mTOR Expression in Liver Transplant Candidates with Hepatocellular Carcinoma: Impact on Histological Features and Tumour Recurrence

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Population Characteristics and HCC Recurrence
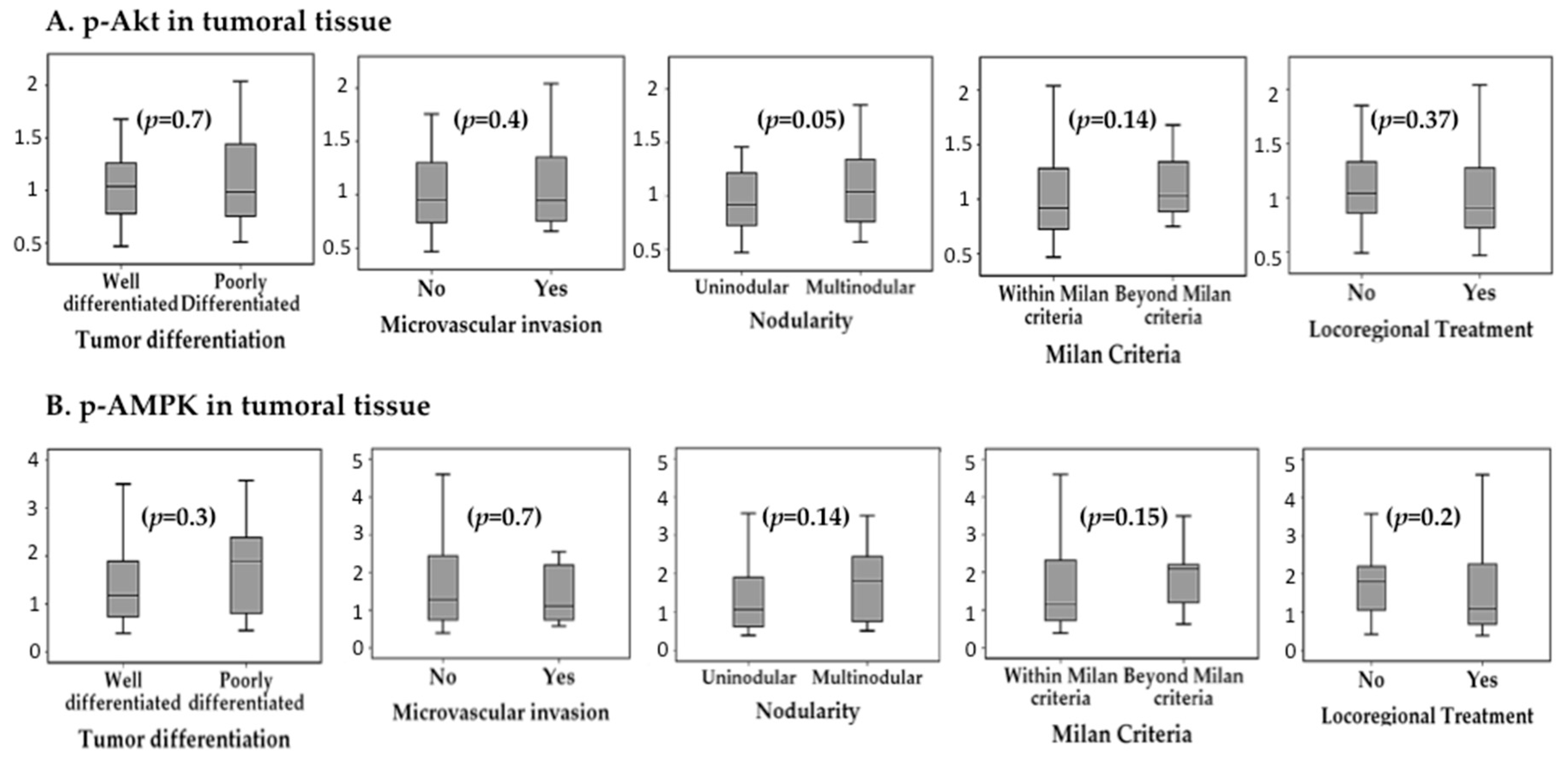
2.2. Activation of mTOR Pathway in Tumoral and Peritumoral Tissue and Association with HCC Histological Features
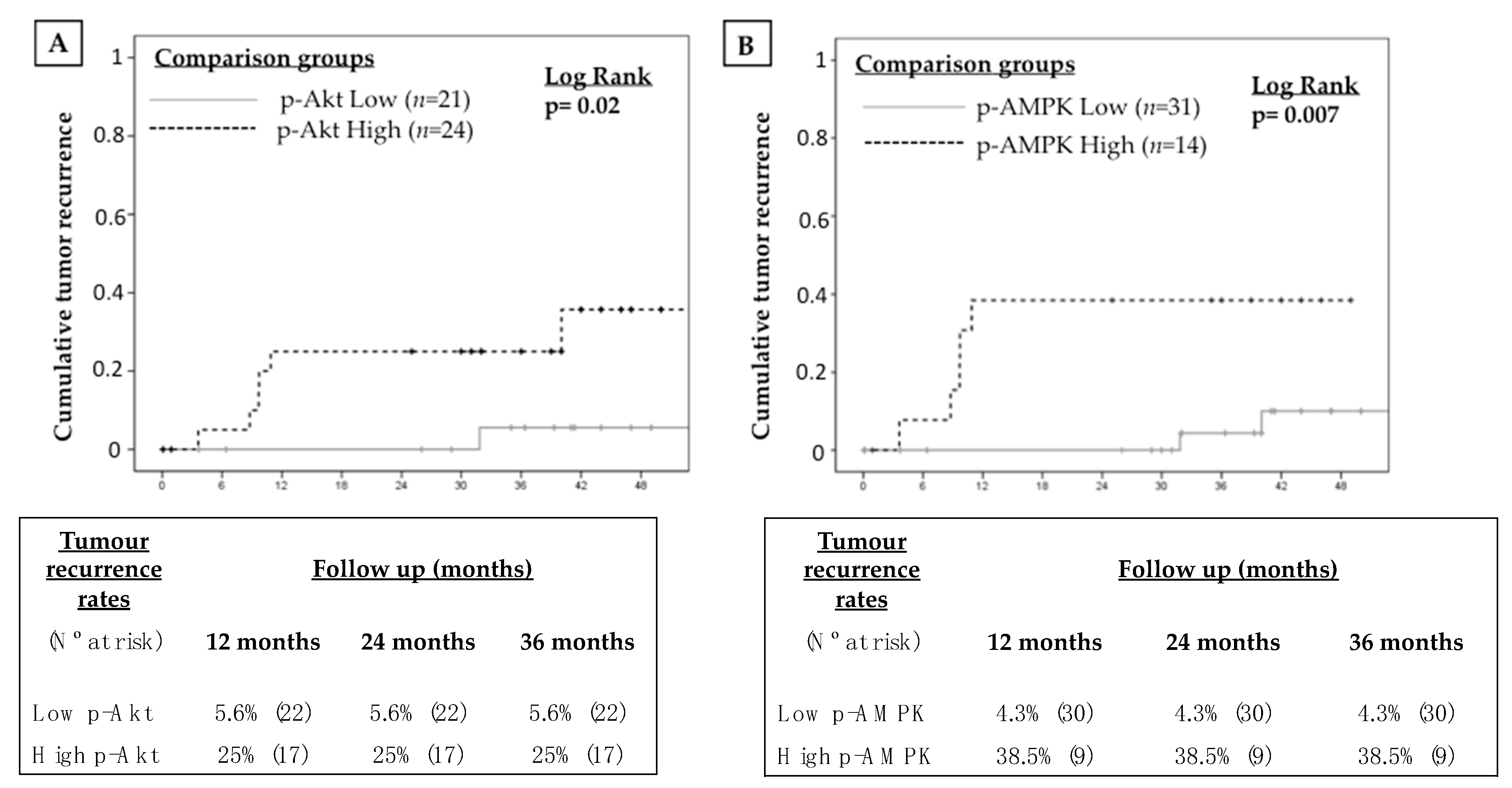
2.3. Impact of mTOR Pathway Activation in Tumour Recurrence
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Histopathology
4.3. Protein Extraction from FFPE Tissues
4.4. Detection and Quantification of Protein Related to the mTOR Signalling Pathway
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgements
Conflicts of Interest
Abbreviations
| HCC | Hepatocellular carcinoma |
| LT | Liver transplantation |
| CNI | Calcineurin inhibitors |
| mTOR | Mammalian target of rapamycin |
| mTORC1 | mTOR complex 1 |
| mTORC2 | mTOR complex 2 |
| p- | phospho |
| TACE | Transarterial Chemoembolization |
| RFA | Radiofrequency ablation |
References
- Organisation, W.H. Globocan. Available online: http://globocan.iarc.fr/Default.aspx (accessed on 14 July 2018).
- Bruix, J.; Reig, M.; Sherman, M. Evidence-Based Diagnosis, Staging, and Treatment of Patients With Hepatocellular Carcinoma. Gastroenterology 2016, 150, 835–853. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed]
- Klintmalm, G.B. Liver transplantation for hepatocellular carcinoma: A registry report of the impact of tumor characteristics on outcome. Ann. Surg. 1998, 228, 479–490. [Google Scholar] [CrossRef]
- Yao, F.Y.; Ferrell, L.; Bass, N.M.; Watson, J.J.; Bacchetti, P.; Venook, A.; Ascher, N.L.; Roberts, J.P. Liver transplantation for hepatocellular carcinoma: Expansion of the tumor size limits does not adversely impact survival. Hepatology 2001, 33, 1394–1403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarbassov, D.D.; Ali, S.M.; Sabatini, D.M. Growing roles for the mTOR pathway. Curr. Opin. Cell Biol. 2005, 17, 596–603. [Google Scholar] [CrossRef] [PubMed]
- Bhat, M.; Sonenberg, N.; Gores, G.J. The mTOR pathway in hepatic malignancies. Hepatology 2013, 58, 810–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villanueva, A.; Chiang, D.Y.; Newell, P.; Peix, J.; Thung, S.; Alsinet, C.; Tovar, V.; Roayaie, S.; Minguez, B.; Sole, M.; et al. Pivotal role of mTOR signaling in hepatocellular carcinoma. Gastroenterology 2008, 135, 1972–1983.e11. [Google Scholar] [CrossRef]
- Sahin, F.; Kannangai, R.; Adegbola, O.; Wang, J.; Su, G.; Torbenson, M. mTOR and P70 S6 kinase expression in primary liver neoplasms. Clin. Cancer Res. 2004, 10, 8421–8425. [Google Scholar] [CrossRef]
- Zhou, L.; Huang, Y.; Li, J.; Wang, Z. The mTOR pathway is associated with the poor prognosis of human hepatocellular carcinoma. Med. Oncol. 2010, 27, 255–261. [Google Scholar] [CrossRef]
- Fischer, L.; Saliba, F.; Kaiser, G.M.; De Carlis, L.; Metselaar, H.J.; De Simone, P.; Duvoux, C.; Nevens, F.; Fung, J.J.; Dong, G.; et al. Three-year Outcomes in De Novo Liver Transplant Patients Receiving Everolimus With Reduced Tacrolimus: Follow-Up Results From a Randomized, Multicenter Study. Transplantation 2015, 99, 1455–1462. [Google Scholar] [CrossRef]
- Schumacher, G.; Oidtmann, M.; Rueggeberg, A.; Jacob, D.; Jonas, S.; Langrehr, J.M.; Neuhaus, R.; Bahra, M.; Neuhaus, P. Sirolimus inhibits growth of human hepatoma cells alone or combined with tacrolimus, while tacrolimus promotes cell growth. World J. Gastroenterol. 2005, 11, 1420–1425. [Google Scholar] [CrossRef] [PubMed]
- Toso, C.; Merani, S.; Bigam, D.L.; Shapiro, A.M.; Kneteman, N.M. Sirolimus-based immunosuppression is associated with increased survival after liver transplantation for hepatocellular carcinoma. Hepatology 2010, 51, 1237–1243. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, M.A.; Trotter, J.F.; Wachs, M.; Bak, T.; Campsen, J.; Skibba, A.; Kam, I. Sirolimus-based immunosuppression following liver transplantation for hepatocellular carcinoma. Liver Transpl. 2008, 14, 633–638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menon, K.V.; Hakeem, A.R.; Heaton, N.D. Meta-analysis: Recurrence and survival following the use of sirolimus in liver transplantation for hepatocellular carcinoma. Aliment. Pharmacol. Ther. 2013, 37, 411–419. [Google Scholar] [CrossRef]
- Geissler, E.K.; Schnitzbauer, A.A.; Zulke, C.; Lamby, P.E.; Proneth, A.; Duvoux, C.; Burra, P.; Jauch, K.W.; Rentsch, M.; Ganten, T.M.; et al. Sirolimus Use in Liver Transplant Recipients With Hepatocellular Carcinoma: A Randomized, Multicenter, Open-Label Phase 3 Trial. Transplantation 2016, 100, 116–125. [Google Scholar] [CrossRef]
- Rodriguez-Peralvarez, M.; Guerrero, M.; Barrera, L.; Ferrin, G.; Alamo, J.M.; Ayllon, M.D.; Artacho, G.S.; Montero, J.L.; Briceno, J.; Bernal, C.; et al. Impact of Early Initiated Everolimus on the Recurrence of Hepatocellular Carcinoma after Liver Transplantation. Transplantation 2018. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Peralvarez, M.; Guerrero-Misas, M.; Thorburn, D.; Davidson, B.R.; Tsochatzis, E.; Gurusamy, K.S. Maintenance immunosuppression for adults undergoing liver transplantation: A network meta-analysis. Cochrane Database Syst. Rev. 2017, 3, CD011639. [Google Scholar] [CrossRef]
- Jin, Y.P.; Valenzuela, N.M.; Ziegler, M.E.; Rozengurt, E.; Reed, E.F. Everolimus inhibits anti-HLA I antibody-mediated endothelial cell signaling, migration and proliferation more potently than sirolimus. Am. J. Transpl. 2014, 14, 806–819. [Google Scholar] [CrossRef]
- Qi, H.L.; Zhuang, B.J.; Li, C.S.; Liu, Q.Y. Peri-operative use of sorafenib in liver transplantation: A time-to-event meta-analysis. World J. Gastroenterol. 2015, 21, 1636–1640. [Google Scholar] [CrossRef]
- Murali, A.R.; Patil, S.; Phillips, K.T.; Voigt, M. Locoregional Therapy with Curative Intent versus Primary Liver Transplant for Hepatocellular Carcinoma: Systematic Review and Meta-analysis. Transplantation 2017, 101, e249–e257. [Google Scholar] [CrossRef]
- Guerrero-Misas, M.; Rodriguez-Peralvarez, M.; De la Mata, M. Strategies to improve outcome of patients with hepatocellular carcinoma receiving a liver transplantation. World J. Hepatol. 2015, 7, 649–661. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Peralvarez, M.; Tsochatzis, E.; Naveas, M.C.; Pieri, G.; Garcia-Caparros, C.; O’Beirne, J.; Poyato-Gonzalez, A.; Ferrin-Sanchez, G.; Montero-Alvarez, J.L.; Patch, D.; et al. Reduced exposure to calcineurin inhibitors early after liver transplantation prevents recurrence of hepatocellular carcinoma. J. Hepatol. 2013, 59, 1193–1199. [Google Scholar] [CrossRef] [PubMed]
- Vivarelli, M.; Cucchetti, A.; La Barba, G.; Ravaioli, M.; Del Glaudio, M.; Lauro, A.; Grazi, G.L.; Pinna, A.D. Liver Transplantation for hepatocellular carcinoma under calcineurn inhibitors: Reassessment of risk factors for tumor recurrence. Ann. Surg. 2008, 248, 857–862. [Google Scholar] [CrossRef]
- Zarogoulidis, P.; Lampaki, S.; Turner, J.F.; Huang, H.; Kakolyris, S.; Syrigos, K.; Zarogoulidis, K. mTOR pathway: A current, up-to-date mini-review (Review). Oncol. Lett. 2014, 8, 2367–2370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matter, M.S.; Decaens, T.; Andersen, J.B.; Thorgeirsson, S.S. Targeting the mTOR pathway in hepatocellular carcinoma: Current state and future trends. J. Hepatol. 2014, 60, 855–865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Z.; Jin, W.; Jin, H.; Wang, X. mTOR in viral hepatitis and hepatocellular carcinoma: Function and treatment. BioMed Res. Int. 2014, 2014, 735672. [Google Scholar] [CrossRef]
- Duvoux, C.; Toso, C. mTOR inhibitor therapy: Does it prevent HCC recurrence after liver transplantation? Transpl. Rev. (Orlando) 2015, 29, 168–174. [Google Scholar] [CrossRef]
- Calvisi, D.F.; Wang, C.; Ho, C.; Ladu, S.; Lee, S.A.; Mattu, S.; Destefanis, G.; Delogu, S.; Zimmermann, A.; Ericsson, J.; et al. Increased lipogenesis, induced by AKT-mTORC1-RPS6 signaling, promotes development of human hepatocellular carcinoma. Gastroenterology 2011, 140, 1071–1083. [Google Scholar] [CrossRef]
- Van Zijl, F.; Mair, M.; Csiszar, A.; Schneller, D.; Zulehner, G.; Huber, H.; Eferl, R.; Beug, H.; Dolznig, H.; Mikulits, W. Hepatic tumor-stroma crosstalk guides epithelial to mesenchymal transition at the tumor edge. Oncogene 2009, 28, 4022–4033. [Google Scholar] [CrossRef]
- Gupta, S.C.; Kunnumakkara, A.B.; Aggarwal, S.; Aggarwal, B.B. Inflammation, a Double-Edge Sword for Cancer and Other Age-Related Diseases. Front. Immunol. 2018, 9, 2160. [Google Scholar] [CrossRef]
- Kuang, D.M.; Zhao, Q.; Wu, Y.; Peng, C.; Wang, J.; Xu, Z.; Yin, X.Y.; Zheng, L. Peritumoral neutrophils link inflammatory response to disease progression by fostering angiogenesis in hepatocellular carcinoma. J. Hepatol. 2011, 54, 948–955. [Google Scholar] [CrossRef] [PubMed]
- Tsochatzis, E.; Garcovich, M.; Marelli, L.; Papastergiou, V.; Fatourou, E.; Rodriguez-Peralvarez, M.L.; Germani, G.; Davies, N.; Yu, D.; Luong, T.V.; et al. Transarterial embolization as neo-adjuvant therapy pretransplantation in patients with hepatocellular carcinoma. Liver Int. 2013. [Google Scholar] [CrossRef] [PubMed]
- Edmonson, H.A.; Steiner, P.E. Primary carcinoma of the liver: A study of 100 cases among 48,900 necropsies. Cancer 1954, 7, 462–503. [Google Scholar] [CrossRef]
- Rodriguez-Peralvarez, M.; Luong, T.V.; Andreana, L.; Meyer, T.; Dhillon, A.P.; Burroughs, A.K. A systematic review of microvascular invasion in hepatocellular carcinoma: Diagnostic and prognostic variability. Ann. Surg. Oncol. 2013, 20, 325–339. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics (N = 49) | |
| Age, mean (SD) | 56.4 (7.2) |
| Gender | |
| Male, n (%)/Female, n (%) | 42 (85.7)/7 (14.3) |
| Aetiology of liver disease | |
| HCV, n (%) | 33 (67.3) |
| Alcohol, n (%) | 26 (53.1) |
| HBV, n (%) | 3 (6.1) |
| Autoimmune liver disease, n (%) | 1 (2) |
| NAFLD, n (%) | 1 (2) |
| Hemochromatosis, n (%) | 1 (2) |
| Cryptogenetic, n (%) | 3 (6.1) |
| MELD score, mean (SD) | 13.6 (5.1) |
| Previous hepatic decompensation, n (%) | 34 (69.4) |
| Ascites, n (%) | 28 (57.1) |
| Hepatic encephalopathy, n (%) | 21 (42.9) |
| Variceal bleeding, n (%) | 11 (22.4) |
| SBP, n (%) | 7 (14.3) |
| HRS, n (%) | 3 (6.1) |
| Bridging LRT, n (%) | 31 (63.3) |
| TACE, n (%) | 15 (36.7) |
| RFA, n (%) | 8 (16.3) |
| TACE + RFA, n (%) | 6 (12.2) |
| Liver resection, n (%) | 2 (4.1) |
| HCC radiological features | |
| Uninodular/multinodular, n (%) | 21 (42.9)/21 (42.9) |
| Number of nodules, mean (SD) | 1.62 (0.7) |
| DLN, mean (SD) | 2.5 (0.9) |
| TTB, mean (SD) | 3.3 (1.5) |
| HCC histological features | |
| Uninodular/multinodular, n (%) | 26 (53.1)/23 (46.9) |
| Number of nodules, mean (SD) | 1.7 (0.9) |
| DLN, mean (SD) | 3.1 (2) |
| TTB, mean (SD) | 4.1 (2.5) |
| Well differentiated or complete necrosis, n (%) | 22 (44.9) |
| Beyond Milan criteria, n (%) | 12 (24.5) |
| Microvascular invasion, n (%) | 13 (26.5) |
| Satellitosis, n (%) | 2 (4.1) |
| Macrovascular invasion, n (%) | 2 (4.1) |
| Protein | Location | Mean (SD) | ΔSignal (%) | p |
|---|---|---|---|---|
| p-mTOR | Tumoral | 0.9(0.2) | 22.2 | <0.001 |
| Peritumoral | 1.1 (0.3) | |||
| p-AKT | Tumoral | 1.1 (0.4) | 18.2 | 0.004 |
| Peritumoral | 1.3 (0.5) | |||
| p-AMPK | Tumoral | 1.6 (1.1) | 56.3 | <0.001 |
| Peritumoral | 2.5 (1.7) | |||
| p-P70S6K | Tumoral | 0.3 (0.14) | 33.3 | <0.001 |
| Peritumoral | 0.4 (0.2) | |||
| p-S6RP | Tumoral | 1.1 (0.5) | 54.6 | <0.001 |
| Peritumoral | 1.7 (1) |
| Protein | Origin | Threshold | Sensitivity (%) | Specificity (%) | AUC |
|---|---|---|---|---|---|
| p-mTOR | Tumoral | 0.85 | 85.70 | 57.90 | 71.80 |
| Peritumoral | 1.18 | 42.90 | 73.70 | 58.27 | |
| p-AKT | Tumoral | 1.00 | 85.70 | 57.90 | 69.17 |
| Peritumoral | 1.96 | 28.57 | 84.20 | 53.57 | |
| p-AMPK | Tumoral | 2.19 | 71.40 | 76.30 | 73.87 |
| Peritumoral | 0.70 | 100.00 | 13.2 | 56.58 | |
| p-P70S6K | Tumoral | 0.47 | 42.90 | 89.50 | 66.17 |
| Peritumoral | 0.41 | 71.40 | 57.90 | 63.35 | |
| p-S6RP | Tumoral | 1.05 | 71.40 | 63.20 | 67.29 |
| Peritumoral | 3.52 | 28.60 | 97.40 | 62.97 |
| Variable | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | |
| LRT | 0.76 | 0.17–3.4 | 0.72 | - | - | - |
| Multinodular | 1.55 | 0.35–6.9 | 0.6 | 0.42 | 0.06–2.8 | 0.37 |
| DLN | 0.86 | 0.54–1.38 | 0.55 | - | - | - |
| TTB | 1.05 | 0.79–1.39 | 0.74 | - | - | - |
| Beyond Milan | 1.11 | 0.22–5.74 | 0.90 | - | - | - |
| Microvascular invasion | 2.37 | 0.53–10.61 | 0.26 | 2.18 | 0.4–11.9 | 0.37 |
| Poorly differentiated | 1.94 | 0.38–10.02 | 0.43 | - | - | - |
| High p-Akt Tumoral | 6.27 | 0.75–52.4 | 0.09 | 1.64 | 0.11–24.9 | 0.72 |
| High p-Akt Peritumoral | 1.49 | 0.33–6.74 | 0.6 | - | - | - |
| High p-AMPK Tumoral | 7.05 | 1.36–36.64 | 0.02 | 6.9 | 1.3–37.1 | 0.03 |
| High p-AMPKa Peritumoral | 25.33 | 0.002–292543 | 0.5 | - | - | - |
| High p-mTOR Tumoral | 6.58 | 0.79–54.72 | 0.08 | 2.08 | 0.21–20.9 | 0.53 |
| High p-mTOR Peritumoral | 2.04 | 0.5–9.13 | 0.4 | - | - | - |
| High p-P70S6K Tumoral | 5.49 | 1.2–24.9 | 0.03 | 1.19 | 0.07–19.41 | 0.9 |
| High p-P70S6K Peritumoral | 3.29 | 0.63–17.18 | 0.16 | 2.25 | 0.34–14.81 | 0.4 |
| High p-S6RP Tumoral | 3.57 | 0.7–18.41 | 0.13 | 0.84 | 0.1–7.28 | 0.87 |
| High p-S6RP Peritumoral | 8.01 | 1.52–41.88 | 0.01 | 7.5 | 1.3–43.7 | 0.02 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guerrero, M.; Ferrín, G.; Rodríguez-Perálvarez, M.; González-Rubio, S.; Sánchez-Frías, M.; Amado, V.; Pozo, J.C.; Poyato, A.; Ciria, R.; Ayllón, M.D.; et al. mTOR Expression in Liver Transplant Candidates with Hepatocellular Carcinoma: Impact on Histological Features and Tumour Recurrence. Int. J. Mol. Sci. 2019, 20, 336. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20020336
Guerrero M, Ferrín G, Rodríguez-Perálvarez M, González-Rubio S, Sánchez-Frías M, Amado V, Pozo JC, Poyato A, Ciria R, Ayllón MD, et al. mTOR Expression in Liver Transplant Candidates with Hepatocellular Carcinoma: Impact on Histological Features and Tumour Recurrence. International Journal of Molecular Sciences. 2019; 20(2):336. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20020336
Chicago/Turabian StyleGuerrero, Marta, Gustavo Ferrín, Manuel Rodríguez-Perálvarez, Sandra González-Rubio, Marina Sánchez-Frías, Víctor Amado, Juan C. Pozo, Antonio Poyato, Rubén Ciria, María D. Ayllón, and et al. 2019. "mTOR Expression in Liver Transplant Candidates with Hepatocellular Carcinoma: Impact on Histological Features and Tumour Recurrence" International Journal of Molecular Sciences 20, no. 2: 336. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20020336