Natural Products in Neurodegenerative Diseases: A Great Promise but an Ethical Challenge



{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Natural Products in Neurodegeneration
3. Natural Products: On the Cutting Edge of Ethics?
3.1. Patient Autonomy
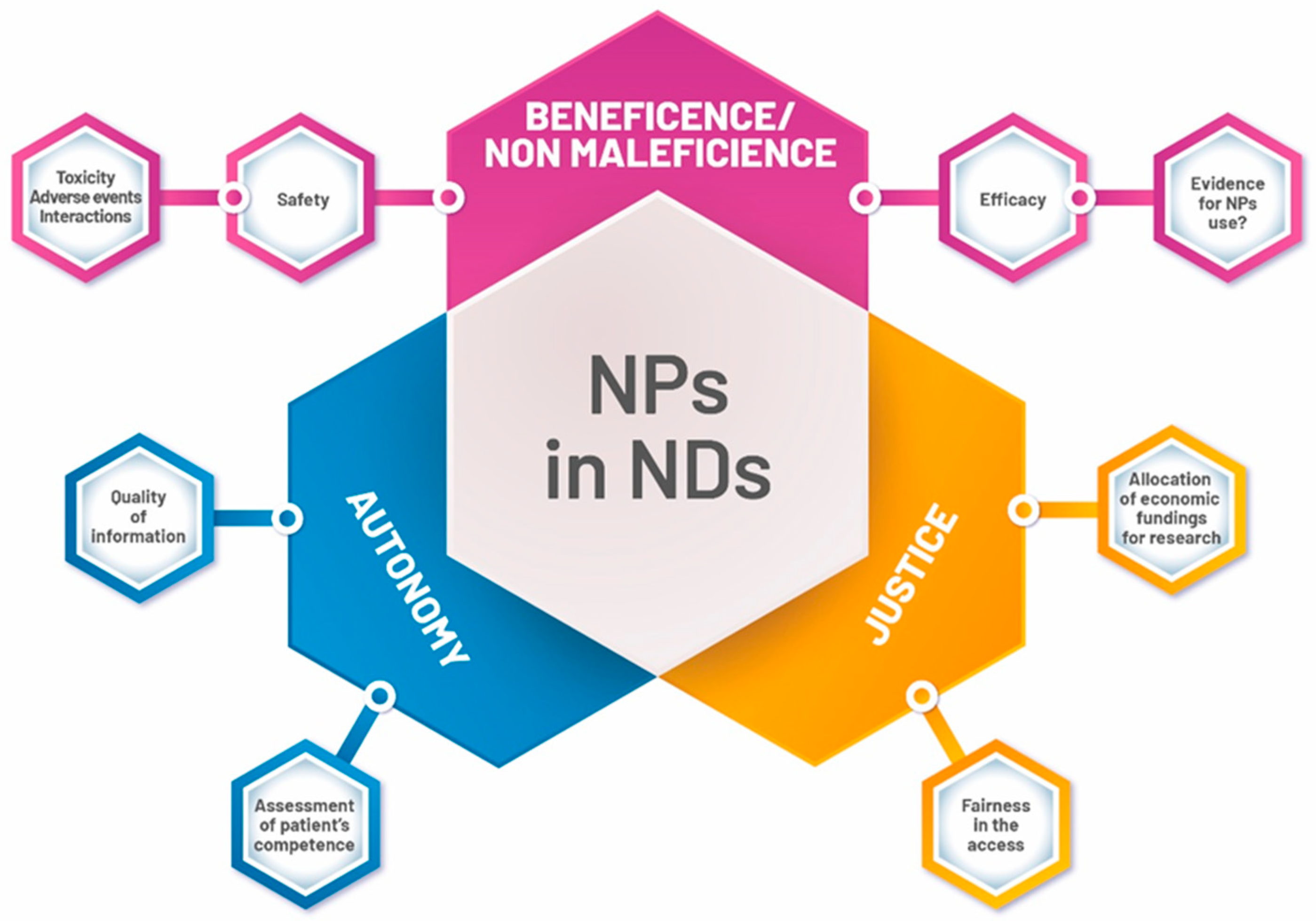
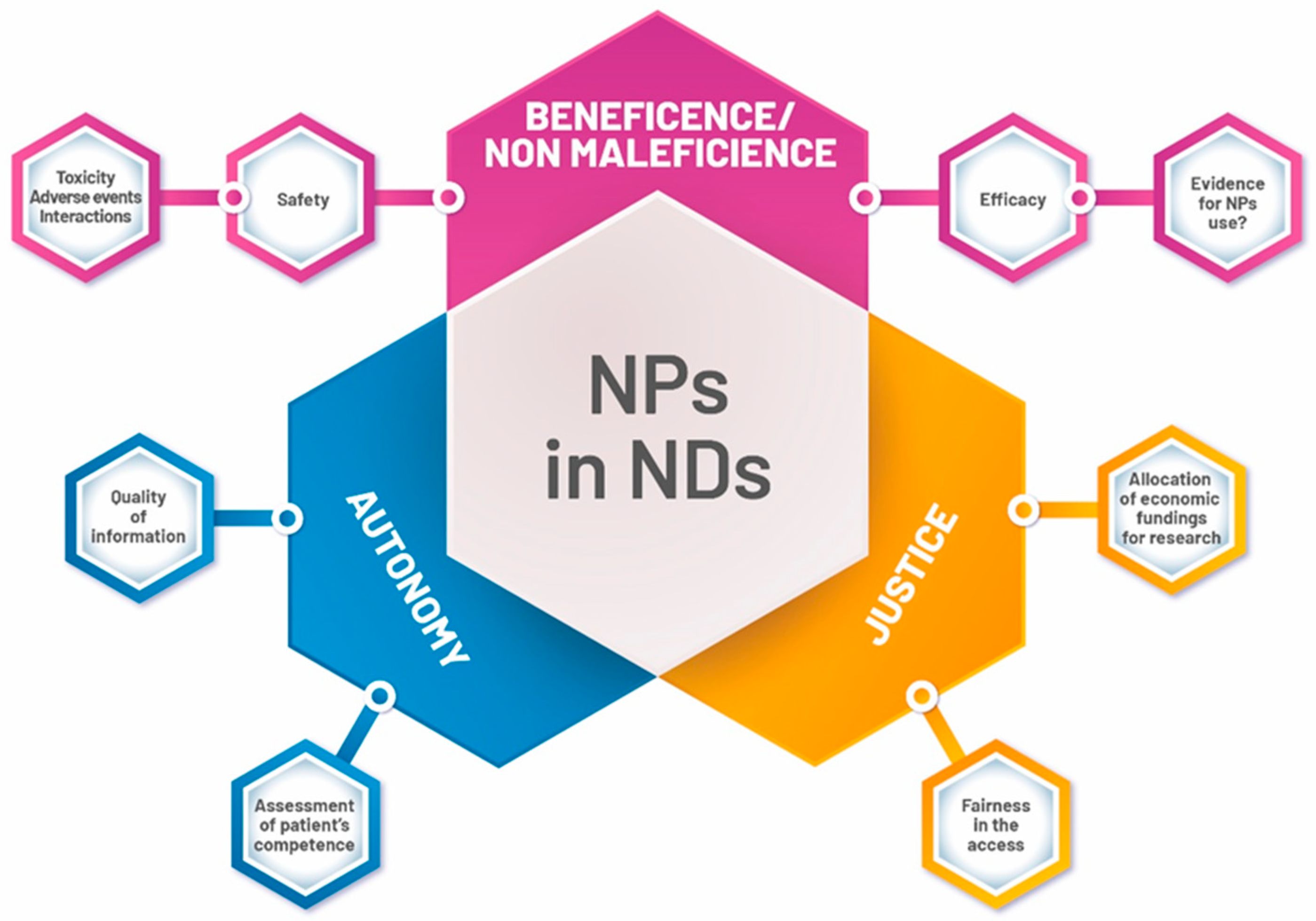
3.2. Beneficence/Nonmaleficence/Justice
4. Medical Liability Scenarios
5. Concluding Remarks
Author Contributions
Conflicts of Interest
References
- Heemels, M.T. Neurodegenerative diseases. Nature 2016, 539, 179. [Google Scholar] [CrossRef] [PubMed]
- GBD. 2015 Neurological Disorders Collaborator Group. Global, regional, and national burden of neurological disorders during 1990-2015: A systematic analysis for the global burden of disease study 2015. Lancet Neurol. 2017, 16, 877–897. [Google Scholar] [CrossRef]
- Hung, C.-W.; Chen, Y.-C.; Hsieh, W.-L.; Chiou, S.-H.; Kao, C.-L. Ageing and neurodegenerative diseases. Ageing Res. Rev. 2010, 9, S36–S46. [Google Scholar] [CrossRef] [PubMed]
- Burgunder, J.M. Neurodegeneration. IUBMB Life 2003, 55, 291. [Google Scholar] [CrossRef] [PubMed]
- Erkkinen, M.G.; Kim, M.O.; Geschwind, M.D. Clinical Neurology and Epidemiology of the Major Neurodegenerative Diseases. Cold Spring Harb. Perspect. Biol. 2018, 10, a033118. [Google Scholar] [CrossRef] [PubMed]
- Katsnelson, A.; De Strooper, B.; Zoghbi, H.Y. Neurodegeneration: From cellular concepts to clinical applications. Sci. Transl. Med. 2016, 8, 364ps18. [Google Scholar] [CrossRef]
- Ekor, M. The growing use of herbal medicines: Issues relating to adverse reactions and challenges in monitoring safety. Front. Pharmacol. 2013, 4, 177. [Google Scholar] [CrossRef]
- Bandaranayake, W.M. Quality control, screening, toxicity, and regulation of herbal drugs. In Modern Phytomeicine; Turning Medicinal Plants into Drugs; Ahmad, I., Aquil, F., Owains, M., Eds.; Wiley-VCH GmbH & Co. KGaA: Weinheim, Germany, 2008; pp. 25–27. [Google Scholar]
- Dubey, S.K.; Singhvi, G.; Krishna, K.V.; Agnihotri, T.; Saha, R.N.; Gupta, G.; Agnihitri, T. Herbal Medicines in Neurodegenerative Disorders: An Evolutionary Approach through Novel Drug Delivery System. J. Environ. Pathol. Toxicol. Oncol. 2018, 37, 199–208. [Google Scholar] [CrossRef]
- Parvez, M.K. Natural or Plant Products for the Treatment of Neurological Disorders: Current Knowledge. Curr. Drug Metab. 2018, 19, 424–428. [Google Scholar] [CrossRef]
- Ernst, E.; Cohen, M.H.; Stone, J. Ethical problems arising in evidence based complementary and alternative medicine. J. Med. Ethics 2004, 30, 156–159. [Google Scholar] [CrossRef]
- Kim, H.J.; Jeon, B.; Chung, S.J. Professional ethics in complementary and alternative medicines in management of Parkinson’s disease. J. Park. Dis. 2016, 6, 675–683. [Google Scholar] [CrossRef] [PubMed]
- Beauchamp, T.; Childress, J. Principles of Biomedical Ethics, 5th ed.; Oxford University Press: New York, NY, USA, 2001. [Google Scholar]
- Dadhania, V.P.; Trivedi, P.P.; Vikram, A.; Tripathi, D.N. Nutraceuticals against Neurodegeneration: A Mechanistic Insight. Curr. Neuropharmacol. 2016, 14, 627–640. [Google Scholar] [CrossRef] [PubMed]
- Durrenberger, P.F.; Fernando, F.S.; Kashefi, S.N.; Bonnert, T.P.; Seilhean, D.; Nait-Oumesmar, B.; Schmitt, A.; Gebicke-Haerter, P.J.; Falkai, P.; Grünblatt, E.; et al. Common mechanisms in neurodegeneration and neuroinflammation: A BrainNet Europe gene expression microarray study. J. Neural Transm. (Vienna) 2015, 122, 1055–1068. [Google Scholar] [CrossRef] [PubMed]
- Rasool, M.; Malik, A.; Qureshi, M.S.; Manan, A.; Pushparaj, P.N.; Asif, M.; Qazi, M.H.; Qazi, A.M.; Kamal, M.A.; Gan, S.H.; et al. Recent Updates in the Treatment of Neurodegenerative Disorders Using Natural Compounds. Evid. Based Complement. Altern. Med. 2014, 2014, 97973. [Google Scholar] [CrossRef]
- Srivastava, P.; Yadav, R.S. Efficacy of Natural Compounds in Neurodegenerative Disorders. In Glutamate and ATP at the Interface of Metabolism and Signaling in the Brain; Springer Science and Business Media LLC: Berlin, Germany, 2016; Volume 12, pp. 107–123. [Google Scholar]
- Lökk, J.; Nilsson, M. Frequency, type and factors associated with the use of complementary and alternative medicine in patients with Parkinson’s disease at a neurological outpatient clinic. Parkinsonism Relat. Disord. 2010, 16, 540–544. [Google Scholar] [CrossRef]
- Shan, C.S.; Zhang, H.F.; Xu, Q.Q.; Shi, Y.H.; Wang, Y.; Li, Y.; Lin, Y.; Zheng, G.Q. Herbal Medicine Formulas for Parkinson’s Disease: A Systematic Review and Meta-Analysis of Randomized Double-Blind Placebo-Controlled Clinical Trials. Front. Aging Neurosci. 2018, 10, 349. [Google Scholar] [CrossRef]
- Panda, S.S.; Jhanji, N. Natural Products as Potential anti-Alzheimer Agents. Curr. Med. Chem. 2018. [Google Scholar] [CrossRef]
- Leonoudakis, D.; Rane, A.; Angeli, S.; Lithgow, G.J.; Andersen, J.K.; Chinta, S.J. Anti-Inflammatory and Neuroprotective Role of Natural Product Securinine in Activated Glial Cells: Implications for Parkinson’s Disease. Mediat. Inflamm. 2017, 2017, 8302636. [Google Scholar] [CrossRef]
- Bagli, E.; Goussia, A.; Moschos, M.M.; Agnantis, N.; Kitsos, G. Natural Compounds and Neuroprotection: Mechanisms of Action and Novel Delivery Systems. In Vivo 2016, 30, 535–547. [Google Scholar]
- Starkov, A.A.; Beal, F.M. Portal to Alzheimer’s disease. Nat. Med. 2008, 14, 1020–1021. [Google Scholar] [CrossRef]
- Venkatesan, R.; Ji, E.; Kim, S.Y. Phytochemicals That Regulate Neurodegenerative Disease by Targeting Neurotrophins: A Comprehensive Review. Biomed Res. Int. 2015, 2015, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, P.; Gogia, N.; Singh, A. Exploring the efficacy of natural products in alleviating Alzheimer’s disease. Neural Regen. Res. 2019, 14, 1321–1329. [Google Scholar] [PubMed]
- Wollen, K.A. Alzheimer’s disease: The pros and cons of pharmaceutical, nutritional, botanical, and stimulatory therapies, with a discussion of treatment strategies from the perspective of patients and practitioners. Altern. Med. Rev. 2010, 15, 223–244. [Google Scholar] [PubMed]
- Cicero, A.F.; Ruscica, M.; Banach, M. Resveratrol and cognitive decline: A clinician perspective. Arch. Med. Sci. 2019, 15, 936–943. [Google Scholar] [CrossRef] [PubMed]
- Castelli, V.; Grassi, D.; Bocale, R.; d’Angelo, M.; Antonosante, A.; Cimini, A.; Ferri, C.; Desideri, G. Diet and Brain Health: Which Role for Polyphenols? Curr. Pharm. Des. 2018, 24, 227–238. [Google Scholar] [CrossRef] [PubMed]
- Barry, A.R. Patients’ perceptions and use of natural health products. Can. Pharm. J. 2018, 151, 254–262. [Google Scholar] [CrossRef]
- Karimi, A.; Majlesi, M.; Rafieian-Kopaei, M. Herbal versus synthetic drugs; beliefs and facts. J. Nephropharmacol. 2015, 4, 27–30. [Google Scholar]
- Khazdair, M.R.; Anaeigoudari, A.; Hashemzehi, M.; Mohebbati, R. Neuroprotective potency of some spice herbs, a literature review. J. Tradit. Complement. Med. 2018, 9, 98–105. [Google Scholar] [CrossRef]
- Coimbra, M.; Isacchi, B.; Van Bloois, L.; Toraño, J.S.; Ket, A.; Wu, X.; Broere, F.; Metselaar, J.M.; Rijcken, C.J.; Storm, G.; et al. Improving solubility and chemical stability of natural compounds for medicinal use by incorporation into liposomes. Int. J. Pharm. 2011, 416, 433–442. [Google Scholar] [CrossRef]
- Shoji, Y.; Nakashima, H. Nutraceutics and delivery systems. J. Drug Target. 2004, 12, 385–391. [Google Scholar] [CrossRef]
- Van Der Schyf, C.J.; Geldenhuys, W.J.; Youdim, M.B.H. Multifunctional drugs with different CNS targets for neuropsychiatric disorders. J. Neurochem. 2006, 99, 1033–1048. [Google Scholar] [CrossRef]
- Pohl, F.; Kong Thoo Lin, P. The Potential Use of Plant Natural Products and Plant Extracts with Antioxidant Properties for the Prevention/Treatment of Neurodegenerative Diseases: In Vitro, In Vivo and Clinical Trials. Molecules 2018, 23, 3283. [Google Scholar] [CrossRef]
- Parveen, A.; Parveen, B.; Parveen, R.; Ahmad, S. Challenges and guidelines for clinical trial of herbal drugs. J. Pharm. Bioallied Sci. 2015, 7, 329–333. [Google Scholar]
- Cicero, A.F.G.; Fogacci, F.; Banach, M. Botanicals and phytochemicals active on cognitive decline: The clinical evidence. Pharmacol. Res. 2018, 130, 204–212. [Google Scholar] [CrossRef]
- Cicero, A.F.; Bove, M.; Colletti, A.; Rizzo, M.; Fogacci, F.; Giovannini, M.; Borghi, C. Short-Term Impact of a Combined Nutraceutical on Cognitive Function, Perceived Stress and Depression in Young Elderly with Cognitive Impairment: A Pilot, Double-Blind, Randomized Clinical Trial. Alzheimers Dis. 2017, 4, 12–15. [Google Scholar]
- Kemper, K.J.; Vohra, S.; Walls, R. Task Force on Complementary and Alternative Medicine; Provisional Section on Complementary, Holistic, and Integrative Medicine. American Academy of Pediatrics. The use of complementary and alternative medicine in pediatrics. Pediatrics 2008, 122, 1374–1386. [Google Scholar] [CrossRef]
- Abdel-Tawab, M. Do We Need Plant Food Supplements? A Critical Examination of Quality, Safety, Efficacy, and Necessity for a New Regulatory Framework. Planta Med. 2018, 84, 372–393. [Google Scholar] [CrossRef]
- Heinrich, M. Quality and safety of herbal medical products: Regulation and the need for quality assurance along the value chains. Br. J. Clin. Pharmacol. 2015, 80, 62–66. [Google Scholar] [CrossRef]
- Manoharan, S.; Essa, M.M.; Vinoth, A.; Kowsalya, R.; Manimaran, A.; Selvasundaram, R. Alzheimer’s Disease and Medicinal Plants: An Overview. Adv. Neurobiol. 2016, 12, 95–105. [Google Scholar]
- Young, R. Informed consent and patient autonomy. Chapter 42. In A Companion to Bioethics; Khuse, H., Singer, P., Eds.; Blackwell Publishing Ltd: Hoboken, NJ, USA, 2009; p. 442. [Google Scholar]
- White, A.; Boon, H.; Alraek, T.; Lewith, G.; Liu, J.P.; Norheim, A.J.; Steinsbekk, A.; Yamashita, H.; Fønnebø, V. Reducing the risk of complementary and alternative medicine (CAM): Challenges and priorities. J. Integr. Med. 2014, 6, 404–408. [Google Scholar] [CrossRef]
- Chatfield, K.; Salehi, B.; Sharifi-Rad, J.; Afshar, L. Applying an Ethical Framework to Herbal Medicine. Evid. Based Complement. Altern. Med. 2018, 2018, 1903629. [Google Scholar] [CrossRef]
- Barnes, J.; Mills, S.Y.; Abbot, N.C.; Willoughby, M.; Ernst, E. Different standards for reporting ADRs to herbal remedies and conventional OTC medicines: Face-to-face interviews with 515 users of herbal remedies. Br. J. Clin. Pharmacol. 1998, 45, 496–500. [Google Scholar] [CrossRef]
- Ernst, E. Risks of herbal medicinal products. Pharmacoepidemiol. Drug Saf. 2004, 13, 767–771. [Google Scholar] [CrossRef]
- Shahvisi, A. No Understanding, No Consent: The Case Against Alternative Medicine. Bioethics 2016, 30, 69–76. [Google Scholar] [CrossRef]
- Entwistle, V.A.; Watt, I.S. Treating Patients as Persons: A Capabilities Approach to Support Delivery of Person-Centered Care. Am. J. Bioeth. 2013, 13, 29–39. [Google Scholar] [CrossRef] [Green Version]
- Epstein, R.M. The ambiguity of personhood. Am. J. Bioeth. 2013, 13, 42–44. [Google Scholar] [CrossRef]
- Ernst, E. Ethics of complementary medicine: Practical issues. Br. J. Gen. Pract. 2009, 59, 517–519. [Google Scholar] [CrossRef]
- Fields, L.M.; Calvert, J.D. Informed consent procedures with cognitively impaired patients: A review of ethics and best practices. Psychiatry Clin. Neurosci. 2015, 69, 462–471. [Google Scholar] [CrossRef]
- Dunn, L.B.; Alici, Y.; Roberts, L.W. Ethical Challenges in the Treatment of Cognitive Impairment in Aging. Curr. Behav. Neurosci. Rep. 2015, 2, 226–233. [Google Scholar] [CrossRef] [Green Version]
- Moye, J.; Karel, M.J.; Azar, A.R.; Gurrera, R.J. Capacity to consent to treatment: Empirical comparison of three instruments in older adults with and without dementia. Gerontologist 2004, 44, 166–175. [Google Scholar] [CrossRef]
- Appelbaum, P.S. Clinical practice. Assessment of patients’ competence to consent to treatment. N. Engl. J. Med. 2007, 357, 1834–1840. [Google Scholar] [CrossRef]
- Nissen, N.; Weidenhammer, W.; Schunder-Tatzber, S.; Johannessen, H. Public health ethics for complementary and alternative medicine. Eur. J. Integr. Med. 2013, 5, 62–67. [Google Scholar] [CrossRef]
- Hegyi, G.; Petri, R.P., Jr.; di Sarsina, P.R.; Niemtzow, R.C. Overview of Integrative Medicine Practices and Policies in NATO Participant Countries. Med. Acupunct. 2015, 27, 318–327. [Google Scholar] [CrossRef] [Green Version]
- von Ammon, K.; Cardini, F.; Daig, U.; Dragan, S.; FreiErb, M.; Hegyi, G.; Roberti di Sarsina, P.; Sørensen, J.; Ursoniu, S.; Weidenhammer, W.; et al. Health Technology Assessment (HTA) and a Map of CAM Provision in the EU: Final Report of CAMbrella Work Package No. 5. 2012. Available online: Phaidra.univie.ac.at/detail_object/o:300096 (accessed on 31 August 2019).
- Ong, C.K.; Petersen, S.; Bodeker, G.C.; Stewart-Brown, S. Health status of people using complementary and alternative medical practitioner services in 4 English counties. Am. J. Public Health 2002, 92, 1653–1656. [Google Scholar] [CrossRef]
- Bodeker, G.; Kronenberg, F. A Public Health Agenda for Traditional, Complementary, and Alternative Medicine. Am. J. Public Health 2002, 92, 1582–1591. [Google Scholar] [CrossRef] [PubMed]
- White House Commission on Complementary and Alternative Medicine Policy; Final Report; March 2002. Available online: http://www.whccamp.hhs.gov/finalreport.html (accessed on 31 August 2019).
- Nahin, R.L.; Nahin, R.; Straus, S.E. Research into complementary and alternative medicine: Problems and potential. BMJ 2001, 322, 161–164. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.H. Complementary & Alternative Medicine: Legal Boundaries and Regulatory Perspectives; Johns Hopkins University Press: Baltimore, MD, USA, 1998. [Google Scholar]
- Raposo, V.L. Complementary and alternative medicine, medical liability and the proper standard of care. Complement. Ther. Clin. Pract. 2019, 35, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Moffett, P.; Moore, G. The Standard of Care: Legal History and Definitions: The Bad and Good News. West. J. Emerg. Med. 2011, 12, 109–112. [Google Scholar] [PubMed]
- Gilmour, J.; Harrison, C.; Asadi, L.; Cohen, M.H.; Vohra, S. Complementary and alternative medicine practitioners’ standard of care: Responsibilities to patients and parents. Pediatrics 2011, 128 (Suppl. S4), S200–S205. [Google Scholar] [CrossRef]
- Cohen, M.H.; Eisenberg, D.M. Potential physician malpractice liability associated with complementary and integrative medical therapies. Ann. Intern. Med. 2002, 136, 596–603. [Google Scholar] [CrossRef]
- Girard, L.; Vohra, S. Ethics of Using Herbal Medicine as Primary or Adjunct Treatment and Issues of Drug–Herb Interaction. Chapter 21. In Herbal Medicine: Biomolecular and Clinical Aspects, 2nd ed.; Benzie, I.F.F., Wachtel-Galor, S., Eds.; CRC Press/Taylor & Francis: Boca Raton, FL, USA, 2011. [Google Scholar]
- Cohen, M.H. Legal issues in caring for patients with kidney disease by selectively integrating complementary therapies. Adv. Chronic Kidney Dis. 2005, 12, 300–311. [Google Scholar] [CrossRef]
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Paolo, M.; Papi, L.; Gori, F.; Turillazzi, E. Natural Products in Neurodegenerative Diseases: A Great Promise but an Ethical Challenge. Int. J. Mol. Sci. 2019, 20, 5170. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20205170
Di Paolo M, Papi L, Gori F, Turillazzi E. Natural Products in Neurodegenerative Diseases: A Great Promise but an Ethical Challenge. International Journal of Molecular Sciences. 2019; 20(20):5170. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20205170
Chicago/Turabian StyleDi Paolo, Marco, Luigi Papi, Federica Gori, and Emanuela Turillazzi. 2019. "Natural Products in Neurodegenerative Diseases: A Great Promise but an Ethical Challenge" International Journal of Molecular Sciences 20, no. 20: 5170. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20205170