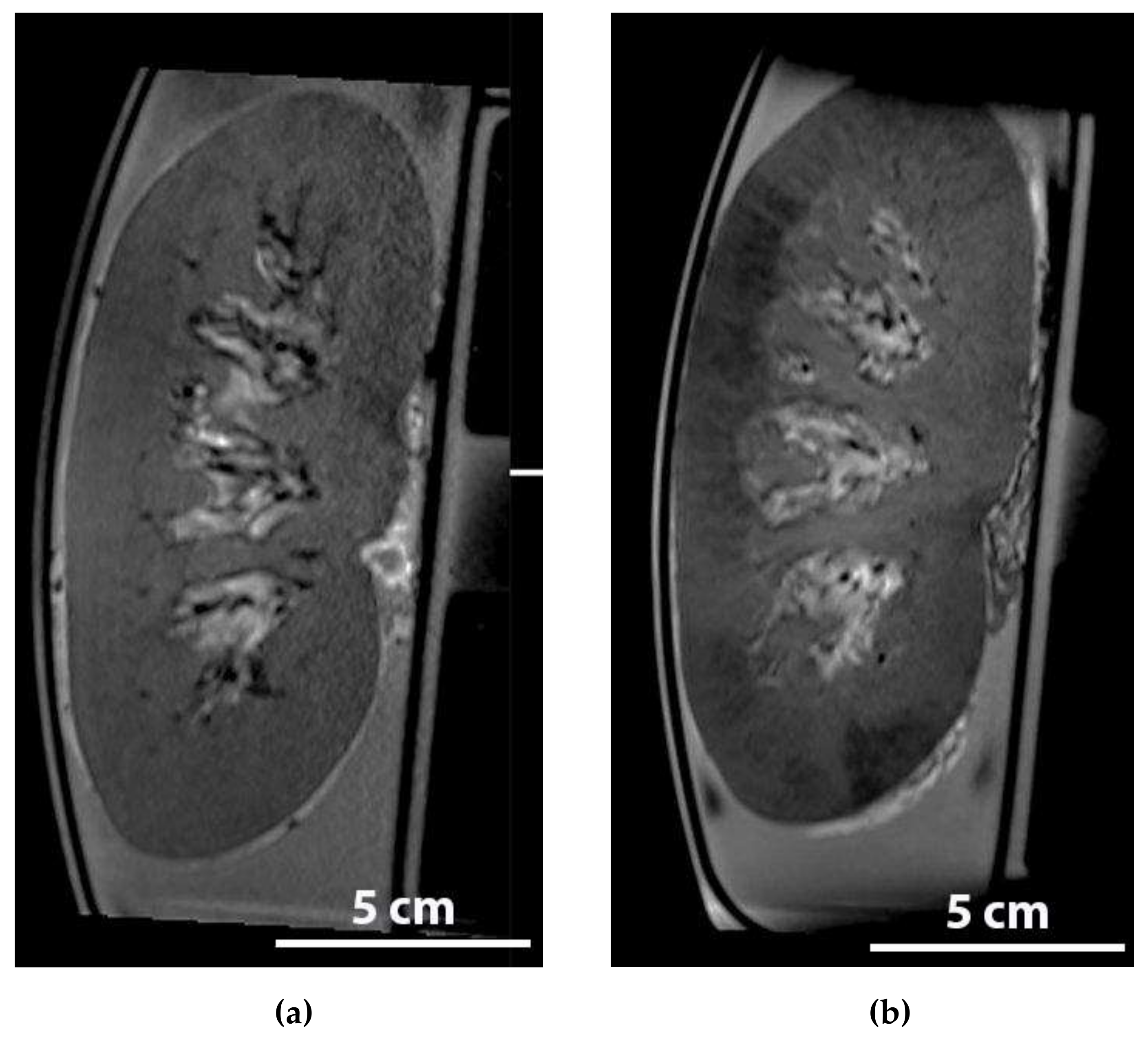
2.6. Detection of Iron Labelled MSCs during NMP in An MRI
3. Discussion
4. Materials and Methods
4.1. Organ and Blood Retrieval
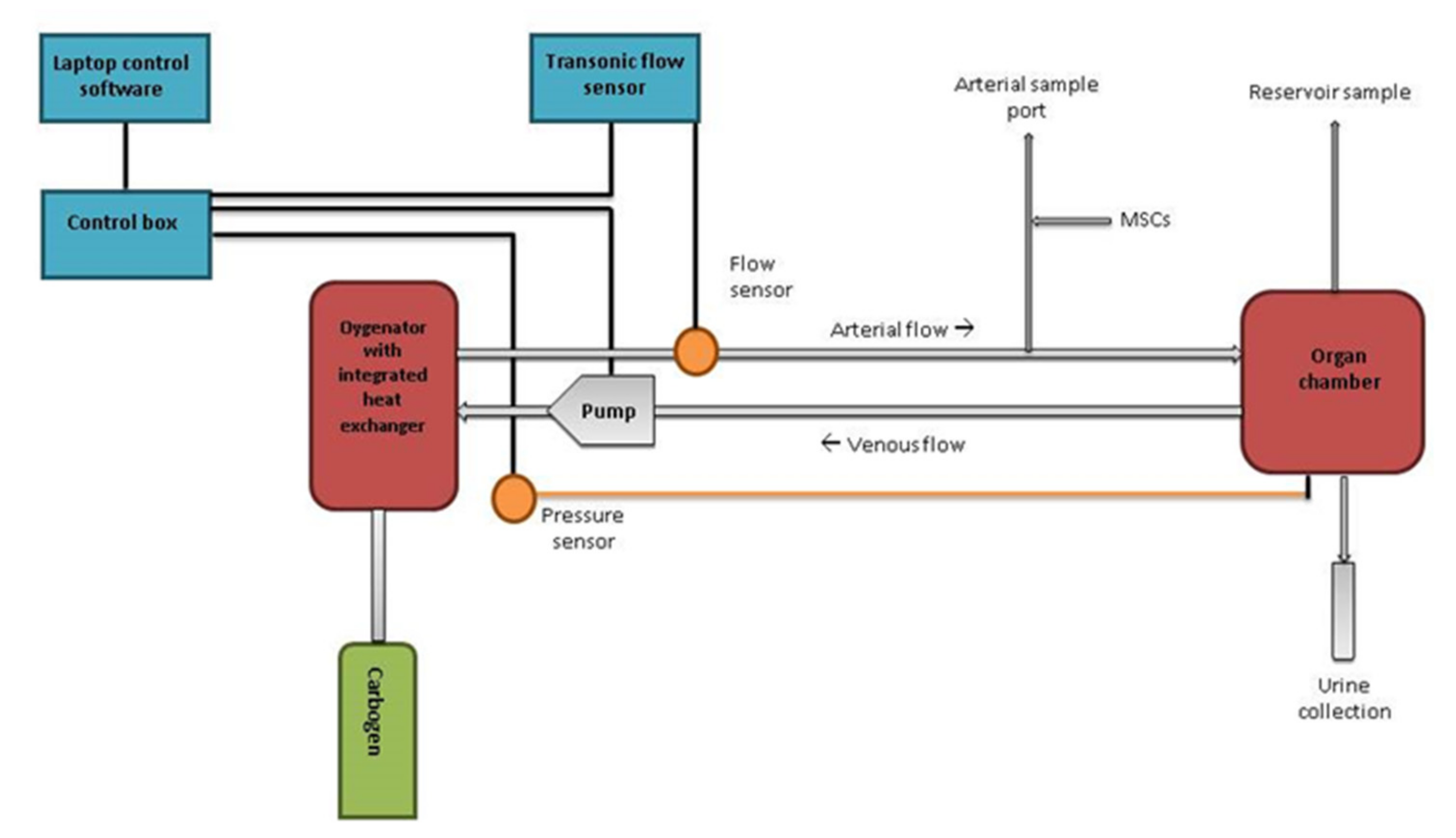
4.2. Perfusion Setup
4.3. Isolation, Culture and Infusion of MSCs
4.4. Pre-labelling of MSCs
4.5. Fluorescence-Activated Cell Sorting (FACS)
4.6. Histology and Fluorescence Microscopy
4.7. Detection of Iron Labelled MSCs during NMP in An MRI
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| DAPI | 4,6-diamidino-2-phenylindole dihydrochloride |
| DCD | Donation after circulatory death |
| FACS | Fluorescence activated cell sorting |
| FBS | Foetal bovine serum |
| FFPE | Formalin-fixed paraffin-embedded |
| GARPO | Goat anti rat polyclonal |
| HE | Haematoxylin and eosin |
| MEM-α | Minimal essential medium eagle-alpha |
| MRI | Magnetic resonance imaging |
| MSCS | Mesenchymal stromal cells |
| NMP | Normothermic machine perfusion |
| RAMPO | Rat anti-mouse polyclonal |
Appendix A




References
- Moers, C.; Leuvenink, H.G.D.; Ploeg, R.J. Donation after cardiac death: Evaluation of revisiting an important donor source. Nephrol Dial. Transpl. 2010, 25, 666–673. [Google Scholar] [CrossRef] [PubMed]
- Woodside, K.J.; Goldfarb, D.A.; Rabets, J.C.; Sanchez, E.Q.; Lebovitz, D.J.; Schulak, J.A.; Fung, J.J.; Eghtesad, B. Enhancing kidney function with thrombolytic therapy following donation after cardiac death: A multicenter quasi-blinded prospective randomized trial. Clin. Transpl. 2015, 29, 1173–1180. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, M.L.; Metcalfe, M.S.; White, S.A.; Waller, J.A.; Doughman, T.M.; Horsburgh, T.; Feehally, J.; Carr, S.J.; Veitch, P.S. A comparison of the results of renal transplantation from non–heart-beating, conventional cadaveric, and living donors. Kidney Int. 2000, 58, 2585–2591. [Google Scholar] [CrossRef] [PubMed]
- Hosgood, S.A.; van Heurn, E.; Nicholson, M.L. Normothermic machine perfusion of the kidney: Better conditioning and repair? Transpl. Int. 2015, 28, 657–664. [Google Scholar] [CrossRef] [PubMed]
- Bon, D.; Chatauret, N.; Giraud, S.; Thuillier, R.; Favreau, F.; Hauet, T. New strategies to optimize kidney recovery and preservation in transplantation. Nat. Rev. Nephrol. 2012, 8, 339–347. [Google Scholar] [CrossRef] [PubMed]
- Hosgood, S.A.; Barlow, A.D.; Yates, P.J.; Snoeijs, M.G.J.; van Heurn, E.L.; Nicholson, M.L. A pilot study assessing the feasibility of a short period of normothermic preservation in an experimental model of non heart beating donor kidneys. J. Surg. Res. 2011, 171, 283–290. [Google Scholar] [CrossRef]
- Kern, S.; Eichler, H.; Stoeve, J.; Klüter, H.; Bieback, K. Comparative analysis of mesenchymal stem cells from bone marrow, umbilical cord blood, or adipose tissue. Stem Cells. 2006, 24, 1294–1301. [Google Scholar] [CrossRef]
- Dominici, M.; Le Blanc, K.; Mueller, I.; Slaper-Cortenback, I.; Marini, F.; Krause, D.; Deans, R.; Keating, A.; Prockop, D.J.; Horwitz, E. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy 2006, 8, 315–317. [Google Scholar] [CrossRef]
- Casiraghi, F.; Remuzzi, G.; Perico, N. Mesenchymal stromal cells to promote kidney transplantation tolerance. Curr. Opin. Organ. Transpl. 2014, 19, 47–53. [Google Scholar] [CrossRef]
- De Vries, D.K.; Schaapherder, A.F.M.; Reinders, M.E.J. Mesenchymal stromal cells in renal ischemia/reperfusion injury. Front. Immunol. 2012, 3, 162. [Google Scholar] [CrossRef] [Green Version]
- Casiraghi, F.; Perico, N.; Cortinovis, M.; Remuzzi, G. Mesenchymal stromal cells in renal transplantation: Opportunities and challenges. Nat. Rev. Nephrol. 2016, 12, 241–253. [Google Scholar] [CrossRef] [PubMed]
- Franquesa, M.; Hoogduijn, M.J.; Reinders, M.E.; Eggenhofer, E.; Engela, A.U.; Mensah, F.K.; Torras, J.; Pileggi, A.; van Kooten, C.; Mahon, B.; et al. Mesenchymal Stem Cells in Solid Organ Transplantation (MiSOT) Fourth Meeting: Lessons Learned from First Clinical Trials. Transplantation 2013, 96, 234–238. [Google Scholar] [CrossRef] [PubMed]
- Reinders, M.E.J.; van Kooten, C.; Rabelink, T.J.; de Fijter, J.W. Mesenchymal Stromal Cell Therapy for Solid Organ Transplantation. Transplantation 2017, 102, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Hoogduijn, M.J.; Roemeling-van Rhijn, M.; Engela, A.U.; Korevaar, S.S.; Mensah, F.K.; Franquesa, M.; de Bruin, R.W.; Betjes, M.G.; Weimar, W.; Baan, C.C. Mesenchymal stem cells induce an inflammatory response after intravenous infusion. Stem Cells Dev. 2013, 22, 2825–2835. [Google Scholar] [CrossRef] [PubMed]
- Sierra-Parraga, J.M.; Eijken, M.; Hunter, J.; Moers, C.; Leuvenink, H.G.D.; Møller, B.; Ploeg, R.J.; Baan, C.C.; Jespersen, B.; Hoogduijn, M.J. Mesenchymal stromal cells as anti-inflammatory and regenerative mediators for donor kidneys during normothermic machine perfusion. Stem Cells Dev. 2017, 26, 1162–1170. [Google Scholar] [CrossRef] [PubMed]
- Satchell, S.C.; Braet, F. Glomerular endothelial cell fenestrations: An integral component of the glomerular filtration barrier. Am. J. Physiol. Ren Physiol. 2009, 296, F947–F956. [Google Scholar] [CrossRef] [PubMed]
- Ge, J.; Guo, L.; Wang, S.; Zhang, Y.; Cai, T.; Zhao, R.C.; Wu, Y. The Size of Mesenchymal Stem Cells is a Significant Cause of Vascular Obstructions and Stroke. Stem Cell Rev. 2014, 10, 295–303. [Google Scholar] [CrossRef] [PubMed]
- Scott, R.P.; Quaggin, S.E. The cell biology of renal filtration. JCB 2015, 209, 199–210. [Google Scholar] [CrossRef] [PubMed]
- Taghizadeh, R.R.; Cetrulo, K.J.; Cetrulo, C.L. Collagenase Impacts the Quantity and Quality of Native Mesenchymal Stem/Stromal Cells Derived during Processing of Umbilical Cord Tissue. Cell Transplant. 2018, 27, 181–193. [Google Scholar] [CrossRef]
- Mckee, C.; Chaudhry, G.R. Advances and challenges in stem cell culture. Colloids Surfaces B Biointerfaces 2017, 159, 62–77. [Google Scholar] [CrossRef]
- Eggenhofer, E.; Luk, F.; Dahlke, M.H.; Hoogduijn, M.J. The life and fate of mesenchymal stem cells. Front. Immunol. 2014, 5, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Luk, F.; Korevaar, S.S.; Roemeling-van Rhijn, M.R.; Franquesa, M.; Strini, T.; van den Engel, S.; Garqesha, M.; Roy, D.; Dor, F.J.; Horwitz, E.M.; et al. Inactivated Mesenchymal Stem Cells Maintain Immunomodulatory Capacity. Stem Cells Dev. 2016, 25, 1342–1355. [Google Scholar] [CrossRef] [PubMed]
- Mansilla, E.; Marin, G.H.; Sturla, F.; Drago, H.E.; Gil, M.A.; Salas, E.; Gardiner, M.C.; Piccinelli, G.; Bossi, S.; Salas, E.; et al. Human mesenchymal stem cells are tolerized by mice and improve skin and spinal cord injuries. Transplant. Proc. 2005, 37, 292–294. [Google Scholar] [CrossRef] [PubMed]
- Toma, C.; Pittenger, M.F.; Cahill, K.S.; Byrne, B.J.; Kessler, P.D. Human mesenchymal stem cells differentiate to a cardiomyocyte phenotype in the adult murine heart. Circulation 2002, 105, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Grinnemo, K.; Mansson, A.; Dellgren, G.; Klingberg, D.; Wardell, E.; Drvota, V.; Tammik, C.; Holgersson, J.; Ringdén, O.; Sylvén, C.; et al. Xenoreactivitey and engraftment of human mesenchymal stem cells transplanted into infarcted rat myocardium. J. Thorac. Cardiovasc. Surg. 2004, 127, 1293–1300. [Google Scholar] [CrossRef] [PubMed]
- Mordant, P.; Nakajima, D.; Kalaf, R.; Iskender, I.; Maahs, L.; Behrens, P.; Coutinho, R.; Iyer, R.K.; Davies, J.E.; Cypel, M.; et al. Mesenchymal stem cell treatment is associated with decreased perfusate concentration of interleukin-8 during ex vivo perfusion of donor lungs after 18-hour preservation. J. Hear. Lung Transplant. 2016, 35, 1245–1254. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Ezzelarab, M.B.; Cooper, D.K. Do Mesenchymal Stem Cells Function Across Species Barriers? Xenotransplantation 2012, 19, 273–285. [Google Scholar] [CrossRef] [PubMed]
- Venema, L.H.; Brat, A.; Moers, C.; Hart, N.A.; Ploeg, R.J.; Hannaert, P.; Minor, T.; Leuvenink, H.G.D. Effects of oxygen during long-term hypothermic machine perfusion in a porcine model of kidney donation after circulatory death. Transplantation 2019, 1. [Google Scholar] [CrossRef] [PubMed]
- Bagul, A.; Hosgood, S.A.; Kaushik, M.; Kay, M.D.; Waller, H.L.; Nicholson, M.L. Experimental renal preservation by normothermic resuscitation perfusion with autologous blood. Br. J. Surg. 2008, 95, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Hou, J. Mesenchymal stem cell-based therapy in kidney transplantation. Stem Cell Res. Ther. 2016, 7, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDonald, C.A.; Oehme, D.; Pham, Y.; Kelly, K.; Itescu, S.; Gibbon, A.; Jenkin, G. Evaluation of the safety and tolerability of a high-dose intravenous infusion of allogeneic mesenchymal precursor cells. Cytotherapy 2015, 17, 1178–1187. [Google Scholar] [CrossRef] [PubMed]






© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pool, M.; Eertman, T.; Sierra Parraga, J.; ’t Hart, N.; Roemeling-van Rhijn, M.; Eijken, M.; Jespersen, B.; Reinders, M.; Hoogduijn, M.; Ploeg, R.; et al. Infusing Mesenchymal Stromal Cells into Porcine Kidneys during Normothermic Machine Perfusion: Intact MSCs Can Be Traced and Localised to Glomeruli. Int. J. Mol. Sci. 2019, 20, 3607. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20143607
Pool M, Eertman T, Sierra Parraga J, ’t Hart N, Roemeling-van Rhijn M, Eijken M, Jespersen B, Reinders M, Hoogduijn M, Ploeg R, et al. Infusing Mesenchymal Stromal Cells into Porcine Kidneys during Normothermic Machine Perfusion: Intact MSCs Can Be Traced and Localised to Glomeruli. International Journal of Molecular Sciences. 2019; 20(14):3607. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20143607
Chicago/Turabian StylePool, Merel, Tim Eertman, Jesus Sierra Parraga, Nils ’t Hart, Marieke Roemeling-van Rhijn, Marco Eijken, Bente Jespersen, Marlies Reinders, Martin Hoogduijn, Rutger Ploeg, and et al. 2019. "Infusing Mesenchymal Stromal Cells into Porcine Kidneys during Normothermic Machine Perfusion: Intact MSCs Can Be Traced and Localised to Glomeruli" International Journal of Molecular Sciences 20, no. 14: 3607. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20143607