The Q-LAMP Method Represents a Valid and Rapid Alternative for the Detection of the BCR-ABL1 Rearrangement in Philadelphia-Positive Leukemias


 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Concordance between the Q-LAMP Assay and the Standard BIOMED-1 Method on p210 and p190 BCR-ABL1 Isoforms
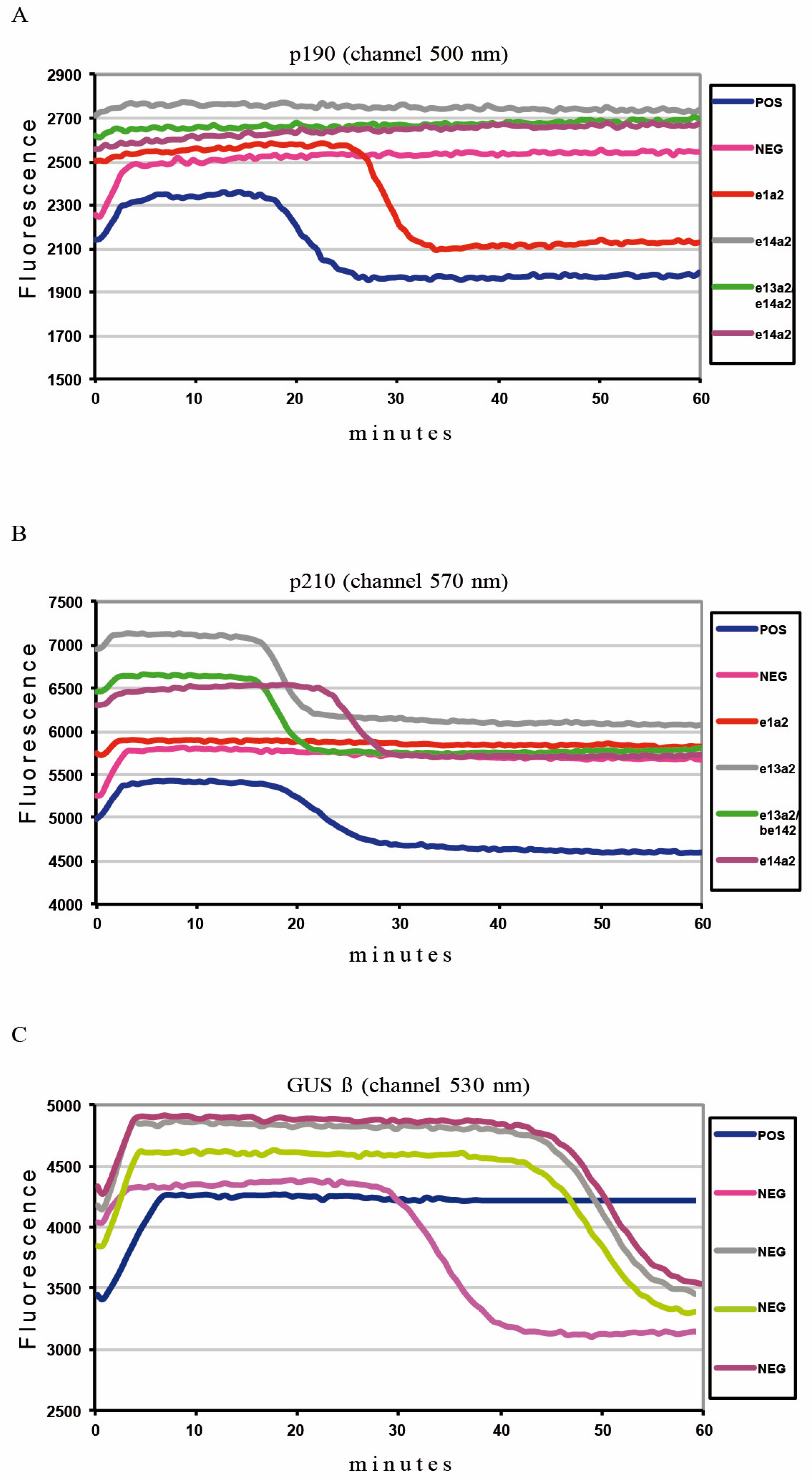
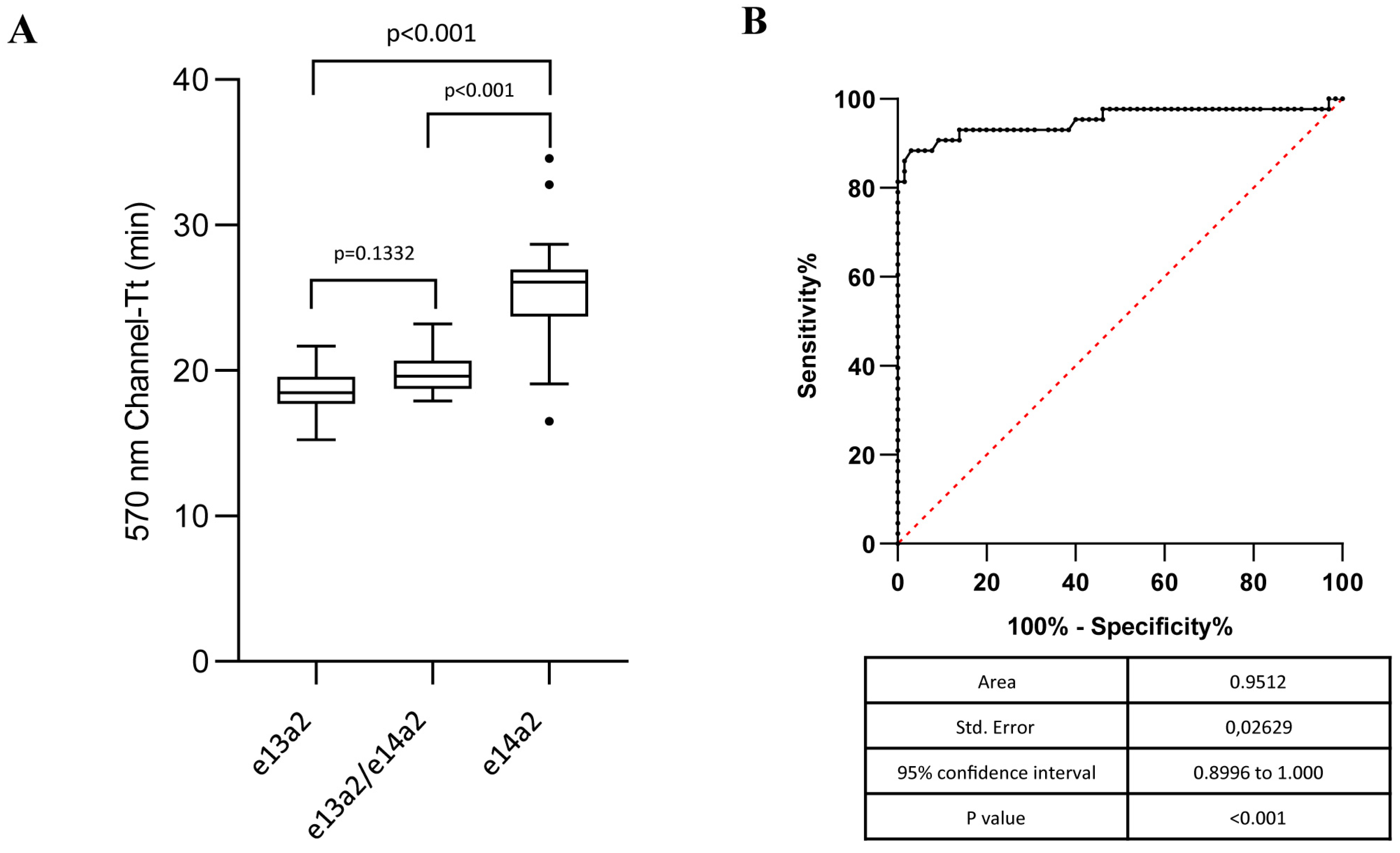
2.2. Q-LAMP Performance on Common BCR-ABL1 p210 Isoforms
2.3. Concordance between the Q-LAMP Assay and the Standard BIOMED-1 Method on Rare p210 and p190 BCR-ABL1 Isoforms
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. RNA Extraction
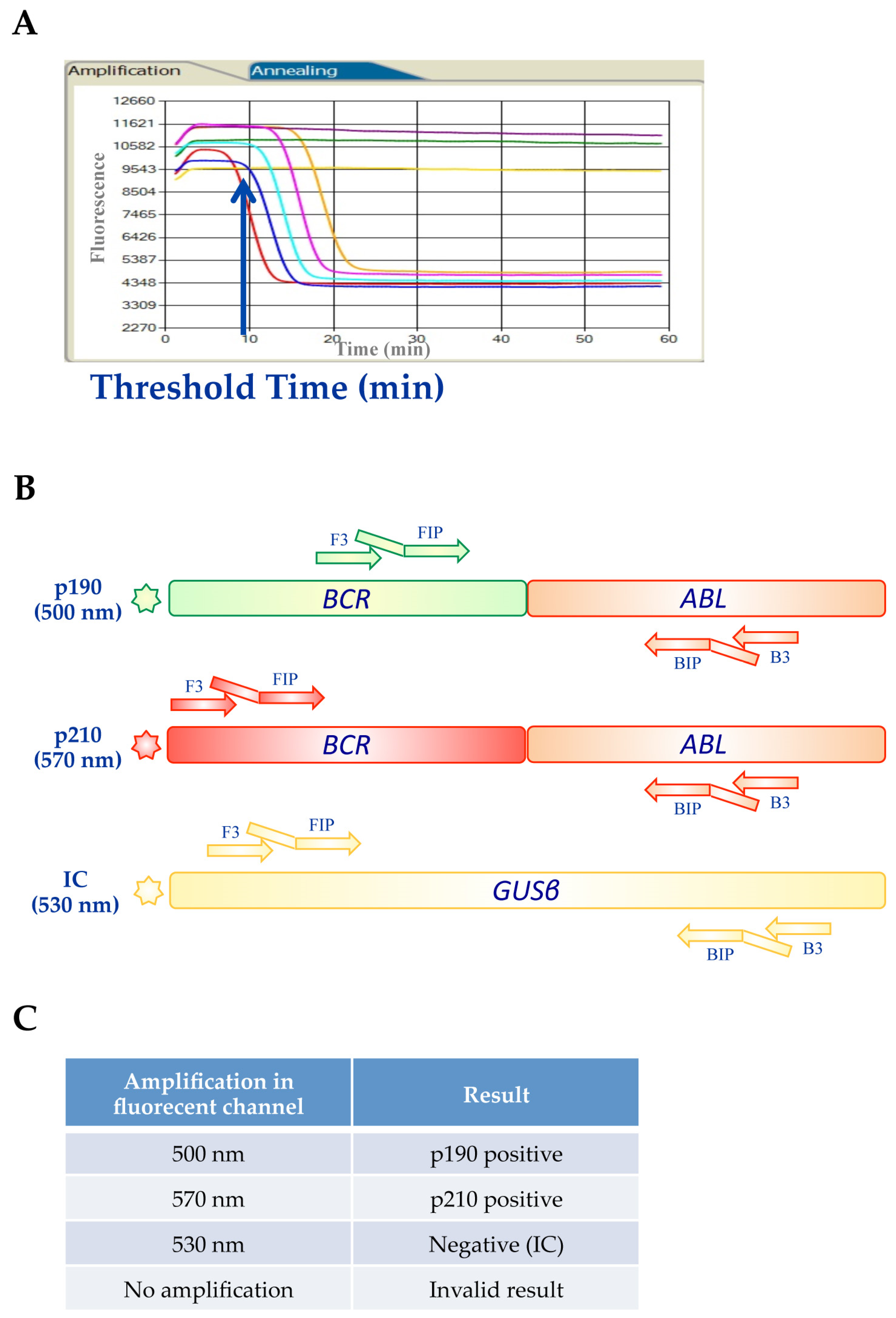
4.3. BCR-ABL1 Q-LAMP Assay
4.4. Statistical Analyses
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ABL1 | Abelson murine leukemia |
| ALL | acute lymphoblastic leukemia |
| BCR | breakpoint cluster region |
| CML | chronic myeloid leukemia |
| GUSβ | β-glucuronidase |
| LAMP | loop-mediated isothermal amplification |
| ROC | receiver operating characteristic |
| TK | tyrosine kinase |
| TKI | tyrosine kinase inhibitor |
| TFR | treatment-free remission |
References
- Foroni, L.; Wilson, G.; Gerrard, G.; Mason, J.; Grimwade, D.; White, H.E.; De Castro, D.G.; Austin, S.; Awan, A.; Burt, E.; et al. Guidelines for the measurement of BCR-ABL1 transcripts in chronic myeloid leukaemia. Br. J. Haematol. 2011, 153, 179–190. [Google Scholar] [CrossRef] [PubMed]
- Westbrook, C.A.; Hooberman, A.L.; Spino, C.; Dodge, R.K.; Larson, R.A.; Davey, F.; Wurster-Hill, D.H.; Sobol, R.E.; Schiffer, C.; Bloomfield, C.D. Clinical significance of the BCR-ABL fusion gene in adult acute lymphoblastic leukemia: A Cancer and Leukemia Group B Study (8762). Blood 1992, 80, 2983–2990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujimaki, K.; Hattori, Y.; Nakajima, H. 10-year complete remission in a Philadelphia chromosome-positive acute lymphoblastic leukemia patient using imatinib without high-intensity chemotherapy or allogeneic stem cell transplantation. Int. J. Hematol. 2018, 107, 709–711. [Google Scholar] [CrossRef] [PubMed]
- Apperley, J.F. Chronic myeloid leukaemia. Lancet 2015, 385, 1447–1459. [Google Scholar] [CrossRef]
- Stagno, F.; Stella, S.; Spitaleri, A.; Pennisi, M.S.; Di Raimondo, F.; Vigneri, P. Imatinib mesylate in chronic myeloid leukemia: Frontline treatment and long-term outcomes. Expert Rev. Anticancer Ther. 2016, 16, 273–278. [Google Scholar] [CrossRef]
- Quintas-Cardama, A.; Cortes, J. Molecular biology of bcr-abl1-positive chronic myeloid leukemia. Blood 2009, 113, 1619–1630. [Google Scholar] [CrossRef] [Green Version]
- Giallongo, C.; Parrinello, N.; Tibullo, D.; La Cava, P.; Romano, A.; Chiarenza, A.; Barbagallo, I.; Palumbo, G.A.; Stagno, F.; Vigneri, P.; et al. Myeloid derived suppressor cells (MDSCs) are increased and exert immunosuppressive activity together with polymorphonuclear leukocytes (PMNs) in chronic myeloid leukemia patients. PLoS ONE 2014, 9, e101848. [Google Scholar] [CrossRef] [Green Version]
- Preyer, M.; Vigneri, P.; Wang, J.Y. Interplay between kinase domain autophosphorylation and F-actin binding domain in regulating imatinib sensitivity and nuclear import of BCR-ABL. PLoS ONE 2011, 6, e17020. [Google Scholar] [CrossRef]
- Manzella, L.; Tirro, E.; Pennisi, M.S.; Massimino, M.; Stella, S.; Romano, C.; Vitale, S.R.; Vigneri, P. Roles of Interferon Regulatory Factors in Chronic Myeloid Leukemia. Curr. Cancer Drug Targ. 2016, 16, 594–605. [Google Scholar] [CrossRef]
- Jain, P.; Kantarjian, H.; Patel, K.P.; Gonzalez, G.N.; Luthra, R.; Kanagal Shamanna, R.; Sasaki, K.; Jabbour, E.; Romo, C.G.; Kadia, T.M.; et al. Impact of BCR-ABL transcript type on outcome in patients with chronic-phase CML treated with tyrosine kinase inhibitors. Blood 2016, 127, 1269–1275. [Google Scholar] [CrossRef]
- Jinawath, N.; Norris-Kirby, A.; Smith, B.D.; Gocke, C.D.; Batista, D.A.; Griffin, C.A.; Murphy, K.M. A rare e14a3 (b3a3) BCR-ABL fusion transcript in chronic myeloid leukemia: Diagnostic challenges in clinical laboratory practice. J. Mol. Diagn. JMD 2009, 11, 359–363. [Google Scholar] [CrossRef] [Green Version]
- Fujisawa, S.; Nakamura, S.; Naito, K.; Kobayashi, M.; Ohnishi, K. A variant transcript, e1a3, of the minor BCR-ABL fusion gene in acute lymphoblastic leukemia: Case report and review of the literature. Int. J. Hematol. 2008, 87, 184–188. [Google Scholar] [CrossRef]
- Massimino, M.; Stella, S.; Tirro, E.; Consoli, M.L.; Pennisi, M.S.; Puma, A.; Vitale, S.R.; Romano, C.; Zammit, V.; Stagno, F.; et al. Efficacy of Dasatinib in a Very Elderly CML Patient Expressing a Rare E13a3 Bcr-Abl1 Fusion Transcript: A Case Report. Anticancer Res. 2019, 39, 3949–3954. [Google Scholar] [CrossRef]
- Massimino, M.; Stella, S.; Tirro, E.; Consoli, M.L.; Pennisi, M.S.; Puma, A.; Vitale, S.R.; Romano, C.; Zammit, V.; Stagno, F.; et al. Rapid decline of Philadelphia-positive metaphases after nilotinib treatment in a CML patient expressing a rare e14a3 BCR-ABL1 fusion transcript: A case report. Oncol. Lett. 2019, 18, 2648–2653. [Google Scholar] [CrossRef] [Green Version]
- Lucas, C.M.; Harris, R.J.; Giannoudis, A.; Davies, A.; Knight, K.; Watmough, S.J.; Wang, L.; Clark, R.E. Chronic myeloid leukemia patients with the e13a2 BCR-ABL fusion transcript have inferior responses to imatinib compared to patients with the e14a2 transcript. Haematologica 2009, 94, 1362–1367. [Google Scholar] [CrossRef] [Green Version]
- Hanfstein, B.; Lauseker, M.; Hehlmann, R.; Saussele, S.; Erben, P.; Dietz, C.; Fabarius, A.; Proetel, U.; Schnittger, S.; Haferlach, C.; et al. Distinct characteristics of e13a2 versus e14a2 BCR-ABL1 driven chronic myeloid leukemia under first-line therapy with imatinib. Haematologica 2014, 99, 1441–1447. [Google Scholar] [CrossRef]
- Bonifacio, M.S.; Binotto, G.; De Marchi, F.; Maino, E.; Calistri, E.; Bonalumi, A.; Frison, L.; Marin, L.; Medeot, M.; De Matteis, G.; et al. Predictive Factors of Stable Deep Molecular Response in Chronic Myeloid Leukemia Patients Treated with Imatinib Standard Dose: A Study from the Gruppo Triveneto LMC. Blood 2015, 126, 597. [Google Scholar] [CrossRef]
- Vigneri, P.; Stagno, F.; Stella, S.; Cupri, A.; Forte, S.; Massimino, M.; Antolino, A.; Siragusa, S.; Mannina, D.; Impera, S.S.; et al. High BCR-ABL/GUS(IS) Levels at Diagnosis of Chronic Phase CML Are Associated with Unfavorable Responses to Standard-Dose Imatinib. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2017, 23, 7189–7198. [Google Scholar] [CrossRef] [Green Version]
- Castagnetti, F.; Gugliotta, G.; Breccia, M.; Iurlo, A.; Levato, L.; Albano, F.; Vigneri, P.; Abruzzese, E.; Rossi, G.; Rupoli, S.; et al. The BCR-ABL1 transcript type influences response and outcome in Philadelphia chromosome-positive chronic myeloid leukemia patients treated frontline with imatinib. Am. J. Hematol. 2017, 92, 797–805. [Google Scholar] [CrossRef] [Green Version]
- Baccarani, M.; Deininger, M.W.; Rosti, G.; Hochhaus, A.; Soverini, S.; Apperley, J.F.; Cervantes, F.; Clark, R.E.; Cortes, J.E.; Guilhot, F.; et al. European LeukemiaNet recommendations for the management of chronic myeloid leukemia: 2013. Blood 2013, 122, 872–884. [Google Scholar] [CrossRef]
- Bassan, R.; Rossi, G.; Pogliani, E.M.; Di Bona, E.; Angelucci, E.; Cavattoni, I.; Lambertenghi-Deliliers, G.; Mannelli, F.; Levis, A.; Ciceri, F.; et al. Chemotherapy-phased imatinib pulses improve long-term outcome of adult patients with Philadelphia chromosome-positive acute lymphoblastic leukemia: Northern Italy Leukemia Group protocol 09/00. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2010, 28, 3644–3652. [Google Scholar] [CrossRef] [PubMed]
- Jabbour, E.; Kantarjian, H.; Ravandi, F.; Thomas, D.; Huang, X.; Faderl, S.; Pemmaraju, N.; Daver, N.; Garcia-Manero, G.; Sasaki, K.; et al. Combination of hyper-CVAD with ponatinib as first-line therapy for patients with Philadelphia chromosome-positive acute lymphoblastic leukaemia: A single-centre, phase 2 study. Lancet. Oncol. 2015, 16, 1547–1555. [Google Scholar] [CrossRef] [Green Version]
- Pirosa, M.C.; Leotta, S.; Cupri, A.; Stella, S.; Martino, E.A.; Scalise, L.; Sapienza, G.; Calafiore, V.; Mauro, E.; Spadaro, A.; et al. Long-Term Molecular Remission Achieved by Antibody Anti-CD22 and Ponatinib in a Patient Affected by Ph’+ Acute Lymphoblastic Leukemia Relapsed after Second Allogeneic Hematopoietic Stem Cell Transplantation: A Case Report. Chemotherapy 2018, 63, 220–224. [Google Scholar] [CrossRef] [PubMed]
- Stella, S.; Massimino, M.; Tirro, E.; Vitale, S.R.; Scalise, L.; Leotta, S.; Pennisi, M.S.; Puma, A.; Romano, C.; Stagno, F.; et al. B-ALL Relapses After Autologous Stem Cell Transplantation Associated With a Shift from e1a2 to e14a2 BCR-ABL Transcripts: A Case Report. Anticancer Res. 2019, 39, 431–435. [Google Scholar] [CrossRef] [PubMed]
- Van Dongen, J.J.; Macintyre, E.A.; Gabert, J.A.; Delabesse, E.; Rossi, V.; Saglio, G.; Gottardi, E.; Rambaldi, A.; Dotti, G.; Griesinger, F.; et al. Standardized RT-PCR analysis of fusion gene transcripts from chromosome aberrations in acute leukemia for detection of minimal residual disease. Report of the BIOMED-1 Concerted Action: Investigation of minimal residual disease in acute leukemia. Leukemia 1999, 13, 1901–1928. [Google Scholar] [CrossRef]
- Notomi, T.; Okayama, H.; Masubuchi, H.; Yonekawa, T.; Watanabe, K.; Amino, N.; Hase, T. Loop-mediated isothermal amplification of DNA. Nucleic Acids Res. 2000, 28, e63. [Google Scholar] [CrossRef] [Green Version]
- Fu, S.; Qu, G.; Guo, S.; Ma, L.; Zhang, N.; Zhang, S.; Gao, S.; Shen, Z. Applications of loop-mediated isothermal DNA amplification. Appl. Biochem. Biotechnol. 2011, 163, 845–850. [Google Scholar] [CrossRef]
- Nakao, R.; Stromdahl, E.Y.; Magona, J.W.; Faburay, B.; Namangala, B.; Malele, I.; Inoue, N.; Geysen, D.; Kajino, K.; Jongejan, F.; et al. Development of loop-mediated isothermal amplification (LAMP) assays for rapid detection of Ehrlichia ruminantium. BMC Microbiol. 2010, 10, 296. [Google Scholar] [CrossRef] [Green Version]
- Soleimani, M.; Shams, S.; Majidzadeh, A.K. Developing a real-time quantitative loop-mediated isothermal amplification assay as a rapid and accurate method for detection of Brucellosis. J. Appl. Microbiol. 2013, 115, 828–834. [Google Scholar] [CrossRef]
- Spinelli, O.; Rambaldi, A.; Rigo, F.; Zanghi, P.; D’Agostini, E.; Amicarelli, G.; Colotta, F.; Divona, M.; Ciardi, C.; Coco, F.L.; et al. Simple, rapid and accurate molecular diagnosis of acute promyelocytic leukemia by loop mediated amplification technology. Oncoscience 2015, 2, 50–58. [Google Scholar] [CrossRef]
- Minnucci, G.; Amicarelli, G.; Salmoiraghi, S.; Spinelli, O.; Guinea Montalvo, M.L.; Giussani, U.; Adlerstein, D.; Rambaldi, A. A novel, highly sensitive and rapid allele-specific loop-mediated amplification assay for the detection of the JAK2V617F mutation in chronic myeloproliferative neoplasms. Haematologica 2012, 97, 1394–1400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salmoiraghi, S.; Montalvo, M.L.; D’Agostini, E.; Amicarelli, G.; Minnucci, G.; Spinelli, O.; Rambaldi, A. Mutations and chromosomal rearrangements of JAK2: Not only a myeloid issue. Expert Rev. Hematol. 2013, 6, 429–439. [Google Scholar] [CrossRef] [PubMed]
- Salmoiraghi, S.; Minnucci, G.; Amicarelli, G.; Zanghi, P.; Elidi, L.; Montalvo, M.L.G.; Rigo, F.; D’Agostini, E.; Tettamanzi, V.; Giachelia, M.; et al. Development of new tools for molecular diagnosis of hematologic malignancies. Biochim. Clin. 2016, 40, 234–243. [Google Scholar]
- Hochhaus, A.; Larson, R.A.; Guilhot, F.; Radich, J.P.; Branford, S.; Hughes, T.P.; Baccarani, M.; Deininger, M.W.; Cervantes, F.; Fujihara, S.; et al. Long-Term Outcomes of Imatinib Treatment for Chronic Myeloid Leukemia. N. Engl. J. Med. 2017, 376, 917–927. [Google Scholar] [CrossRef] [PubMed]
- Maino, E.; Sancetta, R.; Viero, P.; Imbergamo, S.; Scattolin, A.M.; Vespignani, M.; Bassan, R. Current and future management of Ph/BCR-ABL positive ALL. Expert Rev. Anticancer Ther. 2014, 14, 723–740. [Google Scholar] [CrossRef] [PubMed]
- Clark, R.E.; Polydoros, F.; Apperley, J.F.; Milojkovic, D.; Pocock, C.; Smith, G.; Byrne, J.L.; De Lavallade, H.; O’Brien, S.G.; Coffey, T.; et al. De-escalation of tyrosine kinase inhibitor dose in patients with chronic myeloid leukaemia with stable major molecular response (DESTINY): An interim analysis of a non-randomised, phase 2 trial. Lancet. Haematol. 2017, 4, e310–e316. [Google Scholar] [CrossRef] [Green Version]
- D’Adda, M.; Farina, M.; Schieppati, F.; Borlenghi, E.; Bottelli, C.; Cerqui, E.; Ferrari, S.; Gramegna, D.; Pagani, C.; Passi, A.; et al. The e13a2 BCR-ABL transcript negatively affects sustained deep molecular response and the achievement of treatment-free remission in patients with chronic myeloid leukemia who receive tyrosine kinase inhibitors. Cancer 2019, 125, 1674–1682. [Google Scholar] [CrossRef]
- Baccarani, M.; Castagnetti, F.; Gugliotta, G.; Rosti, G.; Soverini, S.; Albeer, A.; Pfirrmann, M.; International BCR-ABL Study Group. The proportion of different BCR-ABL1 transcript types in chronic myeloid leukemia. An international overview. Leukemia 2019, 33, 1173–1183. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Results by Conventional RT-PCR (BIOMED-1) | |||||
|---|---|---|---|---|---|
| p190 | p210 | Negative | Total | ||
| Q-LAMP Assay | p190 | 14 | / | / | 14 |
| p210 | / | 108 | / | 107 | |
| Negative | / | / | 50 | 50 | |
| Total | 14 | 108 | 50 | 172 | |
| Isoform (N Sample) | Mean Tt * (st. dev) | Median Tt * (Range) | CV |
|---|---|---|---|
| e1a2 | 27.03 | 26.70 | 0.07 |
| (14) | (1.87) | (24.45–31.80) | / |
| e13a2 | 18.64 | 18.48 | 0.08 |
| (44) | (1.41) | (15.25–21.67) | / |
| e14a2 | 25.46 | 26.08 | 0.13 |
| (43) | (3.29) | (16.53–34.57) | / |
| e13a2/e14a2 | 19.84 | 19.63 | 0.06 |
| (21) | (1.29) | (17.93–23.20) | / |
| Results by conventional RT-PCR (BIOMED-1) | ||||||
|---|---|---|---|---|---|---|
| e1a3 | e13a3 (b2a3) | e14a2 (b3a3) | e19a2 | Total | ||
| Q-LAMP Assay | e1a3 | 5 | / | / | / | 5 |
| e13a2 (b2a3) | / | 9 | / | / | 9 | |
| e14a2 (b3a3) | / | / | 3 | / | 3 | |
| e19a2 | / | / | / | 3 | 3 | |
| Total | 5 | 9 | 3 | 3 | 20 | |
| Q-LAMP Assay | BIOMED-1 Method | |
|---|---|---|
| Nucleic acid input (RNA ng/sample) | RNA (500) | cDNA (1000) |
| Number of steps | 1 | ≥3 |
| Reaction setup | Easy | Moderately complex (RT-PCR is required) |
| Detection of rare BCR-ABL1 isoforms | Possible | Possible |
| Time to results (minutes) | <60 | >300 |
| Mark | CE/IVD | LDT |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stella, S.; Gottardi, E.M.; Favout, V.; Barragan Gonzalez, E.; Errichiello, S.; Vitale, S.R.; Fava, C.; Luciano, L.; Stagno, F.; Grimaldi, F.; et al. The Q-LAMP Method Represents a Valid and Rapid Alternative for the Detection of the BCR-ABL1 Rearrangement in Philadelphia-Positive Leukemias. Int. J. Mol. Sci. 2019, 20, 6106. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20246106
Stella S, Gottardi EM, Favout V, Barragan Gonzalez E, Errichiello S, Vitale SR, Fava C, Luciano L, Stagno F, Grimaldi F, et al. The Q-LAMP Method Represents a Valid and Rapid Alternative for the Detection of the BCR-ABL1 Rearrangement in Philadelphia-Positive Leukemias. International Journal of Molecular Sciences. 2019; 20(24):6106. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20246106
Chicago/Turabian StyleStella, Stefania, Enrico Marco Gottardi, Valeria Favout, Eva Barragan Gonzalez, Santa Errichiello, Silvia Rita Vitale, Carmen Fava, Luigia Luciano, Fabio Stagno, Francesco Grimaldi, and et al. 2019. "The Q-LAMP Method Represents a Valid and Rapid Alternative for the Detection of the BCR-ABL1 Rearrangement in Philadelphia-Positive Leukemias" International Journal of Molecular Sciences 20, no. 24: 6106. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20246106