Fibroblast Growth Factor 23 is Associated with a Frequent Exacerbator Phenotype in COPD: A Cross-Sectional Pilot Study

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Cohort Characteristics
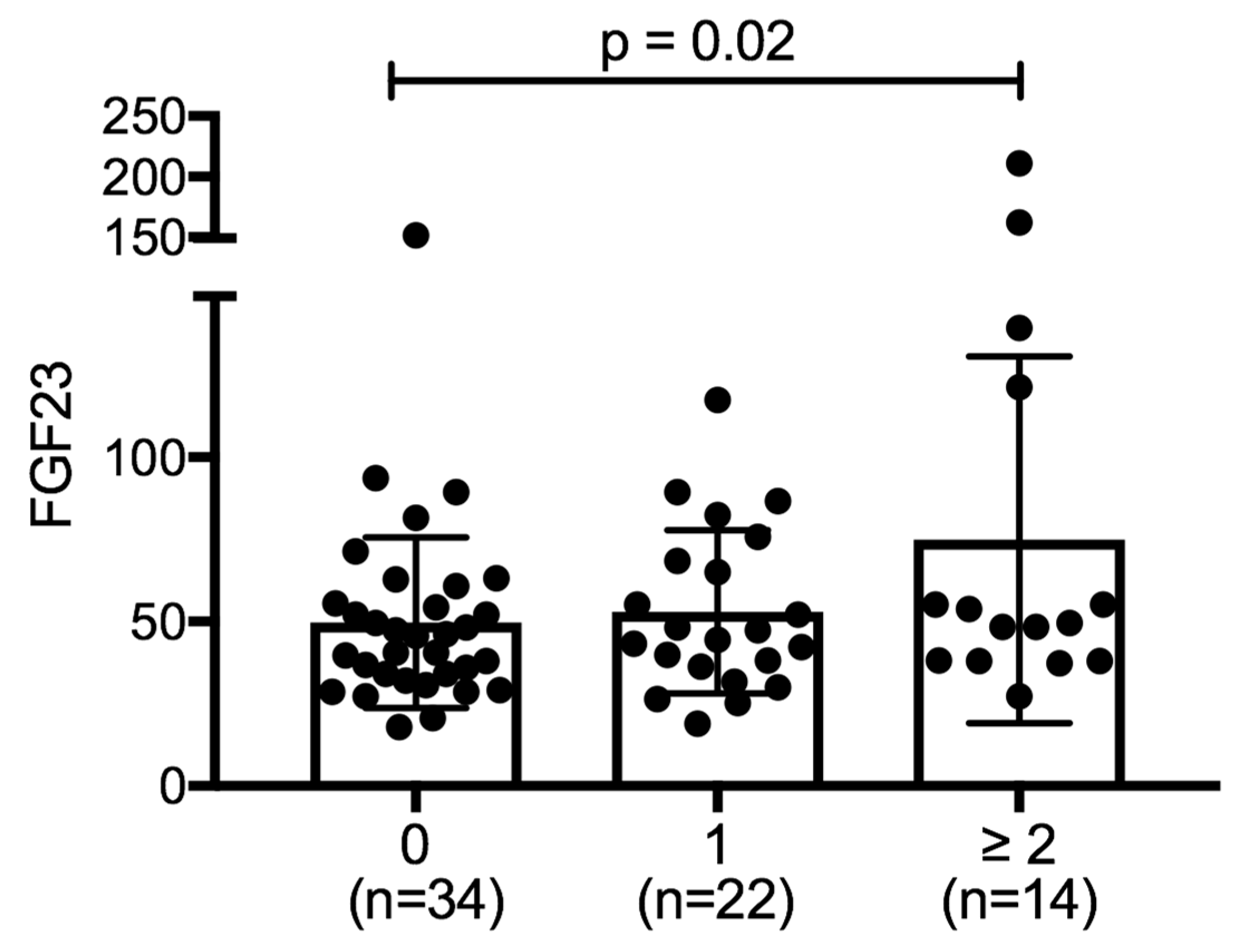
2.2. FGF23 and Past COPD Exacerbations
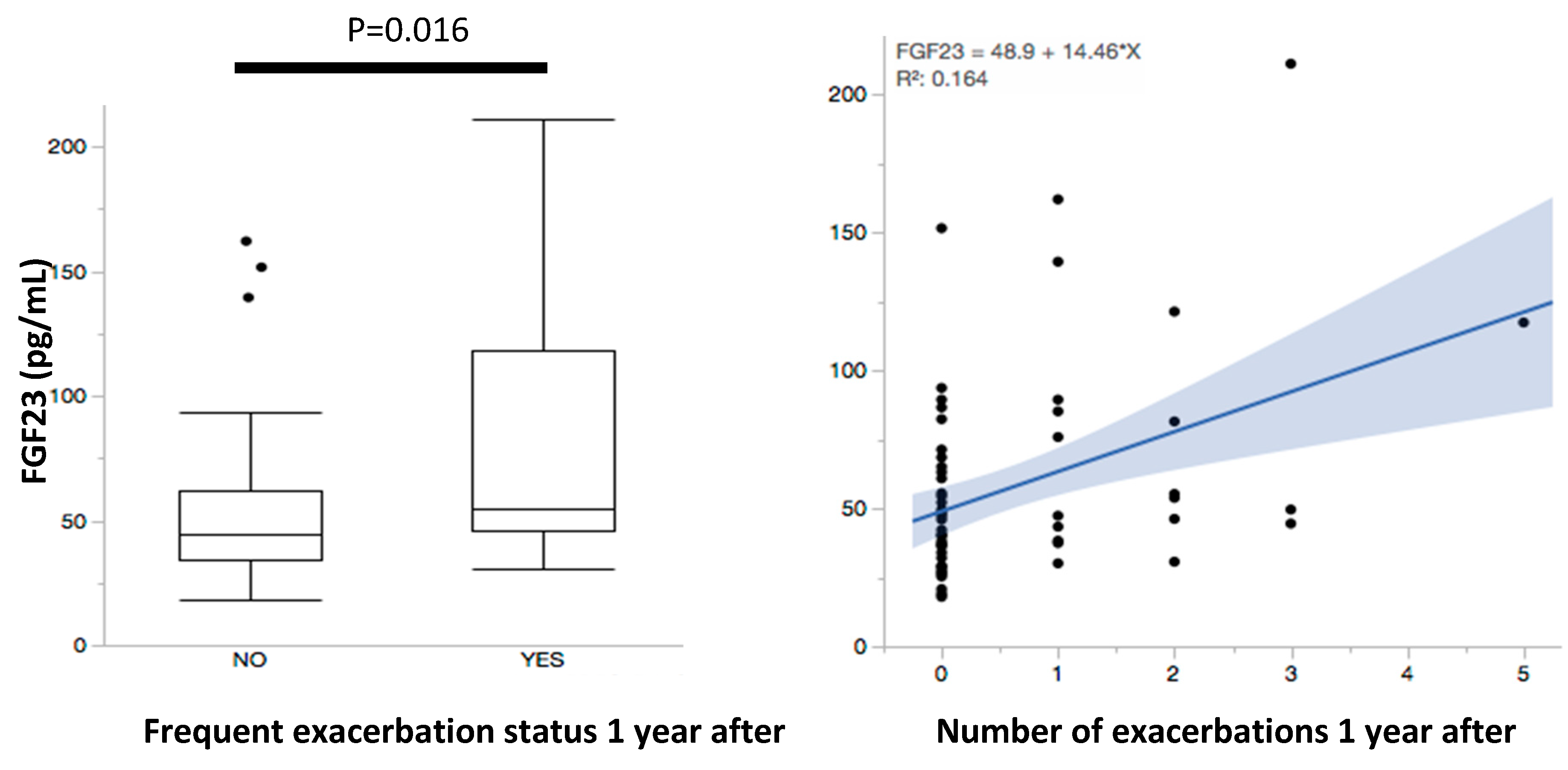
2.3. FGF23 and Future COPD Exacerbations
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Ascertainment of COPD Exacerbations
4.3. Blood Sampling and FGF23 Measurement
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Minino, A.M.; Xu, J.; Kochanek, K.D. Deaths: Preliminary data for 2008. Natl. Vital. Stat. Rep. 2010, 59, 1–52. [Google Scholar]
- Yu, A.P.; Yang, H.; Wu, E.Q.; Setyawan, J.; Mocarski, M.; Blum, S. Incremental third-party costs associated with COPD exacerbations: A retrospective claims analysis. J. Med. Econ. 2011, 14, 315–323. [Google Scholar] [CrossRef]
- Bhowmik, A.; Seemungal, T.A.; Sapsford, R.J.; Wedzicha, J.A. Relation of sputum inflammatory markers to symptoms and lung function changes in COPD exacerbations. Thorax 2000, 55, 114–120. [Google Scholar] [CrossRef] [Green Version]
- Dransfield, M.T.; Kunisaki, K.M.; Strand, M.J.; Anzueto, A.; Bhatt, S.P.; Bowler, R.P.; Criner, G.J.; Curtis, J.L.; Hanania, N.A.; Nath, H.; et al. Acute Exacerbations and Lung Function Loss in Smokers with and without Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2017, 195, 324–330. [Google Scholar] [Green Version]
- Vestbo, J.; Edwards, L.D.; Scanlon, P.D.; Yates, J.C.; Agusti, A.; Bakke, P.; Calverley, P.M.; Celli, B.; Coxson, H.O.; Crim, C.; et al. Changes in forced expiratory volume in 1 second over time in COPD. N. Engl. J. Med. 2011, 365, 1184–1192. [Google Scholar] [CrossRef]
- Seemungal, T.A.; Donaldson, G.C.; Paul, E.A.; Bestall, J.C.; Jeffries, D.J.; Wedzicha, J.A. Effect of exacerbation on quality of life in patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 1998, 157, 1418–1422. [Google Scholar] [CrossRef]
- Le Rouzic, O.; Roche, N.; Cortot, A.B.; Tillie-Leblond, I.; Masure, F.; Perez, T.; Boucot, I.; Hamouti, L.; Ostinelli, J.; Pribil, C.; et al. Defining the “Frequent Exacerbator” Phenotype in COPD: A Hypothesis-Free Approach. Chest 2017, 153, 1106–1115. [Google Scholar] [CrossRef]
- Donaldson, G.C.; Seemungal, T.A.; Bhowmik, A.; Wedzicha, J.A. Relationship between exacerbation frequency and lung function decline in chronic obstructive pulmonary disease. Thorax 2002, 57, 847–852. [Google Scholar] [CrossRef] [Green Version]
- Brusse-Keizer, M.; van der Palen, J.; van der Valk, P.; Hendrix, R.; Kerstjens, H. Clinical predictors of exacerbation frequency in chronic obstructive pulmonary disease. Clin. Respir. J. 2011, 5, 227–234. [Google Scholar] [CrossRef]
- McGarvey, L.; Lee, A.J.; Roberts, J.; Gruffydd-Jones, K.; McKnight, E.; Haughney, J. Characterisation of the frequent exacerbator phenotype in COPD patients in a large UK primary care population. Respir. Med. 2015, 109, 228–237. [Google Scholar] [CrossRef]
- Capozzolo, A.; Carratu, P.; Dragonieri, S.; Falcone, V.A.; Quaranta, V.N.; Liotino, V.; D’Alba, G.; Castellana, G.; Resta, O. Clinical and Functional Lung Parameters Associated With Frequent Exacerbator Phenotype in Subjects With Severe COPD. Respir. Care 2017, 62, 572–578. [Google Scholar] [CrossRef]
- Dilektasli, A.G.; Demirdogen Cetinoglu, E.; Uzaslan, E.; Budak, F.; Coskun, F.; Ursavas, A.; Ercan, I.; Ege, E. Serum CCL-18 level is a risk factor for COPD exacerbations requiring hospitalization. Int. J. Chron. Obstruct. Pulmon. Dis. 2017, 12, 199–208. [Google Scholar] [CrossRef] [Green Version]
- Wedzicha, J.A.; Brill, S.E.; Allinson, J.P.; Donaldson, G.C. Mechanisms and impact of the frequent exacerbator phenotype in chronic obstructive pulmonary disease. BMC Med. 2013, 11, 181. [Google Scholar] [CrossRef]
- Wedzicha, J.A.; Rabe, K.F.; Martinez, F.J.; Bredenbroker, D.; Brose, M.; Goehring, U.M.; Calverley, P.M.A. Efficacy of roflumilast in the COPD frequent exacerbator phenotype. Chest 2013, 143, 1302–1311. [Google Scholar] [CrossRef]
- Uzun, S.; Djamin, R.S.; Kluytmans, J.A.; Mulder, P.G.; van’t Veer, N.E.; Ermens, A.A.; Pelle, A.J.; Hoogsteden, H.C.; Aerts, J.G.; van der Eerden, M.M. Azithromycin maintenance treatment in patients with frequent exacerbations of chronic obstructive pulmonary disease (COLUMBUS): A randomised, double-blind, placebo-controlled trial. Lancet Respir. Med. 2014, 2, 361–368. [Google Scholar] [CrossRef]
- Reilev, M.; Lykkegaard, J.; Halling, A.; Vestbo, J.; Sondergaard, J.; Pottegard, A. Stability of the frequent COPD exacerbator in the general population: A Danish nationwide register-based study. NPJ Prim. Care Respir. Med. 2017, 27, 25. [Google Scholar] [CrossRef]
- Elsammak MY, A.A.; Suleman, M. Fibroblast growth factor-23 and hypophosphatemia in chronic obstructive pulmonary disease patients. J. Med. Biochem. 2012, 31, 12–18. [Google Scholar] [CrossRef]
- Gutierrez, O.M.; Mannstadt, M.; Isakova, T.; Rauh-Hain, J.A.; Tamez, H.; Shah, A.; Smith, K.; Lee, H.; Thadhani, R.; Juppner, H.; et al. Fibroblast growth factor 23 and mortality among patients undergoing hemodialysis. N. Engl. J. Med. 2008, 359, 584–592. [Google Scholar] [CrossRef]
- Munoz Mendoza, J.; Isakova, T.; Cai, X.; Bayes, L.Y.; Faul, C.; Scialla, J.J.; Lash, J.P.; Chen, J.; He, J.; Navaneethan, S.; et al. Inflammation and elevated levels of fibroblast growth factor 23 are independent risk factors for death in chronic kidney disease. Kidney Int. 2017, 91, 711–719. [Google Scholar] [CrossRef]
- Isakova, T.; Cai, X.; Lee, J.; Xie, D.; Wang, X.; Mehta, R.; Allen, N.B.; Scialla, J.J.; Pencina, M.J.; Anderson, A.H.; et al. Longitudinal FGF23 Trajectories and Mortality in Patients with CKD. J. Am. Soc. Nephrol. 2018, 29, 579–590. [Google Scholar] [CrossRef]
- Yuen, S.N.; Kramer, H.; Luke, A.; Bovet, P.; Plange-Rhule, J.; Forrester, T.; Lambert, V.; Wolf, M.; Camacho, P.; Harders, R.; et al. Fibroblast Growth Factor-23 (FGF-23) Levels Differ Across Populations by Degree of Industrialization. J. Clin. Endocrinol. Metab. 2016, 101, 2246–2253. [Google Scholar] [CrossRef] [Green Version]
- Wolf, M. Update on fibroblast growth factor 23 in chronic kidney disease. Kidney Int. 2012, 82, 737–747. [Google Scholar] [CrossRef]
- Krick, S.; Grabner, A.; Baumlin, N.; Yanucil, C.; Helton, S.; Grosche, A.; Sailland, J.; Geraghty, P.; Viera, L.; Russell, D.W.; et al. Fibroblast Growth Factor 23 and Klotho Contribute to Airway Inflammation. Eur. Respir. J. 2018, 52, 1800236. [Google Scholar] [CrossRef]
- Hurst, J.R.; Vestbo, J.; Anzueto, A.; Locantore, N.; Mullerova, H.; Tal-Singer, R.; Miller, B.; Lomas, D.A.; Agusti, A.; Macnee, W.; et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N. Engl. J. Med. 2010, 363, 1128–1138. [Google Scholar] [CrossRef]
- He, X.; Shen, Y.; Ma, X.; Ying, L.; Peng, J.; Pan, X.; Bao, Y.; Zhou, J. The association of serum FGF23 and non-alcoholic fatty liver disease is independent of vitamin D in type 2 diabetes patients. Clin. Exp. Pharmacol. Physiol. 2018, 45, 668–674. [Google Scholar] [CrossRef]
- Hu, X.; Ma, X.; Luo, Y.; Xu, Y.; Xiong, Q.; Pan, X.; Bao, Y.; Jia, W. Elevation in fibroblast growth factor 23 and its value for identifying subclinical atherosclerosis in first-degree relatives of patients with diabetes. Sci. Rep. 2016, 6, 34696. [Google Scholar] [CrossRef] [Green Version]
- Shimada, T.; Urakawa, I.; Isakova, T.; Yamazaki, Y.; Epstein, M.; Wesseling-Perry, K.; Wolf, M.; Salusky, I.B.; Juppner, H. Circulating fibroblast growth factor 23 in patients with end-stage renal disease treated by peritoneal dialysis is intact and biologically active. J. Clin. Endocrinol. Metab. 2010, 95, 578–585. [Google Scholar] [CrossRef]
- Fernandez-Real, J.M.; Puig, J.; Serrano, M.; Sabater, M.; Rubio, A.; Moreno-Navarrete, J.M.; Fontan, M.; Casamitjana, R.; Xifra, G.; Ortega, F.J.; et al. Iron and obesity status-associated insulin resistance influence circulating fibroblast-growth factor-23 concentrations. PLoS ONE 2013, 8, e58961. [Google Scholar] [CrossRef]
- Mirza, M.A.; Alsio, J.; Hammarstedt, A.; Erben, R.G.; Michaelsson, K.; Tivesten, A.; Marsell, R.; Orwoll, E.; Karlsson, M.K.; Ljunggren, O.; et al. Circulating fibroblast growth factor-23 is associated with fat mass and dyslipidemia in two independent cohorts of elderly individuals. Arterioscler. Thromb. Vasc. Biol. 2011, 31, 219–227. [Google Scholar] [CrossRef]
- Leaf, D.E.; Waikar, S.S.; Wolf, M.; Cremers, S.; Bhan, I.; Stern, L. Dysregulated mineral metabolism in patients with acute kidney injury and risk of adverse outcomes. Clin. Endocrinol. 2013, 79, 491–498. [Google Scholar] [CrossRef]
- Andersen, I.A.; Huntley, B.K.; Sandberg, S.S.; Heublein, D.M.; Burnett, J.C., Jr. Elevation of circulating but not myocardial FGF23 in human acute decompensated heart failure. Nephrol. Dial. Transplant 2016, 31, 767–772. [Google Scholar] [CrossRef]
- Couillard, A.; Muir, J.F.; Veale, D. COPD recent findings: Impact on clinical practice. COPD 2010, 7, 204–213. [Google Scholar] [CrossRef]
- Fiaccadori, E.; Coffrini, E.; Fracchia, C.; Rampulla, C.; Montagna, T.; Borghetti, A. Hypophosphatemia and phosphorus depletion in respiratory and peripheral muscles of patients with respiratory failure due to COPD. Chest 1994, 105, 1392–1398. [Google Scholar] [CrossRef]
- Crul, T.; Spruit, M.A.; Gayan-Ramirez, G.; Quarck, R.; Gosselink, R.; Troosters, T.; Pitta, F.; Decramer, M. Markers of inflammation and disuse in vastus lateralis of chronic obstructive pulmonary disease patients. Eur. J. Clin. Investig. 2007, 37, 897–904. [Google Scholar] [CrossRef]
- Pitta, F.; Troosters, T.; Probst, V.S.; Spruit, M.A.; Decramer, M.; Gosselink, R. Physical activity and hospitalization for exacerbation of COPD. Chest 2006, 129, 536–544. [Google Scholar] [CrossRef]
- Serres, I.; Gautier, V.; Varray, A.; Prefaut, C. Impaired skeletal muscle endurance related to physical inactivity and altered lung function in COPD patients. Chest 1998, 113, 900–905. [Google Scholar] [CrossRef]
- Singh, S.; Grabner, A.; Yanucil, C.; Schramm, K.; Czaya, B.; Krick, S.; Czaja, M.J.; Bartz, R.; Abraham, R.; Di Marco, G.S.; et al. Fibroblast growth factor 23 directly targets hepatocytes to promote inflammation in chronic kidney disease. Kidney Int. 2016, 90, 985–996. [Google Scholar] [CrossRef] [Green Version]
- Krick, S.; Baumlin, N.; Aller, S.P.; Aguiar, C.; Grabner, A.; Sailland, J.; Mendes, E.; Schmid, A.; Qi, L.; David, N.V.; et al. Klotho Inhibits Interleukin-8 Secretion from Cystic Fibrosis Airway Epithelia. Sci. Rep. 2017, 7, 14388. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Martin, A.; David, V.; Quarles, L.D. Compound deletion of Fgfr3 and Fgfr4 partially rescues the Hyp mouse phenotype. Am. J. Physiol. Endocrinol. Metab. 2011, 300, E508–E517. [Google Scholar] [CrossRef]
- Gao, W.; Yuan, C.; Zhang, J.; Li, L.; Yu, L.; Wiegman, C.H.; Barnes, P.J.; Adcock, I.M.; Huang, M.; Yao, X. Klotho expression is reduced in COPD airway epithelial cells: Effects on inflammation and oxidant injury. Clin. Sci. 2015, 129, 1011–1023. [Google Scholar] [CrossRef]
- Culver, B.H.; Graham, B.L.; Coates, A.L.; Wanger, J.; Berry, C.E.; Clarke, P.K.; Hallstrand, T.S.; Hankinson, J.L.; Kaminsky, D.A.; MacIntyre, N.R.; et al. Recommendations for a Standardized Pulmonary Function Report. An Official American Thoracic Society Technical Statement. Am. J. Respir. Crit. Care Med. 2017, 196, 1463–1472. [Google Scholar] [CrossRef]
- Rodriguez-Roisin, R. Toward a consensus definition for COPD exacerbations. Chest 2000, 117, 398S–401S. [Google Scholar] [CrossRef]
- Burge, S.; Wedzicha, J.A. COPD exacerbations: Definitions and classifications. Eur. Respir. J. 2003, 21 (Suppl. 41), 46s–53s. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable (n = 70) | |
|---|---|
| Age, years (SD) | 69 (6) |
| Male, % | 94% |
| White race, % | 69% |
| BMI, kg/m2 (SD) | 25.6 (5.5) |
| FEV1, %predicted (SD) | 46.5 (15.5) |
| FEV1/FVC, (SD) | 0.44 (0.11) |
| Current smokers, % | 26% |
| Smoking pack years, (SD) | 60 (37) |
| Supplemental oxygen use | 18 (26%) |
| Serum WBC (103 cells/mm3) (SD) | 8.5 (7.1) |
| Plasma FGF23, pg/mL, (SD) | 56.5 (35.3) |
| Serum Creatinine (mg/dL) (SD) | 1.0 (0.2) |
| Variable, n (SD) | Infrequent Exacerbators (n = 62) * | Frequent Exacerbators (n = 8) # | p Value |
|---|---|---|---|
| Age, years (SD) | 68.4 (5.7) | 70.2 (4.8) | 0.386 |
| Male, % | 58 (93.5%) | 8 (100%) | 0.323 |
| White race | 47 (75.8%) | 3 (37.5%) | 0.037 |
| BMI, mg/k2 (SD) | 25.6 (5.8) | 26.2 (3.4) | 0.769 |
| FEV1, % (SD) | 46.5 (15.6) | 46.5 (16.0) | 1.00 |
| FEV1/FVC, | 43.7 (11.4) | 47.7 (12.3) | 0.359 |
| Creatinine, mg/dL (SD) | 0.99 (0.22) | 1.0 (0.29) | 0.296 |
| Current smoker | 17 (27.4%) | 1 (12.5%) | 0.539 |
| Smoking pack years | 60.7 (38.6) | 55.2 (19.3) | 0.696 |
| Supplemental O2 use | 15 (24.2%) | 3 (37.5%) | 0.412 |
| CAT score | 17.6 (9.0) | 16.2 (7.7) | 0.712 |
| mMRC dyspnea scale | 1.91 (1.3) | 1.85 (1.3) | 0.906 |
| SGRQ, Total | 46.7 (21.4) | 50.0 (26.2) | 0.748 |
| Charlson Index | 5.0 (2.1) | 6.8 (5.0) | 0.068 |
| BODE score | 4.5 (2.0) | 4.1 (2.0) | 0.670 |
| Variable | Unadjusted Model | Adjusted Model | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p Value | OR | 95% CI | p Value | |
| Age | 1.13 | 1.00–1.26 | 0.043 | 1.04 | 0.90–1.21 | 0.601 |
| Smoking, pack years | 0.97 | 0.95–1.00 | 0.046 | 0.98 | 0.95–1.01 | 0.106 |
| Post-BD FEV1, % | 0.99 | 0.95−1.03 | 0.683 | |||
| WBC | 1.10 | 0.94–1.29 | 0.228 | |||
| Creatinine | 2.34 | 0.22–25.1 | 0.483 | |||
| FGF23 | 1.02 | 1.00–1.04 | 0.017 | 1.02 | 1.004–1.04 | 0.019 |
| Suppl. Oxygen Use | 4.09 | 1.19–14.1 | 0.026 | 4.85 | 1.18–19.9 | 0.028 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gulati, S.; Wells, J.M.; Urdaneta, G.P.; Balestrini, K.; Vital, I.; Tovar, K.; Barnes, J.W.; Bhatt, S.P.; Campos, M.; Krick, S. Fibroblast Growth Factor 23 is Associated with a Frequent Exacerbator Phenotype in COPD: A Cross-Sectional Pilot Study. Int. J. Mol. Sci. 2019, 20, 2292. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20092292
Gulati S, Wells JM, Urdaneta GP, Balestrini K, Vital I, Tovar K, Barnes JW, Bhatt SP, Campos M, Krick S. Fibroblast Growth Factor 23 is Associated with a Frequent Exacerbator Phenotype in COPD: A Cross-Sectional Pilot Study. International Journal of Molecular Sciences. 2019; 20(9):2292. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20092292
Chicago/Turabian StyleGulati, Swati, J. Michael Wells, Gisel P. Urdaneta, Kira Balestrini, Isabel Vital, Katherine Tovar, Jarrod W. Barnes, Surya P. Bhatt, Michael Campos, and Stefanie Krick. 2019. "Fibroblast Growth Factor 23 is Associated with a Frequent Exacerbator Phenotype in COPD: A Cross-Sectional Pilot Study" International Journal of Molecular Sciences 20, no. 9: 2292. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20092292