Genomic Biomarkers of Survival in Patients with Adenocarcinoma of the Uterine Cervix Receiving Chemoradiotherapy

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Treatment Outcomes
2.2. Genomic Alterations
2.3. Predictive Ability of Genomic Alteration, the TMN, and Immunohistochemical (IHC) Biomarkers
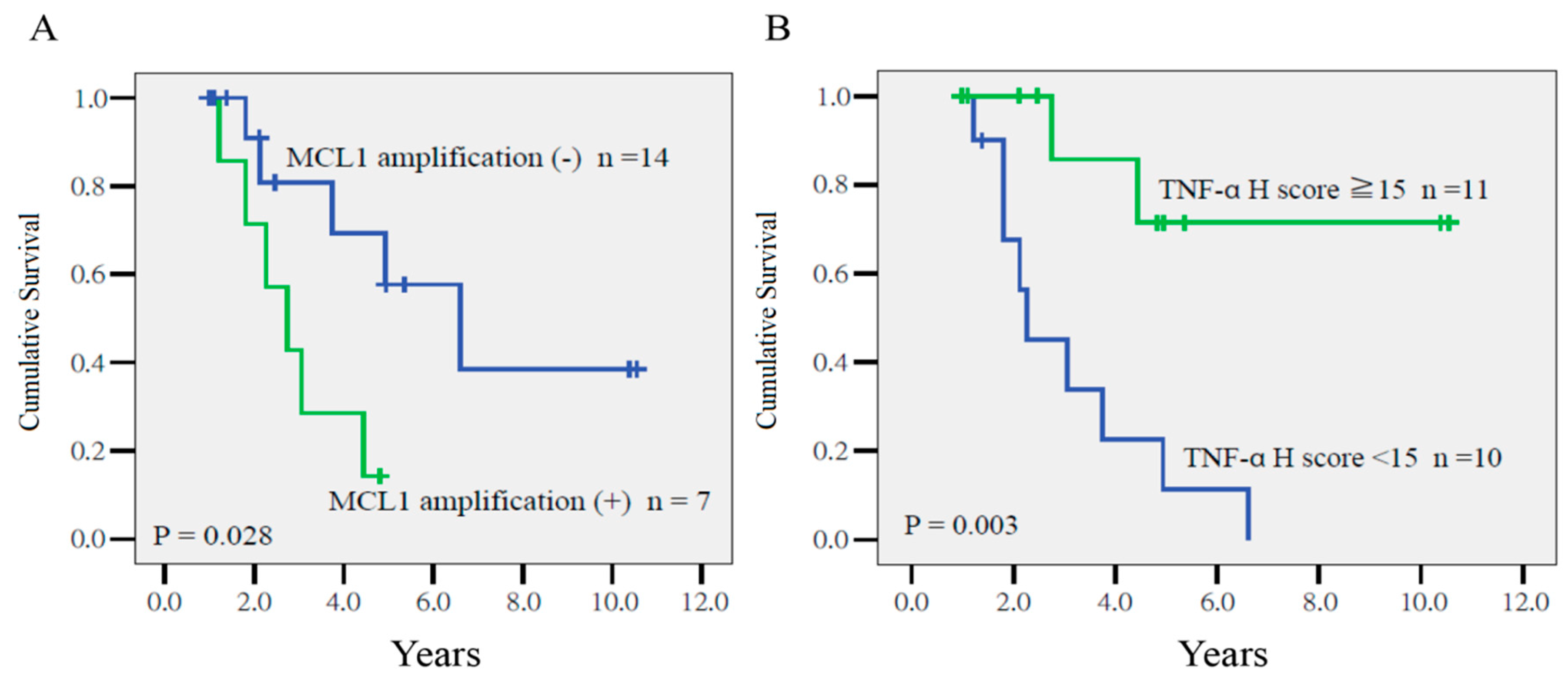
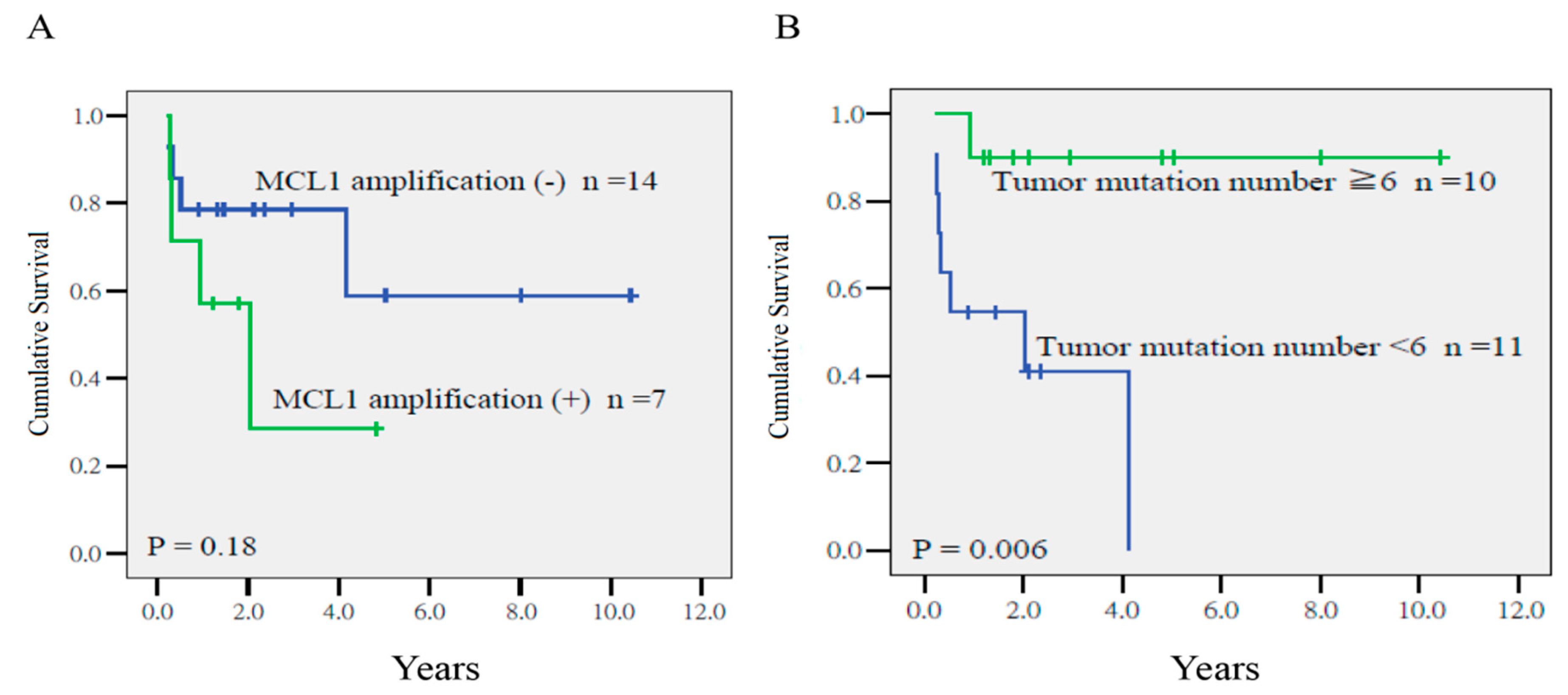
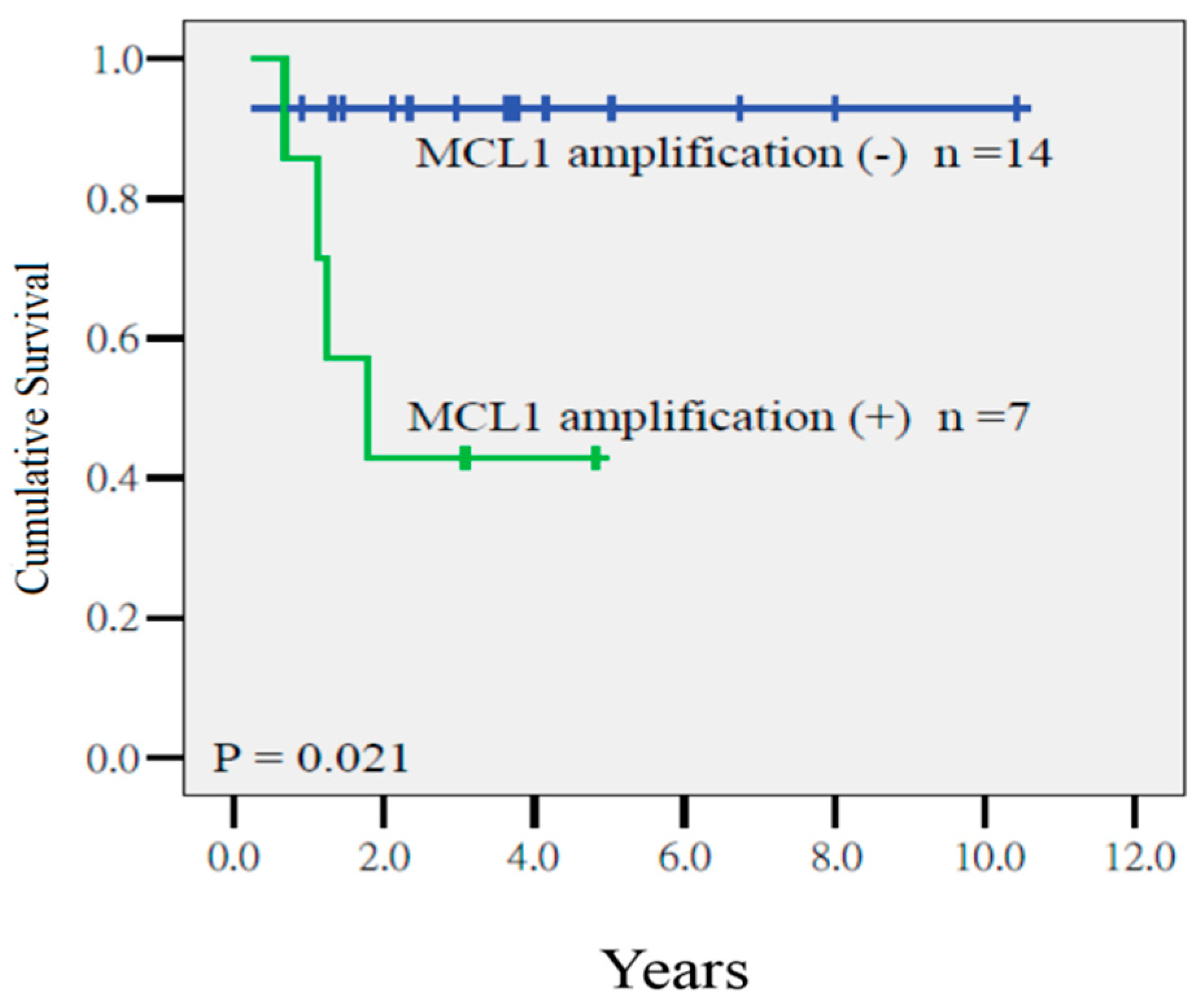
2.4. Prognostic Factors for Disease-Free Survival (DFS), Local Relapse-Free survival (LRFS), and Distant Metastasis-Free Survival (DMFS)
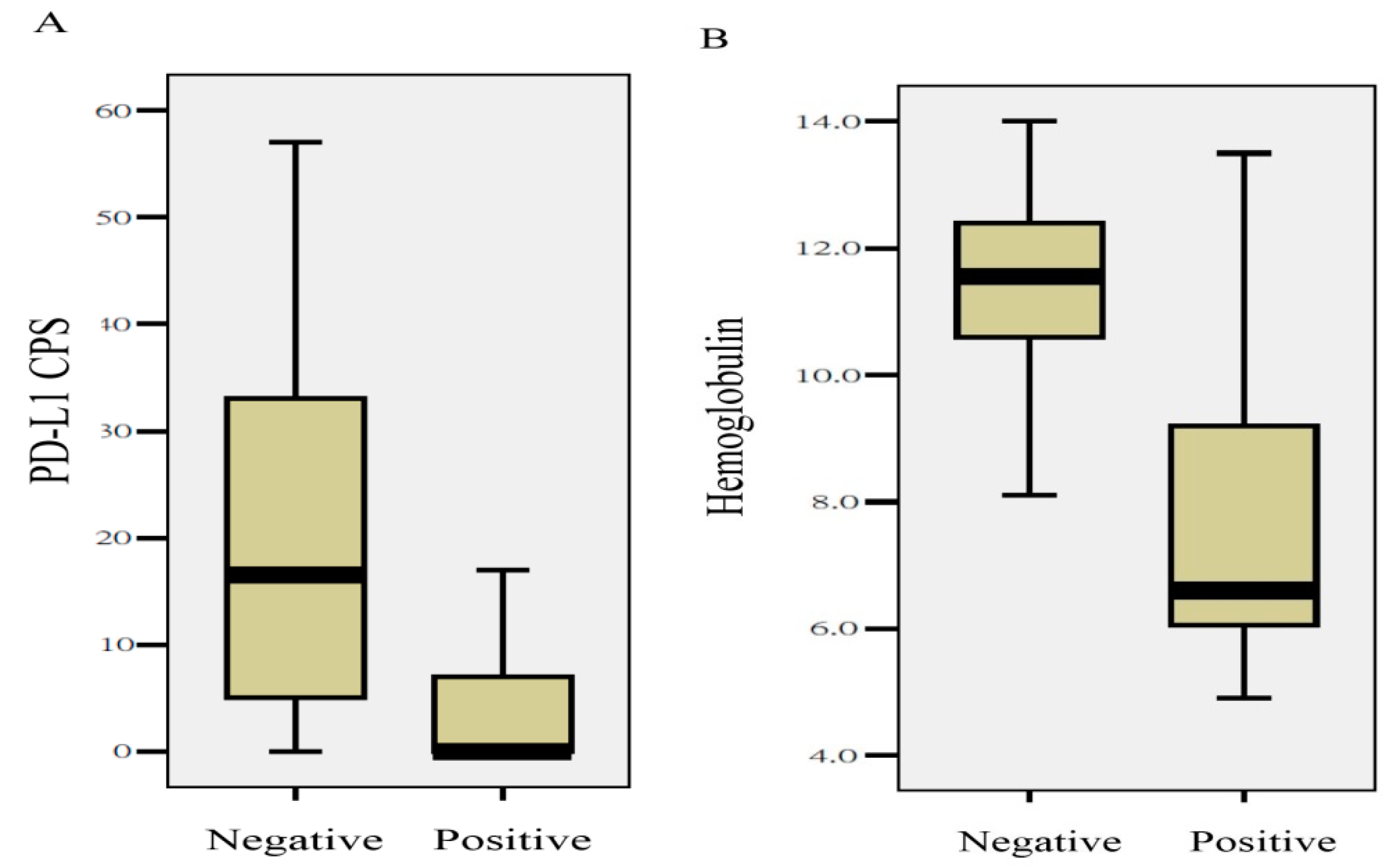
2.5. Quantitative Differences in Clinical Parameters and Biomarkers between Tumors with or without MCL1 Amplification
2.6. Validation Results in TCGA
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. DNA Extraction
4.3. Whole Exome Sequencing
4.4. Targeted DNA Sequencing
4.5. Data Analysis
4.6. Definition of Myeloid Cell Leukemia-1 Amplification
4.7. Immunohistochemistry
4.8. Treatment
4.9. Follow-Up
4.10. Statistical Analysis
4.11. External Validation in TCGA
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Jemal, A.; Bray, F.; Center, M.M.; Ferlay, J.; Ward, E.; Forman, D. Global cancer statistics. CA Cancer J. Clin. 2011, 61, 69–90. [Google Scholar] [CrossRef] [Green Version]
- Mathew, A.; George, P.S. Trends in incidence and mortality rates of squamous cell carcinoma and adenocarcinoma of cervix—Worldwide. Asian Pac. J. Cancer Prev. 2009, 10, 645–650. [Google Scholar]
- Smith, H.O.; Tiffany, M.F.; Qualls, C.R.; Key, C.R. The rising incidence of adenocarcinoma relative to squamous cell carcinoma of the uterine cervix in the United States—A 24-year population-based study. Gynecol. Oncol. 2000, 78, 97–105. [Google Scholar] [CrossRef]
- Gien, L.T.; Beauchemin, M.C.; Thomas, G. Adenocarcinoma: A unique cervical cancer. Gynecol. Oncol. 2010, 116, 140–146. [Google Scholar] [CrossRef]
- Bosch, F.; Manos, M.M.; Muñoz, N.; Sherman, M.; Jansen, A.M.; Peto, J.; Schiffman, M.H.; Moreno, V.; Kurman, R.; Shan, K.V.; et al. Prevalence of Human Papillomavirus in Cervical Cancer: A Worldwide Perspective. J. Natl. Cancer Inst. 1995, 87, 796–802. [Google Scholar] [CrossRef]
- Hopkins, M.P.; Morley, G.W. A comparison of adenocarcinoma and squamous cell carcinoma of the cervix. Obstet. Gynecol. 1991, 77, 912–917. [Google Scholar] [CrossRef]
- Castellsagué, X.; Diaz, M.; De Sanjose, S.; Muñoz, N.; Herrero, R.; Franceschi, S.; Peeling, R.W.; Ashley, R.; Smith, J.S.; Snijders, P.J.; et al. Worldwide Human Papillomavirus Etiology of Cervical Adenocarcinoma and Its Cofactors: Implications for Screening and Prevention. J. Natl. Cancer Inst. 2006, 98, 303–315. [Google Scholar] [CrossRef]
- Contag, S.; Gostout, B.S.; Clayton, A.C.; Dixon, M.H.; McGovern, R.M.; Calhoun, E.S. Comparison of gene expression in squamous cell carcinoma and adenocarcinoma of the uterine cervix. Gynecol. Oncol. 2004, 95, 610–617. [Google Scholar] [CrossRef]
- The Cancer Genome Atlas Research Network; Cancer Genome Atlas Research Network; Albert Einstein College of Medicine; Services, A.B.; Hospital, B.C.; Baylor College of Medicine; Beckman Research Institute of City of Hope; Buck Institute for Research on Aging; Canada’s Michael Smith Genome Sciences Centre; Harvard Medical School; et al. Integrated genomic and molecular characterization of cervical cancer. Nature 2017, 543, 378–384. [Google Scholar] [CrossRef]
- Eifel, P.; Burke, T.; Morris, M.; Smith, T. Adenocarcinoma as an Independent Risk Factor for Disease Recurrence in Patients with Stage IB Cervical Carcinoma. Gynecol. Oncol. 1995, 59, 38–44. [Google Scholar] [CrossRef]
- Lai, C.-H.; Hsueh, S.; Hong, J.-H.; Chang, T.-C.; Tseng, C.-J.; Chou, H.-H.; Huang, K.-G.; Lin, J.-D. Are adenocarcinomas and adenosquamous carcinomas different from squamous carcinomas in stage IB and II cervical cancer patients undergoing primary radical surgery? Int. J. Gynecol. Cancer 1999, 9, 28–36. [Google Scholar] [CrossRef]
- Huang, Y.-T.; Wang, C.-C.; Tsai, C.-S.; Lai, C.-H.; Chang, T.-C.; Chou, H.-H.; Hsueh, S.; Chen, C.-K.; Lee, S.P.; Hong, J.-H. Long-Term Outcome and Prognostic Factors for Adenocarcinoma/Adenosquamous Carcinoma of Cervix After Definitive Radiotherapy. Int. J. Radiat. Oncol. 2011, 80, 429–436. [Google Scholar] [CrossRef]
- Hu, K.; Wang, W.; Liu, X.; Meng, Q.; Zhang, F. Comparison of treatment outcomes between squamous cell carcinoma and adenocarcinoma of cervix after definitive radiotherapy or concurrent chemoradiotherapy. Radiat. Oncol. 2018, 13, 249. [Google Scholar] [CrossRef] [Green Version]
- Niibe, Y.; Kenjo, M.; Onishi, H.; Ogawa, Y.; Kazumoto, T.; Ogino, I.; Tsujino, K.; Harima, Y.; Takahashi, T.; Anbai, A.; et al. High-dose-rate Intracavitary Brachytherapy Combined with External Beam Radiotherapy for Stage IIIb Adenocarcinoma of the Uterine Cervix in Japan: A Multi-Institutional Study of Japanese Society of Therapeutic Radiology and Oncology 2006-2007 (Study of JASTRO 2006-2007). Jpn. J. Clin. Oncol. 2010, 40, 795–799. [Google Scholar] [PubMed]
- Kilic, S.; Cracchiolo, B.; Gabel, M.; Haffty, B.; Mahmoud, O. The relevance of molecular biomarkers in cervical cancer patients treated with radiotherapy. Ann. Transl. Med. 2015, 3, 261. [Google Scholar]
- Rose, P.G.; Java, J.; Whitney, C.W.; Stehman, F.B.; Lanciano, R.; Thomas, G.M.; DiSilvestro, P.A. Nomograms Predicting Progression-Free Survival, Overall Survival, and Pelvic Recurrence in Locally Advanced Cervical Cancer Developed From an Analysis of Identifiable Prognostic Factors in Patients From NRG Oncology/Gynecologic Oncology Group Randomized Trials of Chemoradiotherapy. J. Clin. Oncol. 2015, 33, 2136–2142. [Google Scholar]
- Lin, Y.-C.; Chen, R.-Y.; Liang, J.-A.; Hung, Y.-C.; Yeh, L.-S.; Chang, W.-C.; Lin, W.-C.; Chang, Y.-Y.; Chen, S.-W. Immunohistochemical Biomarkers of Survival in Patients With Adenocarcinoma of the Uterine Cervix Receiving Chemoradiotherapy. Anticancer Res. 2019, 39, 3231–3240. [Google Scholar] [CrossRef]
- Thomas, L.W.; Lam, C.; Edwards, S.W. Mcl-1; the molecular regulation of protein function. FEBS Lett. 2010, 584, 2981–2989. [Google Scholar] [CrossRef] [Green Version]
- Opferman, J.T.; Letai, A.; Beard, C.; Sorcinelli, M.D.; Ong, C.C.; Korsmeyer, S.J. Development and maintenance of B and T lymphocytes requires antiapoptotic MCL-1. Nature 2003, 426, 671–676. [Google Scholar] [CrossRef]
- Chen, L.; Willis, S.N.; Wei, A.H.; Smith, B.J.; Fletcher, J.I.; Hinds, M.G.; Colman, P.M.; Day, C.; Adams, J.M.; Huang, D.C.S. Differential Targeting of Prosurvival Bcl-2 Proteins by Their BH3-Only Ligands Allows Complementary Apoptotic Function. Mol. Cell 2005, 17, 393–403. [Google Scholar] [CrossRef] [PubMed]
- Xiang, W.; Yang, C.-Y.; Bai, L. MCL-1 inhibition in cancer treatment. OncoTargets Ther. 2018, 11, 7301–7314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishibashi, M.; Tamura, H.; Sunakawa, M.; Kondo-Onodera, A.; Okuyama, N.; Hamada, Y.; Moriya, K.; Choi, I.; Tamada, K.; Inokuchi, K. Myeloma drug resistance induced by binding of myeloma B7-H1 (PD-L1) to PD-1. Cancer Immunol. Res. 2016, 4, 779–788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nordsmark, M.; Overgaard, J. Tumor hypoxia is independent of hemoglobin and prognostic for loco-regional tumor control after primary radiotherapy in advanced head and neck cancer. Acta Oncol. 2004, 43, 396–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fancello, L.; Gandini, S.; Pelicci, P.G.; Mazzarella, L. Tumor mutational burden quantification from targeted gene panels: Major advancements and challenges. J. Immunother. Cancer 2019, 7, 183. [Google Scholar] [CrossRef] [Green Version]
- Yan, B.; Wang, H.; Rabbani, Z.N.; Zhao, Y.; Li, W.; Yuan, Y.; Li, F.; Dewhirst, M.W.; Li, C.-Y. Tumor Necrosis Factor- Is a Potent Endogenous Mutagen that Promotes Cellular Transformation. Cancer Res. 2006, 66, 11565–11570. [Google Scholar] [CrossRef] [Green Version]
- Pal, S.; Yadav, P.; Sainis, K.B.; Shankar, B.S. TNF-α and IGF-1 differentially modulate ionizing radiation responses of lung cancer cell lines. Cytokine 2018, 101, 89–98. [Google Scholar] [CrossRef]
- Bermúdez, A.; Bhatla, N.; Leung, E. Cancer of the cervix uteri. Int. J. Gynecol. Obstet. 2015, 131, S88–S95. [Google Scholar] [CrossRef] [Green Version]
- Choudhury, K.R.; Yagle, K.J.; Swanson, P.E.; Krohn, K.A.; Rajendran, J.G. A Robust Automated Measure of Average Antibody Staining in Immunohistochemistry Images. J. Histochem. Cytochem. 2009, 58, 95–107. [Google Scholar] [CrossRef] [Green Version]
- Roach, C.; Zhang, N.; Corigliano, E.; Jansson, M.; Toland, G.; Ponto, G.; Dolled-Filhart, M.; Emancipator, K.; Stanforth, D.; Kulangara, K. Development of a Companion Diagnostic PD-L1 Immunohistochemistry Assay for Pembrolizumab Therapy in Non–Small-cell Lung Cancer. Appl. Immunohistochem. Mol. Morphol. 2016, 24, 392–397. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.-W.; Shen, W.-C.; Hsieh, T.-C.; Liang, J.-A.; Hung, Y.-C.; Yeh, L.-S.; Chang, W.-C.; Lin, W.-C.; Yen, K.-Y.; Kao, C.-H. Textural features of cervical cancers on FDG-PET/CT associate with survival and local relapse in patients treated with definitive chemoradiotherapy. Sci. Rep. 2018, 8, 11859. [Google Scholar] [CrossRef] [Green Version]
- Pötter, R.; Haie-Meder, C.; Van Limbergen, E.; Barillot, I.; De Brabandere, M.; Dimopoulos, J.; Dumas, I.; Erickson, B.; Lang, S.; Nulens, A.; et al. Recommendations from gynaecological (GYN) GEC ESTRO working group (II): Concepts and terms in 3D image-based treatment planning in cervix cancer brachytherapy—3D dose volume parameters and aspects of 3D image-based anatomy, radiation physics, radiobiology. Radiother. Oncol. 2006, 78, 67–77. [Google Scholar] [CrossRef] [PubMed]
- Goldman, M.; Craft, B.; Brooks, A.; Zhu, J.; Haussler, D.J.B. The UCSC Xena Platform for cancer genomics data visualization and interpretation. BioRxiv 2018, 326470. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Kyoto Encyclopedia of Genes and Genomes Signal Pathway | Oncogenic Signaling Pathways in TCGA | Frequency of Mutated Gene in TCGA | |
|---|---|---|---|
| Category | Number (percentage) | ||
| RAS | 3/21 (14%) | KRAS 7/28 (25%) | |
| MAPK | 2/21 (10%) | ||
| ERBB | 4/21 (19%) | ERBB2 6/28 (21%) | |
| Combined RTK/RAS | 5/21 (24%) | 63% | |
| PI3K-AKT | 6/21 (29%) | PIK3CA 9/28 (32%) | |
| mTOR | 5/21 (24%) | ||
| Combined P13K | 6/21 (29%) | 56% | |
| TP53 | 6/21 (29%) | 19% | |
| Cell cycle | 3/21 (14%) | 21% | |
| TGF-beta | 3/21 (14%) | 21% | |
| WNT | 2/21 (10%) | 14% | |
| HIPPO | 2/21 (10%) | 14% | |
| NOTCH | 4/21 (19%) | 30% | |
| APOPTOSIS | 3/21 (14%) | ||
| VEGF | 3/21 (14%) | ||
| Outcome | Variable | p Value | HR | 95% CI |
|---|---|---|---|---|
| Disease-free survival | MCL1 amplification | 0.012 | 10.07 | 1.65–61.49 |
| TNF-α H-score (continuous) | 0.024 | 0.88 | 0.79–0.98 | |
| Local relapse-free survival | Tumor mutation number ≥ 6 | 0.014 | 19.27 | 1.65–225.50 |
| MCL1 amplification | 0.057 | 4.19 | 0.96–18.30 | |
| Distant metastasis-free survival | MCL1 amplification | 0.021 | 22.94 | 1.61–148.57 |
| Variables | Value |
|---|---|
| Age (year) | median 54 (range, 41–77) |
| FIGO stage | |
| IB3 | 5 (24%) |
| IIB | 8 (38%) |
| IIIB | 2 (9%) |
| IIIC1 | 6 (29%) |
| Maximum tumor dimension (cm) | mean 5.7 ± 1.1 (range, 3.9–8.0) |
| Pretreatment hemoglobulin (g/dL) | mean 10.3 ± 2.7 (range, 4.9–13.5) |
| Carcinoembryonic antigen (ng/dL) | mean 36.2 ± 29.3 (range, 0.5–331.7) |
| External beam radiotherapy (cGy) | |
| whole pelvis (Gy) | median 45 (range, 39.6–54) |
| bilateral parametrium boost with central shielding (Gy) | median 54 (range, 50.4–57.6) |
| pelvic lymph node boost (Gy) | median 64 (range, 60–66) |
| Brachytherapy | |
| 2-dimensional brachytherapy (6Gy to point A per session for 5 courses) Cumulative EQD2 of point A (Gy10) | 6 |
| mean 84.3 ± 7.3 | |
| 3-dimensional brachytherapy (HR-CTV > 6.5Gy per session for 5 courses) Cumulative EQD2 of D90 of HR-CTV (Gy10) | 15 |
| mean 88.1 ± 10.3 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, Y.-C.; Chen, Y.-C.; Chen, R.-Y.; Huang, Y.-X.; Tu, S.-J.; Liang, J.-A.; Hung, Y.-C.; Yeh, L.-S.; Chang, W.-C.; Lin, W.-C.; et al. Genomic Biomarkers of Survival in Patients with Adenocarcinoma of the Uterine Cervix Receiving Chemoradiotherapy. Int. J. Mol. Sci. 2020, 21, 4117. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21114117
Lin Y-C, Chen Y-C, Chen R-Y, Huang Y-X, Tu S-J, Liang J-A, Hung Y-C, Yeh L-S, Chang W-C, Lin W-C, et al. Genomic Biomarkers of Survival in Patients with Adenocarcinoma of the Uterine Cervix Receiving Chemoradiotherapy. International Journal of Molecular Sciences. 2020; 21(11):4117. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21114117
Chicago/Turabian StyleLin, Ying-Chun, Yu-Chia Chen, Rui-Yun Chen, Yi-Xuan Huang, Siang-Jyun Tu, Ji-An Liang, Yao-Ching Hung, Lian-Shung Yeh, Wei-Chun Chang, Wu-Chou Lin, and et al. 2020. "Genomic Biomarkers of Survival in Patients with Adenocarcinoma of the Uterine Cervix Receiving Chemoradiotherapy" International Journal of Molecular Sciences 21, no. 11: 4117. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21114117