Reactive Species Interactome Alterations in Oocyte Donation Pregnancies in the Absence and Presence of Pre-Eclampsia

 , , , and
, , , and
Abstract
:1. Introduction
2. Results
2.1. Study Participants, Pregnancy Characteristics and Fetal Characteristics
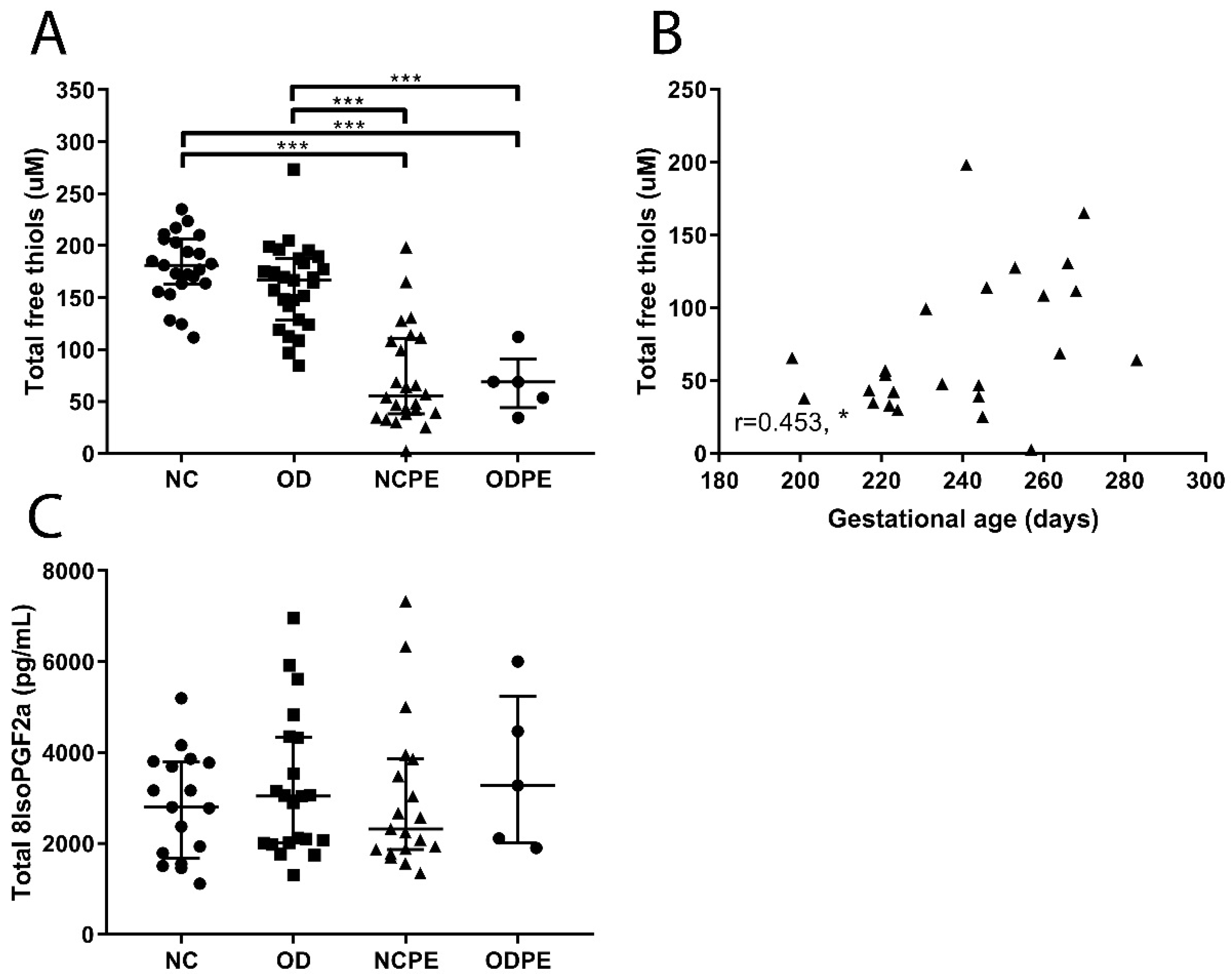
2.2. Presence of Oxidative Stress
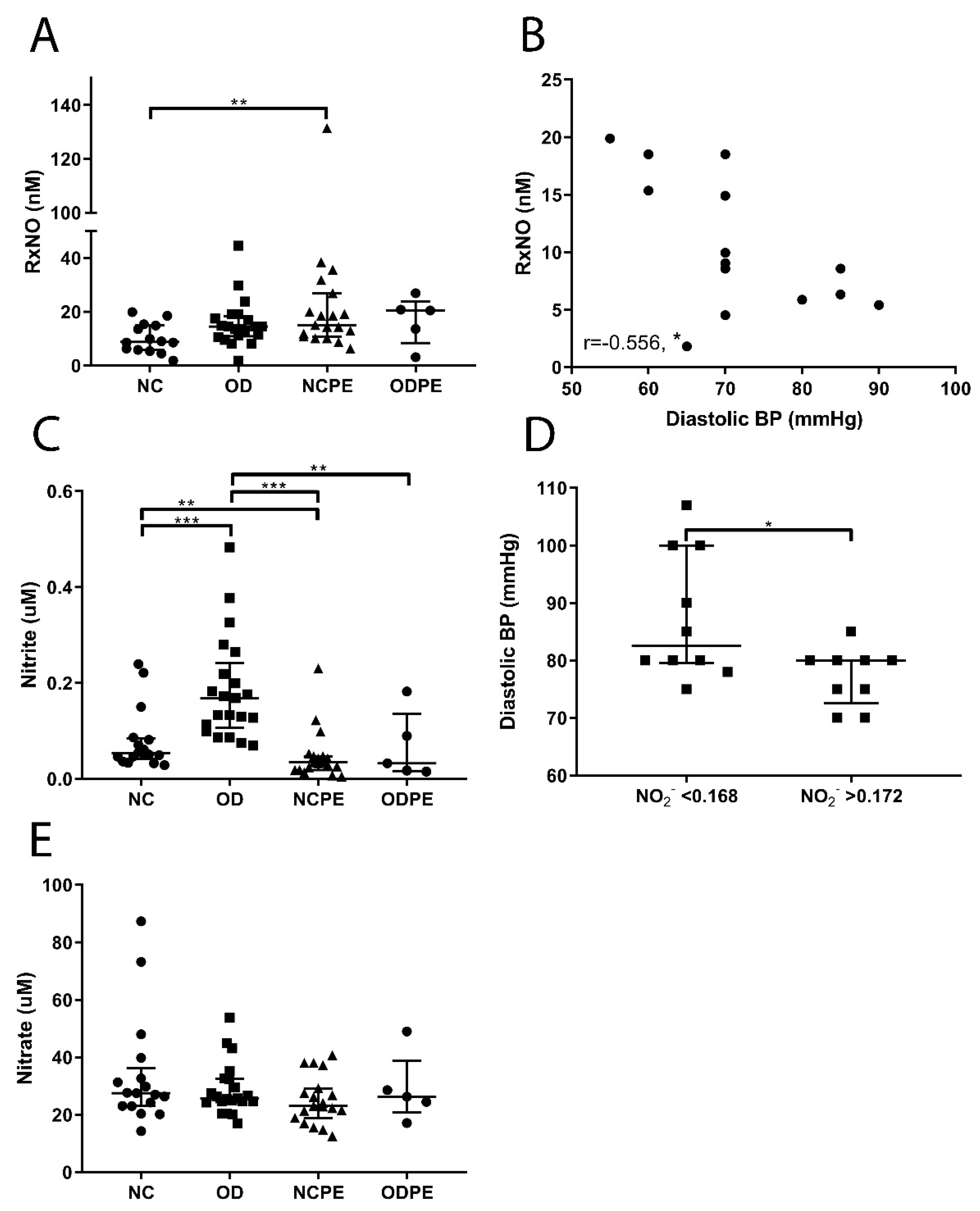
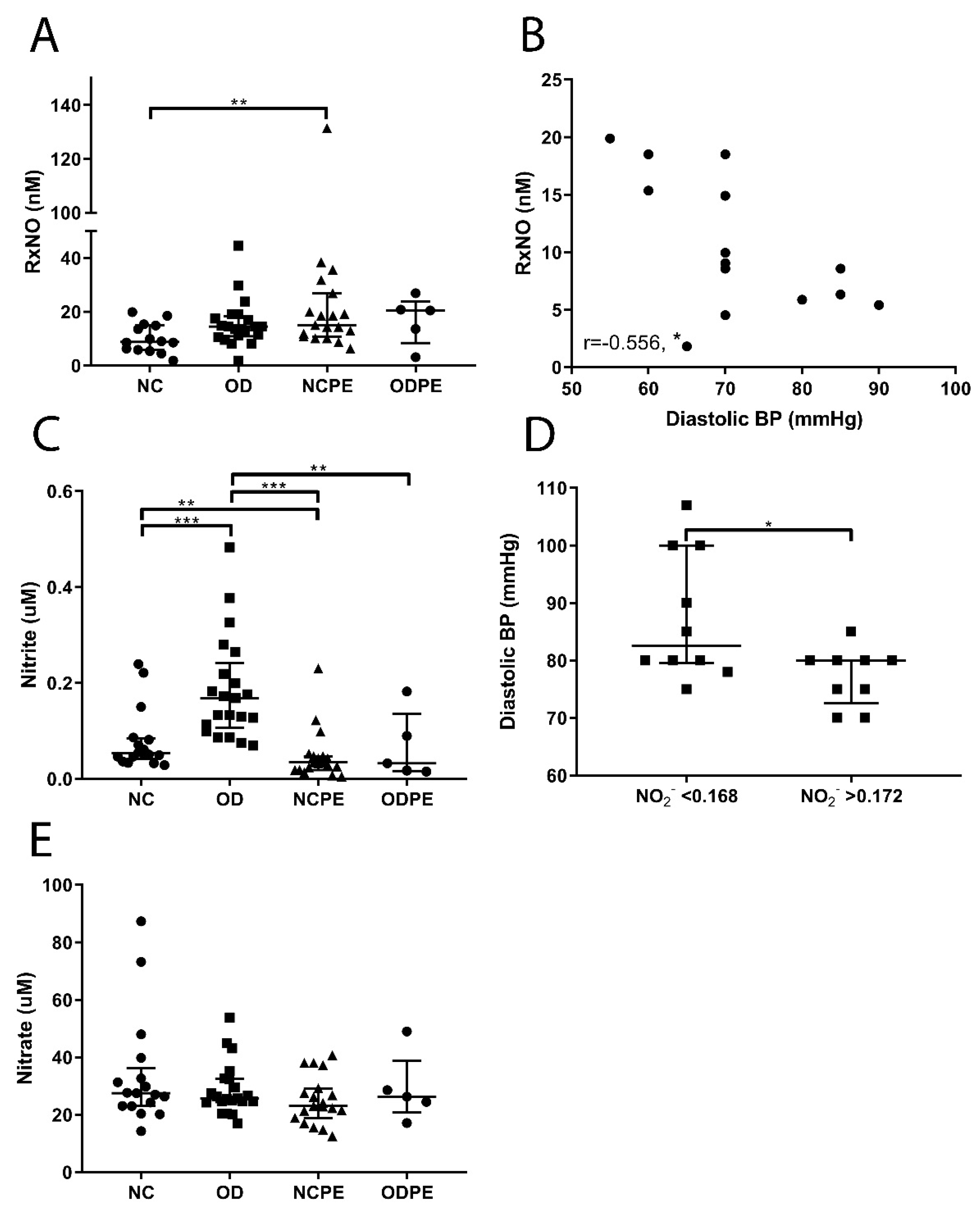
2.3. Nitric Oxide Pathway
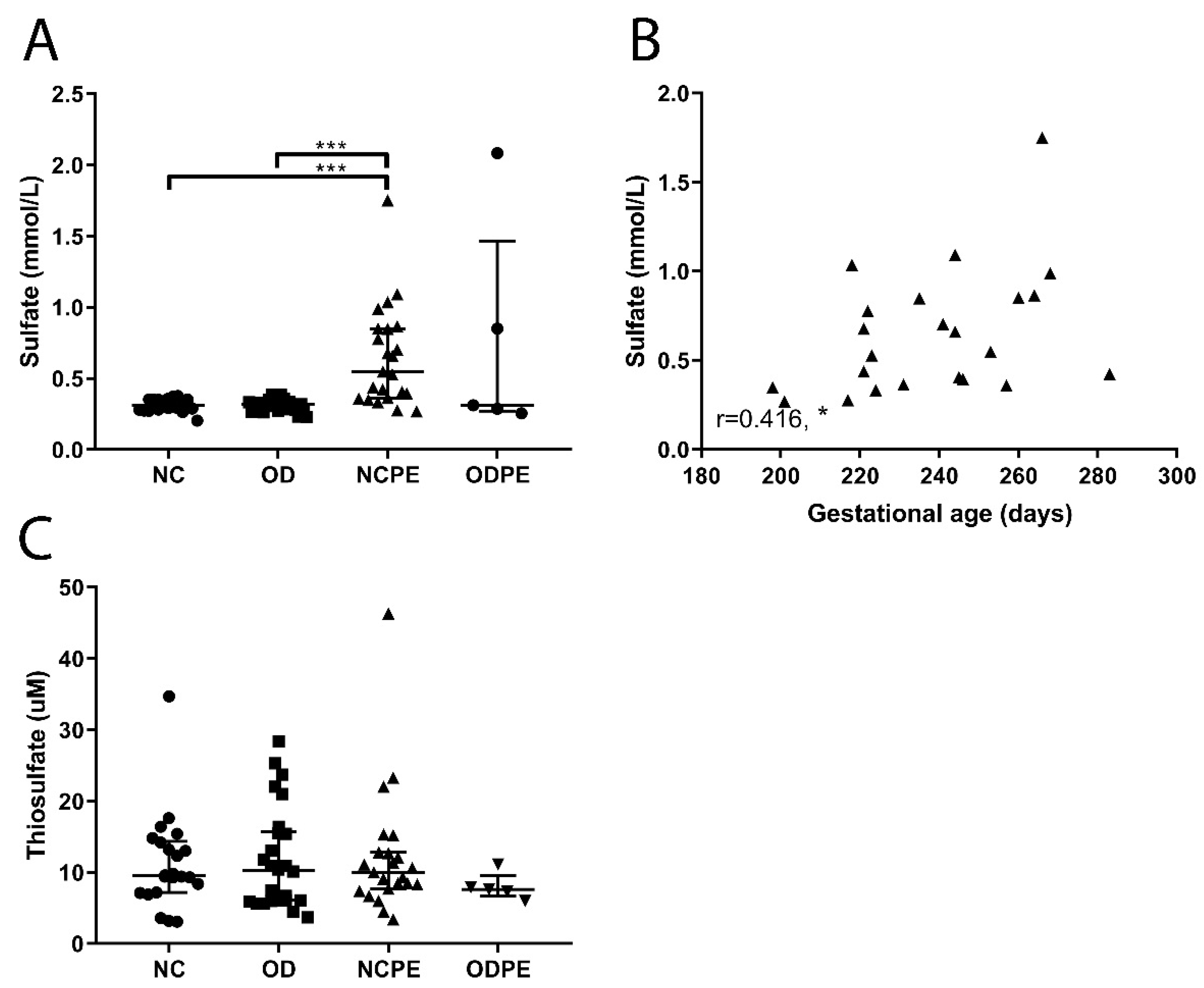
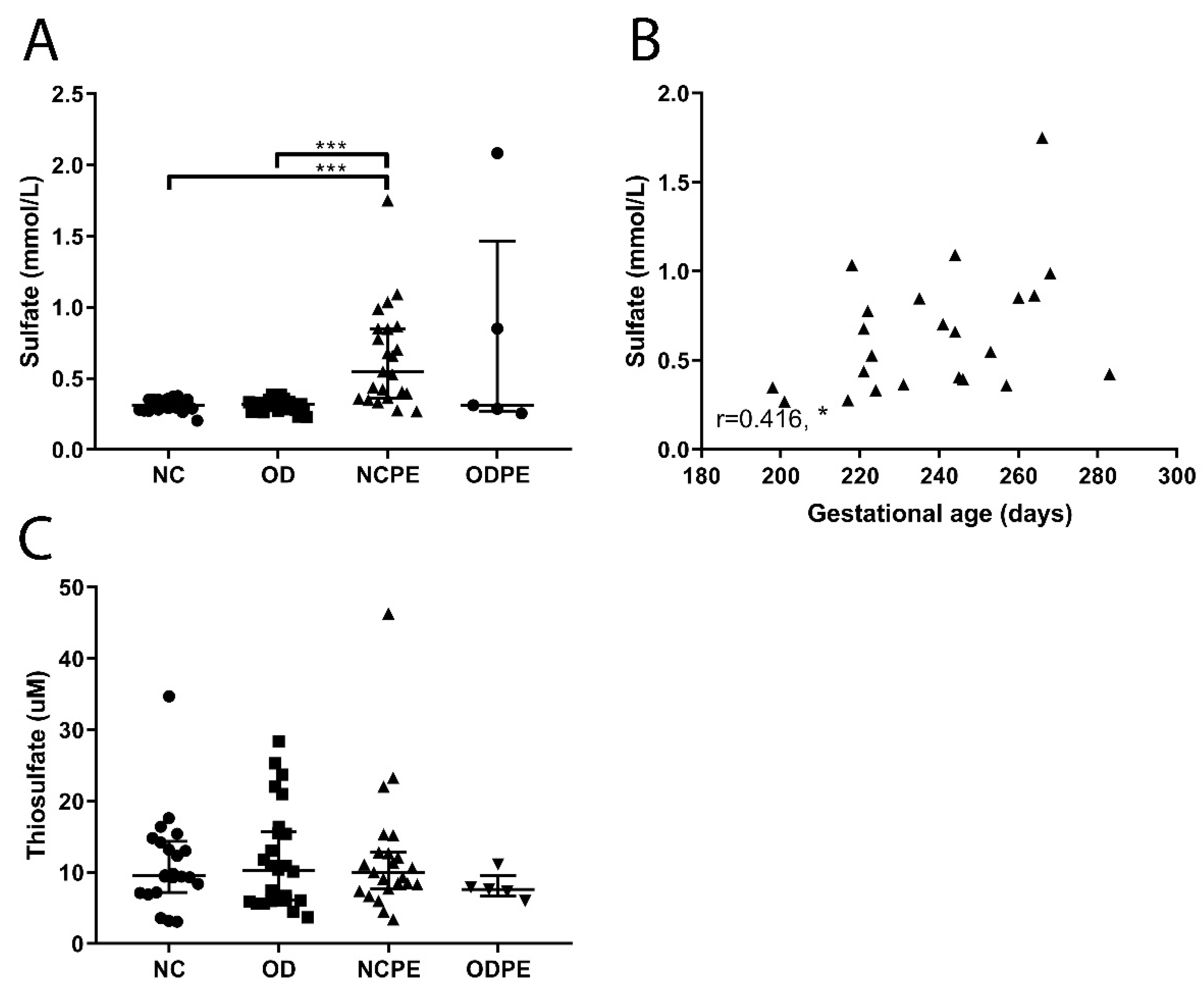
2.4. Hydrogen Sulfide Pathway
3. Discussion
4. Materials and Methods
4.1. Study Participants and Biospecimen Collection
4.2. Clinical Definitions
4.3. Measurements
4.3.1. Colorimetric Detection of Total Free Thiol Groups
4.3.2. Assessment of Nitroso Species via Gas Phase Chemiluminescence Detection
4.3.3. Determination of Nitrite and Nitrate
4.3.4. Total Free 8-Iso-Prostaglandin F2a Determination
4.3.5. Sulfate Determination
4.3.6. Thiosulfate Determination
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| H2S | Hydrogen sulfide |
| NO | Nitric oxide |
| NO2− | Nitrite |
| NO3− | Nitrate |
| ROS | Reactive oxygen species |
| RNS | Reactive nitrogen species |
| RSS | Reactive sulfur species |
| RSI | Reactive species interactome |
| RxNO | Protein bound nitric oxide |
| S2O32− | Thiosulfate |
| SO42− | Sulfate |
References
- Billington, W.D. The immunological problem of pregnancy: 50 years with the hope of progress. A tribute to Peter Medawar. J. Reproduct. Immunol. 2003, 60, 1–11. [Google Scholar] [CrossRef]
- Colucci, F.; Moffett, A.; Trowsdale, J. Medawar and the immunological paradox of pregnancy: 60 years on. Eur. J. Immunol. 2014, 44, 1883–1885. [Google Scholar] [CrossRef] [PubMed]
- Clapp, J.F., 3rd; Capeless, E. Cardiovascular function before, during, and after the first and subsequent pregnancies. Am. J. Cardiol. 1997, 80, 1469–1473. [Google Scholar] [CrossRef]
- Hussein, W.; Lafayette, R.A. Renal function in normal and disordered pregnancy. Curr. Opin. Nephrol. Hypertens. 2014, 23, 46–53. [Google Scholar] [CrossRef] [PubMed]
- van der Hoorn, M.L.; Scherjon, S.A.; Claas, F.H. Egg donation pregnancy as an immunological model for solid organ transplantation. Transplant Immunol. 2011, 25, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Colucci, F.; Kieckbusch, J. Maternal uterine natural killer cells nurture fetal growth: In medio stat virtus. Trends Mol. Med. 2015, 21, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Kumpel, B.M.; Manoussaka, M.S. Placental immunology and maternal alloimmune responses. Vox Sang. 2012, 102, 2–12. [Google Scholar] [CrossRef] [PubMed]
- van Kampen, C.A.; Versteeg-vd Voort Maarschalk, M.F.; Langerak-Langerak, J.; Roelen, D.L.; Claas, F.H. Kinetics of the pregnancy-induced humoral and cellular immune response against the paternal HLA class I antigens of the child. Hum. Immunol. 2002, 63, 452–458. [Google Scholar] [CrossRef]
- van Kampen, C.A.; Versteeg-van der Voort Maarschalk, M.F.; Langerak-Langerak, J.; van Beelen, E.; Roelen, D.L.; Claas, F.H. Pregnancy can induce long-persisting primed CTLs specific for inherited paternal HLA antigens. Hum. Immunol. 2001, 62, 201–207. [Google Scholar] [CrossRef]
- Rijnink, E.C.; Penning, M.E.; Wolterbeek, R.; Wilhelmus, S.; Zandbergen, M.; van Duinen, S.G.; Schutte, J.; Bruijn, J.A.; Bajema, I.M. Tissue microchimerism is increased during pregnancy: A human autopsy study. Mol. Hum. Reproduct. 2015, 21, 857–864. [Google Scholar] [CrossRef]
- Bischoff, F.Z.; Sinacori, M.K.; Dang, D.D.; Marquez-Do, D.; Horne, C.; Lewis, D.E.; Simpson, J.L. Cell-free fetal DNA and intact fetal cells in maternal blood circulation: Implications for first and second trimester non-invasive prenatal diagnosis. Hum. Reproduct. Update 2002, 8, 493–500. [Google Scholar] [CrossRef]
- Lutjen, P.; Trounson, A.; Leeton, J.; Findlay, J.; Wood, C.; Renou, P. The establishment and maintenance of pregnancy using in vitro fertilization and embryo donation in a patient with primary ovarian failure. Nature 1984, 307, 174–175. [Google Scholar] [CrossRef] [PubMed]
- van der Hoorn, M.L.; Lashley, E.E.; Bianchi, D.W.; Claas, F.H.; Schonkeren, C.M.; Scherjon, S.A. Clinical and immunologic aspects of egg donation pregnancies: A systematic review. Hum. Reproduct. Update 2010, 16, 704–712. [Google Scholar] [CrossRef] [PubMed]
- van der Hoorn, M.L.; van Egmond, A.; Swings, G.M.; van Beelen, E.; van der Keur, C.; Tirado-Gonzalez, I.; Blois, S.M.; Karumanchi, S.A.; Bianchi, D.W.; Claas, F.H.; et al. Differential immunoregulation in successful oocyte donation pregnancies compared with naturally conceived pregnancies. J. Reproduct. Immunol. 2014, 101–102, 96–103. [Google Scholar] [CrossRef]
- Saito, S.; Nakabayashi, Y.; Nakashima, A.; Shima, T.; Yoshino, O. A new era in reproductive medicine: Consequences of third-party oocyte donation for maternal and fetal health. Semin. Immunopathol. 2016. [Google Scholar] [CrossRef] [PubMed]
- Blazquez, A.; Garcia, D.; Rodriguez, A.; Vassena, R.; Figueras, F.; Vernaeve, V. Is oocyte donation a risk factor for preeclampsia? A systematic review and meta-analysis. J. Assist. Reproduct. Genet. 2016. [Google Scholar] [CrossRef] [PubMed]
- Mol, B.W.; Roberts, C.T.; Thangaratinam, S.; Magee, L.A.; de Groot, C.J.; Hofmeyr, G.J. Pre-eclampsia. Lancet (Lond. Engl.) 2016. [Google Scholar] [CrossRef]
- Dekker, G.A. Risk factors for preeclampsia. Clin. Obstet. Gynecol. 1999, 42, 422–435. [Google Scholar] [CrossRef] [PubMed]
- Duckitt, K.; Harrington, D. Risk factors for pre-eclampsia at antenatal booking: Systematic review of controlled studies. BMJ 2005, 330, 565. [Google Scholar] [CrossRef] [PubMed]
- Talaulikar, V.S.; Arulkumaran, S. Reproductive outcomes after assisted conception. Obstet. Gynecol. Surv. 2012, 67, 566–583. [Google Scholar] [CrossRef] [PubMed]
- Jacobsson, B.; Ladfors, L.; Milsom, I. Advanced maternal age and adverse perinatal outcome. Obstet. Gynecol. 2004, 104, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Geisler, M.E.; O’Mahony, A.; Meaney, S.; Waterstone, J.J.; O’Donoghue, K. Obstetric and perinatal outcomes of twin pregnancies conceived following IVF/ICSI treatment compared with spontaneously conceived twin pregnancies. Eur. J. Obstet. Gynecol. Reproduct. Biol. 2014, 181, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Krieg, S.A.; Henne, M.B.; Westphal, L.M. Obstetric outcomes in donor oocyte pregnancies compared with advanced maternal age in in vitro fertilization pregnancies. Fertil. Steril. 2008, 90, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Masoudian, P.; Nasr, A.; de Nanassy, J.; Fung-Kee-Fung, K.; Bainbridge, S.A.; El Demellawy, D. Oocyte donation pregnancies and the risk of preeclampsia or gestational hypertension: A systematic review and metaanalysis. Am. J. Obstet. Gynecol. 2016, 214, 328–339. [Google Scholar] [CrossRef] [PubMed]
- Schwarze, J.E.; Borda, P.; Vasquez, P.; Ortega, C.; Villa, S.; Crosby, J.A.; Pommer, R. Is the risk of preeclampsia higher in donor oocyte pregnancies? A systematic review and meta-analysis. JBRA Assist. Reproduct. 2017. [Google Scholar] [CrossRef] [PubMed]
- Storgaard, M.; Loft, A.; Bergh, C.; Wennerholm, U.B.; Soderstrom-Anttila, V.; Romundstad, L.B.; Aittomaki, K.; Oldereid, N.; Forman, J.; Pinborg, A. Obstetric and neonatal complications in pregnancies conceived after oocyte donation: A systematic review and meta-analysis. BJOG 2017, 124, 561–572. [Google Scholar] [CrossRef] [PubMed]
- Steegers, E.A.; von Dadelszen, P.; Duvekot, J.J.; Pijnenborg, R. Pre-eclampsia. Lancet (Lond. Engl.) 2010, 376, 631–644. [Google Scholar] [CrossRef]
- Tranquilli, A.L.; Dekker, G.; Magee, L.; Roberts, J.; Sibai, B.M.; Steyn, W.; Zeeman, G.G.; Brown, M.A. The classification, diagnosis and management of the hypertensive disorders of pregnancy: A revised statement from the ISSHP. Pregnancy Hypertens. 2014, 4, 97–104. [Google Scholar] [CrossRef]
- Ghezzi, P.; Jaquet, V.; Marcucci, F.; Schmidt, H. The oxidative stress theory of disease: Levels of evidence and epistemological aspects. Br. J. Pharmacol. 2017, 174, 1784–1796. [Google Scholar] [CrossRef]
- Myatt, L. Review: Reactive oxygen and nitrogen species and functional adaptation of the placenta. Placenta 2010, 31, S66–S69. [Google Scholar] [CrossRef]
- Staff, A.C.; Ranheim, T.; Khoury, J.; Henriksen, T. Increased contents of phospholipids, cholesterol, and lipid peroxides in decidua basalis in women with preeclampsia. Am. J. Obstet. Gynecol. 1999, 180, 587–592. [Google Scholar] [CrossRef]
- Schoots, M.H.; Gordijn, S.J.; Scherjon, S.A.; van Goor, H.; Hillebrands, J.L. Oxidative stress in placental pathology. Placenta 2018. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.M.; Hubel, C.A. Is oxidative stress the link in the two-stage model of pre-eclampsia? Lancet (Lond. Engl.) 1999, 354, 788–789. [Google Scholar] [CrossRef]
- Matsubara, K.; Higaki, T.; Matsubara, Y.; Nawa, A. Nitric oxide and reactive oxygen species in the pathogenesis of preeclampsia. Int. J. Mol. Sci. 2015, 16, 4600–4614. [Google Scholar] [CrossRef] [PubMed]
- Matsubara, K.; Matsubara, Y.; Hyodo, S.; Katayama, T.; Ito, M. Role of nitric oxide and reactive oxygen species in the pathogenesis of preeclampsia. J. Obstet. Gynaecol. Res. 2010, 36, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Roggensack, A.M.; Zhang, Y.; Davidge, S.T. Evidence for peroxynitrite formation in the vasculature of women with preeclampsia. Hypertension 1999, 33, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Holwerda, K.M.; Faas, M.M.; van Goor, H.; Lely, A.T. Gasotransmitters: A solution for the therapeutic dilemma in preeclampsia? Hypertension 2013, 62, 653–659. [Google Scholar] [CrossRef]
- Holwerda, K.M.; Bos, E.M.; Rajakumar, A.; Ris-Stalpers, C.; van Pampus, M.G.; Timmer, A.; Erwich, J.J.; Faas, M.M.; van Goor, H.; Lely, A.T. Hydrogen sulfide producing enzymes in pregnancy and preeclampsia. Placenta 2012, 33, 518–521. [Google Scholar] [CrossRef]
- Lopez-Jaramillo, P.; Arenas, W.D.; Garcia, R.G.; Rincon, M.Y.; Lopez, M. The role of the L-arginine-nitric oxide pathway in preeclampsia. Ther. Adv. Cardiovasc. Dis. 2008, 2, 261–275. [Google Scholar] [CrossRef]
- Eide, I.P.; Isaksen, C.V.; Salvesen, K.A.; Langaas, M.; Schonberg, S.A.; Austgulen, R. Decidual expression and maternal serum levels of heme oxygenase 1 are increased in pre-eclampsia. Acta Obstet. Gynecol. Scand. 2008, 87, 272–279. [Google Scholar] [CrossRef]
- Cortese-Krott, M.M.; Koning, A.; Kuhnle, G.G.C.; Nagy, P.; Bianco, C.L.; Pasch, A.; Wink, D.A.; Fukuto, J.M.; Jackson, A.A.; van Goor, H.; et al. The Reactive Species Interactome: Evolutionary Emergence, Biological Significance, and Opportunities for Redox Metabolomics and Personalized Medicine. Antioxid. Redox Signal. 2017, 27, 684–712. [Google Scholar] [CrossRef] [PubMed]
- Frenay, A.S.; de Borst, M.H.; Bachtler, M.; Tschopp, N.; Keyzer, C.A.; van den Berg, E.; Bakker, S.J.L.; Feelisch, M.; Pasch, A.; van Goor, H. Serum free sulfhydryl status is associated with patient and graft survival in renal transplant recipients. Free Radic. Biol. Med. 2016, 99, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Snijder, P.M.; van den Berg, E.; Whiteman, M.; Bakker, S.J.; Leuvenink, H.G.; van Goor, H. Emerging role of gasotransmitters in renal transplantation. Am. J. Transplant. 2013, 13, 3067–3075. [Google Scholar] [CrossRef] [PubMed]
- Ott, U.; Aschoff, A.; Funfstuck, R.; Jirikowski, G.; Wolf, G. DNA fragmentation in acute and chronic rejection after renal transplantation. Transplant. Proc. 2007, 39, 73–77. [Google Scholar] [CrossRef] [PubMed]
- La Manna, G.; Lanci, N.; Della Bella, E.; Comai, G.; Cappuccilli, M.L.; Nisi, K.; Todeschini, P.; Carretta, E.; Scolari, M.P.; Stefoni, S. Reduction of oxidative damage reflects a better kidney transplantation outcome. Am. J. Nephrol. 2011, 34, 496–504. [Google Scholar] [CrossRef] [PubMed]
- Rassaf, T.; Bryan, N.S.; Kelm, M.; Feelisch, M. Concomitant presence of N-nitroso and S-nitroso proteins in human plasma. Free Radic. Biol. Med. 2002, 33, 1590–1596. [Google Scholar] [CrossRef]
- Rassaf, T.; Feelisch, M.; Kelm, M. Circulating NO pool: Assessment of nitrite and nitroso species in blood and tissues. Free Radic. Biol. Med. 2004, 36, 413–422. [Google Scholar] [CrossRef] [PubMed]
- Raijmakers, M.T.; Zusterzeel, P.L.; Roes, E.M.; Steegers, E.A.; Mulder, T.P.; Peters, W.H. Oxidized and free whole blood thiols in preeclampsia. Obstet. Gynecol. 2001, 97, 272–276. [Google Scholar] [PubMed]
- Seligman, S.P.; Buyon, J.P.; Clancy, R.M.; Young, B.K.; Abramson, S.B. The role of nitric oxide in the pathogenesis of preeclampsia. Am. J. Obstet. Gynecol. 1994, 171, 944–948. [Google Scholar] [CrossRef]
- Anderson, D.F.; Tompsett, S.L. Observations on the inorganic sulphate content of the blood in eclampsia. Brit. J. Exp. Pathol. 1932, 13, 130–132. [Google Scholar]
- Acauan Filho, B.J.; Pinheiro da Costa, B.E.; Ogando, P.B.; Vieira, M.C.; Antonello, I.C.; Poli-de-Figueiredo, C.E. Serum nitrate and NOx levels in preeclampsia are higher than in normal pregnancy. Hypertens. Pregnancy 2016, 35, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Pathak, N.; Sawhney, H.; Vasishta, K.; Majumdar, S. Estimation of oxidative products of nitric oxide (nitrates, nitrites) in preeclampsia. Aust. N. Z. J. Obstet. Gynaecol. 1999, 39, 484–487. [Google Scholar]
- Guerby, P.; Swiader, A.; Auge, N.; Parant, O.; Vayssiere, C.; Uchida, K.; Salvayre, R.; Negre-Salvayre, A. High glutathionylation of placental endothelial nitric oxide synthase in preeclampsia. Redox Biol. 2019, 22, 101126. [Google Scholar] [CrossRef] [PubMed]
- Dawson, P.A. Sulfate in fetal development. Semin. Cell Dev. Biol. 2011, 22, 653–659. [Google Scholar] [CrossRef]
- Kleinbongard, P.; Dejam, A.; Lauer, T.; Jax, T.; Kerber, S.; Gharini, P.; Balzer, J.; Zotz, R.B.; Scharf, R.E.; Willers, R.; et al. Plasma nitrite concentrations reflect the degree of endothelial dysfunction in humans. Free Radic. Biol. Med. 2006, 40, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Lauer, T.; Preik, M.; Rassaf, T.; Strauer, B.E.; Deussen, A.; Feelisch, M.; Kelm, M. Plasma nitrite rather than nitrate reflects regional endothelial nitric oxide synthase activity but lacks intrinsic vasodilator action. Proc. Natl. Acad. Sci. USA 2001, 98, 12814–12819. [Google Scholar] [CrossRef] [PubMed]
- Moncada, S.; Palmer, R.M.; Higgs, E.A. Nitric oxide: Physiology, pathophysiology, and pharmacology. Pharmacol. Rev. 1991, 43, 109–142. [Google Scholar]
- Deng, A.; Engels, K.; Baylis, C. Impact of nitric oxide deficiency on blood pressure and glomerular hemodynamic adaptations to pregnancy in the rat. Kidney Int. 1996, 50, 1132–1138. [Google Scholar] [CrossRef]
- Koning, A.M.; Meijers, W.C.; Pasch, A.; Leuvenink, H.G.D.; Frenay, A.S.; Dekker, M.M.; Feelisch, M.; de Boer, R.A.; van Goor, H. Serum free thiols in chronic heart failure. Pharmacol. Res. 2016, 111, 452–458. [Google Scholar] [CrossRef]
- Dawson, P.A.; Richard, K.; Perkins, A.; Zhang, Z.; Simmons, D.G. Review: Nutrient sulfate supply from mother to fetus: Placental adaptive responses during human and animal gestation. Placenta 2017, 54, 45–51. [Google Scholar] [CrossRef]
- Bender Atik, R.; Christiansen, O.B.; Elson, J.; Kolte, A.M.; Lewis, S.; Middeldorp, S.; Nelen, W.; Peramo, B.; Quenby, S.; Vermeulen, N.; et al. ESHRE guideline: Recurrent pregnancy loss. Hum. Reproduct. Open 2018, 2018. [Google Scholar] [CrossRef]
- Guideline, G.-T. The Investigation and Treatment of Couples with Recurrent First-Trimester and Second-Trimester Miscarriage. 2011. Available online: https://www.rcog.org.uk/globalassets/documents/guidelines/gtg_17.pdf (accessed on 4 March 2019).
- Kleiverda, G.; Derksen, J. Zwangerschapsafbreking tot 24 Weken [Termination of Pregnancy Until 24 Weeks of Gestational Age]. Guidelines of the Netherlands Association for Obstetrics and Gynaecology (NVOG): 2015. Available online: https://www.nvog.nl/wp-content/uploads/2018/02/Zwangerschapsafbreking-tot-24-weken-2.0-28-05-2015.pdf (accessed on 4 March 2019).
- Silver, R.M.; Branch, D.W.; Goldenberg, R.; Iams, J.D.; Klebanoff, M.A. Nomenclature for pregnancy outcomes: Time for a change. Obstet. Gynecol. 2011, 118, 1402–1408. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.A.; Lindheimer, M.D.; de Swiet, M.; Van Assche, A.; Moutquin, J.M. The classification and diagnosis of the hypertensive disorders of pregnancy: Statement from the International Society for the Study of Hypertension in Pregnancy (ISSHP). Hypertens. Pregnancy 2001, 20. [Google Scholar] [CrossRef] [PubMed]
- Hoftiezer, L.; Hukkelhoven, C.W.; Hogeveen, M.; Straatman, H.M.; van Lingen, R.A. Defining small-for-gestational-age: Prescriptive versus descriptive birthweight standards. Eur. J. Pediatr. 2016, 175, 1047–1057. [Google Scholar] [CrossRef] [PubMed]
- Ellman, G.L. Tissue sulfhydryl groups. Arch. Biochem. Biophys. 1959, 82, 70–77. [Google Scholar] [CrossRef]
- Hu, M.L.; Louie, S.; Cross, C.E.; Motchnik, P.; Halliwell, B. Antioxidant protection against hypochlorous acid in human plasma. J. Lab. Clin. Med. 1993, 121, 257–262. [Google Scholar] [PubMed]
- Newton, G.L.; Dorian, R.; Fahey, R.C. Analysis of biological thiols: Derivatization with monobromobimane and separation by reverse-phase high-performance liquid chromatography. Anal. Biochem. 1981, 114, 383–387. [Google Scholar] [CrossRef]
- Farese, S.; Stauffer, E.; Kalicki, R.; Hildebrandt, T.; Frey, B.M.; Frey, F.J.; Uehlinger, D.E.; Pasch, A. Sodium thiosulfate pharmacokinetics in hemodialysis patients and healthy volunteers. Clin. J. Am. Soc. Nephrol. 2011, 6, 1447–1455. [Google Scholar] [CrossRef]
- van den Berg, E.; Pasch, A.; Westendorp, W.H.; Navis, G.; Brink, E.J.; Gans, R.O.; van Goor, H.; Bakker, S.J. Urinary sulfur metabolites associate with a favorable cardiovascular risk profile and survival benefit in renal transplant recipients. J. Am. Soc. Nephrol. 2014, 25, 1303–1312. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| ART | Naturally Conceived | Oocyte Donation | Naturally Conceived | Oocyte Donation | |
|---|---|---|---|---|---|
| Complication | Uncomplicated | Uncomplicated | Pre-Eclampsia | Pre-Eclampsia | |
| Maternal characteristics | n = 23 | n = 27 | n = 24 | n = 5 | Overall sig. |
| Maternal Age (years), mean (SD) | 31.8 (5.2) | 41.1 (6.4) * | 30.8 (5.8) | 40.0 (7.2) # | p < 0.001 a |
| BMI (kg/m2), median (range) | 25.1 (18.8–37.8) | 24.3 (16.9–31.6) | 24.6 (19.3–36.8) | 25.3 (20.7–27.2) | ns a |
| Smoking, number (%) | 2 (9.5) | 1 (5) | 6 (26.1) | 1 (20.0) | ns c |
| Gravidity, median (range) | 1 (1–8) | 2 (1–8) | 1 (1–5) | 1 (1–10) | ns a |
| Gravidity 1, number (%) | 12 (52.2) | 9 (36.0) | 14 (58.3) | 3 (60.0) | ns c |
| Parity, median (range) | 0 (0–3) | 0 (0–1) | 0 (0–4) | 0 (0–0) | ns a |
| Parity 0, number (%) | 13 (56.5) | 15 (60.0) | 19 (79.2) | 5 (100) | ns c |
| Obstetrical history | n = 11 | n = 15 | n = 10 | n = 2 | |
| Previous pregnancies | n = 26 | n = 39 | n = 15 | n = 10 | |
| Miscarriage, number (%) | 8 (30.8) | 27 (69.2) | 7 (46.7) | 8 (80.0) | p < 0.05 c |
| Abortion, number (%) | 1 (3.8) | 0 | 1 (6.7) | 0 | ns c |
| EUG, number (%) | 0 | 3 (7.7) | 0 | 2 (20) | ns c |
| TOP, number (%) | 0 | 0 | 1 (6.7) | 0 | ns c |
| Pre-term birth, number (%) | 0 | 2 (5.1) | 1 (6.7) | 0 | ns c |
| IUFD, number (%) | 0 | 0 | 1 (6.7) | 0 | ns c |
| Gestational hypertension, number (%) | 0 | 2 (5.1) | 1 (6.7) | 0 | ns c |
| Pre-eclampsia, number (%) | 0 | 0 | 1 (6.7) | 0 | ns c |
| Gestational diabetes, number (%) | 0 | 0 | 0 | 0 | |
| Pregnancies without complications, number (%) | 17 (65.4) | 5 (12.8) * | 3 (20) * | 0 | p < 0.05 c |
| Pregnancy characteristics | |||||
| ART, number (%) | 0 | 27 (100) * | 0 | 5 (100) # | p < 0.001 c |
| Hypertension, number (%) | 3 (13.6) | 4 (17.4) | 24 (100) * | 5 (100) & | p < 0.001 c |
| Highest diastolic BP, (mmHg), mean (SD) | 74 (10) | 82 (10) * | 101 (9) * | 101 (11) & | p < 0.001 a |
| Proteinuria, number (%) | 0 | 0 | 23 (95.8) * | 5 (100) & | p < 0.001 c |
| Pre-eclampsia, number (%) | 0 | 0 | 24 (100) * | 5 (100) & | p < 0.001 c |
| HELLP-syndrome, number (%) | 0 | 0 | 4 (16.7) * | 0 | p = 0.022 c |
| Gestational age (days), median (range (days)) | 275 (269–290) | 279 (231–290) | 243 (198–283) * | 217 (204–270) & | p < 0.001 a |
| Preterm birth, number (%) | 0 | 1 (4.2) | 18 (75.0) * | 4 (80.0) & | p < 0.001 c |
| Gestational diabetes, number (%) | 0 | 0 | 0 | 0 | |
| Delivery, vaginal, number (%) | 6 (26.1) | 11 (45.8) | 12 (50.0) | 1 (25.0) | |
| Delivery, CS, number (%) | 17 (73.9) | 13 (54.2) | 12 (50.0) | 3 (75.0) | ns c |
| Twin, number (%) | 0 | 2 (7.4) | 0 | 1 (20.0) | ns c |
| Fetal characteristics | n = 23 | n = 29 | n = 24 | n = 6 | |
| Sex, male/female (%male) | 16/7 (69.6) | 10/18 (35.7) * | 14/10 (58.3) | 3/3 (50.0) | ns c |
| Birthweight (gram), median (range) | 3455 (2445–4415) | 3500 (1611–4500) | 2372 (705–4030) * | 1319 (1100–3855) & | p < 0.001 a |
| Small for gestational age, number (%) | 1 (4.3) | 5 (19.2) | 10 (41.7) * | 3 (50.0) | p < 0.01 c |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bos, M.; Schoots, M.H.; Fernandez, B.O.; Mikus-Lelinska, M.; Lau, L.C.; Eikmans, M.; van Goor, H.; Gordijn, S.J.; Pasch, A.; Feelisch, M.; et al. Reactive Species Interactome Alterations in Oocyte Donation Pregnancies in the Absence and Presence of Pre-Eclampsia. Int. J. Mol. Sci. 2019, 20, 1150. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20051150
Bos M, Schoots MH, Fernandez BO, Mikus-Lelinska M, Lau LC, Eikmans M, van Goor H, Gordijn SJ, Pasch A, Feelisch M, et al. Reactive Species Interactome Alterations in Oocyte Donation Pregnancies in the Absence and Presence of Pre-Eclampsia. International Journal of Molecular Sciences. 2019; 20(5):1150. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20051150
Chicago/Turabian StyleBos, Manon, Mirthe H. Schoots, Bernadette O. Fernandez, Monika Mikus-Lelinska, Laurie C. Lau, Michael Eikmans, Harry van Goor, Sanne J. Gordijn, Andreas Pasch, Martin Feelisch, and et al. 2019. "Reactive Species Interactome Alterations in Oocyte Donation Pregnancies in the Absence and Presence of Pre-Eclampsia" International Journal of Molecular Sciences 20, no. 5: 1150. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20051150