VEGF-A and ICAM-1 Gene Polymorphisms as Predictors of Clinical Outcome to First-Line Bevacizumab-Based Treatment in Metastatic Colorectal Cancer


 , ,
, ,
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Design
4.2. Pharmacogenetic Analyses
4.3. Statistics and Data Analysis
Author Contributions
Funding
Conflicts of Interest
References
- Folkman, J. Tumor angiogenesis: Therapeutic implications. N. Engl. J. Med. 1971, 285, 1182–1186. [Google Scholar]
- Hicklin, D.J.; Ellis, L.M. Role of the vascular endothelial growth factor pathway in tumor growth and angiogenesis. J. Clin. Oncol. 2005, 23, 1011–1027. [Google Scholar] [CrossRef] [PubMed]
- Ellis, L.M.; Hicklin, D.J. VEGF-targeted therapy: Mechanisms of anti-tumor activity. Nat. Rev. Cancer 2008, 8, 579–591. [Google Scholar] [CrossRef] [PubMed]
- Nagy, J.A.; Vasile, E.; Feng, D.; Sundberg, C.; Brown, L.F.; Detmar, M.J.; Lawitts, J.A.; Benjamin, L.; Tan, X.; Manseau, E.J.; et al. Vascular permeability factor/vascular endothelial growth factor induces lymphangiogenesis as well as angiogenesis. J. Exp. Med. 2002, 196, 1497–1506. [Google Scholar] [CrossRef] [PubMed]
- Kerbel, R.S. Tumor angiogenesis. N. Engl. J. Med. 2008, 358, 2039–2049. [Google Scholar] [CrossRef] [PubMed]
- Hubbard, A.K.; Rothlein, R. Intercellular adhesion molecule-1 (ICAM-1) expression and cell signaling cascades. Free Radic. Biol. Med. 2000, 28, 1379–1386. [Google Scholar] [CrossRef]
- Brooks, K.J.; Coleman, E.J.; Vitetta, E.S. The antitumor activity of an anti-CD54 antibody in SCID mice xenografted with human breast, prostate, non-small cell lung, and pancreatic tumor cell lines. Int. J. Cancer 2008, 123, 2438–2445. [Google Scholar] [CrossRef] [PubMed]
- Werther, K.; Christensen, I.J.; Brünner, N.; Nielsen, H.J. Soluble vascular endothelial growth factor levels in patients with primary colorectal carcinoma. The Danish RANX05 Colorectal Cancer Study Group. Eur. J. Surg. Oncol. 2000, 26, 657–662. [Google Scholar] [CrossRef] [PubMed]
- Broll, R.; Erdmann, H.; Duchrow, M.; Oevermann, E.; Schwandner, O.; Markert, U.; Bruch, H.; Windhövel, U. Vascular endothelial growth factor (VEGF)-a valuable serum tumour marker in patients with colorectal cancer? Eur. J. Surg. Oncol. 2001, 27, 37–42. [Google Scholar] [CrossRef]
- Salgia, R. Prognostic significance of angiogenesis and angiogenic growth factors in nonsmall cell lung cancer. Cancer 2011, 117, 3889–3899. [Google Scholar] [CrossRef]
- Karayiannakis, A.J.; Syrigos, K.N.; Polychronidis, A.; Zbar, A.; Kouraklis, G.; Simopoulos, C.; Karatzas, G. Circulating VEGF levels in the serum of gastric cancer patients: Correlation with pathological variables, patient survival, and tumor surgery. Ann. Surg. 2002, 236, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Karayiannakis, A.J.; Bolanaki, H.; Syrigos, K.N.; Asimakopoulos, B.; Polychronidis, A.; Anagnostoulis, S.; Simopoulos, C. Serum vascular endothelial growth factor levels in pancreatic cancer patients correlate with advanced and metastatic disease and poor prognosis. Cancer Lett. 2002, 194, 119–124. [Google Scholar] [CrossRef]
- Piao, Y.; Henry, V.; Tiao, N.; Park, S.Y.; Martinez-Ledesma, J.; Dong, J.W.; Balasubramaniyan, V.; De Groot, J.F. Targeting intercellular adhesion molecule-1 prolongs survival in mice bearing bevacizumab-resistant glioblastoma. Oncotarget 2017, 8, 96970–96983. [Google Scholar] [CrossRef] [PubMed]
- Global Burden of Disease Cancer Collaboration; Fitzmaurice, C.; Allen, C.; Barber, R.M.; Barregard, L.; Bhutta, Z.A.; Brenner, H.; Dicker, D.J.; Chimed-Orchir, O.; Dandona, R.; et al. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived with Disability, and Disability-Adjusted Life-years for 32 Cancer Groups, 1990 to 2015: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 2017, 3, 524–548. [Google Scholar] [PubMed]
- Yoon, H.H.; Tougeron, D.; Shi, Q.; Alberts, S.R.; Mahoney, M.R.; Nelson, G.D.; Nair, S.G.; Thibodeau, S.N.; Goldberg, R.M.; Sargent, D.J.; et al. KRAS codon 12 and 13 mutations in relation to disease-free survival in BRAF-wild-type stage III colon cancers from an adjuvant chemotherapy trial (N0147 alliance). Clin. Cancer Res. 2014, 20, 3033–3043. [Google Scholar] [CrossRef]
- Modest, D.P.; Ricard, I.; Heinemann, V.; Hegewisch-Becker, S.; Schmiegel, W.; Porschen, R.; Stintzing, S.; Graeven, U.; Arnold, D.; Von Weikersthal, L.F.; et al. Outcome according to KRAS-, NRAS- and BRAF-mutation as well as KRAS mutation variants: Pooled analysis of five randomized trials in metastatic colorectal cancer by the AIO colorectal cancer study group. Ann. Oncol. 2016, 27, 1746–1753. [Google Scholar] [CrossRef]
- Avastin SmPC, EMC. Available online: https://www.medicines.org.uk/emc/product/3885/smpc (accessed on 10 July 2018).
- Gerber, H.P.; Ferrara, N. Pharmacology and pharmacodynamics of bevacizumab as monotherapy or in combination with cytotoxic therapy in preclinical studies. Cancer Res. 2005, 65, 671–680. [Google Scholar]
- Hayes, D.F. Bevacizumab treatment for solid tumors: Boon or bust? JAMA 2011, 305, 506–508. [Google Scholar] [CrossRef]
- De Stefano, A.; Carlomagno, C.; Pepe, S.; Bianco, R.; De Placido, S. Bevacizumab-related arterial hypertension as a predictive marker in metastatic colorectal cancer patients. Cancer Chemother. Pharmacol. 2011, 68, 1207–1213. [Google Scholar] [CrossRef]
- Dowlati, A.; Gray, R.; Sandler, A.B.; Schiller, J.H.; Johnson, D.H. Cell Adhesion Molecules, Vascular Endothelial Growth Factor, and Basic Fibroblast Growth Factor in Patients with Non-Small Cell Lung Cancer Treated with Chemotherapy with or without Bevacizumab an Eastern Cooperative Oncology Group Study. Clin. Cancer Res. 2008, 14, 1407–1412. [Google Scholar] [CrossRef]
- Sathornsumetee, S.; Cao, Y.; Marcello, J.E.; Herndon, J.E.; McLendon, R.E.; Desjardins, A.; Friedman, H.S.; Dewhirst, M.W.; Vredenburgh, J.J.; Rich, J.N. Tumor Angiogenic and Hypoxic Profiles Predict Radiographic Response and Survival in Malignant Astrocytoma Patients Treated with Bevacizumab and Irinotecan. J. Clin. Oncol. 2008, 26, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Loupakis, F.; Cremolini, C.; Yang, D.; Salvatore, L.; Zhang, W.; Wakatsuki, T.; Bohanes, P.; Schirripa, M.; Benhaim, L.; Lonardi, S.; et al. Prospective validation of candidate SNPs of VEGF/VEGFR pathway in metastatic colorectal cancer patients treated with first-line FOLFIRI plus bevacizumab. PLoS ONE 2013, 8, e66774. [Google Scholar] [CrossRef] [PubMed]
- Ulivi, P.; Scarpi, E.; Passardi, A.; Marisi, G.; Calistri, D.; Zoli, W.; Del Re, M.; Frassineti, G.L.; Tassinari, D.; Tamberi, S.; et al. eNOS polymorphisms as predictors of efficacy of bevacizumab-based chemotherapy in metastatic colorectal cancer: Data from a randomized clinical trial. J. Transl. Med. 2015, 13, 258–268. [Google Scholar] [CrossRef] [PubMed]
- Di Salvatore, M.; Giudice, L.L.; Rossi, E.; Santonocito, C.; Nazzicone, G.; Rodriquenz, M.G.; Cappuccio, S.; Inno, A.; Fuso, P.; Orlandi, A.; et al. Association of IL-8 and eNOS polymorphisms with clinical outcomes in bevacizumab-treated breast cancer patients: An exploratory analysis. Clin. Transl. Oncol. 2016, 18, 40–46. [Google Scholar] [CrossRef]
- Gerger, A.; El-Khoueiry, A.; Zhang, W.; Yang, D.; Singh, H.; Bohanes, P.; Ning, Y.; Winder, T.; LaBonte, M.J.; Wilson, P.M.; et al. Pharmacogenetic angiogenesis profiling for first-line Bevacizumab plus oxaliplatin-based chemotherapy in patients with metastatic colorectal cancer. Clin. Cancer Res. 2011, 17, 5783–5792. [Google Scholar] [CrossRef]
- Panoilia, E.; Schindler, E.; Samantas, E.; Aravantinos, G.; Kalofonos, H.P.; Christodoulou, C.; Patrinos, G.P.; Friberg, L.E.; Sivolapenko, G. A pharmacokinetic binding model for bevacizumab and VEGF165 in colorectal cancer patients. Cancer Chemother. Pharm. 2015, 75, 791–803. [Google Scholar] [CrossRef]
- Koutras, A.K.; Antonacopoulou, A.G.; Eleftheraki, A.G.; Dimitrakopoulos, F.I.; Koumarianou, A.; Varthalitis, I.; Fostira, F.; Sgouros, J.; Briasoulis, E.; Bournakis, E.; et al. Vascular endothelial growth factor polymorphisms and clinical outcome in colorectal cancer patients treated with irinotecan-based chemotherapy and bevacizumab. Pharm. J. 2012, 12, 468–475. [Google Scholar] [CrossRef]
- Schneider, B.P.; Wang, M.; Radovich, M.; Sledge, G.W.; Badve, S.; Thor, A.; Flockhart, D.A.; Hancock, B.; Davidson, N.; Gralow, J.; et al. Association of vascular endothelial growth factor and vascular endothelial growth factor receptor-2 genetic polymorphisms with outcome in a trial of paclitaxel compared with paclitaxel plus bevacizumab in advanced breast cancer: ECOG 2100. J. Clin. Oncol. 2008, 26, 4672–4678. [Google Scholar] [CrossRef]
- Galanis, E.; Anderson, S.K.; Lafky, J.M.; Uhm, J.H.; Giannini, C.; Kumar, S.K.; Kimlinger, T.K.; Northfelt, D.W.; Flynn, P.J.; Jaeckle, K.A.; et al. Phase II study of bevacizumab in combination with sorafenib in recurrent glioblastoma (N0776): A north central cancer treatment group trial. Clin. Cancer Res. 2013, 19, 4816–4823. [Google Scholar] [CrossRef]
- Etienne-Grimaldi, M.; Formento, P.; Degeorges, A.; Pierga, J.-Y.; Delva, R.; Pivot, X.; Dalenc, F.; Espié, M.; Veyret, C.; Formento, J.-L.; et al. Prospective analysis of the impact of VEGF-A gene polymorphisms on the pharmacodynamics of bevacizumab-based therapy in metastatic breast cancer patients. Br. J. Clin. Pharmacol. 2011, 71, 921–928. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Okamoto, W.; Makiyama, A.; Shitara, K.; Denda, T.; Ogura, T.; Nakano, Y.; Nishina, T.; Komoda, M.; Hara, H.; et al. Plasma ICAM-1 (pICAM-1) and plasma IL-8 (pIL-8) level as biomarker of metastatic colorectal cancer patients (mCRC) treated with mFOLFOX6/XELOX plus bevacizumab (BV) (WJOG7612GTR). J. Clin. Oncol. 2018, 36, 670. [Google Scholar] [CrossRef]
- Horn, L.; Dahlberg, S.E.; Sandler, A.B.; Dowlati, A.; Moore, D.F.; Murren, J.R.; Schiller, J.H. Phase II Study of Cisplatin Plus Etoposide and Bevacizumab for Previously Untreated, Extensive-Stage Small-Cell Lung Cancer: Eastern Cooperative Oncology Group Study E3501. J. Clin. Oncol. 2009, 27, 6006–6011. [Google Scholar] [CrossRef] [PubMed]
- Mok, T.; Gorbunova, V.; Juhász, E.; Szima, B.; Burdaeva, O.; Orlov, S.; Yu, C.-J.; Archer, V.; Hilton, M.; Delmar, P.; et al. A correlative biomarker analysis of the combination of bevacizumab and carboplatin-based chemotherapy for advanced nonsquamous non-small-cell lung cancer: Results of the phase II randomized ABIGAIL study (BO21015). J. Thorac. Oncol. 2014, 9, 848–855. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, V.K.; Overman, M.J.; Jiang, Z.-Q.; Garrett, C.; Agarwal, S.; Eng, C.; Kee, B.; Fogelman, D.; Dasari, A.; Wolff, R.; et al. Progression-free survival remains poor over sequential lines of systemic therapy in patients with BRAF-mutated colorectal cancer. Clin. Colorectal Cancer 2014, 13, 164–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruera, G.; Pepe, F.; Malapelle, U.; Pisapia, P.; Mas, A.D.; Di Giacomo, D.; Calvisi, G.; Troncone, G.; Ricevuto, E. KRAS, NRAS and BRAF mutations detected by next generation sequencing, and differential clinical outcome in metastatic colorectal cancer (MCRC) patients treated with first line FIr-B/FOx adding bevacizumab (BEV) to triplet chemotherapy. Oncotarget 2018, 9, 26279–26290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tol, J.; Nagtegaal, I.D.; Punt, C.J. BRAF mutation in metastatic colorectal cancer. N. Engl. J. Med. 2009, 361, 98–99. [Google Scholar] [CrossRef] [Green Version]
- Ince, W.L.; Jubb, A.M.; Holden, S.N.; Holmgren, E.B.; Tobin, P.; Sridhar, M.; Hurwitz, H.I.; Kabbinavar, F.; Novotny, W.F.; Hillan, K.J.; et al. Association of k-ras, b-raf, and p53 status with the treatment effect of bevacizumab. J. Natl. Cancer Inst. 2005, 97, 981–989. [Google Scholar] [CrossRef]
- Price, T.J.; Hardingham, J.E.; Lee, C.K.; Weickhardt, A.; Townsend, A.R.; Wrin, J.W.; Chua, A.; Shivasami, A.; Cummins, M.M.; Murone, C.; et al. Impact of KRAS and BRAF gene mutation status on outcomes from the phase III AGITG MAX trial of capecitabine alone or in combination with bevacizumab and mitomycin in advanced colorectal cancer. J. Clin. Oncol. 2011, 29, 2675–2682. [Google Scholar] [CrossRef]
- Price, T.J.; A Bruhn, M.; Lee, C.K.; E Hardingham, J.; Townsend, A.R.; Mann, K.P.; Simes, J.; Weickhardt, A.; Wrin, J.W.; Wilson, K.; et al. Correlation of extended RAS and PIK3CA gene mutation status with outcomes from the phase III AGITG MAX STUDY involving capecitabine alone or in combination with bevacizumab plus or minus mitomycin C in advanced colorectal cancer. Br. J. Cancer 2015, 112, 963–970. [Google Scholar] [CrossRef]
- Hurwitz, H.I.; Yi, J.; Ince, W.; Novotny, W.F.; Rosen, O. The clinical benefit of bevacizumab in metastatic colorectal cancer is independent of K-ras mutation status: Analysis of a phase III study of bevacizumab with chemotherapy in previously untreated metastatic colorectal cancer. Oncologist 2009, 14, 22–28. [Google Scholar] [CrossRef] [Green Version]
- DNA Sequencing by Capillary Electrophoresis. Applied Biosystems Chemistry Guide, 2nd Edition. Available online: https://tools.thermofisher.com/content/sfs/manuals/cms_041003.pdf (accessed on 9 May 2015).
- Simen, B.B.; Yin, L.; Goswami, C.P.; Davis, K.O.; Bajaj, R.; Gong, J.Z.; Peiper, S.C.; Johnson, E.S.; Wang, Z.-X. Validation of a next-generation-sequencing cancer panel for use in the clinical laboratory. Arch. Pathol. Lab. Med. 2015, 139, 508–517. [Google Scholar] [CrossRef] [PubMed]
- Tops, B.B.J.; Normanno, N.; Kurth, H.; Amato, E.; Mafficini, A.; Rieber, N.; Le Corre, D.; Rachiglio, A.M.; Reiman, A.; Sheils, O.; et al. Development of a semi-conductor sequencing-based panel for genotyping of colon and lung cancer by the Onconetwork consortium. BMC Cancer 2015, 31, 15–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | All Treated Patients (n = 46) |
|---|---|
| Sex, n (%) | |
| Female | 18 (39%) |
| Male | 28 (61%) |
| Age (years), n (%) | |
| <55 | 14 (30%) |
| 55–65 | 12 (26%) |
| >65 | 20 (44%) |
| Metastatic site, n (%) | |
| 1 | 15 (33%) |
| 2 | 12 (26%) |
| >2 | 19 (41%) |
| VEGF rs2010963, n (%) | |
| G/G | 27 (58.7%) |
| G/C | 13 (28.3%) |
| C/C | 6 (13%) |
| VEGF rs1570360, n (%) | |
| G/G | 31 (67.4%) |
| G/A | 10 (21.7%) |
| A/A | 5 (10.9%) |
| VEGF rs699947, n (%) | |
| C/C | 34 (74%) |
| C/A | - |
| A/A | 12 (26%) |
| ICAM rs5498, n (%) | |
| A/A | 13 (28.3%) |
| A/G | 23 (50%) |
| G/G | 10 (21.7%) |
| ICAM rs1799969, n (%) | |
| G/G | 36 (78.3%) |
| G/A | 10 (21.7%) |
| A/A | - |
| KRAS rs61764370, n (%) | |
| Wild type | 12 (50%) |
| Mutant | 12 (50%) |
| NRAS rs11554290, n (%) | |
| Wild type | 9 (38.8%) |
| Mutant | 15 (61.2%) |
| BRAF rs113488022, n (%) | |
| Wild type | 20 (81.8%) |
| Mutant | 4 (18.2%) |
| Treatment Regimens | |
|---|---|
| Initial, n (%) | |
| Bevacizumab-mFOLFOX6 | 22 (48%) |
| Bevacizumab-FOLFIRI | 13 (28%) |
| Bevacizumab-CapOX | 2 (4%) |
| Bevacizumab-CapIRI | 9 (20%) |
| Maintenance, n (%) | |
| Bevacizumab-mFOLFOX6 | 4 (9%) |
| Bevacizumab-FOLFIRI | 5 (10%) |
| Bevacizumab-CapIRI | 9 (20%) |
| Bevacizumab-De Gramont | 11 (24%) |
| Bevacizumab-Capecitabine | 3 (7%) |
| Bevacizumab monotherapy | 14 (30%) |
| PFS | OS | |||
|---|---|---|---|---|
| Median Months (95% CI) | p-Value | Median Months (95% CI) | p-Value | |
| VEGF rs2010963 | ||||
| G/G | 7.6 (4.8–10.4) | 0.600 | 35.4 (11.6–59.2) | 0.811 |
| G/C | 9.6 (5.9–13.2) | 22.5 (21.5–47.6) | ||
| C/C | 8.9 (7.1–10.7) | 16.9 (15–18.8) | ||
| VEGF rs1570360 | 0.554 | 0.074 | ||
| G/G | 8.9 (6.9–10.9) | 27.8 (20–35.6) | ||
| G/A | 12.6 (1.6–23.6) | 43.2 (33.2–53.2) | ||
| A/A | 9.3 (3.7–18.9) | 39.2 (12.4–65.9) | ||
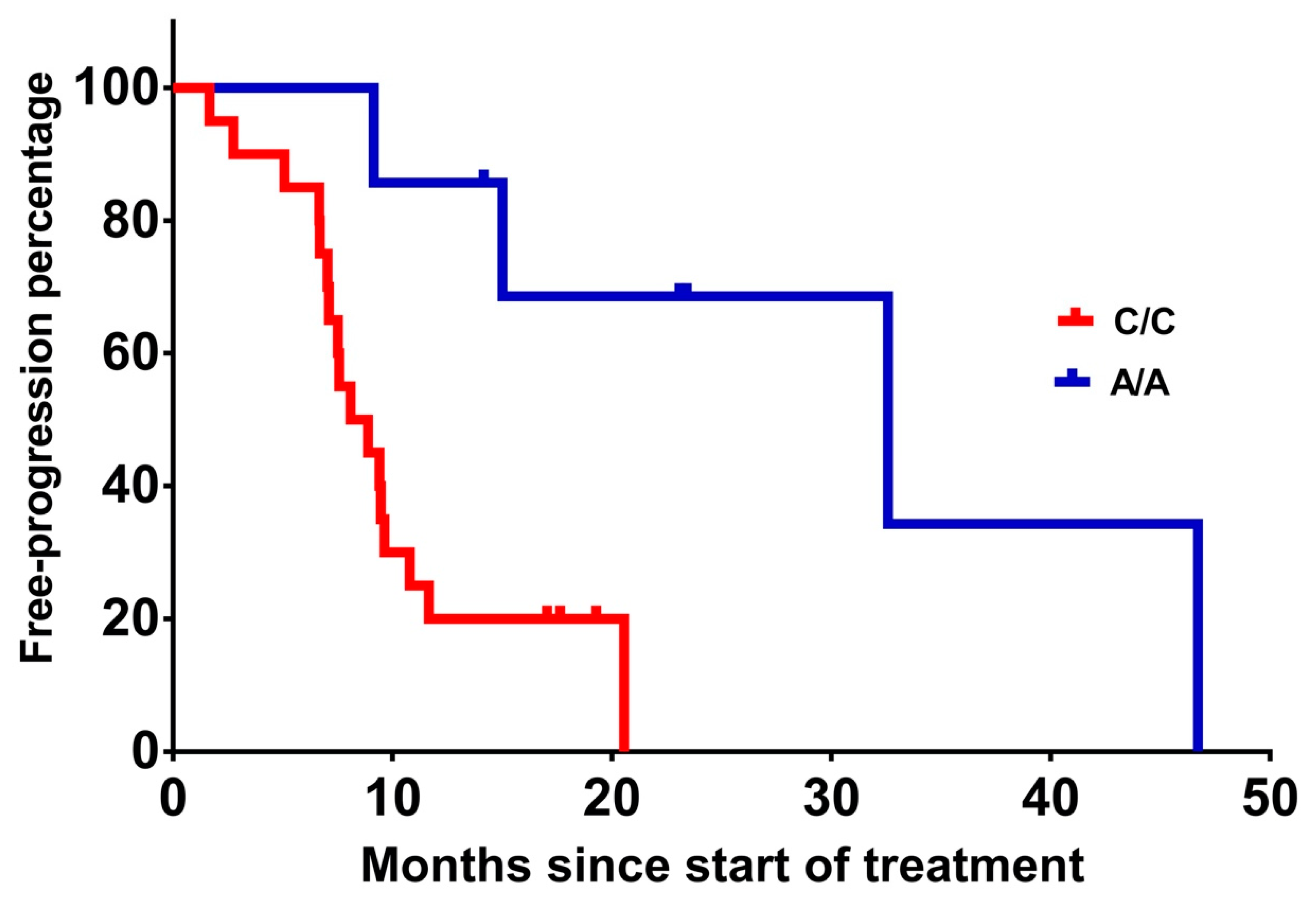
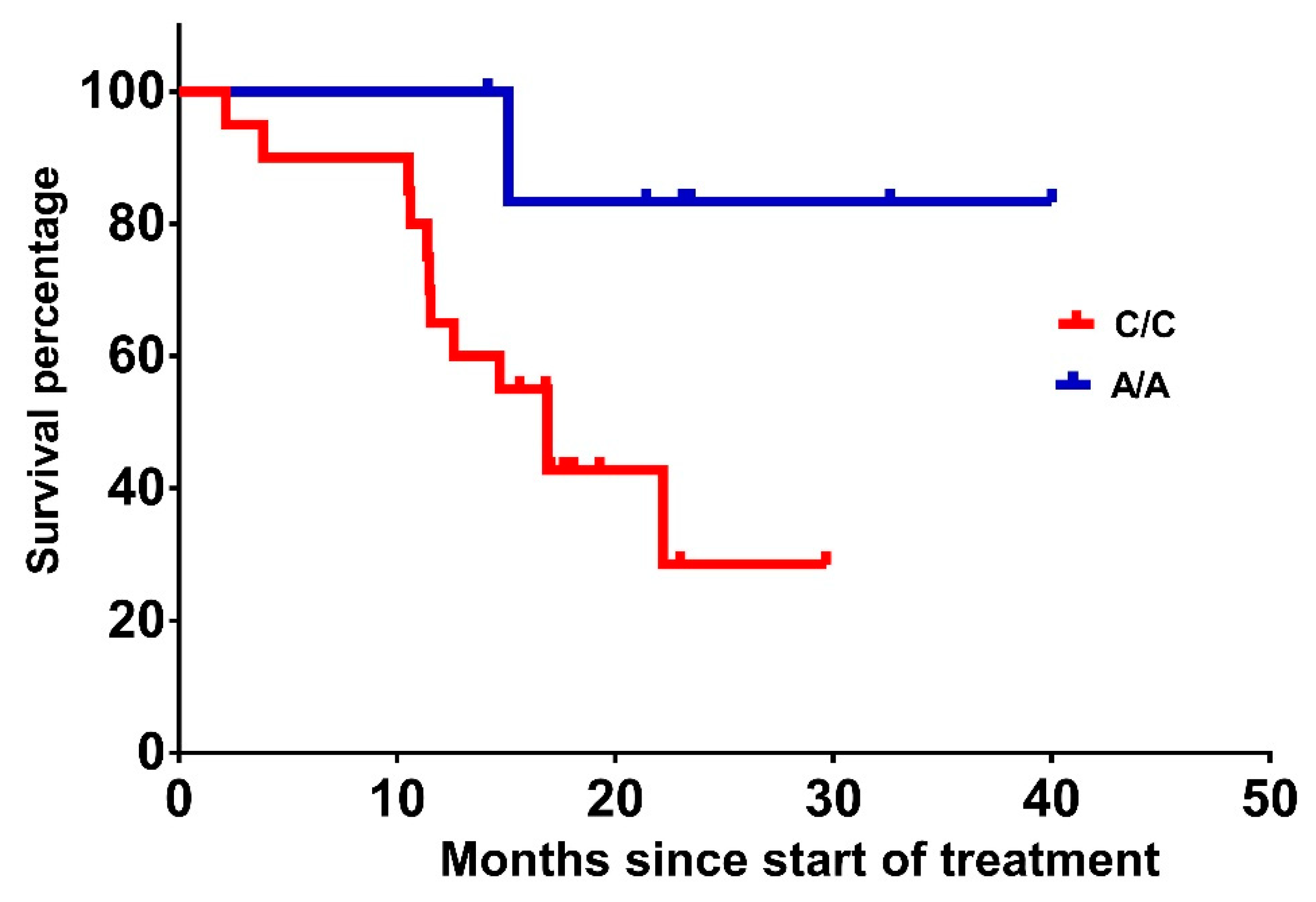
| VEGF rs699947 | ||||
| C/C | 8.1 (5.3–10.9) | 0.006 | 16.9 (12.8–20.9) | 0.043 |
| C/A | N/A | N/A | ||
| A/A | 32.6 (13.2–44.9) | 59.4 (33.3–70.7) | ||
| ICAM rs5498 | ||||
| A/A | 8.9 (6.6–11.2) | 0.700 | 16.9 (12.6–21.2) | 0.159 |
| A/G | 8.1 (4.8–11.4) | 35.4 (11.2–59.5) | ||
| G/G | 9.4 (4.6–14.2) | 47.9 (26.5–85.7) | ||
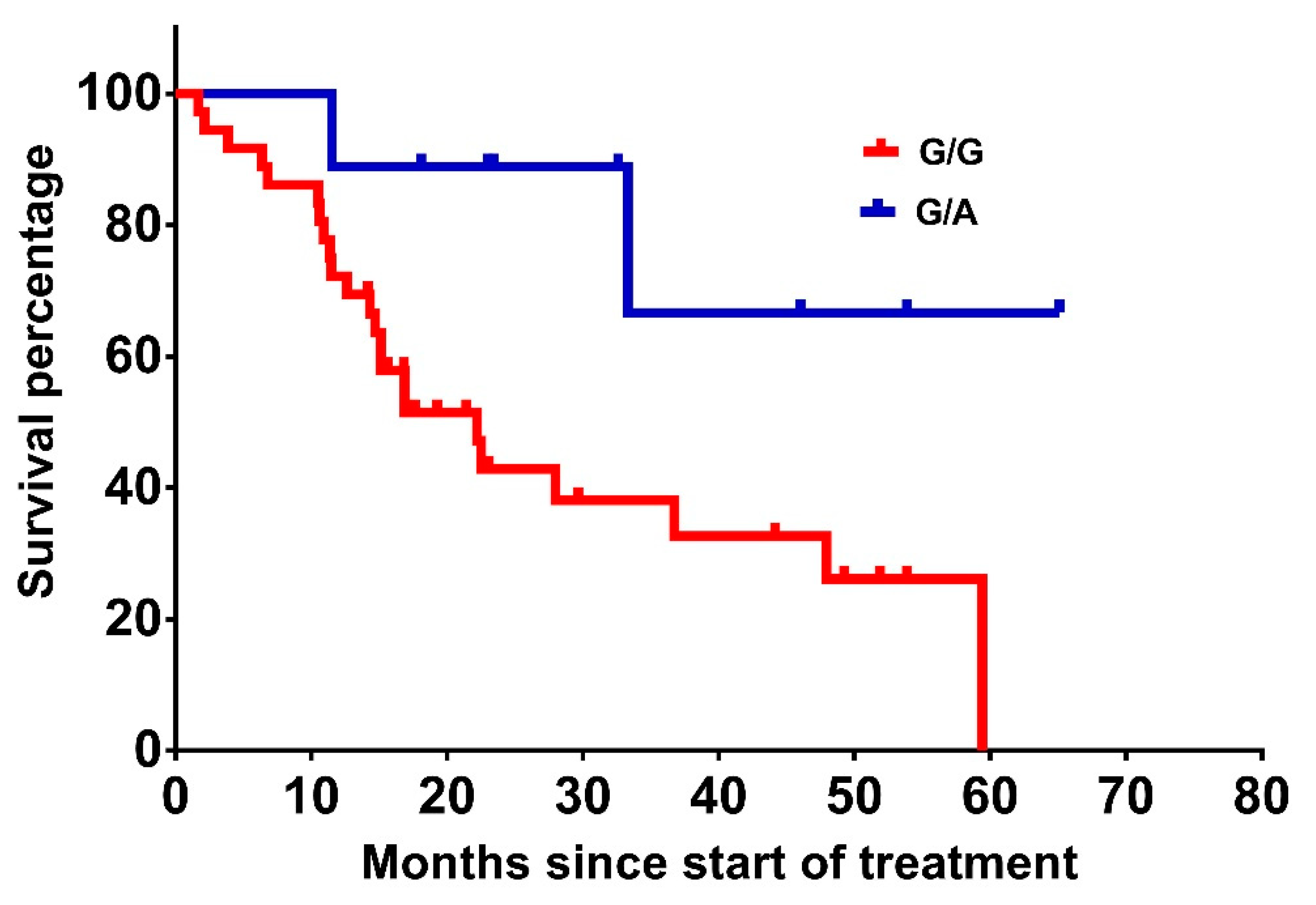
| ICAM rs1799969 | ||||
| G/G | 9.1 (7–11.2) | 0.938 | 29.1 (21.4–36.9) | 0.036 |
| G/A | 8.1 (3.5–12.7) | 48.7 (34.5–62.8) | ||
| A/A | N/A | N/A | ||
| KRAS rs61764370 | ||||
| Wild type | 8.9 (3.9–13.8) | 0.880 | 43.5 (29–57.7) | 0.511 |
| Mutant | 8.1 (5.6–10.7) | 20.8 (13.9–27.7) | ||
| NRAS rs11554290 | ||||
| Wild type | 8.9 (6.2–11.6) | 0.783 | 25 (19.2–30.9) | 0.374 |
| Mutant | 8.1 (5.3–10.9) | 33.7 (19.2–30.9) | ||
| BRAF rs113488022 | ||||
| Wild type | 7.1 (6.8–7.4) | 0.466 | 16.7 (14.3–19.1) | 0.027 |
| Mutant | 5.6 (3.9–13.4) | 6.8 (4.6–15.9) | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papachristos, A.; Kemos, P.; Katsila, T.; Panoilia, E.; Patrinos, G.P.; Kalofonos, H.; Sivolapenko, G.B. VEGF-A and ICAM-1 Gene Polymorphisms as Predictors of Clinical Outcome to First-Line Bevacizumab-Based Treatment in Metastatic Colorectal Cancer. Int. J. Mol. Sci. 2019, 20, 5791. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20225791
Papachristos A, Kemos P, Katsila T, Panoilia E, Patrinos GP, Kalofonos H, Sivolapenko GB. VEGF-A and ICAM-1 Gene Polymorphisms as Predictors of Clinical Outcome to First-Line Bevacizumab-Based Treatment in Metastatic Colorectal Cancer. International Journal of Molecular Sciences. 2019; 20(22):5791. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20225791
Chicago/Turabian StylePapachristos, Apostolos, Polychronis Kemos, Theodora Katsila, Eirini Panoilia, George P. Patrinos, Haralabos Kalofonos, and Gregory B. Sivolapenko. 2019. "VEGF-A and ICAM-1 Gene Polymorphisms as Predictors of Clinical Outcome to First-Line Bevacizumab-Based Treatment in Metastatic Colorectal Cancer" International Journal of Molecular Sciences 20, no. 22: 5791. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20225791