The Influence of Local Pamidronate Application on Alveolar Dimensional Preservation after Tooth Extraction—An Animal Experimental Study

 , ,
, , 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
2.1. Cast Models
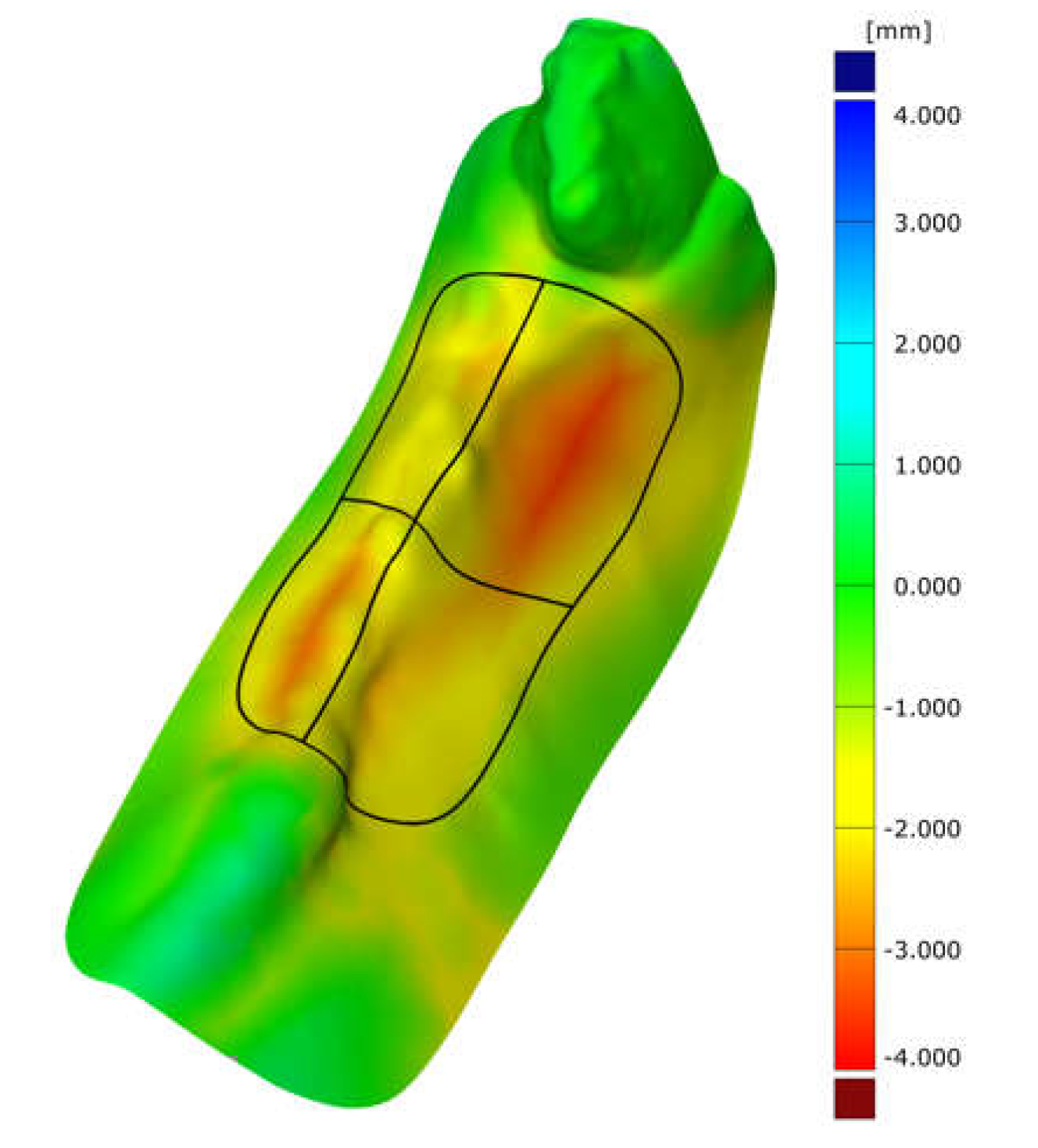
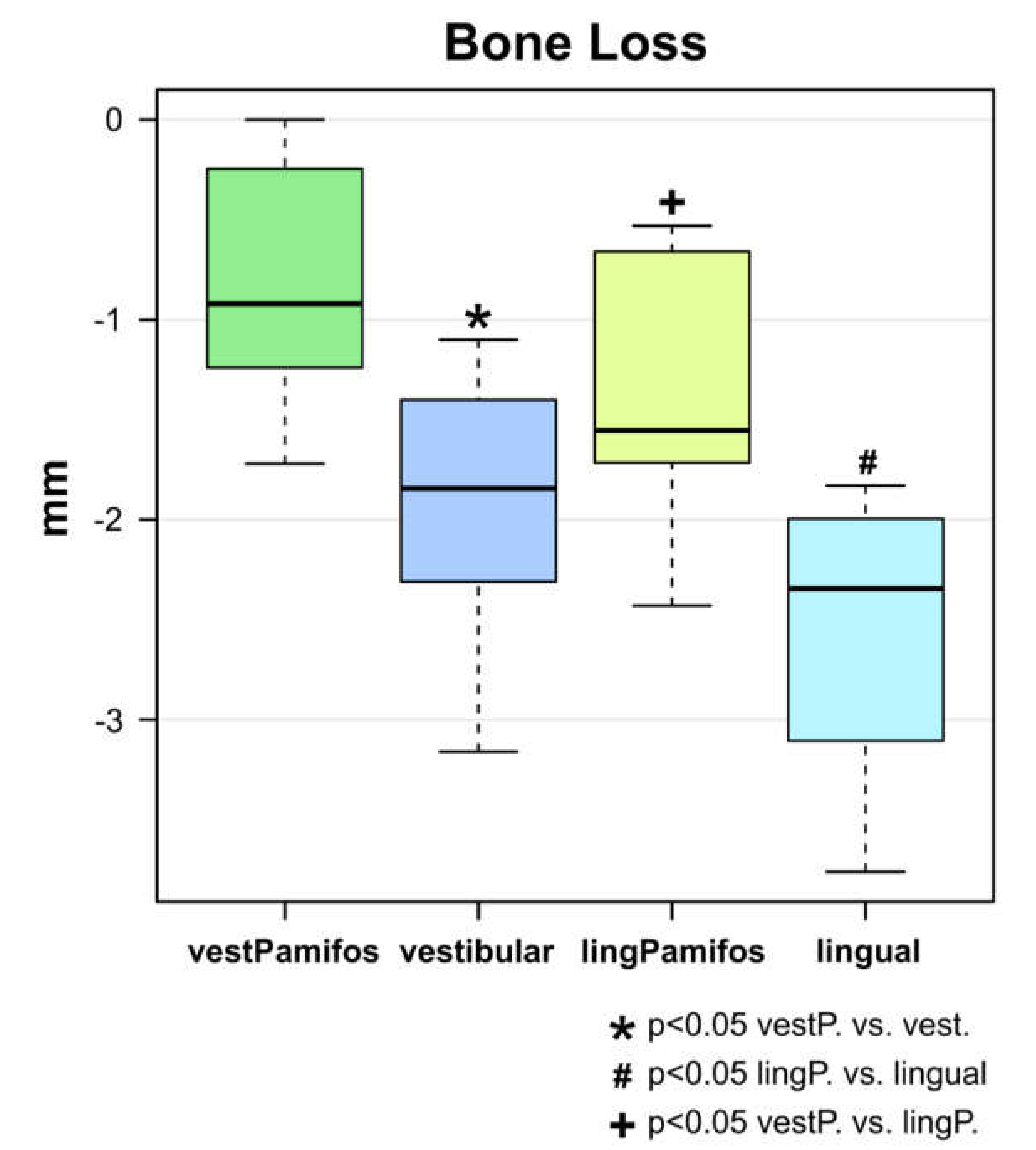
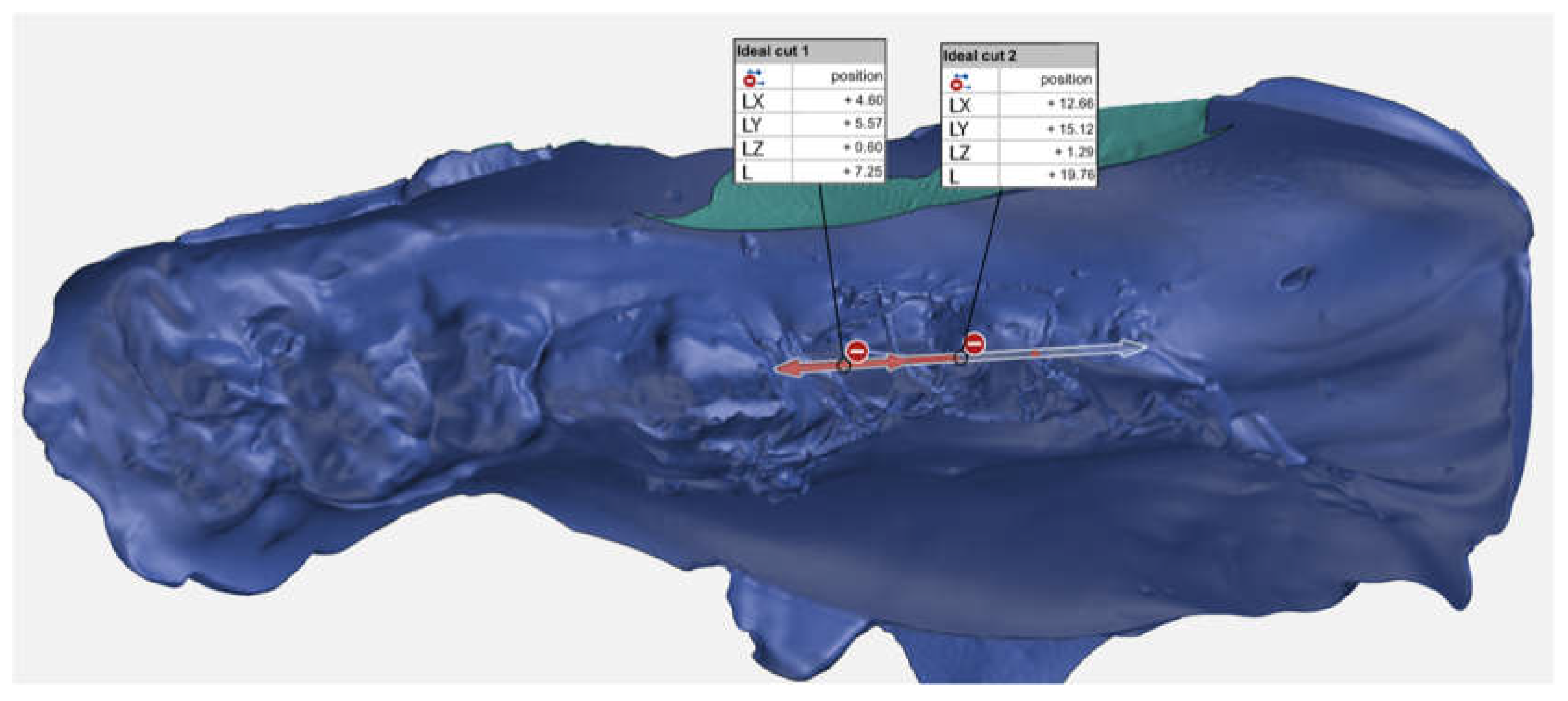
2.2. Superimposition Analysis
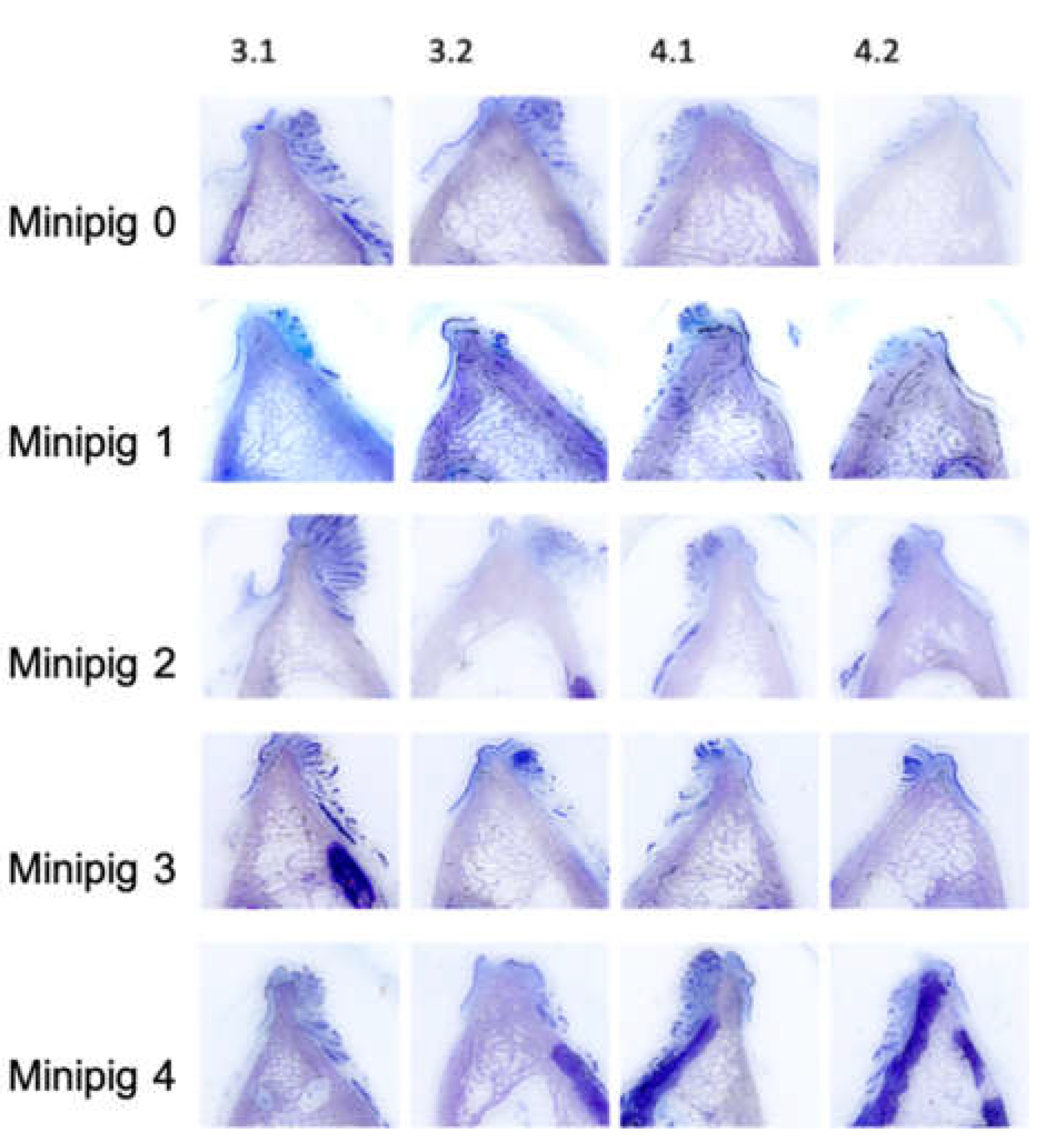
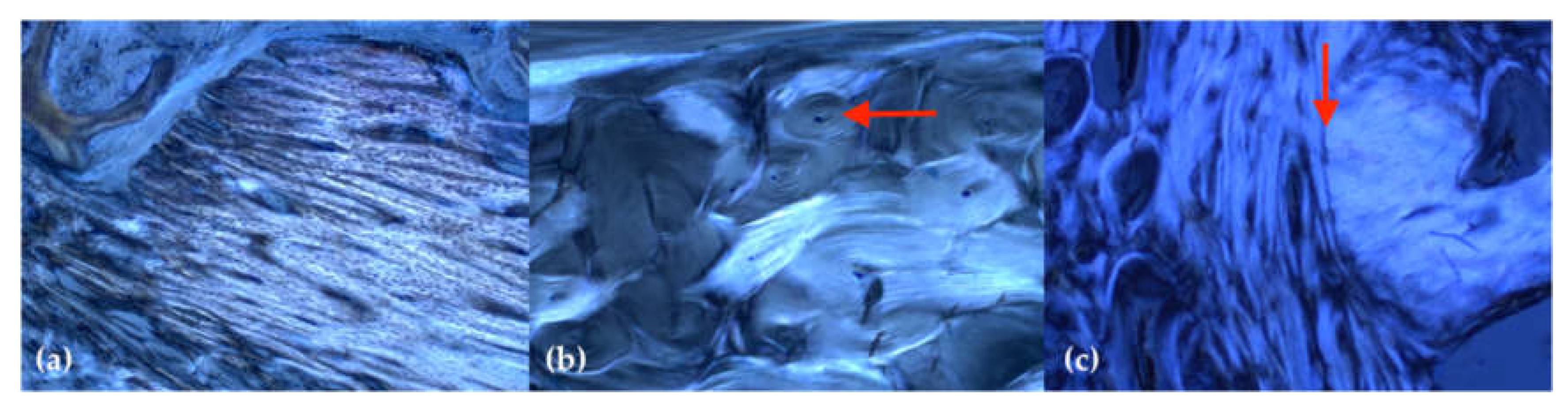
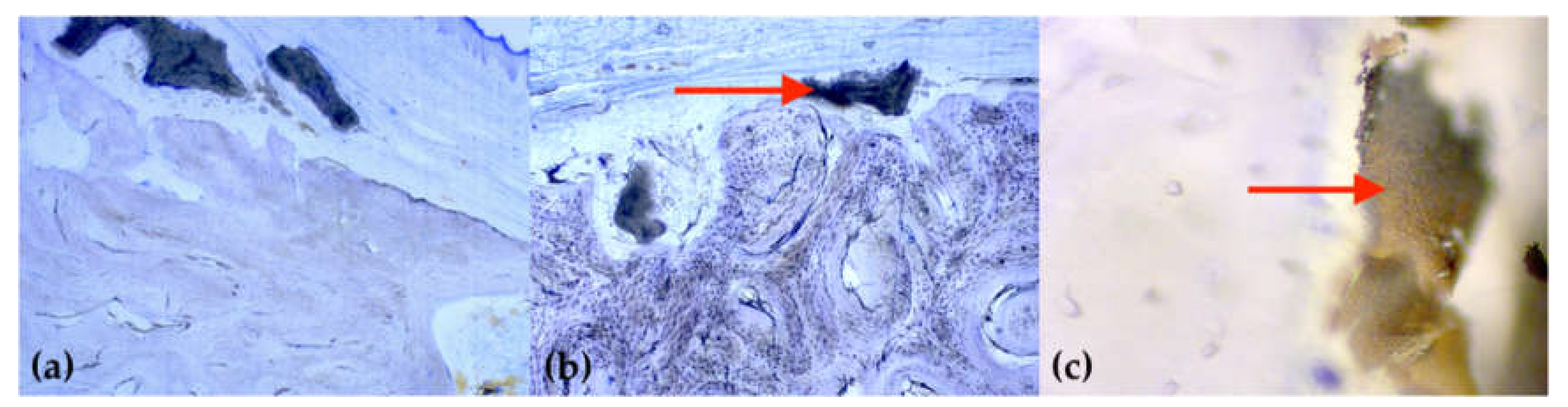
2.3. Histology
3. Discussion
4. Materials and Methods
4.1. Animals—General Information
4.2. Animals—Anesthesia and Surgery
4.3. Dental Models, Scanning Procedure, and Digital Analysis
4.4. Histological Analysis
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| BSM | Bone substitute material |
| GBR | Guided bone regeneration |
| rhBMP2 | Recombinant human bone morphogenic protein 2 |
| bFGF | Basic fibroblast growth factor |
| rhPDGF | Recombinant human platelet derived growth factor |
| TGF-b | Transforming growth factor beta |
| APC | Autologous platelet concentrates |
| SP | Socket preservation |
| BP | Bisphosphonate |
| BRONJ | Bisphosphonate-related osteonecrosis of the jaw |
| APD | Pamidronate |
| ALN | Alendronate |
| CBCT | Cone-beam computed tomography |
References
- Persson, R.E.; Hollender, L.G.; Laurell, L.; Persson, G.R. Horizontal alveolar bone loss and vertical bone defects in an adult patient population. J. Periodontol. 1998, 69, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Schei, O.; Waerhaug, J.; Lovdal, A.; Arno, A. Alveolar bone loss as related to oral hygiene and age. J. Periodontol. 1959, 30, 7–16. [Google Scholar] [CrossRef]
- Tan, W.L.; Wong, T.L.; Wong, M.C.; Lang, N.P. A systematic review of post-extractional alveolar hard and soft tissue dimensional changes in humans. Clin. Oral Implant. Res. 2012, 23 (Suppl. 5), 1–21. [Google Scholar] [CrossRef] [PubMed]
- van der Weijden, F.; Dell’Acqua, F.; Slot, D.E. Alveolar bone dimensional changes of post-extraction sockets in humans: A systematic review. J. Clin. Periodontol. 2009, 36, 1048–1058. [Google Scholar] [CrossRef]
- Araujo, M.G.; Lindhe, J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J. Clin. Periodontol. 2005, 32, 212–218. [Google Scholar] [CrossRef]
- Cardaropoli, G.; Araujo, M.G.; Lindhe, J. Dynamics of bone tissue formation in tooth extraction sites: An experimental study in dogs. J. Clin. Periodontol. 2003, 30, 809–818. [Google Scholar] [CrossRef]
- Araujo, M.G.; Wennstrom, J.L.; Lindhe, J. Modeling of the buccal and lingual bone walls of fresh extraction sites following implant installation. Clin. Oral Implant. Res. 2006, 17, 606–614. [Google Scholar] [CrossRef]
- Chappuis, V.; Engel, O.; Reyes, M.; Shahim, K.; Nolte, L.P.; Buser, D. Ridge alterations post-extraction in the esthetic zone: A 3D analysis with CBCT. J. Dent. Res. 2013, 92 (Suppl. 12), 195–201. [Google Scholar] [CrossRef] [Green Version]
- McAllister, B.S.; Haghighat, K. Bone augmentation techniques. J. Periodontol. 2007, 78, 377–396. [Google Scholar] [CrossRef] [Green Version]
- Chiapasco, M.; Casentini, P.; Zaniboni, M. Bone augmentation procedures in implant dentistry. Int. J. Oral Maxillofac. Implant. 2009, 24, 237–259. [Google Scholar]
- Yamada, M.; Egusa, H. Current bone substitutes for implant dentistry. J. Prosthodont. Res. 2018, 62, 152–161. [Google Scholar] [CrossRef] [PubMed]
- Bauer, T.W.; Muschler, G.F. Bone graft materials. An overview of the basic science. Clin. Orthop. Relat. Res. 2000, 371, 10–27. [Google Scholar] [CrossRef]
- Jambhekar, S.; Kernen, F.; Bidra, A.S. Clinical and histologic outcomes of socket grafting after flapless tooth extraction: A systematic review of randomized controlled clinical trials. J. Prosthet. Dent. 2015, 113, 371–382. [Google Scholar] [CrossRef] [PubMed]
- Troiano, G.; Zhurakivska, K.; Lo Muzio, L.; Laino, L.; Cicciu, M.; Lo Russo, L. Combination of bone graft and resorbable membrane for alveolar ridge preservation: A systematic review, meta-analysis and trial sequential analysis. J. Periodontol. 2018, 89, 46–57. [Google Scholar] [CrossRef]
- Wang, R.E.; Lang, N.P. Ridge preservation after tooth extraction. Clin. Oral Implant. Res. 2012, 23 (Suppl. 6), 147–156. [Google Scholar] [CrossRef] [PubMed]
- Howell, T.H.; Fiorellini, J.; Jones, A.; Alder, M.; Nummikoski, P.; Lazaro, M.; Lilly, L.; Cochran, D. A feasibility study evaluating rhBMP-2/absorbable collagen sponge device for local alveolar ridge preservation or augmentation. Int. J. Periodontics Restor. Dent. 1997, 17, 124–139. [Google Scholar]
- Wang, L.; Huang, Y.; Pan, K.; Jiang, X.; Liu, C. Osteogenic responses to different concentrations/ratios of BMP-2 and bFGF in bone formation. Ann. Biomed. Eng. 2010, 38, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Anitua, E.; Andia, I.; Ardanza, B.; Nurden, P.; Nurden, A.T. Autologous platelets as a source of proteins for healing and tissue regeneration. Thromb. Haemost. 2004, 91, 4–15. [Google Scholar] [CrossRef]
- Anitua, E.; Murias-Freijo, A.; Alkhraisat, M.H.; Orive, G. Clinical, radiographical, and histological outcomes of plasma rich in growth factors in extraction socket: A randomized controlled clinical trial. Clin. Oral Investig. 2015, 19, 589–600. [Google Scholar] [CrossRef]
- Del Fabbro, M.; Bucchi, C.; Lolato, A.; Corbella, S.; Testori, T.; Taschieri, S. Healing of postextraction sockets preserved with autologous platelet concentrates. A systematic review and meta-analysis. J. Oral Maxillofac. Surg. 2017, 75, 1601–1615. [Google Scholar] [CrossRef]
- Fickl, S.; Zuhr, O.; Wachtel, H.; Stappert, C.F.; Stein, J.M.; Hurzeler, M.B. Dimensional changes of the alveolar ridge contour after different socket preservation techniques. J. Clin. Periodontol. 2008, 35, 906–913. [Google Scholar] [CrossRef] [PubMed]
- Horváth, A.; Mardas, N.; Mezzomo, L.A.; Needleman, I.G.; Donos, N. Alveolar ridge preservation. A systematic review. Clin. Oral Investig. 2013, 17, 341–363. [Google Scholar] [CrossRef] [PubMed]
- De Risi, V.; Clementini, M.; Vittorini, G.; Mannocci, A.; De Sanctis, M. Alveolar ridge preservation techniques: A systematic review and meta-analysis of histological and histomorphometrical data. Clin. Oral Implant. Res. 2015, 26, 50–68. [Google Scholar] [CrossRef]
- Chaudhry, A.N.; Ruggiero, S.L. Osteonecrosis and bisphosphonates in oral and maxillofacial surgery. Oral Maxillofac. Surg. Clin. N. Am. 2007, 19, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Frijlink, W.B.; Bijvoet, O.L.; Te Velde, J.; Heynen, G. Treatment of Paget’s disease with (3-amino-1-hydroxypropylidene)-1, 1-bisphosphonate (A.P.D.). Lancet 1979, 1, 799–803. [Google Scholar] [CrossRef]
- Mundy, G.R. Metastasis to bone: Causes, consequences and therapeutic opportunities. Nat. Rev. Cancer 2002, 2, 584–593. [Google Scholar] [CrossRef]
- Sajid-Crockett, S.; Singer, F.R.; Hershman, J.M. Cinacalcet for the treatment of primary hyperparathyroidism. Metabolism 2008, 57, 517–521. [Google Scholar] [CrossRef]
- Black, D.M.; Bauer, D.C.; Schwartz, A.V.; Cummings, S.R.; Rosen, C.J. Continuing bisphosphonate treatment for osteoporosis—For whom and for how long? N. Engl. J. Med. 2012, 366, 2051–2053. [Google Scholar] [CrossRef] [Green Version]
- Djulbegovic, B.; Wheatley, K.; Ross, H.; Clark, O.A.C.; Bos, G.; Goldschmidt, H.; Cremer, F.; Alsina, M.; Glasmacher, A. Bisphosphonates in multiple myeloma. Cochrane Database Syst. Rev. 2002, 4. [Google Scholar] [CrossRef]
- de Groen, P.C.; Lubbe, D.F.; Hirsch, L.J.; Daifotis, A.; Stephenson, W.; Freedholm, D.; Pryor-Tillotson, S.; Seleznick, M.J.; Pinkas, H.; Wang, K.K. Esophagitis associated with the use of alendronate. New Engl. J. Med. 1996, 335, 1016–1021. [Google Scholar] [CrossRef]
- Kuhl, S.; Walter, C.; Acham, S.; Pfeffer, R.; Lambrecht, J.T. Bisphosphonate-related osteonecrosis of the jaws—A review. Oral Oncol. 2012, 48, 938–947. [Google Scholar] [CrossRef] [PubMed]
- Jakobsen, T.; Baas, J.; Bechtold, J.E.; Elmengaard, B.; Soballe, K. The effect of soaking allograft in bisphosphonate: A pilot dose-response study. Clin. Orthop. Relat. Res. 2010, 468, 867–874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, J.H.; Guo, W.S.; Li, Z.R.; Wang, B.L. Local administration of bisphosphonate-soaked hydroxyapatite for the treatment of osteonecrosis of the femoral head in rabbit. Chin. Med. J. 2016, 129, 2559–2566. [Google Scholar] [CrossRef] [PubMed]
- Abtahi, J.; Tengvall, P.; Aspenberg, P. A bisphosphonate-coating improves the fixation of metal implants in human bone. A randomized trial of dental implants. Bone 2012, 50, 1148–1151. [Google Scholar] [CrossRef] [Green Version]
- Jakobsen, T.; Baas, J.; Kold, S.; Bechtold, J.E.; Elmengaard, B.; Soballe, K. Local bisphosphonate treatment increases fixation of hydroxyapatite-coated implants inserted with bone compaction. J. Orthop. Res. 2009, 27, 189–194. [Google Scholar] [CrossRef] [Green Version]
- Wermelin, K.; Aspenberg, P.; Linderback, P.; Tengvall, P. Bisphosphonate coating on titanium screws increases mechanical fixation in rat tibia after two weeks. J. Biomed. Mater. Res. A 2008, 86, 220–227. [Google Scholar] [CrossRef]
- Möller, B.; Wiltfang, J.; Acil, Y.; Gierloff, M.; Lippross, S.; Terheyden, H. Prevention of the surface resorption of bone grafts by topical application of bisphosphonate on different carrier materials. Clin. Oral Investig. 2014, 18, 2203–2211. [Google Scholar] [CrossRef]
- McKenzie, K.; Dennis Bobyn, J.; Roberts, J.; Karabasz, D.; Tanzer, M. Bisphosphonate remains highly localized after elution from porous implants. Clin. Orthop. Relat. Res. 2011, 469, 514–522. [Google Scholar] [CrossRef] [Green Version]
- Schropp, L.; Wenzel, A.; Kostopoulos, L.; Karring, T. Bone healing and soft tissue contour changes following single-tooth extraction: A clinical and radiographic 12-month prospective study. Int. J. Periodontics Restor. Dent. 2003, 23, 313–323. [Google Scholar]
- Faria-Almeida, R.; Astramskaite-Januseviciene, I.; Puisys, A.; Correia, F. Extraction socket preservation with or without membranes, soft tissue influence on post extraction alveolar ridge preservation: A systematic review. J. Oral Maxillofac. Res. 2019, 10, e5. [Google Scholar] [CrossRef]
- Stumbras, A.; Kuliesius, P.; Januzis, G.; Juodzbalys, G. Alveolar ridge preservation after tooth extraction using different bone graft materials and autologous platelet concentrates: A systematic review. J. Oral Maxillofac. Res. 2019, 10, e2. [Google Scholar] [CrossRef] [PubMed]
- Guglielmotti, M.B.; Cabrini, R.L. Alveolar wound healing and ridge remodeling after tooth extraction in the rat: A histologic, radiographic, and histometric study. J. Oral Maxillofac. Surg. 1985, 43, 359–364. [Google Scholar] [CrossRef]
- Chappuis, V.; Araujo, M.G.; Buser, D. Clinical relevance of dimensional bone and soft tissue alterations post-extraction in esthetic sites. Periodontology 2000, 73, 73–83. [Google Scholar] [CrossRef] [PubMed]
- Russell, R.G.G.; Xia, Z.; Dunford, J.E.; Oppermann, U.; Kwaasi, A.; Hulley, P.A.; Kavanagh, K.; Triffitt, J.T.; Lundy, M.W.; Phipps, R.J.; et al. Bisphosphonates: An update on mechanisms of action and how these relate to clinical efficacy. Ann. N. Y. Acad. Sci. 2007, 1117, 209–257. [Google Scholar] [CrossRef] [PubMed]
- Powell, D.; Bowler, C.; Roberts, T.; Garton, M.; Matthews, C.; McCall, I.; Davie, M. Incidence of serious side effects with intravenous bisphosphonate: A clinical audit. QJM Int. J. Med. 2012, 105, 965–971. [Google Scholar] [CrossRef] [Green Version]
- Assaf, A.T.; Smeets, R.; Riecke, B.; Weise, E.; Groebe, A.; Blessmann, M.; Steiner, T.; Wikner, J.; Friedrich, R.E.; Heiland, M.; et al. Incidence of bisphosphonate-related osteonecrosis of the jaw in consideration of primary diseases and concomitant therapies. Anticancer Res. 2013, 33, 3917–3924. [Google Scholar]
- Yaffe, A.; Iztkovich, M.; Earon, Y.; Alt, I.; Lilov, R.; Binderman, I. Local delivery of an amino bisphosphonate prevents the resorptive phase of alveolar bone following mucoperiosteal flap surgery in rats. J. Periodontol. 1997, 68, 884–889. [Google Scholar] [CrossRef]
- Aspenberg, P.; Astrand, J. Bone allografts pretreated with a bisphosphonate are not resorbed. Acta Orthop. Scand. 2002, 73, 20–23. [Google Scholar] [CrossRef]
- Fischer, K.R.; Stavropoulos, A.; Calvo-Guirado, J.L.; Schneider, D.; Fickl, S. Influence of local administration of pamidronate on extraction socket healing—A histomorphometric proof-of-principle pre-clinical In Vivo evaluation. Clin. Oral Implant. Res. 2015, 26, 1135–1142. [Google Scholar] [CrossRef]
- Lozano-Carrascal, N.; Delgado-Ruiz, R.A.; Gargallo-Albiol, J.; Maté-Sánchez, J.E.; Hernandez Alfaro, F.; Calvo-Guirado, J.L. Xenografts supplemented with Pamindronate placed in postextraction sockets to avoid crestal bone resorption. Experimental study in Fox hound dogs. Clin. Oral Implant. Res. 2016, 27, 149–155. [Google Scholar] [CrossRef]
- Cha, J.K.; Sun, Y.K.; Kim, M.J.; Sanz, M.; Jung, U.W. Anti-Resorptive effect of pamidronate on extraction socket wall in dogs. Clin. Oral Implant. Res. 2018, 29, 688–696. [Google Scholar] [CrossRef] [PubMed]
- Saulacic, N.; Muñoz, F.; Kobayashi, E.; Chappuis, V.; Gonzáles-Cantalapiedra, A.; Hofstetter, W. Effects of local application of alendronate on early healing of extraction socket in dogs. Clin. Oral Investig. 2019, 1–11. [Google Scholar] [CrossRef] [PubMed]
- De Sarkar, A.; Singhvi, N.; Shetty, J.N.; Ramakrishna, T.; Shetye, O.; Islam, M.; Keerthy, H. The local effect of alendronate with intra-alveolar collagen sponges on post extraction alveolar ridge resorption: A clinical trial. J. Maxillofac. Oral Surg. 2015, 14, 344–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Research Council. Guide for the Care and Use of Laboratory Animals; National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Hahn, M.; Vogel, M.; Delling, G. Undecalcified preparation of bone tissue: Report of technical experience and development of new methods. Virchows Arch. A Pathol. Anat. 1991, 418, 1–7. [Google Scholar] [CrossRef]






© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kauffmann, F.; Höhne, C.; Assaf, A.T.; Vollkommer, T.; Semmusch, J.; Reitmeier, A.; Michel Stein, J.; Heiland, M.; Smeets, R.; Rutkowski, R. The Influence of Local Pamidronate Application on Alveolar Dimensional Preservation after Tooth Extraction—An Animal Experimental Study. Int. J. Mol. Sci. 2020, 21, 3616. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21103616
Kauffmann F, Höhne C, Assaf AT, Vollkommer T, Semmusch J, Reitmeier A, Michel Stein J, Heiland M, Smeets R, Rutkowski R. The Influence of Local Pamidronate Application on Alveolar Dimensional Preservation after Tooth Extraction—An Animal Experimental Study. International Journal of Molecular Sciences. 2020; 21(10):3616. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21103616
Chicago/Turabian StyleKauffmann, Frederic, Christian Höhne, Alexandre Thomas Assaf, Tobias Vollkommer, Jan Semmusch, Aline Reitmeier, Jamal Michel Stein, Max Heiland, Ralf Smeets, and Rico Rutkowski. 2020. "The Influence of Local Pamidronate Application on Alveolar Dimensional Preservation after Tooth Extraction—An Animal Experimental Study" International Journal of Molecular Sciences 21, no. 10: 3616. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21103616