FKBP5 rs4713916: A Potential Genetic Predictor of Interindividual Different Response to Inhaled Corticosteroids in Patients with Chronic Obstructive Pulmonary Disease in a Real-Life Setting


 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Results
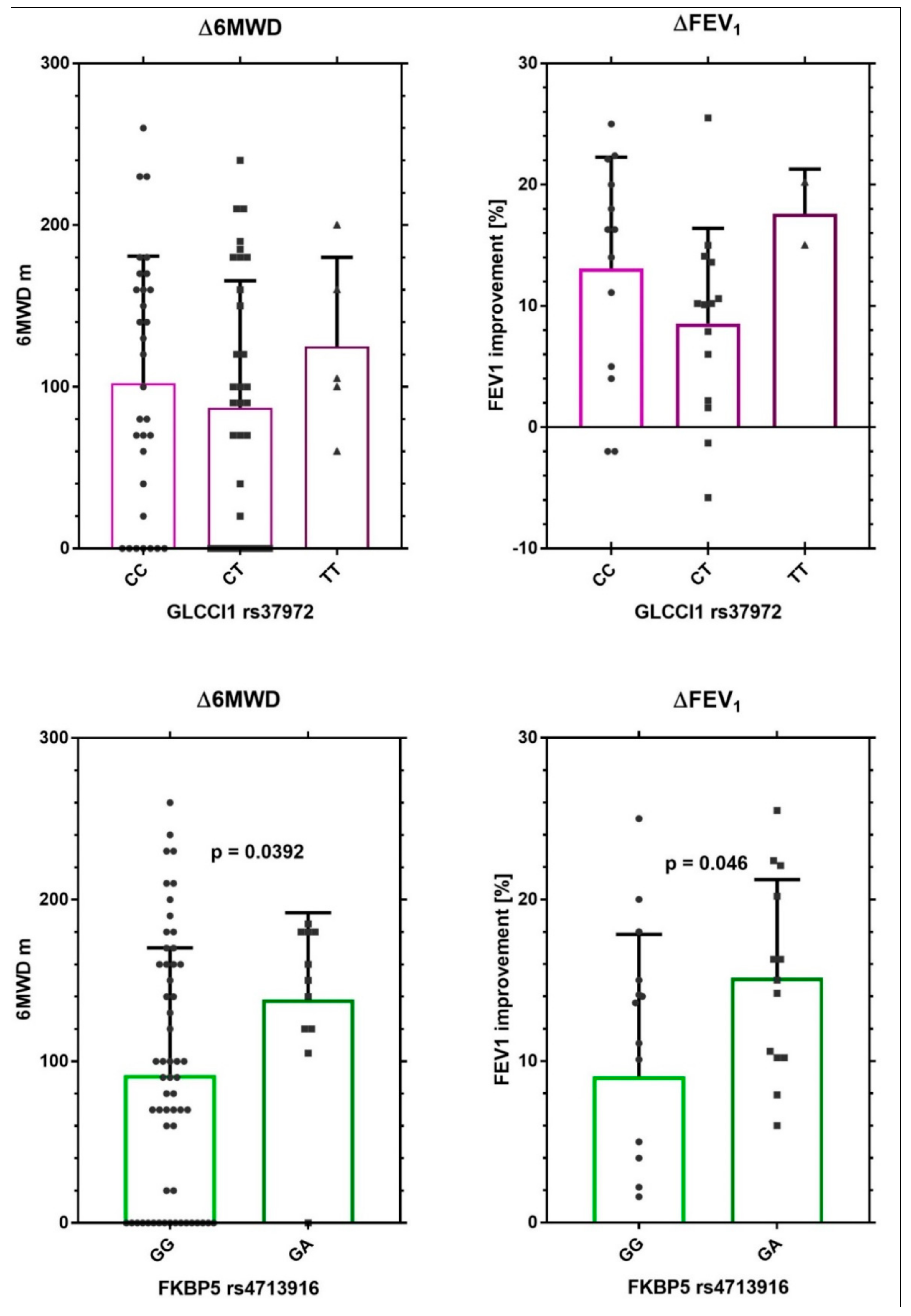
Genotype and Association with Outcomes of Pulmonary Rehabilitation
3. Discussion
Strengths and Limitations
4. Methods
4.1. Subjects
4.2. Patient Characteristics Measured at Baseline And/Or after Completion of PR
4.3. Drug Therapy
4.4. Pulmonary Rehabilitation
4.5. DNA Extraction and Genotyping
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| 6MWD | six minutes walking distance |
| 6MWT | six minutes walking test |
| AECOPD | acute exacerbations of chronic obstructive pulmonary disease |
| BMI | body mass index |
| COPD | chronic obstructive pulmonary disease |
| EBM | evidence-based medicine |
| ECG | electrocardiography |
| FEV1 | forced expiratory volume in 1 s |
| CSs | corticosteroids |
| GR | glucocorticoids receptor |
| ICS | inhaled corticosteroids |
| LTOT | long term oxygen therapy |
| MMSE | mini-mental state examination |
| MoCa | Montreal cognitive assessment |
| MRC | medical research council |
| MRF26 | Maugeri foundation respiratory failure questionnaire |
| PR | pulmonary rehabilitation |
| PRU | pulmonary rehabilitation unit |
| QoL | quality of life |
| SD | standard deviation |
| SF-36 | 36-item short form health survey general |
| SGRQ | Saint George’s respiratory questionnaire |
| SNPs | single nucleotide polymorphisms |
| Δ6MWD | delta6MWD (difference between 6MWD in dismission and admission in meters) |
| ΔFEV1 | deltaFEV1 (difference between values of FEV1 in dismission and admission in percentage) |
References
- Sackett, D.L.; Rosenberg, W.M.; Gray, J.A.; Haynes, R.B.; Richardson, W.S. Evidence based medicine: What it is and what it isn’t. BMJ 1996, 312, 71–72. [Google Scholar] [CrossRef] [PubMed]
- The Centre for Evidence-Based Medicine. Available online: https://www.cebm.net/ (accessed on 27 January 2019).
- Chang, S.; Lee, T.H. Beyond Evidence-Based Medicine. N. Engl. J. Med. 2018, 379, 1983–1985. [Google Scholar] [CrossRef] [PubMed]
- European Lung Foundation. Lung Diseases COPD. Lung Disease & Information. 2012. Available online: http://www.europeanlung.org/en/lung-disease-and-information/lung-diseases/copd (accessed on 9 March 2017).
- Jensen, H.H.; Godtfredsen, N.S.; Lange, P.; Vestbo, J. Potential misclassification of causes of death from COPD. Eur. Respir. J. 2006, 28, 781–785. [Google Scholar] [PubMed] [Green Version]
- Quaderi, S.A.; Hurst, J.R. The unmet global burden of COPD. Glob. Health Epidemiol. Genom. 2018, 3, e4. [Google Scholar] [CrossRef] [PubMed]
- Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. 2017 Report. Available online: http://goldcopd.org/gold-2017-global-strategy-diagnosis-management-prevention-copd/ (accessed on 9 March 2017).
- Calverley, P.M.; Anderson, J.A.; Celli, B.; Ferguson, G.T.; Jenkins, C.; Jones, P.W.; Yates, J.C.; Vestbo, J. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N. Engl. J. Med. 2007, 356, 775–789. [Google Scholar] [CrossRef]
- NIH Medical Rehabilitation Coordinating Committee. National Institutes of Health research plan on rehabilitation. Assist. Technol. 2017. [Google Scholar] [CrossRef]
- Wagner, A.K. TBI Rehabilomics Research: An Exemplar of a Biomarker-Based Approach to Precision Care for Populations with Disability. Curr. Neurol. Neurosci. Rep. 2017, 17, 84. [Google Scholar] [CrossRef] [PubMed]
- Russo, P.; Prinzi, G.; Kisialou, A.; Cardaci, V.; Stirpe, E.; Conti, V.; Fini, M.; Bonassi, S. Action plans and coping strategies in elderly COPD patients influence the result of pulmonary rehabilitation: An observational study. Eur. J. Phys. Rehabil. Med. 2017. [Google Scholar] [CrossRef]
- Singh, D.; Miravitlles, M.; Vogelmeier, C. Chronic Obstructive Pulmonary Disease Individualized Therapy: Tailored Approach to Symptom Management. Adv. Ther. 2017, 34, 281–299. [Google Scholar] [CrossRef]
- Barnes, P.J. Glucocorticosteroids. Handb. Exp. Pharmacol. 2017, 237, 93–115. [Google Scholar]
- Cruz-Topete, D.; Cidlowski, J.A. One hormone, two actions: Anti-and pro-inflammatory effects of glucocorticoids. Neuroimmunomodulation 2015, 22, 20–32. [Google Scholar] [CrossRef] [PubMed]
- Quax, R.A.; Manenschijn, L.; Koper, J.W.; Hazes, J.M.; Lamberts, S.W.; van Rossum, E.F.; Feelders, R.A. Glucocorticoid sensitivity in health and disease. Nat. Rev. Endocrinol. 2013, 9, 670–686. [Google Scholar] [CrossRef] [PubMed]
- Kadmiel, M.; Cidlowski, J.A. Glucocorticoid receptor signaling in health and disease. Trends Pharmacol. Sci. 2013, 34, 518–530. [Google Scholar] [CrossRef] [Green Version]
- Maltese, P.; Palma, L.; Sfara, C.; de Rocco, P.; Latiano, A.; Palmieri, O.; Corritore, G.; Annese, V.; Magnani, M. Glucocorticoid resistance in Crohn’s disease and ulcerative colitis: An association study investigating GR and FKBP5 gene polymorphisms. Pharmacogenom. J. 2012, 12, 432–438. [Google Scholar] [CrossRef] [PubMed]
- Tantisira, K.G.; Lasky-Su, J.; Harada, M.; Harada, M.; Murphy, A.; Litonjua, A.A.; Himes, B.E.; Lange, C.; Lazarus, R.; Sylvia, J.; et al. Genomewide association between GLCCI1 and response to glucocorticoid therapy in asthma. N. Engl. J. Med. 2011, 365, 1173–1183. [Google Scholar] [CrossRef] [PubMed]
- Van den Berge, M.; Hiemstra, P.S.; Postma, D.S. Genetics of glucocorticoids in asthma. N. Engl. J. Med. 2011, 365, 2434–2435. [Google Scholar] [PubMed]
- Mosteller, M.; van den Berge, M.; Hosking, L.; Timens, W.; Hiemstra, P.S.; Crim, C.; Postma, D.S.; Ghosh, S. Genetic evaluation of the effect of GLCCI1 rs37972 on corticosteroid response in chronic obstructive pulmonary disease. COPD Res. Pract. 2017, 3, 2. [Google Scholar] [CrossRef]
- Lei, Y.; Gao, Y.; Chen, J.; Li, M.; Wu, X.; Ning, Q.; Zhao, J.; Xiong, W.; Xu, Y.; Xie, J. GLCCI1 rs37972: A potential genetic predictor of therapeutic response to inhaled corticosteroids in Chinese chronic obstructive pulmonary disease patients. Sci. Rep. 2017, 7, 42552. [Google Scholar] [CrossRef]
- Drozdzik, M.; Rudas, T.; Pawlik, A.; Kurzawski, M.; Czerny, B.; Gornik, W.; Herczynska, M. The effect of 3435C>T MDR1 gene polymorphism on rheumatoid arthritis treatment with disease-modifying antirheumatic drugs. Eur. J. Clin. Pharmacol. 2006, 62, 933–937. [Google Scholar] [CrossRef] [PubMed]
- Potocnik, U.; Ferkolj, I.; Glavac, D.; Dean, M. Polymorphisms in multidrug resistance 1 (MDR1) gene are associated with refractory Crohn disease and ulcerative colitis. Genes Immun. 2004, 5, 530–539. [Google Scholar] [CrossRef] [Green Version]
- WHO. Obesity and Overweight. Available online: http://www.who.int/mediacentre/factsheets/fs311/en/ (accessed on 24 October 2016).
- rs37972. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/snp/?term=rs37972 (accessed on 5 March 2019).
- rs6189. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/snp/?term=rs6189 (accessed on 5 March 2019).
- rs6190. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/snp/?term=rs6190 (accessed on 5 March 2019).
- rs41423247. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/snp/?term=rs41423247 (accessed on 5 March 2019).
- rs2032582. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/snp/?term=rs2032582 (accessed on 5 March 2019).
- rs4713916. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/snp/?term=rs4713916 (accessed on 5 March 2019).
- Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/SNP/snp_ref.cgi?searchType=adhoc_search&type=rs&rs=rs4713916 (accessed on 29 March 2017).
- Horsfall, L.J.; Rait, G.; Walters, K.; Swallow, D.M.; Pereira, S.P.; Nazareth, I.; Petersen, I. Serum bilirubin and risk of respiratory disease and death. JAMA 2011, 305, 691–697. [Google Scholar] [CrossRef]
- Curjuric, I.; Imboden, M.; Adam, M.; Bettschart, R.W.; Gerbase, M.W.; Künzli, N.; Rochat, T.; Rohrer, L.; Rothe, T.B.; Schwartz, J.; et al. Serum bilirubin is associated with lung function in a Swiss general population sample. Eur. Respir. J. 2014, 43, 1278–1288. [Google Scholar] [CrossRef] [PubMed]
- Apperley, S.; Park, H.Y.; Holmes, D.T.; Man, S.F.P.; Tashkin, D.; Wise, RA.; Connett, J.E.; Sin, D.D. Serum Bilirubin and Disease Progression in Mild COPD. Chest 2015, 148, 169–175. [Google Scholar] [CrossRef]
- Reinhold, D.; Morrow, J.D.; Jacobson, S.; Hu, J.; Ringel, B.; Seibold, M.A.; Hersh, C.P.; Kechris, K.J.; Bowler, R.P. Meta-analysis of peripheral blood gene expression modules for COPD phenotypes. PLoS ONE 2017, 12, e0185682. [Google Scholar] [CrossRef] [PubMed]
- Hobbs, B.D.; de Jong, K.; Lamontagne, M.; Bossé, Y.; Shrine, N.; Artigas, M.S.; Wain, L.V.; Hall, I.P.; Jackson, V.E.; Wyss, A.B.; et al. Genetic loci associated with chronic obstructive pulmonary disease overlap with loci for lung function and pulmonary fibrosis. Nat. Genet. 2017, 49, 426–432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wain, L.V.; Shrine, N.; Artigas, M.S.; Erzurumluoglu, A.M.; Noyvert, B.; Bossini-Castillo, L.; Obeidat, M.; Henry, A.P.; Portelli, M.A.; Hall, R.J.; et al. Genome-wide association analyses for lung function and chronic obstructive pulmonary disease identify new loci and potential druggable targets. Nat. Genet. 2017, 49, 416–425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Postma, D.S.; Weiss, S.T.; van den Berge, M.; Kerstjens, H.A.; Koppelman, G.H. Revisiting the Dutch hypothesis. J. Allergy Clin. Immunol. 2015, 136, 521–529. [Google Scholar] [CrossRef]
- Li, Y.; Cho, M.H.; Zhou, X. What do polymorphisms tell us about the mechanisms of COPD? Clin. Sci. 2017, 131, 2847–2863. [Google Scholar] [CrossRef] [PubMed]
- Mizuno, S.; Ishizaki, T.; Kadowaki, M.; Akai, M.; Shiozaki, K.; Iguchi, M.; Oikawa, T.; Nakagawa, K.; Osanai, K.; Toga, H.; et al. p53 Signaling Pathway Polymorphisms Associated with Emphysematous Changes in Patients With COPD. Chest 2017, 152, 58–69. [Google Scholar] [CrossRef]
- Hansen, J.G.; Gao, W.; Dupuis, J.; O’Connor, G.T.; Tang, W.; Kowgier, M.; Sood, A.; Gharib, S.A.; Palmer, L.J.; Fornage, M.; et al. Association of 25-Hydroxyvitamin D status and genetic variation in the vitamin D metabolic pathway with FEV1 in the Framingham Heart Study. Respir. Res. 2015, 16, 81. [Google Scholar] [CrossRef] [PubMed]
- Hall, R.; Hall, I.P.; Sayers, I. Genetic risk factors for the development of pulmonary disease identified by genome-wide association. Respirology 2018. [Google Scholar] [CrossRef] [PubMed]
- Russo, P.; Lococo, F.; Kisialiou, A.; Cardaci, V.; Fini, M.; Russo, P. Pharmacological management of chronic obstructive lung disease (COPD). Focus on mutations. Curr. Med. Chem. 2018, in press. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.; Sin, D.D.; Voelker, H.; Connett, J.E.; Niewoehner, D.E.; Kunisaki, K.M. COPD Clinical Research Network.Serum bilirubin and the risk of chronic obstructive pulmonary disease exacerbations. Respir. Res. 2017, 18, 179. [Google Scholar] [CrossRef] [PubMed]
- Annemans, L.; Aristides, M.; Kubin, M. Real-Life Data: A Growing Need. ISPOR. Available online: www.ispor.org/news/articles/oct07/rld.asp (accessed on 29 March 2017).
- Du Bois, R.M.; Weycker, D.; Albera, C.; Bradford, W.Z.; Costabel, U.; Kartashov, A.; Lancaster, L.; Noble, P.W.; Sahn, S.A.; Szwarcberg, J.; et al. Six-minute-walk test in idiopathic pulmonary fibrosis: Test validation and minimal clinically important difference. Am. J. Respir. Crit. Care Med. 2011, 183, 1231–1237. [Google Scholar] [CrossRef] [PubMed]
- Puente-Maestu, L.; Palange, P.; Casaburi, R.; Laveneziana, P.; Maltais, F.; Neder, J.A.; O’Donnell, D.E.; Onorati, P.; Porszasz, J.; Rabinovich, R.; et al. Use of exercise testing in the evaluation of interventional efficacy: An official ERS statement. Eur. Respir. J. 2016, 47, 429–460. [Google Scholar] [CrossRef]
- Polkey, M.I.; Spruit, M.A.; Edwards, L.D.; Watkins, M.L.; Pinto-Plata, V.; Vestbo, J.; Calverley, P.M.; Tal-Singer, R.; Agustí, A.; Bakke, P.S.; et al. Six-minute-walk test in chronic obstructive pulmonary disease: Minimal clinically important difference for death or hospitalization. Am. J. Respir. Crit. Care Med. 2013, 187, 382–386. [Google Scholar] [CrossRef] [PubMed]
- Pepin, V.; Saey, D.; Whittom, F.; LeBlanc, P.; Maltais, F. Walking versus cycling: Sensitivity to bronchodilation in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2005, 172, 1517–1522. [Google Scholar] [CrossRef]
- Celli, B.; Tetzlaff, K.; Criner, G.; Polkey, M.I.; Sciurba, F.; Casaburi, R.; Tal-Singer, R.; Kawata, A.; Merrill, D.; Rennard, S. The 6-Minute-Walk Distance Test as a Chronic Obstructive Pulmonary Disease Stratification Tool. Insights from the COPD Biomarker Qualification Consortium. Am. J. Respir. Crit. Care Med. 2016, 194, 1483–1493. [Google Scholar] [CrossRef] [Green Version]
- Sharafkhaneh, A.; Southard, J.G.; Goldman, M.; Uryniak, T.; Martin, U.J. Effect of budesonide/formoterol pMDI on COPD exacerbations: A double-blind, randomized study. Respir. Med. 2012, 106, 257–268. [Google Scholar] [CrossRef] [Green Version]
- Viechtbauer, W.; Smits, L.; Kotz, D.; Budé, L.; Spigt, M.; Serroyen, J.; Crutzen, R. A simple formula for the calculation of sample size in pilot studies. J. Clin. Epidemiol. 2015, 68, 1375–1379. [Google Scholar] [CrossRef]
- Italian Minister of Health DM 18/10/2012. Remunerazione Prestazioni di Assistenza Ospedaliera per Acuti, Assistenza Ospedaliera di Riabilitazione e di Lungodegenza post Acuzie e di Assistenza Specialistica Ambulatoriale. (13A00528). Available online: http://www.gazzettaufficiale.it/eli/id/2013/01/28/13A00528/sg (accessed on 3 January 2018).
- Lazio Region. DCA Lazio 316/2012. Piano Indirizzo Sulla Riabilitazione. Available online: http://www.regione.lazio.it/binary/rl_sanita/tbl_normativa/SAN_DCA_U00159_13_05_2016.pdf (accessed on 2 January 2018).
- Spruit, M.A.; Singh, S.J.; Garvey, C.; ZuWallack, R.; Nici, L.; Rochester, C.; Hill, K.; Holland, A.E.; Lareau, S.C.; Man, W.D.; et al. An official American Thoracic Society/European Respiratory Society statement: Key concepts and advances in pulmonary rehabilitation. Am. J. Respir. Crit. Care Med. 2013, 188, e13–e64. [Google Scholar] [CrossRef] [PubMed]
- Cesario, A.; Auffray, C.; Agusti, A.; Apolone, G.; Balling, R.; Barbanti, P.; Bellia, A.; Boccia, S.; Bousquet, J.; Cardaci, V.; et al. A systems medicine clinical platform for understanding and managing non- communicable diseases. Curr. Pharm. Des. 2014, 20, 5945–5956. [Google Scholar] [CrossRef] [PubMed]
- Jones, P.W.; Quirk, F.H.; Baveystock, C.M.; Littlejohns, P. A self complete measure of health status for chronic airflow limitation. The St. George’s Respiratory Questionnaire. Am. Rev. Respir. Dis. 1992, 145, 1321e7. [Google Scholar] [CrossRef]
- Available online: https://www.thoracic.org/members/assemblies/assemblies/srn/questionaires/sgrq.php (accessed on 29 March 2017).
- Available online: http://pulmonaryrehab.com.au/patient-assessment/assessing-quality-of-life/ (accessed on 29 March 2017).
- Holland, A.E.; Spruit, M.A.; Troosters, T.; Puhan, M.A.; Pepin, V.; Saey, D.; McCormack, MC.; Carlin, B.W.; Sciurba, F.C.; Pitta, F.; et al. An official European Respiratory Society/American Thoracic Society technical standard: Field walking tests in chronic respiratory disease. Eur. Respir. J. 2014, 44, 1428–1446. [Google Scholar] [CrossRef] [PubMed]
- Spruit, M.A. Pulmonary rehabilitation. Eur. Respir. Rev. 2014, 23, 55–63. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Patients n = 71 |
|---|---|
| Males | 30 (42.2%) |
| Females | 41 (57.8%) |
| Years of Education | 8.9 ± 4.08 |
| Marital Status | |
| Single | 3 (4.2%) |
| Married | 36 (50.7%) |
| Divorced/widow | 32 (45.1%) |
| No smokers | 6 (8.5%) |
| Current smokers | 11 (15.5%) |
| Ex-smokers | 46 (64.7%) |
| Not Responders | 8 (11.3%) |
| Occupational Status | |
| Retired | 63 (88.7%) |
| Housewife | 8 (11.3%) |
| BMI | 27.57 ± 4.9 |
| Therapy With O2 | 23 (32.4%) |
| Corticosteroids therapy | 71 (100%) |
| MRC dyspnea grade | 4.0 ± 0 |
| Borg grade | 7.87 ± 0.92 |
| SGRQ-Total points | 49.33± 16.02 |
| 6MWD (meters) | 96.76 ± 85.25 |
| MRF26 | 72.14 ± 15.65 |
| Barthel | 68.32 ± 24.37 |
| FEV1 | 48.40 ± 24.2 |
| MMSE | 26.78 ± 2.83 |
| MoCa | 25.57 ± 3.73 |
| SF-36 General Health | 73.40 ± 11.54 |
| SF-36 Mental Health | 62.56 ± 8.54 |
| CIRS-severity | 1.58 ± 0.23 |
| CIRS-comorbidity | 2.44 ± 1.36 |
| Before PR (x ± SD) | After PR (x ± SD) | Δ | p Value * | |
|---|---|---|---|---|
| 6MWD (meters) | 96.76 ± 85.25 | 191.1 ± 132.7 | 94.37 ± 79.97 | <0.0001 |
| FEV1 (%) | 48.11 ± 23.35 | 62.46 ± 11.74 | 11.32 ± 8.42 | 0.0073 |
| MRC | 4.0 ± 0.0 | 3.34 ± 0.61 | −0.66 ±0.61 | <0.0001 |
| Borg | 7.87 ± 0.92 | 5.20 ± 2.47 | 2.676 ± 1.911 | <0.0001 |
| SGRQ | 49.33 ± 16.02 | 44.29 ± 16.08 | −2.59 ± 16.69 | NS |
| Barthel | 68.32 ± 24.37 | 86.1 ± 16.72 | 17.77 ± 15.01 | <0.0001 |
| MRF26 | 72.14 ± 15.65 | 48.69 ± 19.07 | −23.3 ± 14.17 | <0.0001 |
| GLCCI1 rs37972 | NR3C1 rs6189 | NR3C1 rs6190 | NR3C1 Bcl2 rs41423247 | MDR-1 rs2032582 | FKBP5 rs4713916 |
|---|---|---|---|---|---|
| CC 31 (43.7%) | GG 66 (93%) | GG 66 (93%) | GG 35 (49.3%) | GG 25 (35.2%) | GG 57 (80.3%) |
| CT 34 (47.9%) | GA 3 (4.2%) | GA 3 (4.2%) | GC 28 (39.4%) | GA 3 (4.2%) | GA 13 (18.3%) |
| TT 5 (7%) | - | - | CC 7 (9.9%) | GT 22 (31%) | - |
| - | - | - | - | TT 20 (28.2%) | - |
| NA 1 (1.4%) | NA 2 (2.8%) | NA 2 (2.8%) | NA 1 (1.4%) | NA 1 (1.4%) | NA 1 (1.4%) |
| SNP | Responders Patients Number (% Over Total) | Non-Responders Patients Number (% Over Total) | % Responders Genotype | p * |
|---|---|---|---|---|
| rs37972 | ||||
| CC | 22 (32.35%) | 8 (11.77%) | 73.3% | 0.08 |
| CT | 21(30.88%) | 12 (17.65%) | 62.6% | |
| TT | 5 (7.35%) | 0 | 100% | |
| rs4713916 | ||||
| GG | 37 (55.22%) | 19 (28.36%) | 60% | 0.039 |
| GA | 10 (14.92%) | 1 (1.5%) | 90.91% | |
| rs6189 | ||||
| GG | 45 (67.16%) | 19 (28.35%) | 70.31% | NS |
| GA | 3 (4.48%) | 0 | 100% | |
| rs6190 | ||||
| GG | 44 (65.67%) | 20 (29.85%) | 68.75% | NS |
| GA | 3 (4.48%) | 0 | 100% | |
| rs41423247 | ||||
| CC | 4 (5.88%) | 3 (4.41%) | 57.14% | NS |
| GC | 19 (27.94%) | 7 (10.29%) | 73.07% | |
| GG | 25 (36.76%) | 10 (14.71%) | 71.42% | |
| rs2032582 | ||||
| GG | 14 (20.59%) | 10 (14.71%) | 58.33% | NS |
| GA | 3 (4.41%) | 0 | 100% | |
| GT | 15 (22.06%) | 6 (8.82%) | 71.43% | |
| TT | 16 (23.53%) | 4 (5.88%) | 80% |
| Characteristics | All GA | All GG | p Value |
|---|---|---|---|
| Δ Borg | −3.50 ± 1.35 | −2.35 ± 1.99 | 0.0862 |
| Δ SGRQ-Total points | 14.0 ± 24.17 | −4.14 ± 10.68 | 0.037 |
| Δ Basophiles * | 0.15 ± 0.28 | −0.11 ± 0.26 | 0.085 |
| Bilirubin ** | 0.94 ± 0.55 | 0.58 ± 0.29 | 0.0453 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Russo, P.; Tomino, C.; Santoro, A.; Prinzi, G.; Proietti, S.; Kisialiou, A.; Cardaci, V.; Fini, M.; Magnani, M.; Collacchi, F.; et al. FKBP5 rs4713916: A Potential Genetic Predictor of Interindividual Different Response to Inhaled Corticosteroids in Patients with Chronic Obstructive Pulmonary Disease in a Real-Life Setting. Int. J. Mol. Sci. 2019, 20, 2024. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20082024
Russo P, Tomino C, Santoro A, Prinzi G, Proietti S, Kisialiou A, Cardaci V, Fini M, Magnani M, Collacchi F, et al. FKBP5 rs4713916: A Potential Genetic Predictor of Interindividual Different Response to Inhaled Corticosteroids in Patients with Chronic Obstructive Pulmonary Disease in a Real-Life Setting. International Journal of Molecular Sciences. 2019; 20(8):2024. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20082024
Chicago/Turabian StyleRusso, Patrizia, Carlo Tomino, Alessia Santoro, Giulia Prinzi, Stefania Proietti, Aliaksei Kisialiou, Vittorio Cardaci, Massimo Fini, Mauro Magnani, Francesco Collacchi, and et al. 2019. "FKBP5 rs4713916: A Potential Genetic Predictor of Interindividual Different Response to Inhaled Corticosteroids in Patients with Chronic Obstructive Pulmonary Disease in a Real-Life Setting" International Journal of Molecular Sciences 20, no. 8: 2024. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20082024