EP3 Is an Independent Prognostic Marker Only for Unifocal Breast Cancer Cases

 , ,
, ,
Abstract
:1. Introduction
2. Results
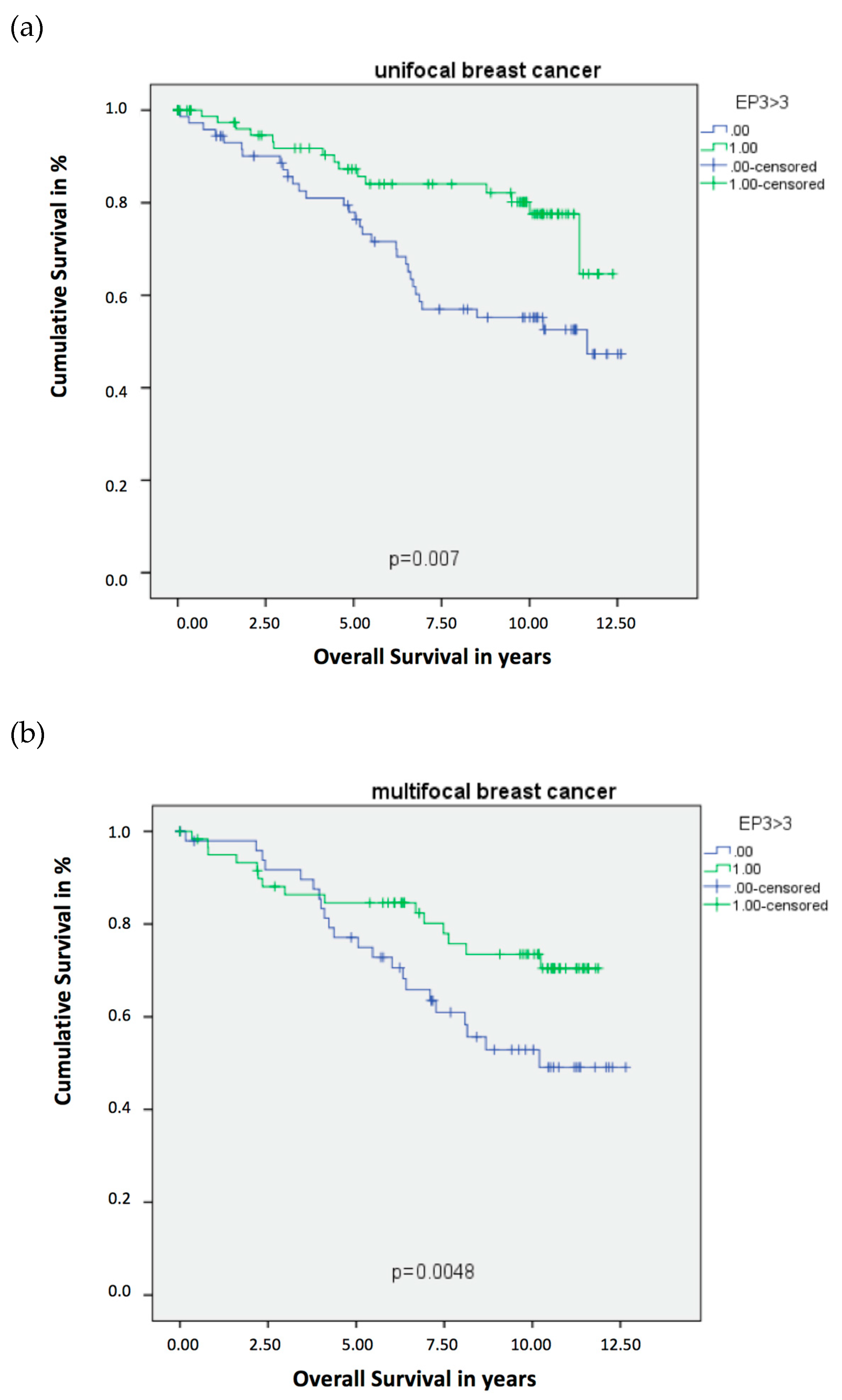
2.1. Unifocal BC
2.2. Multifocal and Multicentric BC
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Ethics Approval and Consent to Participate
4.3. Immunohistochemistry
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| BC | Breast Cancer |
| EP1–4 | Prostaglandin receptor E2 1–4 |
| ER | Estrogen receptor |
| COX | Cyclooxygenase |
| HER2 | Human epidermal growth factor receptor 2 |
| IRS | immune-reactive score of Remmele and Stegner |
| OS | Overall Survival |
| PG | Prostaglandin |
| PR | Progesteronreceptor |
| LD | linear dichroism |
| UICC | union of international cancer control |
| VDR | Vitamin-D receptor |
| VEGF-C | Vascular endothelial growth factor C |
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jemal, A.; Bray, F.; Center, M.M.; Ferlay, J.; Ward, E.; Forman, D. Global cancer statistics. CA Cancer J. Clin. 2011, 61, 69–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harbeck, N.; Gnant, M. Breast cancer. Lancet 2017, 389, 1134–1150. [Google Scholar] [CrossRef]
- Narumiya, S.; Sugimoto, Y.; Ushikubi, F. Prostanoid receptors: Structures, properties, and functions. Physiol. Rev. 1999, 79, 1193–1226. [Google Scholar] [CrossRef]
- Gomes, R.N.; Felipe da Costa, S.; Colquhoun, A. Eicosanoids and cancer. Clinics 2018, 73 (Suppl. 1), e530s. [Google Scholar] [CrossRef]
- Reader, J.; Holt, D.; Fulton, A. Prostaglandin E2 EP receptors as therapeutic targets in breast cancer. Cancer Metastasis Rev. 2011, 30, 449–463. [Google Scholar] [CrossRef] [Green Version]
- Ma, J.; Chen, M.; Xia, S.K.; Shu, W.; Guo, Y.; Wang, Y.H.; Xu, Y.; Bai, X.M.; Zhang, L.; Zhang, H.; et al. Prostaglandin E2 promotes liver cancer cell growth by the upregulation of FUSE-binding protein 1 expression. Int. J. Oncol. 2013, 42, 1093–1104. [Google Scholar] [CrossRef] [Green Version]
- Hester, A.; Salzmann, B.; Rahmeh, M.; Kolben, T.; Czogalla, B.; Ditsch, N.; Mahner, S.; Jeschke, U.; Kolben, T.M. EP3 receptor antagonist L798,106 reduces proliferation and migration of SK-BR-3 breast cancer cells. Onco. Targets Ther. 2019, 12, 6053–6068. [Google Scholar] [CrossRef] [Green Version]
- Chang, S.H.; Ai, Y.; Breyer, R.M.; Lane, T.F.; Hla, T. The prostaglandin E2 receptor EP2 is required for cyclooxygenase 2-mediated mammary hyperplasia. Cancer Res. 2005, 65, 4496–4499. [Google Scholar] [CrossRef] [Green Version]
- Chang, S.H.; Liu, C.H.; Conway, R.; Han, D.K.; Nithipatikom, K.; Trifan, O.C.; Lane, T.F.; Hla, T. Role of prostaglandin E2-dependent angiogenic switch in cyclooxygenase 2-induced breast cancer progression. Proc. Natl. Acad. Sci. USA 2004, 101, 591–596. [Google Scholar] [CrossRef] [Green Version]
- Chang, S.H.; Liu, C.H.; Wu, M.T.; Hla, T. Regulation of vascular endothelial cell growth factor expression in mouse mammary tumor cells by the EP2 subtype of the prostaglandin E2 receptor. Prostaglandins Other Lipid Mediat. 2005, 76, 48–58. [Google Scholar] [CrossRef] [PubMed]
- Kundu, N.; Ma, X.; Kochel, T.; Goloubeva, O.; Staats, P.; Thompson, K.; Martin, S.; Reader, J.; Take, Y.; Collin, P.; et al. Prostaglandin E receptor EP4 is a therapeutic target in breast cancer cells with stem-like properties. Breast Cancer Res. Treat. 2014, 143, 19–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Majumder, M.; Xin, X.; Liu, L.; Tutunea-Fatan, E.; Rodriguez-Torres, M.; Vincent, K.; Postovit, L.M.; Hess, D.; Lala, P.K. COX-2 Induces Breast Cancer Stem Cells via EP4/PI3K/AKT/NOTCH/WNT Axis. Stem Cells 2016, 34, 2290–2305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tian, M.; Schiemann, W.P. PGE2 receptor EP2 mediates the antagonistic effect of COX-2 on TGF-beta signaling during mammary tumorigenesis. FASEB J. 2010, 24, 1105–1116. [Google Scholar] [CrossRef] [Green Version]
- Semmlinger, A.; von Schoenfeldt, V.; Wolf, V.; Meuter, A.; Kolben, T.M.; Kolben, T.; Zeder-Goess, C.; Weis, F.; Gallwas, J.; Wuerstlein, R.; et al. EP3 (prostaglandin E2 receptor 3) expression is a prognostic factor for progression-free and overall survival in sporadic breast cancer. BMC Cancer 2018, 18, 431. [Google Scholar] [CrossRef] [Green Version]
- Czogalla, B.; Kuhn, C.; Heublein, S.; Schmockel, E.; Mayr, D.; Kolben, T.; Trillsch, F.; Burges, A.; Mahner, S.; Jeschke, U.; et al. EP3 receptor is a prognostic factor in TA-MUC1-negative ovarian cancer. J. Cancer Res. Clin. Oncol. 2019, 145, 2519–2527. [Google Scholar] [CrossRef]
- Hester, A.; Ritzer, M.; Kuhn, C.; Schmoeckel, E.; Mayr, D.; Kolben, T.; Dannecker, C.; Mahner, S.; Jeschke, U.; Kolben, T.M. The role of EP3-receptor expression in cervical dysplasia. J. Cancer Res. Clin. Oncol. 2019, 145, 313–319. [Google Scholar] [CrossRef]
- Weissenbacher, T.M.; Zschage, M.; Janni, W.; Jeschke, U.; Dimpfl, T.; Mayr, D.; Rack, B.; Schindlbeck, C.; Friese, K.; Dian, D. Multicentric and multifocal versus unifocal breast cancer: Is the tumor-node-metastasis classification justified? Breast Cancer Res. Treat. 2010, 122, 27–34. [Google Scholar] [CrossRef] [Green Version]
- Lang, Z.; Wu, Y.; Li, C.; Li, X.; Wang, X.; Qu, G. Multifocal and Multicentric Breast Carcinoma: A Significantly More Aggressive Tumor than Unifocal Breast Cancer. Anticancer Res. 2017, 37, 4593–4598. [Google Scholar]
- Boros, M.; Voidazan, S.; Moldovan, C.; Georgescu, R.; Toganel, C.; Moncea, D.; Molnar, C.V.; Podoleanu, C.; Eniu, A.; Stolnicu, S. Clinical implications of multifocality as a prognostic factor in breast carcinoma—A multivariate analysis study comprising 460 cases. Int. J. Clin. Exp. Med. 2015, 8, 9839–9846. [Google Scholar]
- Sicking, I.; Rommens, K.; Battista, M.J.; Bohm, D.; Gebhard, S.; Lebrecht, A.; Cotarelo, C.; Hoffmann, G.; Hengstler, J.G.; Schmidt, M. Prognostic influence of cyclooxygenase-2 protein and mRNA expression in node-negative breast cancer patients. BMC Cancer 2014, 14, 952. [Google Scholar] [CrossRef] [Green Version]
- Coussens, L.M.; Werb, Z. Inflammation and cancer. Nature 2002, 420, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Ristimaki, A.; Sivula, A.; Lundin, J.; Lundin, M.; Salminen, T.; Haglund, C.; Joensuu, H.; Isola, J. Prognostic significance of elevated cyclooxygenase-2 expression in breast cancer. Cancer Res. 2002, 62, 632–635. [Google Scholar] [PubMed]
- Howe, L.R. Inflammation and breast cancer. Cyclooxygenase/prostaglandin signaling and breast cancer. Breast Cancer Res. 2007, 9, 210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, R.E.; Beebe-Donk, J.; Alshafie, G.A. Reduction in the risk of human breast cancer by selective cyclooxygenase-2 (COX-2) inhibitors. BMC Cancer 2006, 6, 27. [Google Scholar] [CrossRef] [PubMed]
- Serra, F.; Lapidari, P.; Quaquarini, E.; Tagliaferri, B.; Sottotetti, F.; Palumbo, R. Palbociclib in metastatic breast cancer: Current evidence and real-life data. Drugs Context 2019, 8, 212579. [Google Scholar] [CrossRef] [Green Version]
- Filipenko, I.; Schwalm, S.; Reali, L.; Pfeilschifter, J.; Fabbro, D.; Huwiler, A.; Zangemeister-Wittke, U. Upregulation of the S1P3 receptor in metastatic breast cancer cells increases migration and invasion by induction of PGE2 and EP2/EP4 activation. Biochim. Biophys. Acta 2016, 1861, 1840–1851. [Google Scholar] [CrossRef] [Green Version]
- Greenhough, A.; Smartt, H.J.; Moore, A.E.; Roberts, H.R.; Williams, A.C.; Paraskeva, C.; Kaidi, A. The COX-2/PGE2 pathway: Key roles in the hallmarks of cancer and adaptation to the tumour microenvironment. Carcinogenesis 2009, 30, 377–386. [Google Scholar] [CrossRef] [Green Version]
- Richards, J.A.; Brueggemeier, R.W. Prostaglandin E2 regulates aromatase activity and expression in human adipose stromal cells via two distinct receptor subtypes. J. Clin. Endocrinol. Metab. 2003, 88, 2810–2816. [Google Scholar] [CrossRef] [Green Version]
- Timoshenko, A.V.; Chakraborty, C.; Wagner, G.F.; Lala, P.K. COX-2-mediated stimulation of the lymphangiogenic factor VEGF-C in human breast cancer. Br. J. Cancer 2006, 94, 1154–1163. [Google Scholar] [CrossRef]
- Ma, X.; Kundu, N.; Ioffe, O.B.; Goloubeva, O.; Konger, R.; Baquet, C.; Gimotty, P.; Reader, J.; Fulton, A.M. Prostaglandin E receptor EP1 suppresses breast cancer metastasis and is linked to survival differences and cancer disparities. Mol. Cancer Res. 2010, 8, 1310–1318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thorat, M.A.; Morimiya, A.; Mehrotra, S.; Konger, R.; Badve, S.S. Prostanoid receptor EP1 expression in breast cancer. Mod. Pathol. 2008, 21, 15–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blindt, R.; Bosserhoff, A.K.; vom Dahl, J.; Hanrath, P.; Schror, K.; Hohlfeld, T.; Meyer-Kirchrath, J. Activation of IP and EP(3) receptors alters cAMP-dependent cell migration. Eur. J. Pharmacol. 2002, 444, 31–37. [Google Scholar] [CrossRef]
- Zati Zehni, A.; Jacob, S.N.; Mumm, J.N.; Heidegger, H.H.; Ditsch, N.; Mahner, S.; Jeschke, U.; Vilsmaier, T. Hormone Receptor Expression in Multicentric/Multifocal versus Unifocal Breast Cancer: Especially the VDR Determines the Outcome Related to Focality. Int. J. Mol. Sci. 2019, 20, 5740. [Google Scholar] [CrossRef] [Green Version]
- Elston, C.W.; Ellis, I.O. Pathological prognostic factors in breast cancer. I. The value of histological grade in breast cancer: Experience from a large study with long-term follow-up. Histopathology 1991, 19, 403–410. [Google Scholar] [CrossRef]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef]
- Kashif, M.; Ishfaq, M.; Nagi, A.H. Expression of Prostanoid EP3 Receptors in Oral Squamous Epithelium and Oral Squamous Cell Carcinoma. Patholog. Res. Int. 2015, 2015, 602929. [Google Scholar] [CrossRef]
- Remmele, W.; Stegner, H.E. Recommendation for uniform definition of an immunoreactive score (IRS) for immunohistochemical estrogen receptor detection (ER-ICA) in breast cancer tissue. Pathologe 1987, 8, 138–140. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| EP3 | Unifocal | Multifocal |
|---|---|---|
| Overall survival | ● + | ● + |
| Disease-free survival | ||
| Grading | ● + | |
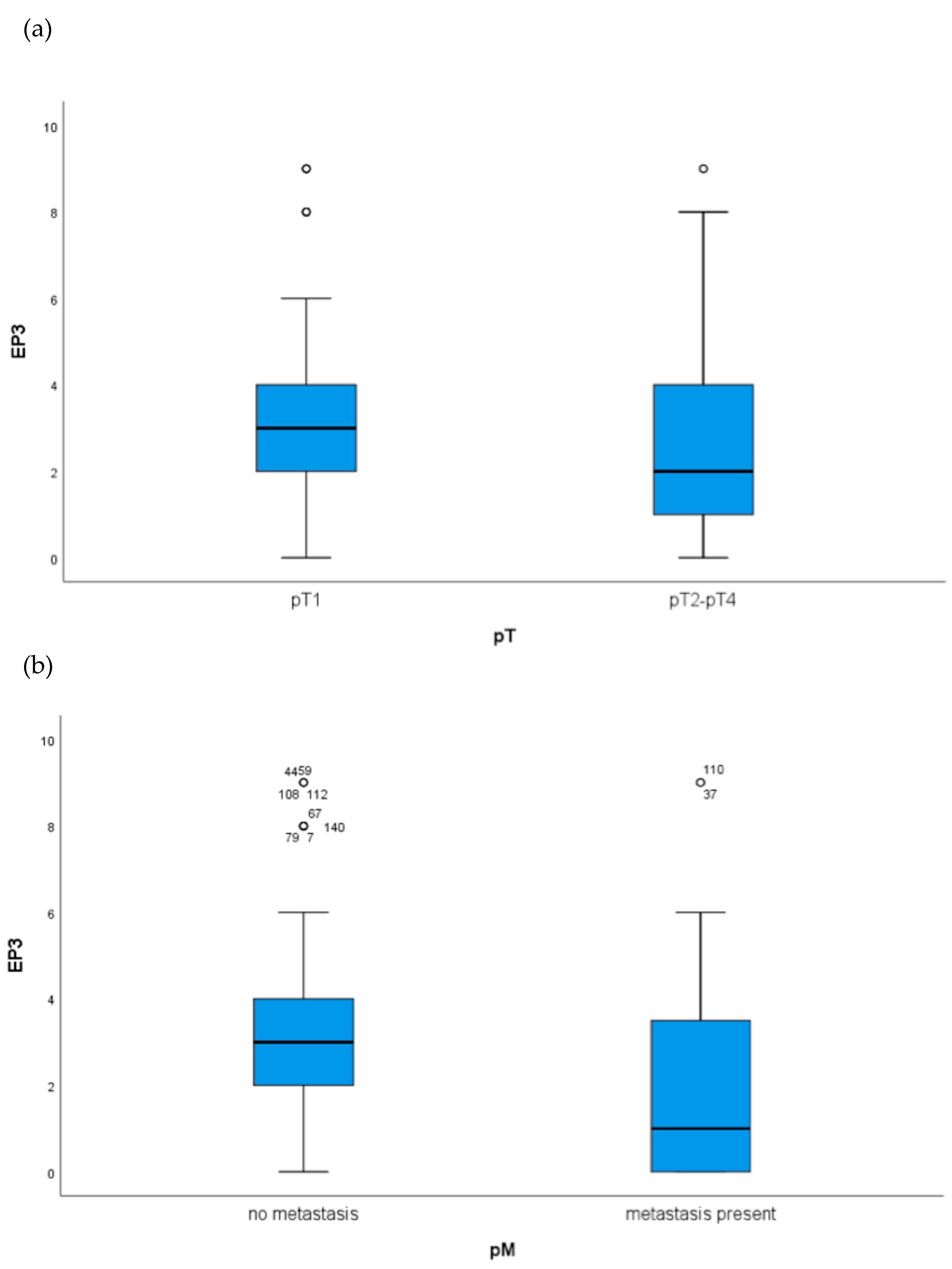
| pT | ● + | |
| pN | ||
| pM | ● + |
| Variable | Coefficient | HR (95%CI) | p-Value |
|---|---|---|---|
| Age | 0.028 | 1.028 (0.997–1.061) | 0.079 |
| Grading | 1.358 | 3.889 (1.899–7.964) | 0.000 |
| pT | 0.297 | 1.346 (1.005–1.8804) | 0.046 |
| pN | 0.644 | 1.904 (1.225–2.960) | 0.004 |
| pM | −1.190 | 0.304 (0.049–1.883) | 0.201 |
| EP3 | −1.403 | 0.246 (0.100–0.603) | 0.002 |
| VDR | 0.066 | 1.068 (0.912–1.251) | 0.417 |
| ER | −0.861 | 0.423 (0.151–1.184) | 0.101 |
| PR | −0.533 | 0.587 (0.231–1.489) | 0.262 |
| Variable | Coefficient | HR (95%CI) | p-Value |
|---|---|---|---|
| Age | 0.031 | 1.032 (1.007–1.057) | 0.012 |
| Grading | 0.002 | 1.002 (0.995–1.008) | 0.591 |
| pT | 0.289 | 1.335 (1.030–1.730) | 0.029 |
| pN | 0.320 | 1.377 (1.087–1.743) | 0.008 |
| pM | −0.306 | 0.737 (0.585–0.928) | 0.009 |
| EP3 | −0.76 | 0.927 (0.498–1.724) | 0.810 |
| VDR | 0.100 | 1.105 (0.940–1.299) | 0.226 |
| ER | −1.227 | 0.293 (0.98–0.874) | 0.028 |
| PR | −0.869 | 0.419(0.173–1.017) | 0.055 |
| Patient Characteristics | n (%) |
|---|---|
| Age (years) | Mean 59.9 Standard deviation 13.06 |
| Tumor foci | Unifocal 151 (52.2) Multifocal 138 (47.8) |
| Histology | NST 144 (49.8) Non-NST 145 (50.2) |
| Tumor grade | G1 or G2 107 (70.9) G3 44 (29.1) |
| pT | pT1 193 (66.8) pT2-pT4 96 (33.2) |
| pN | pN0 165 (57.5) pN1-pN3 122 (42.5) |
| EP3 + | Unifocal 101 (51.8) Multifocal 94 (48.2) |
| EP3 − | Unifocal 50 (53.2) Multifocal 44 (64.8) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zati Zehni, A.; Jeschke, U.; Hester, A.; Kolben, T.; Ditsch, N.; Jacob, S.-N.; Mumm, J.-N.; Heidegger, H.H.; Mahner, S.; Vilsmaier, T. EP3 Is an Independent Prognostic Marker Only for Unifocal Breast Cancer Cases. Int. J. Mol. Sci. 2020, 21, 4418. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21124418
Zati Zehni A, Jeschke U, Hester A, Kolben T, Ditsch N, Jacob S-N, Mumm J-N, Heidegger HH, Mahner S, Vilsmaier T. EP3 Is an Independent Prognostic Marker Only for Unifocal Breast Cancer Cases. International Journal of Molecular Sciences. 2020; 21(12):4418. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21124418
Chicago/Turabian StyleZati Zehni, Alaleh, Udo Jeschke, Anna Hester, Thomas Kolben, Nina Ditsch, Sven-Niclas Jacob, Jan-Niclas Mumm, Helene Hildegard Heidegger, Sven Mahner, and Theresa Vilsmaier. 2020. "EP3 Is an Independent Prognostic Marker Only for Unifocal Breast Cancer Cases" International Journal of Molecular Sciences 21, no. 12: 4418. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21124418