Therapeutic Approaches with Intravitreal Injections in Geographic Atrophy Secondary to Age-Related Macular Degeneration: Current Drugs and Potential Molecules

 , , and
, , and
Abstract
:
1. Introduction
2. Methods
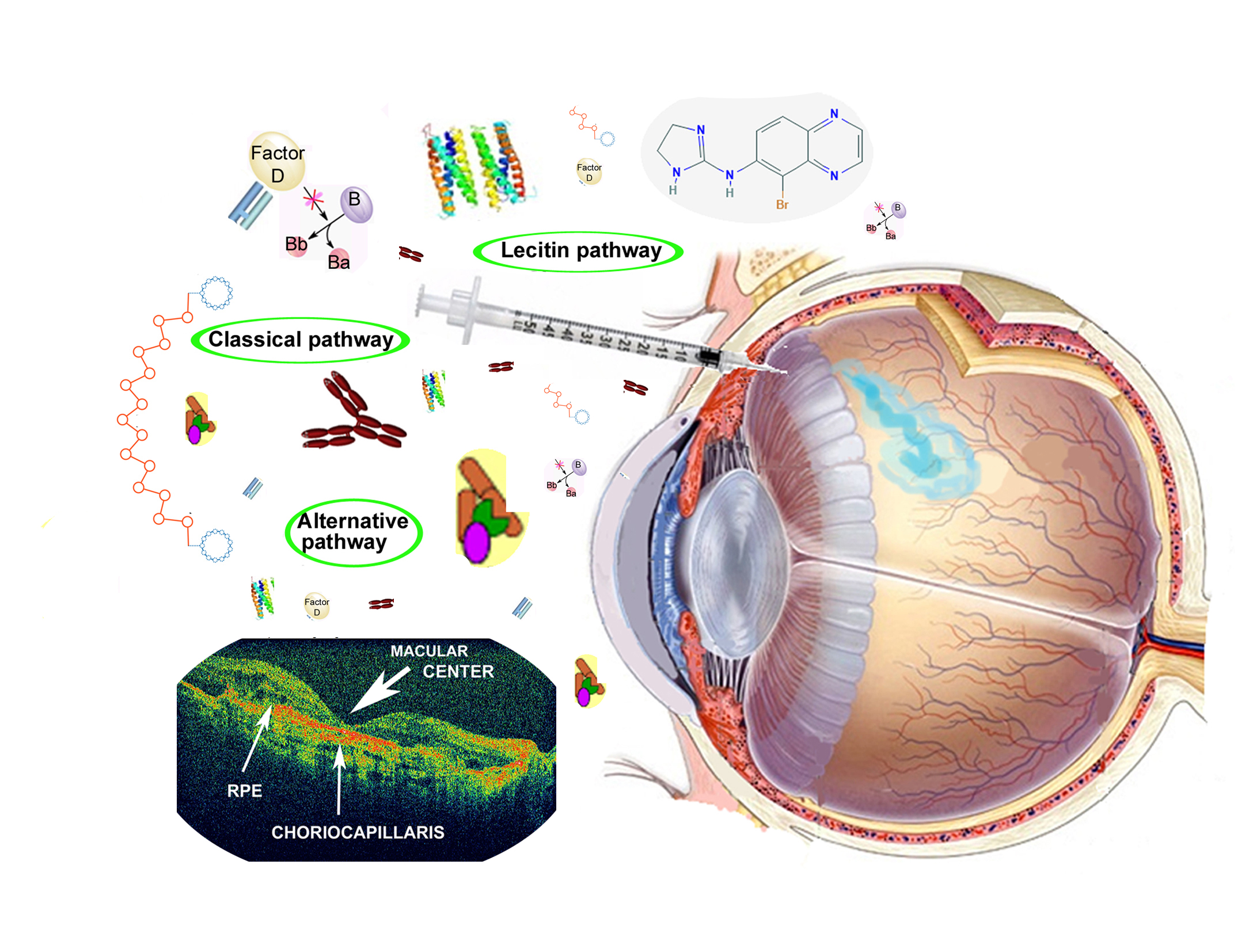
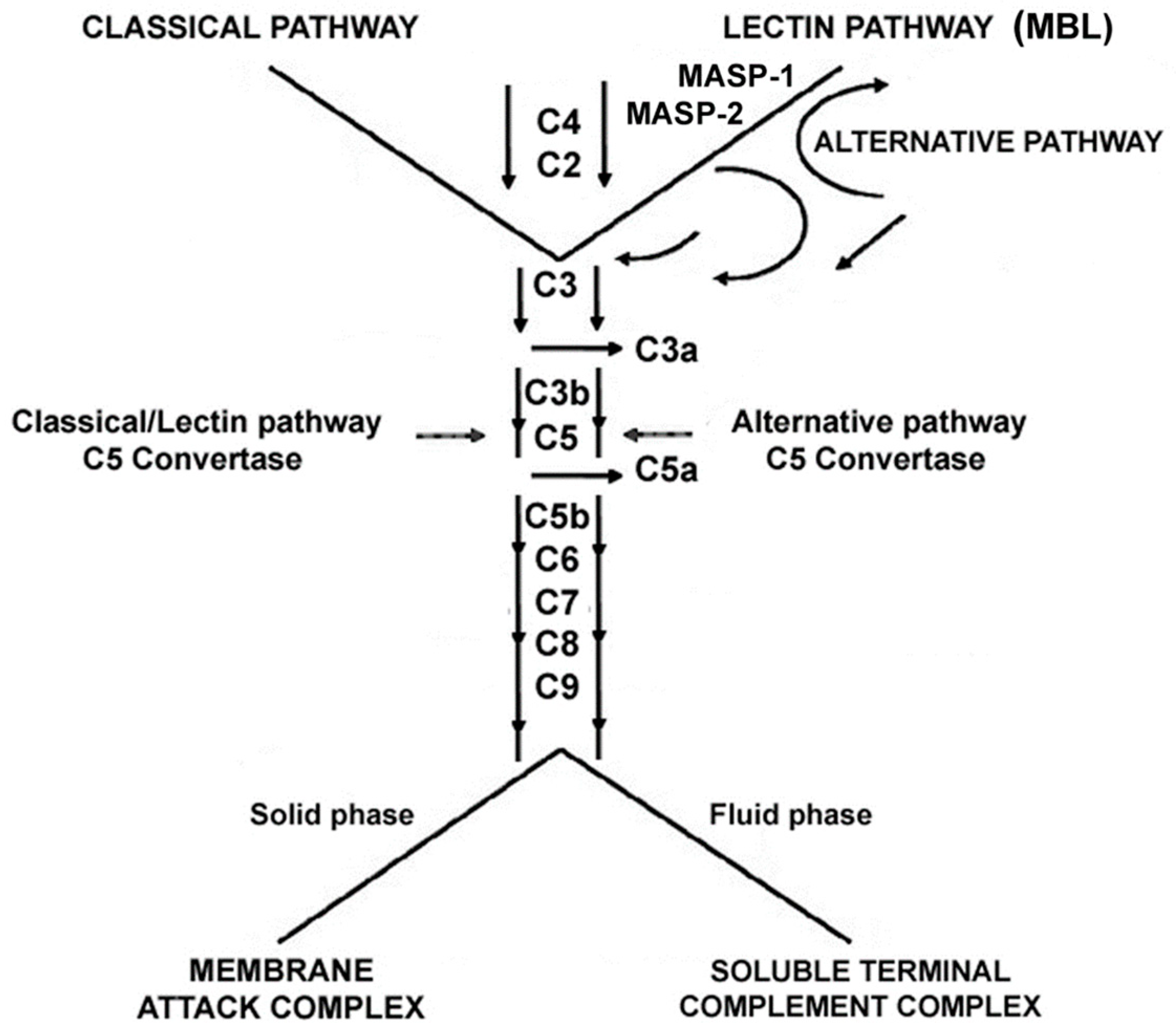
3. Main Pathogenetic Pathways in Dry AMD: Complement Dysfunction and Inflammation
4. Potential Therapeutic Molecules in Dry AMD
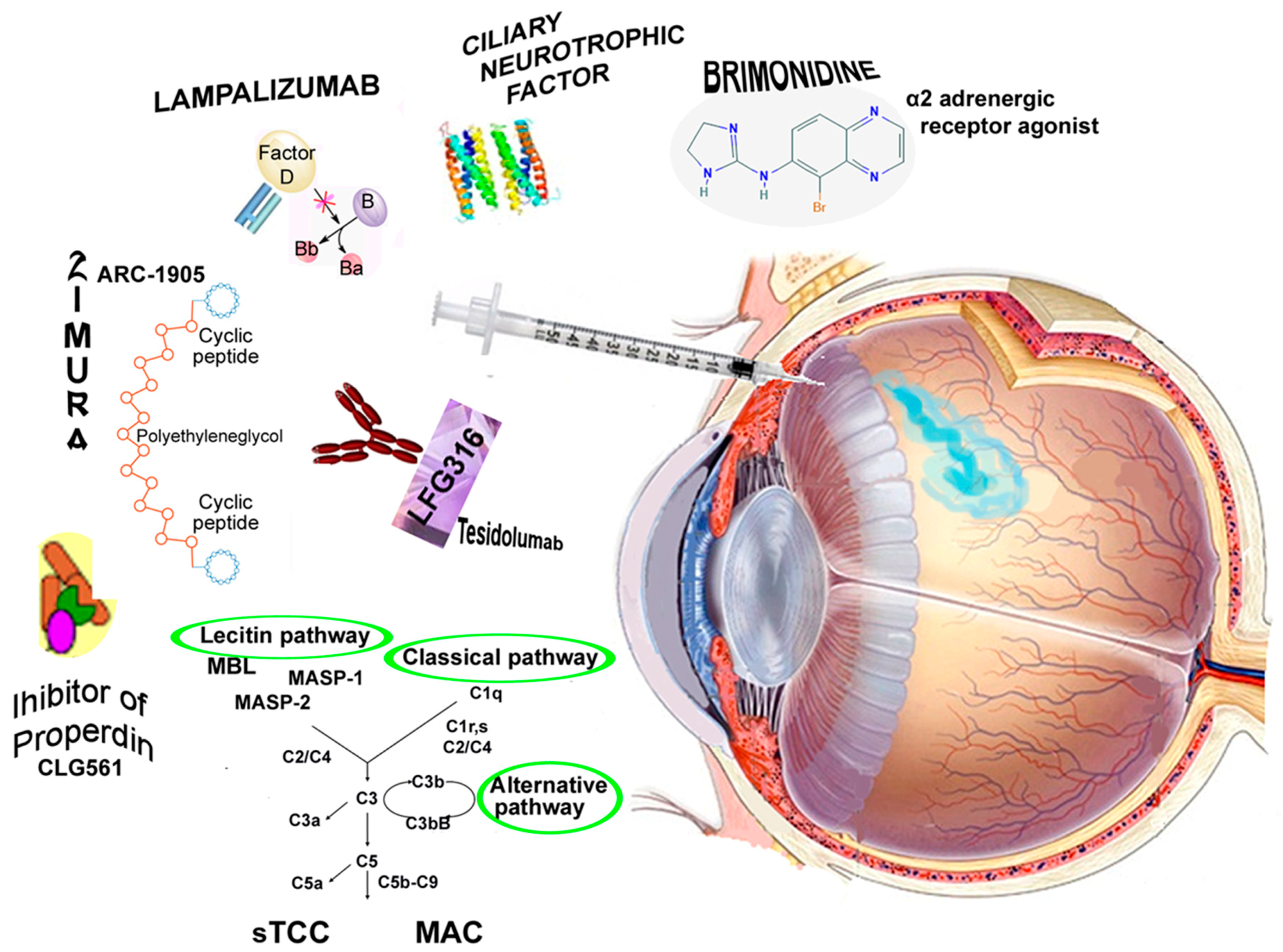
4.1. Neuroprotective Agents Designed to Prevent Retinal Ganglion Cell Apoptosis
4.1.1. Brimonidine
4.1.2. Ciliary Neurotrophic Factor
4.2. Immune Modulating or Anti-Inflammatory Agents
4.2.1. Lampalizumab
4.2.2. Zimura
4.2.3. POT-4 and APL-2
4.2.4. CLG561
4.2.5. LFG316
4.2.6. Suppressors of Inflammation: Iluvien
4.3. Anti-Oxidative Stress
Risuteganib (Luminate)
4.4. Other Treatment Modalities
Ocular Gene Therapy: AAVCAGsCD59
4.5. Novel Compounds Derived from High-Throughput Drug Screens
RO7171009
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Wong, W.L.; Su, X.; Li, X.; Cheung, C.M.; Klein, R.; Cheng, C.Y.; Wong, T.Y. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: A systematic review and meta-analysis. Lancet Glob. Health 2014, 2, e106–e116. [Google Scholar] [CrossRef]
- Kandasamy, R.; Wickremasinghe, S.; Guymer, R. New treatment modalities for geographic atrophy. Asia Pac. J. Ophthalmol. 2017, 6, 508–513. [Google Scholar]
- Holz, F.G.; Strauss, E.C.; Schmitz-Valckenberg, S.; van Lookeren Campagne, M. Geographic atrophy: Clinical features and potential therapeutic approaches. Ophthalmology 2014, 121, 1079–1091. [Google Scholar] [CrossRef] [PubMed]
- Patel, H.R.; Eichenbaum, D. Geographic atrophy: Clinical impact and emerging treatments. Ophthalmic Surg. Lasers Imaging Retina 2015, 46, 8–13. [Google Scholar] [CrossRef]
- Chew, E.Y.; Clemons, T.E.; Agron, E.; Sperduto, R.D.; Sangiovanni, J.P.; Davis, M.D.; Ferris, F.L., 3rd; Age-Related Eye Disease Study Research Group. Ten-year follow-up of age-related macular degeneration in the Age-Related Eye Disease Study: AREDS report no. 36. JAMA Ophthalmol. 2014, 132, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Hanus, J.; Zhang, H.; Wang, Z.; Liu, Q.; Zhou, Q.; Wang, S. Induction of necrotic cell death by oxidative stress in retinal pigment epithelial cells. Cell Death Dis. 2013, 4, e965. [Google Scholar] [CrossRef] [PubMed]
- Ding, X.; Patel, M.; Chan, C.C. Molecular pathology of age-related macular degeneration. Prog. Retin. Eye Res. 2009, 28, 1–18. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, V.M.; Chan, C.C. The role of anti-inflammatory agents in age-related macular degeneration (AMD) treatment. Eye 2011, 25, 127–139. [Google Scholar] [CrossRef]
- Weber, B.H.; Charbel Issa, P.; Pauly, D.; Herrmann, P.; Grassmann, F.; Holz, F.G. The role of the complement system in age-related macular degeneration. Dtsch. Arztebl. Int. 2014, 111, 133–138. [Google Scholar] [CrossRef]
- Hanus, J.; Zhao, F.; Wang, S. Current therapeutic developments in atrophic age-related macular degeneration. Br. J. Ophthalmol. 2016, 100, 122–127, Review. Erratum in: Br. J. Ophthalmol. 2016, 100, 744. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Chintalapudi, S.R.; Jablonski, M.M. Current drug and molecular therapies for the treatment of atrophic age-related macular degeneration: Phase I to phase III clinical development. Expert Opin. Investig. Drugs. 2017, 26, 1103–1114. [Google Scholar] [CrossRef]
- Nebbioso, M.; Buomprisco, G.; Pascarella, A.; Pescosolido, N. Modulatory effects of 1,25-dihydroxyvitamin D3 on eye disorders: A critical review. Crit. Rev. Food Sci. Nutr. 2017, 57, 559–565. [Google Scholar] [CrossRef]
- Nizari, S.; Guo, L.; Davis, B.M.; Normando, E.M.; Galvao, J.; Turner, L.A.; Bizrah, M.; Dehabadi, M.; Tian, K.; Cordeiro, M.F. Non-amyloidogenic effects of α2 adrenergic agonists: Implications for brimonidine-mediated neuroprotection. Cell Death Dis. 2016, 7, e2514. [Google Scholar] [CrossRef]
- Doozandeh, A.; Yazdani, S. Neuroprotection in Glaucoma. J. Ophthalmic Vis. Res. 2016, 11, 209–220. [Google Scholar] [CrossRef]
- Zhang, K.; Hopkins, J.J.; Heier, J.S.; Birch, D.G.; Halperin, L.S.; Albini, T.A.; Brown, D.M.; Jaffe, G.J.; Tao, W.; Williams, G.A. Ciliary neurotrophic factor delivered by encapsulated cell intraocular implants for treatment of geographic atrophy in age-related macular degeneration. Proc. Natl. Acad. Sci. USA 2011, 108, 6241–6245. [Google Scholar] [CrossRef]
- Lambert, P.D.; Anderson, K.D.; Sleeman, M.W.; Wong, V.; Tan, J.; Hijarunguru, A.; Corcoran, T.L.; Murray, J.D.; Thabet, K.E.; Yancopoulos, G.D.; et al. Ciliary neurotrophic factor activates leptin-like pathways and reduces body fat, without cachexia or rebound weight gain, even in leptin-resistant obesity. Proc. Natl. Acad. Sci. USA 2001, 98, 4652–4657. [Google Scholar] [CrossRef]
- Thanos, C.G.; Bell, W.J.; O’Rourke, P.; Kauper, K.; Sherman, S.; Stabila, P.; Tao, W. Sustained secretion of ciliary neurotrophic factor to the vitreous, using the encapsulated cell therapy-based NT-501 intraocular device. Tissue Eng. 2004, 10, 1617–1622. [Google Scholar] [CrossRef]
- Kauper, K.; McGovern, C.; Sherman, S.; Heatherton, P.; Rapoza, R.; Stabila, P.; Dean, B.; Lee, A.; Borges, S.; Bouchard, B.; et al. Two-year intraocular delivery of ciliary neurotrophic factor by encapsulated cell technology implants in patients with chronic retinal degenerative diseases. Invest. Ophthalmol. Vis. Sci. 2012, 53, 7484–7491. [Google Scholar] [CrossRef]
- Do, D.V.; Pieramici, D.J.; van Lookeren Campagne, M.; Beres, T.; Friesenhahn, M.; Zhang, Y.; Strauss, E.C. A phase ia dose-escalation study of the anti-factor D monoclonal antibody fragment FCFD4514S in patients with geographic atrophy. Phase Ia Investigators. Retina 2014, 34, 313–320. [Google Scholar] [CrossRef]
- Yaspan, B.L.; Williams, D.F.; Holz, F.G.; Regillo, C.D.; Li, Z.; Dressen, A.; van Lookeren Campagne, M.; Le, K.N.; Graham, R.R.; Beres, T.; et al. Targeting factor D of the alternative complement pathway reduces geographic atrophyprogression secondary to age-related macular degeneration. MAHALO Study Investigators. Sci. Transl. Med. 2017, 9, eaaf1443. [Google Scholar]
- Holz, F.G.; Sadda, S.R.; Busbee, B.; Chew, E.Y.; Mitchell, P.; Tufail, A.; Brittain, C.; Ferrara, D.; Gray, S.; Honigberg, L.; et al. Efficacy and Safety of Lampalizumab for geographic atrophy due to age-related macular degeneration: Chroma and Spectri phase 3 randomized clinical trials. JAMA Ophthalmol. 2018, 136, 666–677. [Google Scholar] [CrossRef]
- Hariri, A.; Nittala, M.G.; Sadda, S.R. Outer retinal tubulation as a predictor of the enlargement amount of geographic atrophy in age-related macular degeneration. Ophthalmology 2015, 122, 407–413. [Google Scholar] [CrossRef]
- Wei, Y.; Liao, H.; Ye, J. Therapeutic effects of various therapeutic strategies on non-exudative age-related macular degeneration: A PRISMA-compliant network meta-analysis of randomized controlled trials. Medicine 2018, 97, e10422. [Google Scholar] [CrossRef]
- Drolet, D.W.; Green, L.S.; Gold, L.; Janjic, N. Fit for the Eye: Aptamers in Ocular Disorders. Nucleic Acid Ther. 2016, 26, 127–146. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; Zu, Y. A Highlight of recent advances in aptamer technology and its application. Molecules 2015, 20, 11959–11980. [Google Scholar] [CrossRef]
- Kassa, E.; Ciulla, T.A.; Hussain, R.M.; Dugel, P.U. Complement inhibition as a therapeutic strategy in retinal disorders. Expert Opin. Biol. Ther. 2019. [Google Scholar] [CrossRef]
- Kaushal, S.; Grossi, F.; Francois, C.; Slakter, J. ASaP Study Group. Complement C3 inhibitor POT-4: Clinical Safety of Intravitreal Administration. Invest. Ophthalmol. Vis. Sci. 2009, 50, 5010. [Google Scholar]
- Singer, M. Advances in the management of macular degeneration. F1000Prime Rep. 2014, 6, 29. [Google Scholar] [CrossRef] [PubMed]
- Ricklin, D.; Lambris, J.D. New milestones ahead in complement-targeted therapy. Semin. Immunol. 2016, 28, 208–222. [Google Scholar] [CrossRef]
- Sagar, A.; Dai, W.; Minot, M.; LeCover, R.; Varner, J.D. Reduced order modeling and analysis of the human complement system. PLoS ONE 2017, 12, e0187373. [Google Scholar] [CrossRef]
- Taskintuna, I.; Abdalla Elsayed, M.E.A.; Schatz, P. Update on clinical trials in dry age-related macular degeneration. Middle East Afr. J. Ophthalmol. 2016, 23, 13–26. [Google Scholar] [PubMed]
- Kaiser, P.K.; Boyer, D.S.; Campochiaro, P.A.; Heier, J.; Kornfield, J.; Kuppermann, B.D.; Quiroz-Mercado, H.; Karageozian, L.; Kutscher, L.; Karpus, M.; et al. Topline results from a prospective, double-masked, placebo-controlled phase-2b clinical study evaluating ALG-1001 (Luminate) in patients with diabetic macular edema. Invest. Ophthalmol. Vis. Sci. 2017, 58, 2029. [Google Scholar]
- Available online: https://clinicaltrials.gov/ct2/show/results/NCT03144999 (accessed on 29 March 2017).
- Available online: https://clinicaltrials.gov/ct2/show/NCT03295877 (accessed on 21 September 2017).
- Al-Shahwan, S.; Al-Torbak, A.A.; Turkmani, S.; Al-Omran, M.; Al-Jadaan, I.; Edward, D.P. Side-effect profile of brimonidine tartrate in children. Ophthalmology 2005, 112, 2143. [Google Scholar] [CrossRef]
- Saylor, M.; McLoon, L.K.; Harrison, A.R.; Lee, M.S. Experimental and clinical evidence for brimonidine as an optic nerve and retinal neuroprotective agent: An evidence-based review. Arch Ophthalmol. 2009, 127, 402–406. [Google Scholar] [CrossRef]
- Fuhrmann, S.; Grabosch, K.; Kirsch, M.; Hofmann, H.D. Distribution of CNTF receptor alpha protein in the central nervous system of the chick embryo. J. Comp. Neurol. 2003, 461, 111–122. [Google Scholar] [CrossRef]
- Tao, W.; Wen, R.; Goddard, M.B.; Sherman, S.D.; O’Rourke, P.J.; Stabila, P.F.; Bell, W.J.; Dean, B.J.; Kauper, K.A.; Budz, V.A.; et al. Encapsulated cell-based delivery of CNTF reduces photoreceptor degeneration in animal models of retinitis pigmentosa. Invest. Ophthalmol. Vis. Sci. 2002, 43, 3292–3298. [Google Scholar]
- Kimura, A.; Namekata, K.; Guo, X.; Harada, C.; Harada, T. Neuroprotection, growth factors and BDNF-TrkB signalling in retinal degeneration. Int. J. Mol. Sci. 2016, 17, 1584. [Google Scholar] [CrossRef]
- Blumenkranz, M.S.; Leung, L.S.; Martin, D.F.; Rosenfeld, P.J.; Zarbin, M.A. Pharmacotherapy of Age-Related Macular Degeneration. Retina 2013, 67, 1213–1255. [Google Scholar]
- Boyer, D.S.; Schmidt-Erfurth, U.; van Lookeren Campagne, M.; Henry, E.C.; Brittain, C. The pathophysiology of geographic atrophy secondary to age-related macular degeneration and the complement pathway as a therapeutic target. Retina 2017, 37, 819–835. [Google Scholar] [CrossRef]
- Volz, C.; Pauly, D. Antibody therapies and their challenges in the treatment of age-related macular degeneration. Eur. J. Pharm. Biopharm. 2015, 95, 158–172. [Google Scholar] [CrossRef] [PubMed]
- Cavallotti, C.; Artico, M.; Pescosolido, N.; Leali, F.M.; Feher, J. Age-related changes in the human retina. Can. J. Ophthalmol. 2004, 39, 61–68. [Google Scholar] [CrossRef]
- Bianchi, E.; Ripandelli, G.; Taurone, S.; Feher, J.; Plateroti, R.; Kovacs, I.; Magliulo, G.; Orlando, M.P.; Micera, A.; Battaglione, E.; et al. Age and diabetes related changes of the retinal capillaries: An ultrastructural and immunohistochemical study. Int. J. Immunopathol. Pharmacol. 2016, 29, 40–53. [Google Scholar] [CrossRef] [PubMed]
- Nebbioso, M.; Barbato, A.; Pescosolido, N. Scotopic microperimetry in the early diagnosis of age-related macular degeneration: Preliminary study. Biomed. Res. Int. 2014, 2014, 671529. [Google Scholar] [CrossRef] [PubMed]
- Fleckenstein, M.; Mitchell, P.; Freund, K.B.; Sadda, S.; Holz, F.G.; Brittain, C.; Henry, E.C.; Ferrara, D. The Progression of Geographic Atrophy Secondary to Age-Related Macular Degeneration. Ophthalmology. 2018, 125, 369–390. [Google Scholar] [CrossRef]
- World Health Organization (WHO). ICD-10 Version: 2016. 2016. Available online: http://apps.who.int/classifications/icd10/browse/2016/en#/H35 (accessed on 2 February 2017).
- Centers for Disease Control (CDC). International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM): 2016 Version. 2016. Available online: https://www.cdc.gov/nchs/icd/icd10cm.htm (accessed on 8 February 2017).
- World Health Organization (WHO). ICD-11 Beta Draft (Mortality and Morbidity Statistics). 2017. Available online: http://id.who.int/icd/entity/627268703 (accessed on 2 February 2017).
- American Academy of Ophthalmology (AAO). ICD10-CM: Subspecialty ICD-10 Decision Trees and Guides; 2016. Available online: https://www.aao.org/practice-management/coding/icd-10-cm (accessed on 2 February 2017).
- Centers for Disease Control (CDC). International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM): 2017 Version. 2017. Available online: https://www.cdc.gov/nchs/icd/icd10cm.htm (accessed on 8 February 2017).
- Holz, F.G.; Sadda, S.R.; Staurenghi, G.; Lindner, M.; Bird, A.C.; Blodi, B.A.; Bottoni, F.; Chakravarthy, U.; Chew, E.Y.; Csaky, K.; et al. Imaging protocols in clinical studies in advanced age-related macular degeneration: Recommendations from classification of atrophy consensus meetings. Ophthalmology 2017, 124, 464–478. [Google Scholar] [CrossRef] [PubMed]
- Lambiase, A.; Coassin, M.; Tirassa, P.; Mantelli, F.; Aloe, L. Nerve growth factor eye drops improve visual acuity and electrofunctional activity in age-related macular degeneration: A case report. Ann. Ist. Super. Sanità. 2009, 45, 439–442. [Google Scholar] [CrossRef] [PubMed]
- Limoli, P.G.; Vingolo, E.M.; Morales, M.U.; Nebbioso, M.; Limoli, C. Preliminary study on electrophysiological changes after cellular autograft in age-related macular degeneration. Medicine 2014, 93, e355. [Google Scholar] [CrossRef] [PubMed]
- Limoli, P.G.; Limoli, C.; Vingolo, E.M.; Scalinci, S.Z.; Nebbioso, M. Cell surgery and growth factors in dry age-related macular degeneration: Visual prognosis and morphological study. Oncotarget 2016, 7, 46913–46923. [Google Scholar] [CrossRef]
- Limoli, P.G.; Vingolo, E.M.; Limoli, C.; Scalinci, S.Z.; Nebbioso, M. Regenerative therapy by suprachoroidal cell autograft in dry age-related macular degeneration: Preliminary in vivo report. J. Vis. Exp. 2018, 132. [Google Scholar] [CrossRef]
- Cocco, L.; Rubbini, S.; Manzoli, L.; Billi, A.M.; Faenza, I.; Peruzzi, D.; Matteucci, A.; Artico, M.; Gilmour, R.S.; Rhee, S.G. Inositides in the nucleus: Presence and characterisation of the isozymes of phospholipasebeta family in NIH 3T3 cells. Biochim. Biophys. Acta 1999, 1438, 295–299. [Google Scholar] [CrossRef]
- Jha, K.A.; Pentecost, M.; Lenin, R.; Klaic, L.; Elshaer, S.L.; Gentry, J.; Russell, J.M.; Beland, A.; Reiner, A.; Jotterand, V.; et al. Concentrated conditioned media from adipose tissue derived mesenchymal stem cells mitigates visual deficits and retinal inflammation following mild traumatic brain injury. Int. J. Mol. Sci. 2018, 19. [Google Scholar] [CrossRef] [PubMed]
- Cheng, W.S.; Lu, D.W.; Chiang, C.H.; Chang, C.J. Overview of clinical trials for dry age-related macular degeneration. J. Med. Sci. 2017, 37, 121–129. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Target | Drug | Action of the Drug | Studies | Authors |
|---|---|---|---|---|
| Neuroprotectors | Brimonidine Tartrate; α2 adrenergic receptor agonist | Prevents RGCs death via the non-amyloidogenic Aβ-pathway | NCT00658619 (2011) Ph1; NCT02087085 (2019) Ph2 (Beacon Allergan Inc., Dublin, Ireland) | Nizari, et al., 2016 [13]; Doozandeh, et al., 2016 [14] |
| Ciliary neurotrophic factor; Encapsulated cell technology (ECT) and NT-501 implant | Member of the IL-6 family of neuropoietic cytokines, prevents photoreceptors degeneration | NCT00063765 (2006) Ph1; NCT00447954 (2009) Ph2; NCT00447993 (2009) Ph2; NCT00447980 (2010) Ph2 (Neurotech Pharmaceuticals, Cumberland, RI, USA) | Zhang, et al., 2011 [15]; Lambert, et al.2001 [16]; Thanos, et al., 2004 [17]; Kauper, et al., 2012 [18] | |
| Immune modulating antinflammatory or complement inhibitors | Lampalizumab; Humanized monoclonal antibody | Inhibits complement factor D (CFD)–mediated activation and amplification of the alternative complement pathway | NCT01229215 (2013) Ph2 Mahalo; NCT02247479 (2018) Ph3 Chroma; NCT02247531 (2018) Ph3 Spectri (Genentech/Roche, South San Francisco, CA, USA) | Do, et al., 2014 [19]; Yaspan, et al., 2017 [20]; Holz, et al., 2018 [21] |
| Zimura (ARC-1905); Single strand nucleic acid aptamer | Inhibits the cleavage of C5 and prevents the formation of the membrane attack complex (MAC) | NCT00950638 (2012) Ph1; NCT03362190 (2018) Ph2/3; NCT02686658 (2018) Ph2 (Ophthotech/Archemix, New York, NY, USA) | Hariri, et al., 2015 [22]; Wei, et al., 2018 [23]; Drolet, et al., 2016 [24]; Sun, et al., 2015 [25] | |
| APL-2; POT-4/AL-78898A; Synthetic cyclic peptide; conjugated to polyethylene glycol polymer. It is a modified version of POT-4 designed to have longer half-life | Binds to C3 blocking all three pathways of complement activation | NCT000473928 (2017) Ph1; NCT02503332 (2018) Ph 2 Filly; NCT03525613 (2022) Ph3 Oaks; NCT03525600 (2022) Ph3 Derby (Apellis Pharmaceuticals Inc., Crestwood, KY, USA) | Kassa, et al., 2019 [26] | |
| POT-4; AL-78898A. Cyclic peptide | Inhibits complement pathways and prevent MAC formation | NCT00473928 (2010) Ph1 (Alcon Inc., Fort Worth, TX, USA) | Kaushal, et al., 2009 [27]; Singer, et al., 2014 [28] | |
| CLG561; Inhibitor of properdin | Stabilizes the alternative pathway C3 and C5 convertases | NCT01835015 (2016) Ph1; NCT02515942 (2018) Ph2; (Novartis, Basel, Switzerland; and Alcon Inc., Fort Worth, TX, USA) | Kassa, et al., 2019 [26]; Ricklin, et al., 2016 [29] | |
| LFG316; Tesidolumab; Human IgG1 | Inhibits the complement system | NCT01255462 (2011) Ph1; NCT02515942 (2018) Ph2; NCT01527500 (2018) Ph2 (Novartis Pharmaceuticals, Basel, Switzerland,) | Kassa, et al., 2019 [26]; Ricklin, et al., 2016 [29]; Sagar, et al., 2017 [30] | |
| Suppressors of inflammation | Iluvien; Fluocinolone acetonide; Corticosteroid | Vasoconstriction, release of inflammatory mediators, mitotic activity, suppression of membrane permeability, and immune response | NCT00695318 (2013) Ph2 (Alimera Sciences, Alpharetta, GA, USA) | Taskintuna, et al., 2016 [31] |
| Anti-oxidative stress | Risuteganib; Anti-Integrin; Luminate (Alg-1001) | Downregulates oxidative stress and restores homeostasis | NCT03626636 Ph2 (Allegro Ophthalmics, LLC, San Juan Capistrano, CA, USA) | Kaiser, 2017 [32] |
| Other treatment modalities | AAVCAGsCD59; HMR59; Ocular gene therapy | Gene therapy expressing C59 complement factor. Soluble recombinant version of the CD59 inhibiting the formation of the MAC | NCT03144999 Ph1 (Hemera Biosciences, Waltham, MA, USA) | Clinicaltrials.gov; No Authors [33] |
| Novel Compounds | RO7171009; RG6147 | Undefined mechanism | NCT03295877 Ph1 (Genentech/Roche, South San Francisco, CA, USA) | Clinicaltrials.gov; No Authors [34] |
| Definitions of Dry AMD or Non-Exudative AMD According to the WHO | ||
|---|---|---|
| World Health Organization (WHO). ICD-10 2016 [47]. Centers for Disease Control (CDC). International Classification of Diseases, Clinical Modification (ICD-10-CM): 2016 [48] | World Health Organization (WHO). ICD-11 Beta Draft (Mortality and Morbidity Statistics); 2017 [49] | American Academy of Ophthalmology (AAO). ICD10-CM: subspecialty ICD-10 decision trees and guides; 2016 [50]. Centers for Disease Control (CDC). International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM): 2017 [51] |
| Non-exudative AMD Any AMD with no choroidal neovascularization, including early, intermediate AMD, and geographic atrophy (GA) | Initial dry AMD Combination of multiple small drusen, some medium drusen (diameter 63–124 µm), or retinal pigment epithelial (RPE) irregularities | Initial AMD Numerous small drusen (≤63 µm), some medium drusen (>63 and ≤124 µm), or RPE irregularities. |
| Progressive dry AMD Medium drusen, one or more large drusen (diameter 125 µm), or GA without involvement of the fovea | Progressive dry AMD Extensive medium drusen (>63 and ≤124 µm), or 1 or more large druse (>125 µm) | |
| Terminal GA GA involving the center of the fovea | Advanced GA GA not involving the center of the fovea | |
| Terminal Geographic Atrophic GA involving the center of the fovea | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nebbioso, M.; Lambiase, A.; Cerini, A.; Limoli, P.G.; La Cava, M.; Greco, A. Therapeutic Approaches with Intravitreal Injections in Geographic Atrophy Secondary to Age-Related Macular Degeneration: Current Drugs and Potential Molecules. Int. J. Mol. Sci. 2019, 20, 1693. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20071693
Nebbioso M, Lambiase A, Cerini A, Limoli PG, La Cava M, Greco A. Therapeutic Approaches with Intravitreal Injections in Geographic Atrophy Secondary to Age-Related Macular Degeneration: Current Drugs and Potential Molecules. International Journal of Molecular Sciences. 2019; 20(7):1693. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20071693
Chicago/Turabian StyleNebbioso, Marcella, Alessandro Lambiase, Alberto Cerini, Paolo Giuseppe Limoli, Maurizio La Cava, and Antonio Greco. 2019. "Therapeutic Approaches with Intravitreal Injections in Geographic Atrophy Secondary to Age-Related Macular Degeneration: Current Drugs and Potential Molecules" International Journal of Molecular Sciences 20, no. 7: 1693. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20071693