Molecular Aspects of Drug-Induced Gingival Overgrowth: An In Vitro Study on Amlodipine and Gingival Fibroblasts

 ,
,  ,
,
Abstract
:1. Introduction
1.1. Genetic Factors
1.2. Objective
2. Results
3. Discussion
4. Materials and Methods
4.1. Primary Human Fibroblast Cells Culture
4.2. Cell Viability Test
4.3. Cell Treatment
4.4. RNA Isolation, Reverse Transcription and Quantitative Real-Time RT-PCR
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Amit, B.; Shalu, B.V. Gingival enlargement induced by anticonvulsants, calcium channel blockers and immunosuppressants: A review. IRJP 2012, 3, 116–119. [Google Scholar]
- Ellis, J.S.; Seymour, R.A.; Steele, J.G.; Roberston, P.; Butler, T.J.; Thomason, J.M. Prevalence of gingival overgrowth induced by calcium channel blockers: A community based study. J. Periodontol. 1999, 70, 63–67. [Google Scholar]
- Bharati, T.; Mukesh Tehmina Veenita Jain, V.V.; Jajoo, U.N. Amlodipine induced gum hypertrophy—A rare case report. J. Mgims 2012, 17, 63–64. [Google Scholar]
- Newman, M.G.; Takei, H.H.; Klokkevold, P.R.; Carranza, F.A. Carranza’s Clinical Periodontology, 10th ed.; Saunders: St Louis, MO, USA, 2006; pp. 373–377. [Google Scholar]
- Drug associated gingival enlargement. J. Periodontol. 2004, 75, 1424–1431. [CrossRef]
- Jorgensen, M.G. Prevalence of amlodipine-related gingival hyperplasia. J. Periodontol. 1997, 68, 676–678. [Google Scholar]
- Jose, J.; Santhosh, Y.L.; Naveen, M.R.; Kumar, V. Case report of amlodipine induced gingival hyperplasia—Late onset at a low use. Asian J. Pharm. Clin. Res. 2011, 4, 65–66. [Google Scholar]
- Seymour, R.A.; Ellis, J.S.; Thomason, J.M.; Monkman, S.; Idle, J.R. Amlodipine induced gingival overgrowth. J. Clin. Periodontal 1994, 21, 281–283. [Google Scholar]
- Lafzi, A.; Farahani, R.M.; Shoja, M.A. Amlodipine induced gingival hyperplasia. Med. Oral Patol. Oral Cir. Bucal. 2006, 11, 480–482. [Google Scholar]
- Meraw, S.J.; Sheridan, P.J. Medically induced gingival hyperplasia. Mayo Clin. Proc. 1996, 73, 1196–1199. [Google Scholar]
- Ellis, J.S.; Seymour, R.A.; Monkman, S.C.; Idle, J.R. Gingival sequestration of nifedipine induced gingival overgrowth. Lancet 1992, 39, 1382–1383. [Google Scholar]
- Grover, V.; Kapoor, A.; Marya, C.M. Amlodipine induced gingival hyperplasia. J. Oral Health Comm. Dent. 2007, 1, 19–22. [Google Scholar]
- Daley, T.D.; Wysocki, G.P.; Day, C. Clinical and pharmacologic correlations in cyclosporine-induced gingival hyperplasia. Oral Surg. Oral Med. Oral Pathol. 1986, 62, 417–421. [Google Scholar]
- Pasupuleti, M.K.; Musalaiah, S.V.; Nagasree, M.; Kumar, P.A. Combination of inflammatory and amlodipine induced gingival overgrowth in a patient with cardiovascular disease. Avicenna J. Med. 2013, 3, 68–72. [Google Scholar] [Green Version]
- Meisel, P.; Giebel, J.; Kunert-Keil, C.; Dazert, P.; Kroemer, H.K.; Kocher, T. MDR1 gene polymorphisms and risk of gingival hyperplasia induced by calcium antagonists. Clin. Pharm. Ther. 2006, 79, 62–71. [Google Scholar]
- Takeuchi, R.; Matsumoto, H.; Akimoto, Y.; Fujii, A. The inhibitory action of amlodipine for TNF-α-induced apoptosis in cultured human gingival fibroblasts. Oral Ther. Pharmacol. 2012, 31, 45–52. [Google Scholar]
- Hassell, T.M. Evidence for production of an inactive collagenase by fibroblasts from phenytoin-enlarged human gingiva. J. Oral Pathol. 1982, 11, 310–317. [Google Scholar]
- Bolzani, G.; Della Coletta, R.; Martelli Junior, H.; Martelli Junior, H.; Graner, E. Cyclosporin A inhibits production and activity of matrix metalloproteinases by gingival fibroblasts. J. Periodontal Res. 2000, 35, 51–58. [Google Scholar]
- Kataoka, M.; Shimizu, Y.; Kunikiyo, K.; Asahara, Y.; Yamashita, K.; Ninomiya, M.; Morisaki, I.; Ohsaki, Y.; Kido, J.-I.; Nagata, T. Cyclosporin A decreases the degradation of type I collagen in rat gingival overgrowth. J. Cell Physiol. 2000, 182, 351–358. [Google Scholar]
- Sucu, M.; Yuce, M.; Davatoglu, V. Amlodipine induced massive gingival hypertrophy. Can. Fam. Phys. 2011, 57, 436–437. [Google Scholar]
- Prisant, L.M.; Herman, W. Calcium channel blocker induced gingival overgrowth. J. Clin. Hypertens. 2002, 4, 310–311. [Google Scholar]
- Pradhan, S.; Mishra, P.; Joshi, S. Drug induced gingival enlargement—A review. PGNM 2009, 8. [Google Scholar]
- Amgelpoulous, A.P.; Goaz, P.W. Incidence of diphenylhydantoin gingival hyperplasia. Oral Surg. Oral Med. Oral Pathol. 1972, 34, 898–906. [Google Scholar]
- Hegde, R.; Kale, R.; Jain, A.S. Cyclosporine and amlodipine induced severe gingival overgrowth–etiopathogenesis and management of a case with electrocautery and carbon-dioxide (CO2) laser. J. Oral Health. Comm. Dent. 2012, 6, 34–42. [Google Scholar]
- Taib, H.; Ali, T.B.T.; Kamin, S. Amlodipine induced gingival overgrowth: A case report. Arch. Orofac. Sci. 2007, 2, 61–64. [Google Scholar]
- Srivastava, A.K.; Kundu, D.; Bandyopadhyay, P.; Pal, A.K. Management of amlodipine induced gingival enlargement: A series of three cases. J. Indian Soc. Perodontol. 2010, 14, 279. [Google Scholar]
- Khan, S.; Mittal, A.; Kanteshwari, I.K. Amlodipine induced gingival overgrowth: A case report. NJDSR 2012, 1, 65–69. [Google Scholar]
- Routray, S.N.; Mishra, T.K.; Pattnaik, U.K.; Satapathy, C.; Mishra, C.K.; Behera, M. Amlodipine induced gingival hyperplasia. J. Assoc. Phys. India 2003, 51, 818–819. [Google Scholar]
- Sharma, S.; Sharma, A. Amlodipine induced gingival enlargement—A clinical report. Compend. Contin. Educ. Dent. 2012, 33, 78–82. [Google Scholar]
- Triveni, M.G.; Rudrakshi, C.; Mehta, D.S. Amlodipine induced gingival overgrowth. J. Indian Soc. Periodontol. 2009, 13, 160–163. [Google Scholar]
- Marshall, R.I.; Bartold, P.M. A clinical review of drug induced gingival overgrowth. Oral Surg. Oral Med. Oral Pathol. 1993, 76, 543–548. [Google Scholar]
- Lombardi, T.; Fiore, D.G.; Belser, U.; Di, F.R. Felodipine induced gingival hyperplasia: A clinical and histologic study. J. Oral Pathol. Med. 1991, 20, 89–92. [Google Scholar]


{kind=link}
| Gene | Fold Change | SD (+/−) | Gene Function |
|---|---|---|---|
| CTNND2 | 2.29 | 0.03 | Cell Adhesion Molecule |
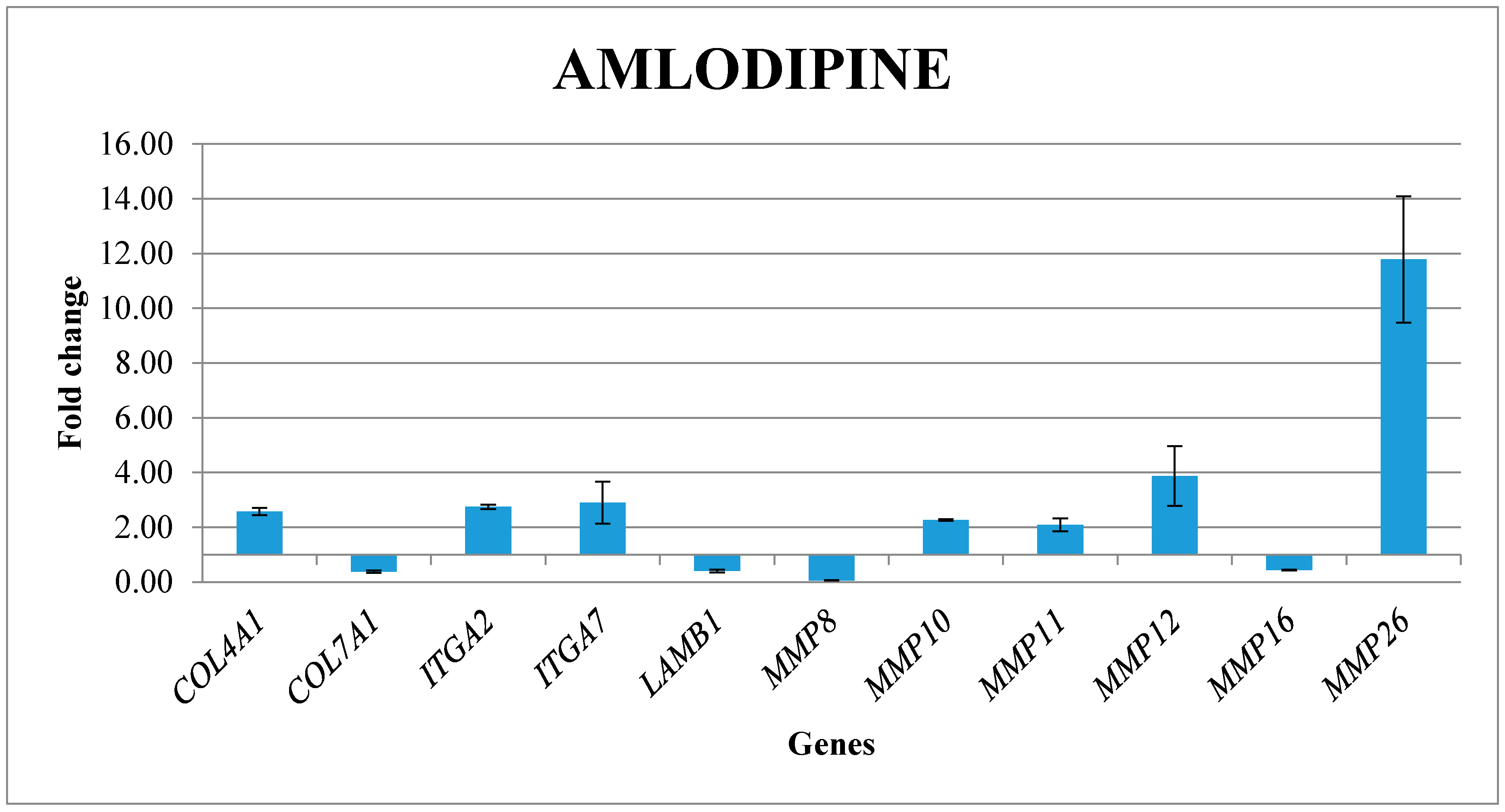
| COL4A1 | 2.57 | 0.13 | Collagens & Extracellular Matrix Structural constituent |
| COL7A1 | 0.38 | 0.04 | Collagens & Extracellular Matrix Structural constituent |
| ITGA2 | 2.75 | 0.08 | Transmembrane Receptor |
| ITGA7 | 2.90 | 0.77 | Transmembrane Receptor |
| LAMB1 | 0.41 | 0.05 | Basement Membrane Constituent |
| MMP8 | 0.06 | 0.01 | Extracellular Matrix Protease |
| MMP10 | 2.27 | 0.03 | Extracellular Matrix Protease |
| MMP11 | 2.09 | 0.24 | Extracellular Matrix Protease |
| MMP12 | 3.88 | 1.09 | Extracellular Matrix Protease |
| MMP16 | 0.44 | 0.02 | Extracellular Matrix Protease |
| MMP26 | 11.78 | 2.31 | Extracellular Matrix Protease |
| Gene Name | Forward Sequence 5′ > 3′ | Reverse Sequence 5′ > 3′ |
|---|---|---|
| CTNND2 | AGAGAATTTGGATGGAGAGAC | TTGTTGTCTCCAAAACAGAG |
| COL4A1 | AAAGGGAGATCAAGGGATAG | TCACCTTTTTCTCCAGGTAG |
| COL7A1 | ATGACCTTGGCATTATCTTG | TGAATATGTCACCTCTCAAGG |
| ITGA2 | GGTGGGGTTAATTCAGTATG | ATATTGGGATGTCTGGGATG |
| ITGA7 | CATGAACAATTTGGGTTCTG | GCCCTTCCAATTATAGGTTC |
| LAMB1 | GTGTGTATAGATACTTCGCC | AAAGCACGAAATATCACCTC |
| MMP8 | AAGTTGATGCAGTTTTCCAG | CTGAACTTCCCTTCAACATTC |
| MMP10 | AGCGGACAAATACTGGAG | GTGATGATCCACTGAAGAAG |
| MMP11 | GATAGACACCAATGAGATTGC | TTTGAAGAAAAAGAGCTCGC |
| MMP12 | AGGTATGATGAAAGGAGACAG | AGGTATGATGAAAGGAGAACAG |
| MMP16 | ACCCTCATGACTTGATAACC | TCTGTCTCCCTTGAAGAAATAG |
| MMP26 | AAGGATCCAGCATTTGTATG | CTTTGATCCTCCAATAAACTCC |
| RPL13 | AAAGCGGATGGTGGTTCCT | GCCCCAGATAGGCAAACTTTC |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lauritano, D.; Lucchese, A.; Di Stasio, D.; Della Vella, F.; Cura, F.; Palmieri, A.; Carinci, F. Molecular Aspects of Drug-Induced Gingival Overgrowth: An In Vitro Study on Amlodipine and Gingival Fibroblasts. Int. J. Mol. Sci. 2019, 20, 2047. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20082047
Lauritano D, Lucchese A, Di Stasio D, Della Vella F, Cura F, Palmieri A, Carinci F. Molecular Aspects of Drug-Induced Gingival Overgrowth: An In Vitro Study on Amlodipine and Gingival Fibroblasts. International Journal of Molecular Sciences. 2019; 20(8):2047. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20082047
Chicago/Turabian StyleLauritano, Dorina, Alberta Lucchese, Dario Di Stasio, Fedora Della Vella, Francesca Cura, Annalisa Palmieri, and Francesco Carinci. 2019. "Molecular Aspects of Drug-Induced Gingival Overgrowth: An In Vitro Study on Amlodipine and Gingival Fibroblasts" International Journal of Molecular Sciences 20, no. 8: 2047. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20082047