Tomographic Task-Related Functional Near-Infrared Spectroscopy in Acute Sport-Related Concussion: An Observational Case Study

 , , , ,
, , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
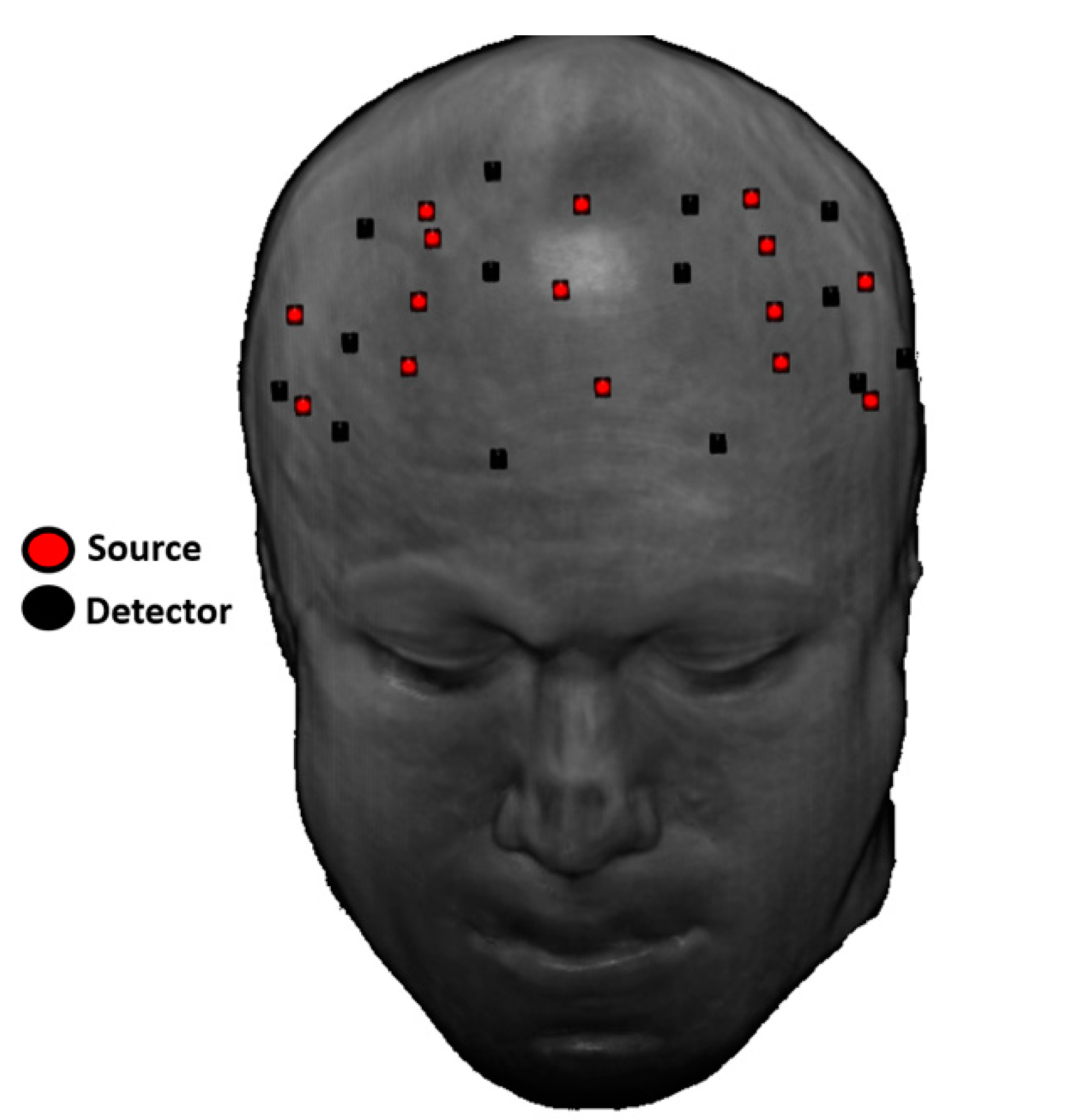
2.1. Co-Registration
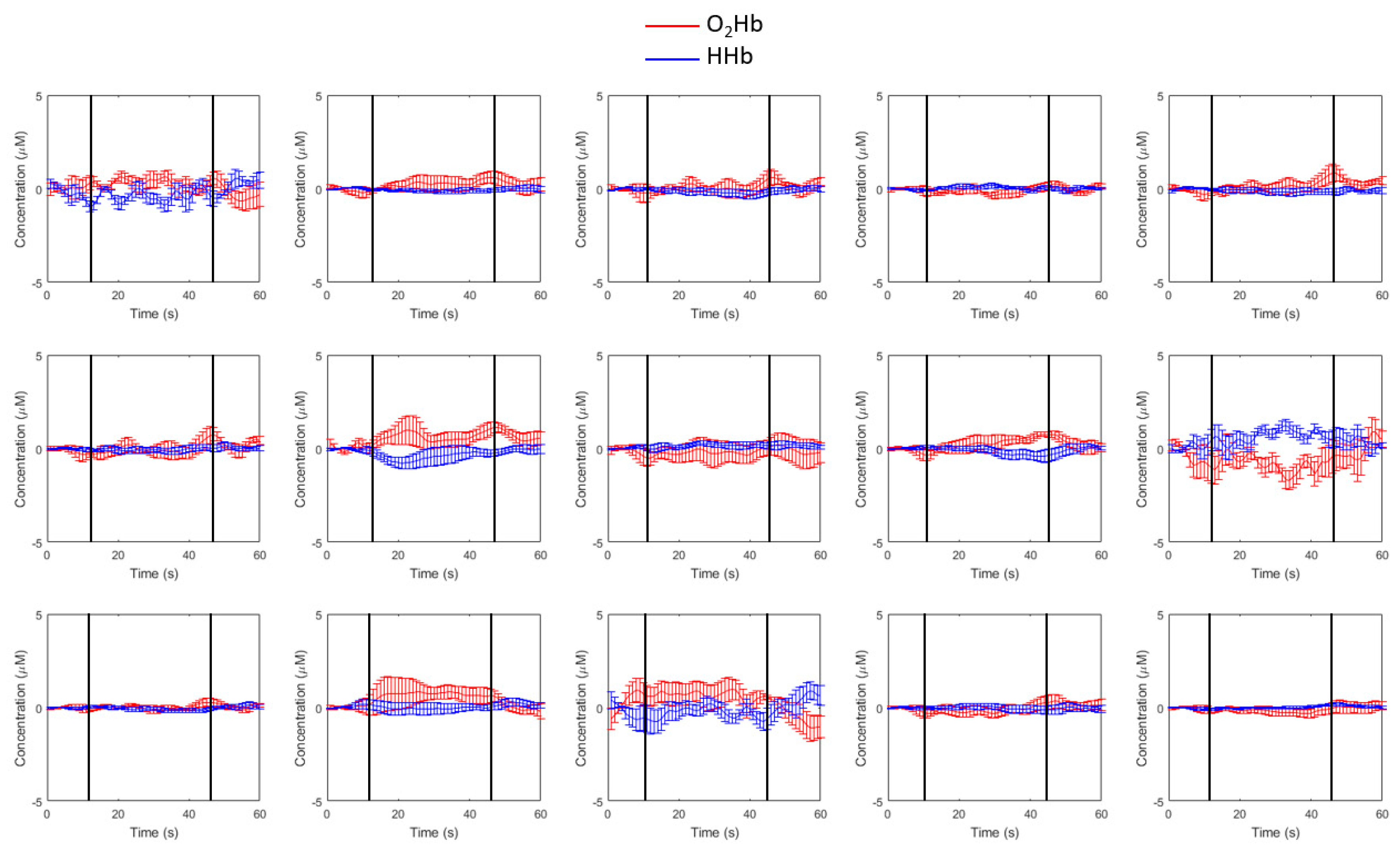
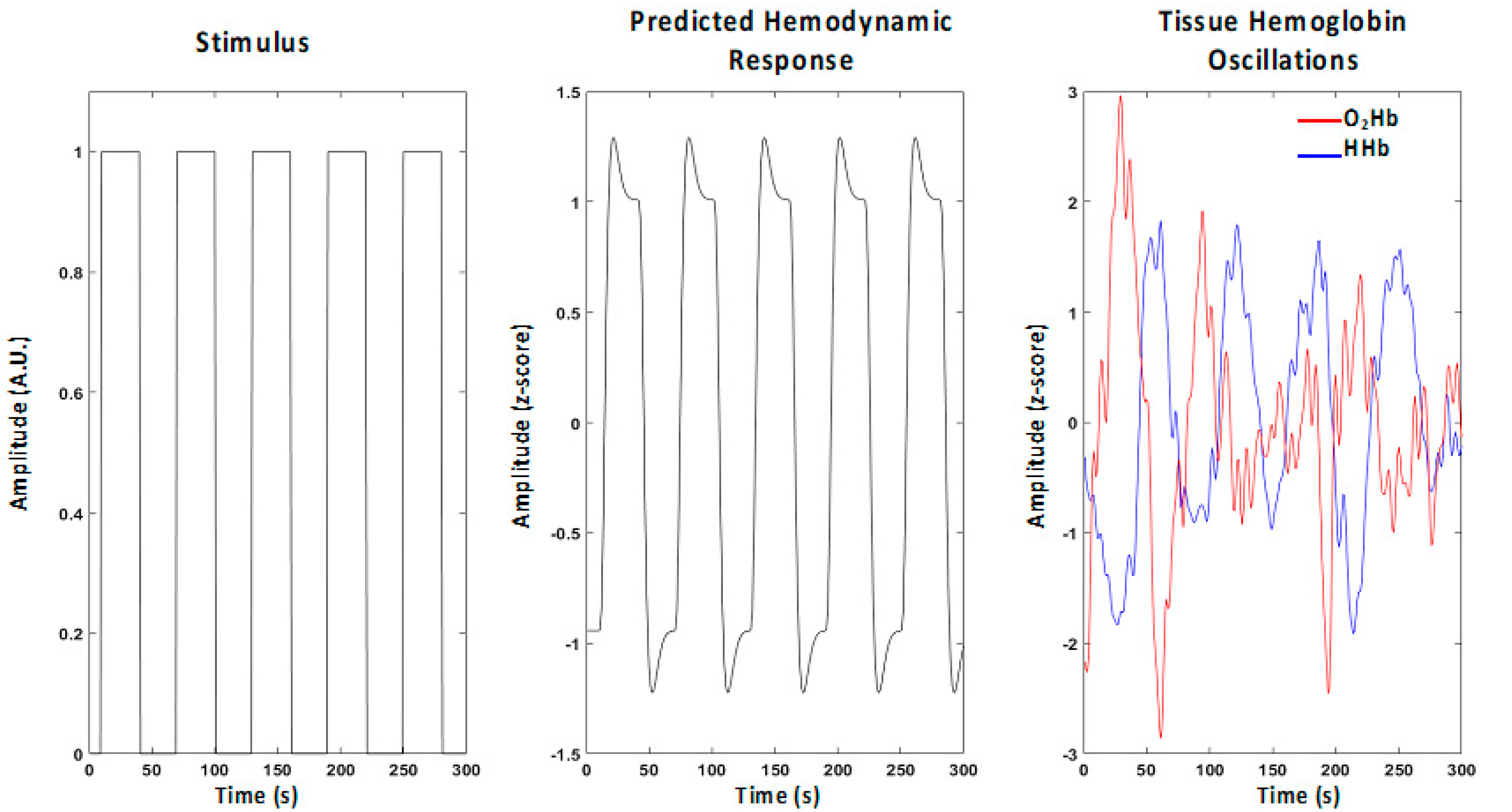
2.2. Oscillations of Oxyhemoglobin and Deoxyhemoglobin Levels
2.3. Statistical Models Used for Single-Subject Optical Tomographic Reconstruction of the Brain Activation Pattern
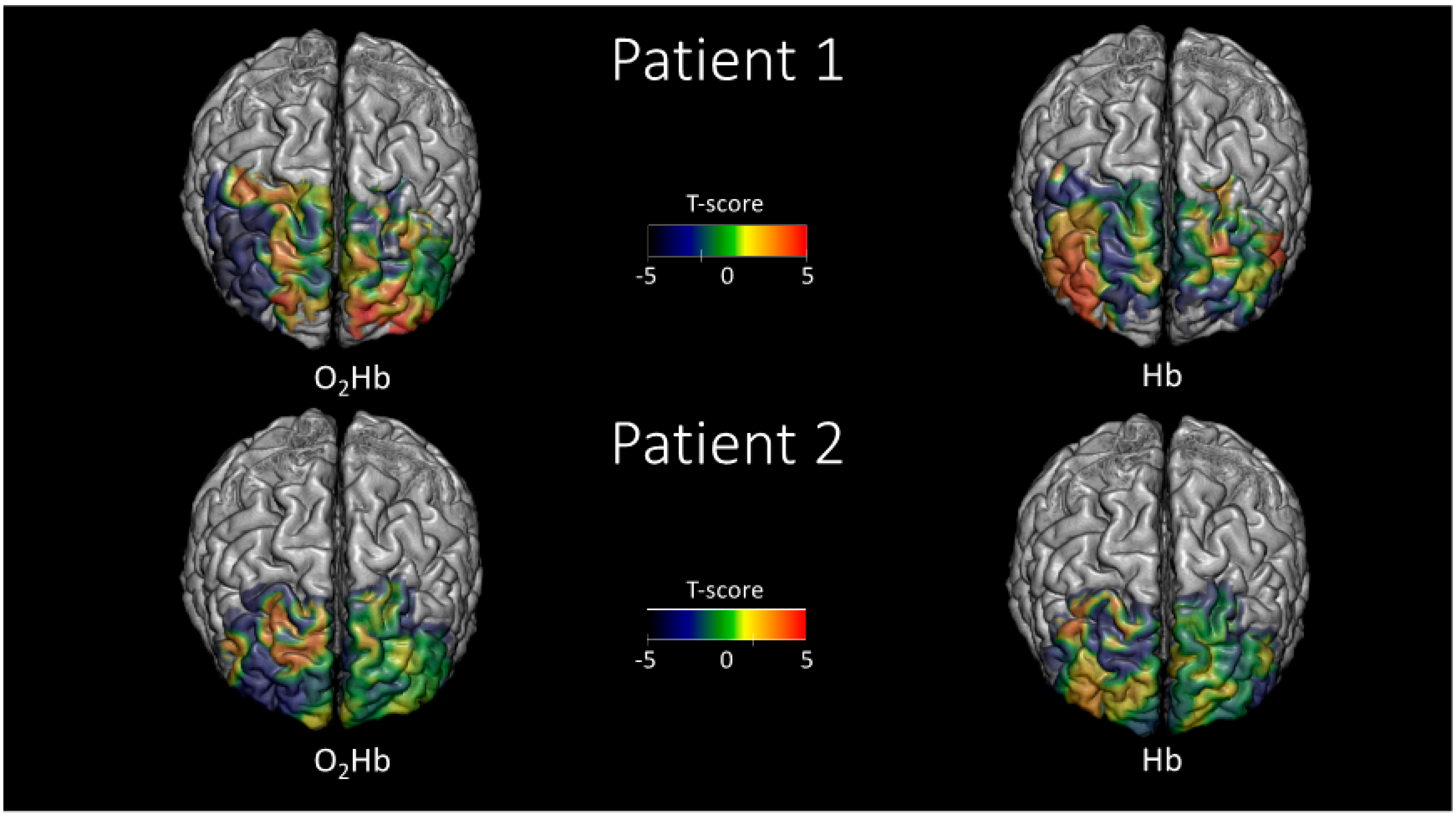
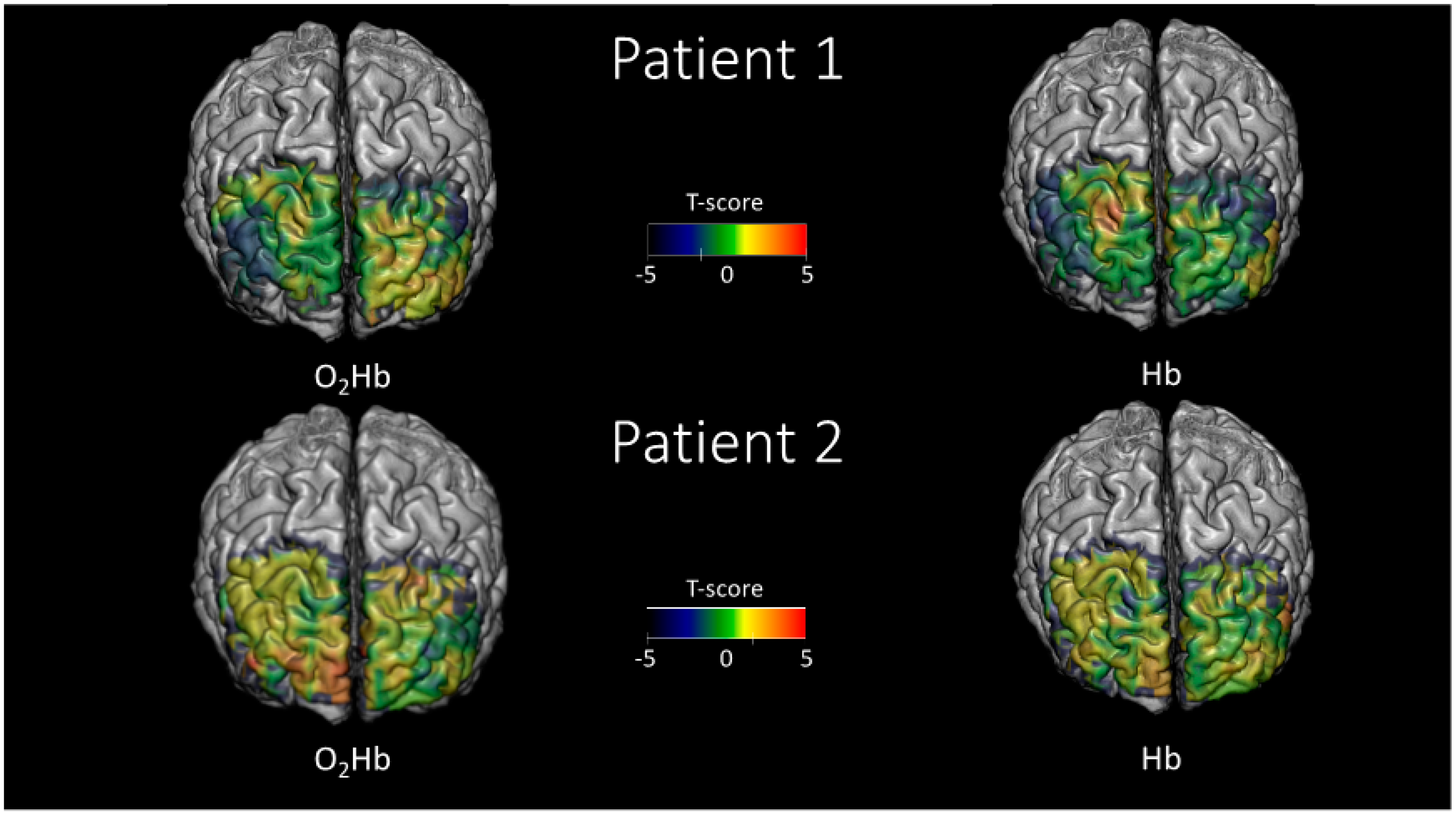
2.4. Brain Activation Patterns Measured
3. Discussion
3.1. Tomographic Task-Related Functional Near-Infrared Spectroscopy Assessment in Sport-Related Concussion within 72 Hours from Injury
3.2. Brain Activation Patterns Measured
3.2.1. Silent Word Generation
3.2.2. Digit Span
3.2.3. Symbol Search
3.3. Design of Clinical Studies for Tomographic Functional Near-Infrared Spectroscopy in Sport-Related Concussion
3.4. Limitations
3.4.1. Sample Size
3.4.2. Confinement of the Results to the Illuminated Areas
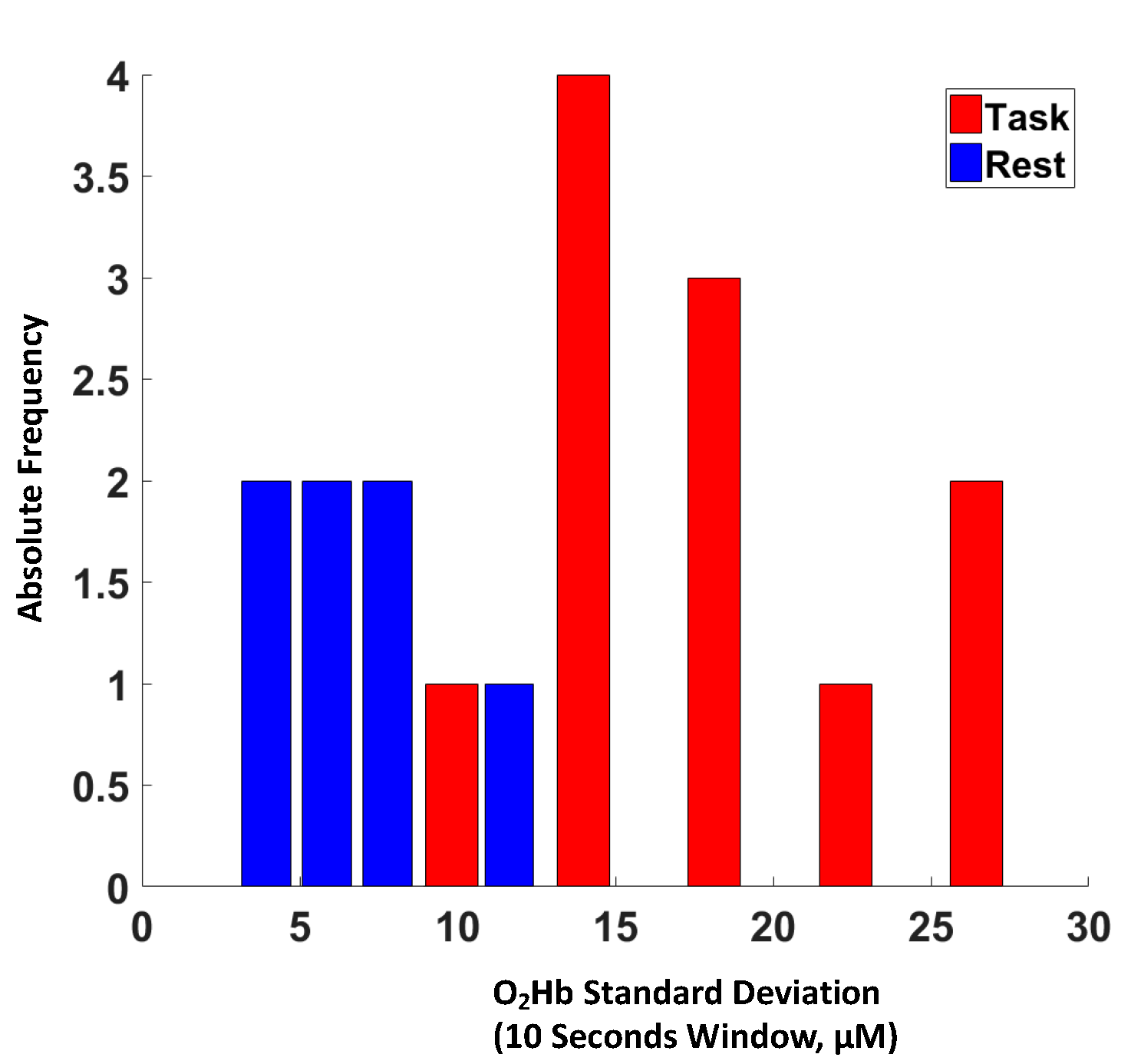
3.4.3. Limitations of the Statistical Model of the Variance of Levels of Oxyhemoglobin
3.4.4. Extracranial Tissue Interference
3.4.5. Hemodynamic Impairments in Sport-Related Concussion
3.4.6. Multiple Patterns of Brain Activation
4. Materials and Methods
4.1. Patients
4.2. Data Recording
4.2.1. Optical Helmet
4.2.2. Digitization
4.2.3. Optical Device
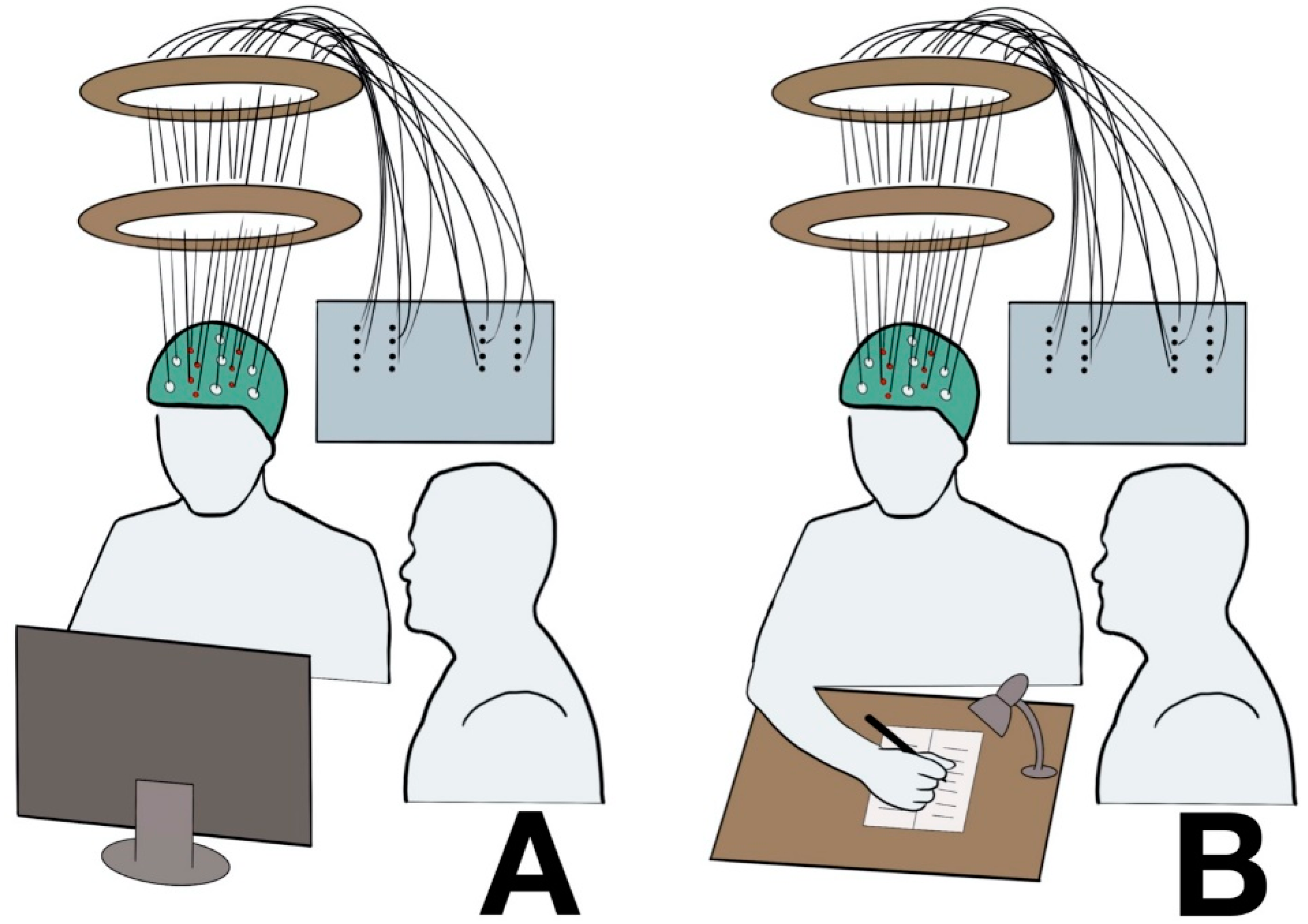
4.2.4. Testing Set-Up
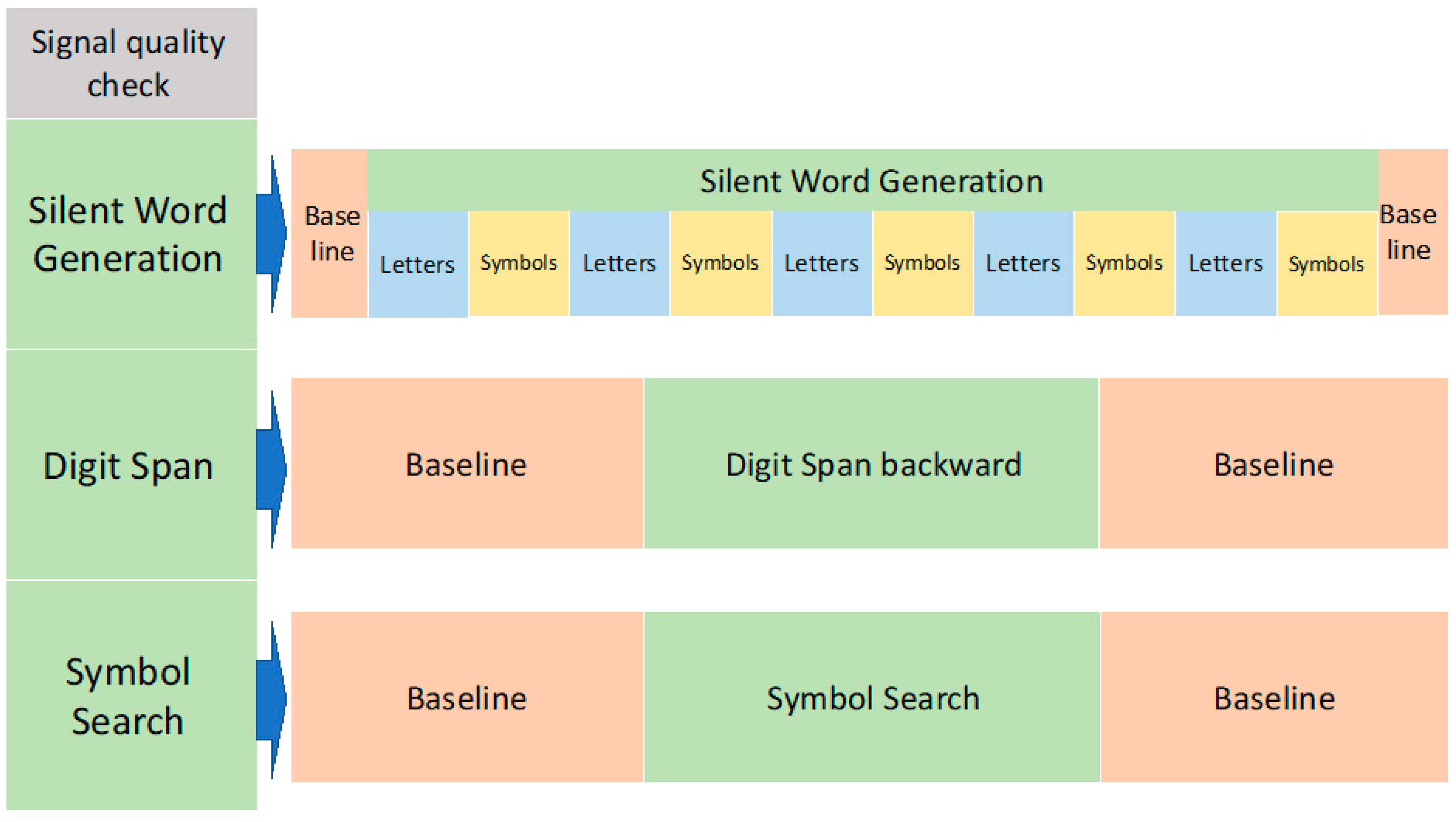
4.2.5. Data Acquisition Protocol
Silent Word Generation
Digit Span Backward
Symbol Search
4.3. Data Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| SRC | Sport-related concussion |
| TBI | Traumatic brain injury |
| MRI | Magnetic resonance imaging |
| ImPACT | Immediate Post-Concussion Assessment and Cognitive Testing |
| SCAT | Sport Concussion Assessment Tool |
| fMRI | Functional magnetic resonance imaging |
| fNIRS | Functional near-infrared spectroscopy |
| O2Hb | Oxyhemoglobin |
| HHb | Deoxyhemoglobin |
| DOT | Diffuse optical tomography |
| SWG | Silent Word Generation |
| DS | Digit Span |
| SS | Symbol Search |
| SD | Source-detector |
| μM | Micromolar |
| GLM | General Linear Model |
| LH | Left hemisphere |
| RH | Right hemisphere |
| ECT | Extracranial tissue |
| WAIS-IV | Wechsler Adult Intelligence Scales, Fourth Edition |
| DC | Direct current |
| OD | Optical density |
| FEM | Finite-element method |
References
- McCrory, P.; Meeuwisse, W.; Dvorak, J.; Aubry, M.; Bailes, J.; Broglio, S.; Cantu, R.C.; Cassidy, D.; Echemendia, R.J.; Castellani, R.J.; et al. Consensus statement on concussion in sport-the 5(th) international conference on concussion in sport held in Berlin, October 2016. Br. J. Sports Med. 2017, 51, 838–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCrory, P.; Meeuwisse, W.H.; Echemendia, R.J.; Iverson, G.L.; Dvorak, J.; Kutcher, J.S. What is the lowest threshold to make a diagnosis of concussion? Br. J. Sports Med. 2013, 47, 268–271. [Google Scholar] [CrossRef] [PubMed]
- Langlois, J.A.; Rutland-Brown, W.; Wald, M.M. The epidemiology and impact of traumatic brain injury: A brief overview. J. Head Trauma Rehabil. 2006, 21, 375–378. [Google Scholar] [CrossRef] [Green Version]
- Zuckerman, S.L.; Kerr, Z.Y.; Yengo-Kahn, A.; Wasserman, E.; Covassin, T.; Solomon, G.S. Epidemiology of Sports-Related Concussion in NCAA Athletes From 2009–2010 to 2013–2014: Incidence, Recurrence, and Mechanisms. Am. J. Sports Med. 2015, 43, 2654–2662. [Google Scholar] [CrossRef] [PubMed]
- McCrea, M.; Hammeke, T.; Olsen, G.; Leo, P.; Guskiewicz, K. Unreported concussion in high school football players: Implications for prevention. Clin. J. Sport Med. 2004, 14, 13–17. [Google Scholar] [CrossRef]
- Lovell, M.R.; Collins, M.W.; Maroon, J.C.; Cantu, R.; Hawn, M.A.; Burke, C.J.; Fu, F. INACCURACY OF SYMPTOM REPORTING FOLLOWING CONCUSSION IN ATHLETES. Med. Sci. Sports Exerc. 2002, 34, S298. [Google Scholar] [CrossRef]
- Vagnozzi, R.; Tavazzi, B.; Signoretti, S.; Amorini, A.M.; Belli, A.; Cimatti, M.; Delfini, R.; Di Pietro, V.; Finocchiaro, A.; Lazzarino, G. Temporal window of metabolic brain vulnerability to concussions: Mitochondrial-related impairment—part I. Neurosurgery 2007, 61, 379–388, discussion 388–389. [Google Scholar] [CrossRef] [Green Version]
- Tavazzi, B.; Vagnozzi, R.; Signoretti, S.; Amorini, A.M.; Belli, A.; Cimatti, M.; Delfini, R.; Di Pietro, V.; Finocchiaro, A.; Lazzarino, G. Temporal window of metabolic brain vulnerability to concussions: Oxidative and nitrosative stresses—part II. Neurosurgery 2007, 61, 390–395, discussion 395–396. [Google Scholar] [CrossRef] [Green Version]
- Longhi, L.; Saatman, K.E.; Fujimoto, S.; Raghupathi, R.; Meaney, D.F.; Davis, J.; McMillan, B.S.A.; Conte, V.; Laurer, H.L.; Stein, S.; et al. Temporal window of vulnerability to repetitive experimental concussive brain injury. Neurosurgery 2005, 56, 364–374, discussion 364–374. [Google Scholar] [CrossRef] [Green Version]
- Guskiewicz, K.M.; McCrea, M.; Marshall, S.W.; Cantu, R.C.; Randolph, C.; Barr, W.; Onate, J.A.; Kelly, J.P. Cumulative effects associated with recurrent concussion in collegiate football players: The NCAA Concussion Study. JAMA 2003, 290, 2549–2555. [Google Scholar] [CrossRef] [Green Version]
- Cross, M.; Kemp, S.; Smith, A.; Trewartha, G.; Stokes, K. Professional Rugby Union players have a 60% greater risk of time loss injury after concussion: A 2-season prospective study of clinical outcomes. Br. J. Sports Med. 2016, 50, 926–931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nordstrom, A.; Nordstrom, P.; Ekstrand, J. Sports-related concussion increases the risk of subsequent injury by about 50% in elite male football players. Br. J. Sports Med. 2014, 48, 1447–1450. [Google Scholar] [CrossRef] [PubMed]
- McCrea, M.; Guskiewicz, K.; Randolph, C.; Barr, W.B.; Hammeke, T.A.; Marshall, S.W.; Kelly, J.P. Effects of a symptom-free waiting period on clinical outcome and risk of reinjury after sport-related concussion. Neurosurgery 2009, 65, 876–882, discussion 882–883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Echemendia, R.J.; Giza, C.C.; Kutcher, J.S. Developing guidelines for return to play: Consensus and evidence-based approaches. Brain Inj. 2015, 29, 185–194. [Google Scholar] [CrossRef] [PubMed]
- Echemendia, R.J.; Putukian, M.; Mackin, R.S.; Julian, L.; Shoss, N. Neuropsychological test performance prior to and following sports-related mild traumatic brain injury. Clin. J. Sport Med. 2001, 11, 23–31. [Google Scholar] [CrossRef]
- Lovell, M.R.; Collins, M.W.; Iverson, G.L.; Field, M.; Maroon, J.C.; Cantu, R.; Podell, K.; Powell, J.W.; Belza, M.; Fu, F.H. Recovery from mild concussion in high school athletes. J. Neurosurg. 2003, 98, 296–301. [Google Scholar] [CrossRef]
- Broglio, S.P.; Macciocchi, S.N.; Ferrara, M.S. Neurocognitive performance of concussed athletes when symptom free. J. Athl. Train. 2007, 42, 504–508. [Google Scholar]
- Van Kampen, D.A.; Lovell, M.R.; Pardini, J.E.; Collins, M.W.; Fu, F.H. The “value added” of neurocognitive testing after sports-related concussion. Am. J. Sports Med. 2006, 34, 1630–1635. [Google Scholar] [CrossRef]
- Slobounov, S.; Tutwiler, R.; Sebastianelli, W.; Slobounov, E. Alteration of postural responses to visual field motion in mild traumatic brain injury. Neurosurgery 2006, 59, 134–139, discussion 134–139. [Google Scholar] [CrossRef]
- Slobounov, S.; Slobounov, E.; Sebastianelli, W.; Cao, C.; Newell, K. Differential rate of recovery in athletes after first and second concussion episodes. Neurosurgery 2007, 61, 338–344, discussion 344. [Google Scholar] [CrossRef]
- Vagnozzi, R.; Signoretti, S.; Cristofori, L.; Alessandrini, F.; Floris, R.; Isgro, E.; Ria, A.; Marziali, S.; Zoccatelli, G.; Tavazzi, B.; et al. Assessment of metabolic brain damage and recovery following mild traumatic brain injury: A multicentre, proton magnetic resonance spectroscopic study in concussed patients. Brain 2010, 133, 3232–3242. [Google Scholar] [CrossRef] [PubMed]
- Lumba-Brown, A.; Ghajar, J.; Cornwell, J.; Bloom, O.J.; Chesnutt, J.; Clugston, J.R.; Kolluri, R.; Leddy, J.J.; Teramoto, M.; Gioia, G. Representation of concussion subtypes in common postconcussion symptom-rating scales. Concussion 2019, 4, CNC65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Echemendia, R.J.; Broglio, S.P.; Davis, G.A.; Guskiewicz, K.M.; Hayden, K.A.; Leddy, J.J.; Meehan, W.P., III; Putukian, M.; Sullivan, S.J.; Schneider, K.J.; et al. What tests and measures should be added to the SCAT3 and related tests to improve their reliability, sensitivity and/or specificity in sideline concussion diagnosis? A systematic review. Br. J. Sports Med. 2017, 51, 895–901. [Google Scholar] [CrossRef] [PubMed]
- Forcione, M.; Colonnese, C.; Belli, A. Cerebral Hemodynamic Influences in Task-Related Functional Magnetic Resonance Imaging and Near-Infrared Spectroscopy in Acute Sport-Related Concussion: A Review. J. Imaging 2018, 4, 59. [Google Scholar] [CrossRef] [Green Version]
- Eklund, A.; Nichols, T.E.; Knutsson, H. Cluster failure: Why fMRI inferences for spatial extent have inflated false-positive rates. Proc. Natl. Acad. Sci. USA 2016, 113, 7900–7905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iyengar, S. Case for fMRI data repositories. Proc. Natl. Acad. Sci. USA 2016, 113, 7699–7700. [Google Scholar] [CrossRef] [Green Version]
- Scholkmann, F.; Kleiser, S.; Metz, A.J.; Zimmermann, R.; Mata Pavia, J.; Wolf, U.; Wolf, M. A review on continuous wave functional near-infrared spectroscopy and imaging instrumentation and methodology. Neuroimage 2014, 85 Pt 1, 6–27. [Google Scholar] [CrossRef]
- Croce, P.; Zappasodi, F.; Merla, A.; Chiarelli, A.M. Exploiting neurovascular coupling: A Bayesian sequential Monte Carlo approach applied to simulated EEG fNIRS data. J. Neural Eng. 2017, 14, 046029. [Google Scholar] [CrossRef]
- Boas, D.A.; Brooks, D.H.; Miller, E.L.; DiMarzio, C.A.; Kilmer, M.; Gaudette, R.J.; Quan, Z. Imaging the body with diffuse optical tomography. IEEE Signal Process. Mag. 2001, 18, 57–75. [Google Scholar] [CrossRef]
- Chiarelli, A.M.; Maclin, E.L.; Low, K.A.; Mathewson, K.E.; Fabiani, M.; Gratton, G. Combining energy and Laplacian regularization to accurately retrieve the depth of brain activity of diffuse optical tomographic data. J. Biomed. Opt. 2016, 21, 36008. [Google Scholar] [CrossRef] [Green Version]
- Wheelock, M.D.; Culver, J.P.; Eggebrecht, A.T. High-density diffuse optical tomography for imaging human brain function. Rev. Sci. Instrum. 2019, 90, 051101. [Google Scholar] [CrossRef] [PubMed]
- Cui, X.; Bray, S.; Bryant, D.M.; Glover, G.H.; Reiss, A.L. A quantitative comparison of NIRS and fMRI across multiple cognitive tasks. Neuroimage 2011, 54, 2808–2821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amyot, F.; Zimmermann, T.; Riley, J.; Kainerstorfer, J.M.; Chernomordik, V.; Mooshagian, E.; Najafizadeh, L.; Krueger, F.; Gandjbakhche, A.H.; Wassermann, E.M. Normative database of judgment of complexity task with functional near infrared spectroscopy—application for TBI. Neuroimage 2012, 60, 879–883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferradal, S.L.; Eggebrecht, A.T.; Hassanpour, M.; Snyder, A.Z.; Culver, J.P. Atlas-based head modeling and spatial normalization for high-density diffuse optical tomography: In vivo validation against fMRI. Neuroimage 2014, 85 Pt 1, 117–126. [Google Scholar] [CrossRef] [Green Version]
- Eggebrecht, A.T.; White, B.R.; Ferradal, S.L.; Chen, C.; Zhan, Y.; Snyder, A.Z.; Dehghani, H.; Culver, J.P. A quantitative spatial comparison of high-density diffuse optical tomography and fMRI cortical mapping. Neuroimage 2012, 61, 1120–1128. [Google Scholar] [CrossRef] [Green Version]
- Sharma, A.; Hind, K.; Hume, P.; Singh, J.; Neary, J.P. Neurovascular Coupling by Functional Near Infra-Red Spectroscopy and Sport-Related Concussion in Retired Rugby Players: The UK Rugby Health Project. Front. Hum. Neurosci. 2020, 14, 42. [Google Scholar] [CrossRef] [Green Version]
- Kontos, A.P.; Huppert, T.J.; Beluk, N.H.; Elbin, R.J.; Henry, L.C.; French, J.; Dakan, S.M.; Collins, M.W. Brain activation during neurocognitive testing using functional near-infrared spectroscopy in patients following concussion compared to healthy controls. Brain Imaging Behav. 2014, 8, 621–634. [Google Scholar] [CrossRef] [Green Version]
- Urban, K.J.; Barlow, K.M.; Jimenez, J.J.; Goodyear, B.G.; Dunn, J.F. Functional near-infrared spectroscopy reveals reduced interhemispheric cortical communication after pediatric concussion. J. Neurotrauma 2015, 32, 833–840. [Google Scholar] [CrossRef]
- Helmich, I.; Berger, A.; Lausberg, H. Neural Control of Posture in Individuals with Persisting Postconcussion Symptoms. Med. Sci. Sports Exerc. 2016, 48, 2362–2369. [Google Scholar] [CrossRef]
- Helmich, I.; Saluja, R.S.; Lausberg, H.; Kempe, M.; Furley, P.; Berger, A.; Chen, J.K.; Ptito, A. Persistent Postconcussive Symptoms Are Accompanied by Decreased Functional Brain Oxygenation. J. Neuropsychiatry Clin. Neurosci. 2015, 27, 287–298. [Google Scholar] [CrossRef]
- Helmich, I.; Coenen, J.; Henckert, S.; Pardalis, E.; Schupp, S.; Lausberg, H. Reduced frontopolar brain activation characterizes concussed athletes with balance deficits. Neuroimage Clin. 2020, 25, 102164. [Google Scholar] [CrossRef] [PubMed]
- Hocke, L.M.; Duszynski, C.C.; Debert, C.T.; Dleikan, D.; Dunn, J.F. Reduced Functional Connectivity in Adults with Persistent Post-Concussion Symptoms: A Functional Near-Infrared Spectroscopy Study. J. Neurotrauma 2018, 35, 1224–1232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bishop, S.A.; Neary, J.P. Assessing prefrontal cortex oxygenation after sport concussion with near-infrared spectroscopy. Clin. Physiol. Funct. Imaging 2018, 38, 573–585. [Google Scholar] [CrossRef] [PubMed]
- Penny, W.; Friston, K.; Ashburner, J.; Kiebel, S.; Nichols, T. Statistical Parametric Mapping: The Analysis of Functional Brain Images; Elsevier: Amsterdam, The Netherlands, 2011. [Google Scholar]
- Chiarelli, A.M.; Romani, G.L.; Merla, A. Fast optical signals in the sensorimotor cortex: General Linear Convolution Model applied to multiple source-detector distance-based data. Neuroimage 2014, 85 Pt 1, 245–254. [Google Scholar] [CrossRef]
- Perpetuini, D.; Cardone, D.; Filippini, C.; Chiarelli, A.M.; Merla, A. Modelling Impulse Response Function of Functional Infrared Imaging for General Linear Model Analysis of Autonomic Activity. Sensors 2019, 19, 849. [Google Scholar] [CrossRef] [Green Version]
- Perpetuini, D.; Cardone, D.; Chiarelli, A.M.; Filippini, C.; Croce, P.; Zappasodi, F.; Rotunno, L.; Anzoletti, N.; Zito, M.; Merla, A. Autonomic impairment in Alzheimer’s disease is revealed by complexity analysis of functional thermal imaging signals during cognitive tasks. Physiol. Meas. 2019, 40, 034002. [Google Scholar] [CrossRef]
- McCrea, M.; Iverson, G.L.; Echemendia, R.J.; Makdissi, M.; Raftery, M. Day of injury assessment of sport-related concussion. Br. J. Sports Med. 2013, 47, 272–284. [Google Scholar] [CrossRef]
- Liebel, S.W.; Clark, U.S.; Xu, X.; Riskin-Jones, H.H.; Hawkshead, B.E.; Schwarz, N.F.; Labbe, D.; Jerskey, B.A.; Sweet, L.H. An FMRI-compatible Symbol Search task. J. Int. Neuropsychol. Soc. 2015, 21, 231–238. [Google Scholar] [CrossRef] [Green Version]
- Sun, X.; Zhang, X.; Chen, X.; Zhang, P.; Bao, M.; Zhang, D.; Chen, J.; He, S.; Hu, X. Age-dependent brain activation during forward and backward digit recall revealed by fMRI. Neuroimage 2005, 26, 36–47. [Google Scholar] [CrossRef]
- Poldrack, R.A. Can cognitive processes be inferred from neuroimaging data? Trends Cogn. Sci. 2006, 10, 59–63. [Google Scholar] [CrossRef] [Green Version]
- Giza, C.C.; Hovda, D.A. The new neurometabolic cascade of concussion. Neurosurgery 2014, 75 (Suppl. 4), S24–S33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macciocchi, S.N.; Barth, J.T.; Alves, W.; Rimel, R.W.; Jane, J.A. Neuropsychological functioning and recovery after mild head injury in collegiate athletes. Neurosurgery 1996, 39, 510–514. [Google Scholar] [CrossRef] [PubMed]
- Pujol, J.; Deus, J.; Losilla, J.M.; Capdevila, A. Cerebral lateralization of language in normal left-handed people studied by functional MRI. Neurology 1999, 52, 1038–1043. [Google Scholar] [CrossRef] [PubMed]
- Vigneau, M.; Beaucousin, V.; Herve, P.Y.; Jobard, G.; Petit, L.; Crivello, F.; Mellet, E.; Zago, L.; Mazoyer, B.; Tzourio-Mazoyer, N. What is right-hemisphere contribution to phonological, lexico-semantic, and sentence processing? Insights from a meta-analysis. Neuroimage 2011, 54, 577–593. [Google Scholar] [CrossRef]
- Saur, D.; Kreher, B.W.; Schnell, S.; Kummerer, D.; Kellmeyer, P.; Vry, M.S.; Umarova, R.; Musso, M.; Glauche, V.; Abel, S.; et al. Ventral and dorsal pathways for language. Proc. Natl. Acad. Sci. USA 2008, 105, 18035–18040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Black, D.F.; Vachha, B.; Mian, A.; Faro, S.H.; Maheshwari, M.; Sair, H.I.; Petrella, J.R.; Pillai, J.J.; Welker, K. American Society of Functional Neuroradiology-Recommended fMRI Paradigm Algorithms for Presurgical Language Assessment. AJNR. Am. J. Neuroradiol. 2017, 38, E65–E73. [Google Scholar] [CrossRef] [Green Version]
- Zaca, D.; Jarso, S.; Pillai, J.J. Role of semantic paradigms for optimization of language mapping in clinical FMRI studies. AJNR Am. J. Neuroradiol. 2013, 34, 1966–1971. [Google Scholar] [CrossRef] [Green Version]
- Pillai, J.J.; Zaca, D. Relative utility for hemispheric lateralization of different clinical fMRI activation tasks within a comprehensive language paradigm battery in brain tumor patients as assessed by both threshold-dependent and threshold-independent analysis methods. Neuroimage 2011, 54 (Suppl. 1), S136–S145. [Google Scholar] [CrossRef]
- Kaneko, H.; Yoshikawa, T.; Nomura, K.; Ito, H.; Yamauchi, H.; Ogura, M.; Honjo, S. Hemodynamic changes in the prefrontal cortex during digit span task: A near-infrared spectroscopy study. Neuropsychobiology 2011, 63, 59–65. [Google Scholar] [CrossRef]
- Hoshi, Y.; Oda, I.; Wada, Y.; Ito, Y.; Yutaka, Y.; Oda, M.; Ohta, K.; Yamada, Y.; Mamoru, T. Visuospatial imagery is a fruitful strategy for the digit span backward task: A study with near-infrared optical tomography. Cogn. Brain Res. 2000, 9, 339–342. [Google Scholar] [CrossRef]
- Aleman, A.; van’t Wout, M. Repetitive transcranial magnetic stimulation over the right dorsolateral prefrontal cortex disrupts digit span task performance. Neuropsychobiology 2008, 57, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Gerton, B.K.; Brown, T.T.; Meyer-Lindenberg, A.; Kohn, P.; Holt, J.L.; Olsen, R.K.; Berman, K.F. Shared and distinct neurophysiological components of the digits forward and backward tasks as revealed by functional neuroimaging. Neuropsychologia 2004, 42, 1781–1787. [Google Scholar] [CrossRef] [PubMed]
- Thoma, R.J.; Cook, J.A.; McGrew, C.; King, J.H.; Pulsipher, D.T.; Yeo, R.A.; Monnig, M.A.; Mayer, A.; Pommy, J.; Campbell, R.A. Convergent and discriminant validity of the ImPACT with traditional neuropsychological measures. Cogent Psychol. 2018, 5, 1430199. [Google Scholar] [CrossRef]
- Maerlender, A.; Flashman, L.; Kessler, A.; Kumbhani, S.; Greenwald, R.; Tosteson, T.; McAllister, T. Examination of the construct validity of ImPACT computerized test, traditional, and experimental neuropsychological measures. Clin. Neuropsychol. 2010, 24, 1309–1325. [Google Scholar] [CrossRef] [Green Version]
- Echemendia, R.J.; Iverson, G.L.; McCrea, M.; Macciocchi, S.N.; Gioia, G.A.; Putukian, M.; Comper, P. Advances in neuropsychological assessment of sport-related concussion. Br. J. Sports Med. 2013, 47, 294–298. [Google Scholar] [CrossRef] [PubMed]
- Jackson, G.D.; Makdissi, M.; Pedersen, M.; Parker, D.M.; Curwood, E.K.; Farquharson, S.; Connelly, A.; Abbott, D.F.; McCrory, P. Functional brain effects of acute concussion in Australian rules football players. J. Concussion 2019, 3, 205970021986120. [Google Scholar] [CrossRef]
- Monti, M.M. Statistical Analysis of fMRI Time-Series: A Critical Review of the GLM Approach. Front. Hum. Neurosci. 2011, 5, 28. [Google Scholar] [CrossRef] [Green Version]
- Kirilina, E.; Jelzow, A.; Heine, A.; Niessing, M.; Wabnitz, H.; Bruhl, R.; Ittermann, B.; Jacobs, A.M.; Tachtsidis, I. The physiological origin of task-evoked systemic artefacts in functional near infrared spectroscopy. Neuroimage 2012, 61, 70–81. [Google Scholar] [CrossRef] [Green Version]
- Erdogan, S.B.; Yucel, M.A.; Akin, A. Analysis of task-evoked systemic interference in fNIRS measurements: Insights from fMRI. Neuroimage 2014, 87, 490–504. [Google Scholar] [CrossRef]
- Rodrigues, A.C.; Lima, M.D.M.; de Souza, L.C.; Furtado, C.; Marques, C.E.; Gonçalves, L.; Lima, M.V.; Lasmar, R.P.; Caramelli, P. No Evidence of Association Between Soccer Heading and Cognitive Performance in Professional Soccer Players: Cross-Sectional Results. Front. Neurol. 2019, 10, 209. [Google Scholar] [CrossRef] [Green Version]
- Seidel-Marzi, O.; Ragert, P. Neurodiagnostics in Sports: Investigating the Athlete’s Brain to Augment Performance and Sport-Specific Skills. Front. Hum. Neurosci. 2020, 14, 133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donders, J.; Stout, J. The Influence of Cognitive Reserve on Recovery from Traumatic Brain Injury. Arch. Clin. Neuropsychol. 2019, 34, 206–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Louey, A.G.; Cromer, J.A.; Schembri, A.J.; Darby, D.G.; Maruff, P.; Makdissi, M.; McCrory, P. Detecting cognitive impairment after concussion: Sensitivity of change from baseline and normative data methods using the CogSport/Axon cognitive test battery. Arch. Clin. Neuropsychol. 2014, 29, 432–441. [Google Scholar] [CrossRef] [PubMed]
- Yakoub, K.M.; Davies, D.J.; Su, Z.; Bentley, C.; Forcione, M.; Toman, E.; Hammond, D.; Watson, C.N.; Bishop, J.; Cooper, L.; et al. Investigation into repetitive concussion in sport (RECOS): Study protocol of a prospective, exploratory, observational cohort study. BMJ Open 2019, 9, e029883. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.H.; Low, K.A.; Kong, T.; Fletcher, M.A.; Zimmerman, B.; Maclin, E.L.; Chiarelli, A.M.; Gratton, G.; Fabiani, M. Mapping cerebral pulse pressure and arterial compliance over the adult lifespan with optical imaging. PLoS ONE 2017, 12, e0171305. [Google Scholar] [CrossRef] [PubMed]
- Mathewson, K.E.; Beck, D.M.; Ro, T.; Maclin, E.L.; Low, K.A.; Fabiani, M.; Gratton, G. Dynamics of alpha control: Preparatory suppression of posterior alpha oscillations by frontal modulators revealed with combined EEG and event-related optical signal. J. Cogn. Neurosci. 2014, 26, 2400–2415. [Google Scholar] [CrossRef] [Green Version]
- Whalen, C.; Maclin, E.L.; Fabiani, M.; Gratton, G. Validation of a method for coregistering scalp recording locations with 3D structural MR images. Hum. Brain Mapp. 2008, 29, 1288–1301. [Google Scholar] [CrossRef]
- Cameron, T.A.; Lucas, S.J.; Machado, L. Near-infrared spectroscopy reveals link between chronic physical activity and anterior frontal oxygenated hemoglobin in healthy young women. Psychophysiology 2015, 52, 609–617. [Google Scholar] [CrossRef]
- Carlozzi, N.E.; Kirsch, N.L.; Kisala, P.A.; Tulsky, D.S. An examination of the Wechsler Adult Intelligence Scales, Fourth Edition (WAIS-IV) in individuals with complicated mild, moderate and Severe traumatic brain injury (TBI). Clin. Neuropsychol. 2015, 29, 21–37. [Google Scholar] [CrossRef]
- Chiarelli, A.M.; Maclin, E.L.; Low, K.A.; Fabiani, M.; Gratton, G. Comparison of procedures for co-registering scalp-recording locations to anatomical magnetic resonance images. J. Biomed. Opt. 2015, 20, 016009. [Google Scholar] [CrossRef] [Green Version]
- Chiarelli, A.M.; Maclin, E.L.; Fabiani, M.; Gratton, G. A kurtosis-based wavelet algorithm for motion artifact correction of fNIRS data. Neuroimage 2015, 112, 128–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sassaroli, A.; Fantini, S. Comment on the modified Beer-Lambert law for scattering media. Phys. Med. Biol. 2004, 49, N255–N257. [Google Scholar] [CrossRef] [Green Version]
- Zijlstra, W.G.; Buursma, A.; Meeuwsen-van der Roest, W.P. Absorption spectra of human fetal and adult oxyhemoglobin, de-oxyhemoglobin, carboxyhemoglobin, and methemoglobin. Clin. Chem. 1991, 37, 1633–1638. [Google Scholar] [CrossRef] [PubMed]
- Chiarelli, A.M.; Perpetuini, D.; Filippini, C.; Cardone, D.; Merla, A. Differential pathlength factor in continuous wave functional near-infrared spectroscopy: Reducing hemoglobin’s cross talk in high-density recordings. Neurophotonics 2019, 6, 035005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scholkmann, F.; Wolf, M. General equation for the differential pathlength factor of the frontal human head depending on wavelength and age. J. Biomed. Opt. 2013, 18, 105004. [Google Scholar] [CrossRef] [Green Version]
- Dehghani, H.; Eames, M.E.; Yalavarthy, P.K.; Davis, S.C.; Srinivasan, S.; Carpenter, C.M.; Pogue, B.W.; Paulsen, K.D. Near infrared optical tomography using NIRFAST: Algorithm for numerical model and image reconstruction. Commun. Numer. Methods Eng. 2008, 25, 711–732. [Google Scholar] [CrossRef]
- Eggebrecht, A.T.; Ferradal, S.L.; Robichaux-Viehoever, A.; Hassanpour, M.S.; Dehghani, H.; Snyder, A.Z.; Hershey, T.; Culver, J.P. Mapping distributed brain function and networks with diffuse optical tomography. Nat. Photonics 2014, 8, 448–454. [Google Scholar] [CrossRef] [Green Version]
- Fang, Q.; Boas, D.A. Tetrahedral mesh generation from volumetric binary and grayscale images. In 2009 IEEE International Symposium on Biomedical Imaging: From Nano to Macro; IEEE: Piscataway, NJ, USA, 2009; pp. 1142–1145. [Google Scholar]
- Tian, F.; Liu, H. Depth-compensated diffuse optical tomography enhanced by general linear model analysis and an anatomical atlas of human head. Neuroimage 2014, 85 Pt 1, 166–180. [Google Scholar] [CrossRef]
- Tachtsidis, I.; Scholkmann, F. False positives and false negatives in functional near-infrared spectroscopy: Issues, challenges, and the way forward. Neurophotonics 2016, 3, 031405. [Google Scholar] [CrossRef] [Green Version]









© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Forcione, M.; Chiarelli, A.M.; Perpetuini, D.; Davies, D.J.; O’Halloran, P.; Hacker, D.; Merla, A.; Belli, A. Tomographic Task-Related Functional Near-Infrared Spectroscopy in Acute Sport-Related Concussion: An Observational Case Study. Int. J. Mol. Sci. 2020, 21, 6273. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21176273
Forcione M, Chiarelli AM, Perpetuini D, Davies DJ, O’Halloran P, Hacker D, Merla A, Belli A. Tomographic Task-Related Functional Near-Infrared Spectroscopy in Acute Sport-Related Concussion: An Observational Case Study. International Journal of Molecular Sciences. 2020; 21(17):6273. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21176273
Chicago/Turabian StyleForcione, Mario, Antonio Maria Chiarelli, David Perpetuini, David James Davies, Patrick O’Halloran, David Hacker, Arcangelo Merla, and Antonio Belli. 2020. "Tomographic Task-Related Functional Near-Infrared Spectroscopy in Acute Sport-Related Concussion: An Observational Case Study" International Journal of Molecular Sciences 21, no. 17: 6273. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21176273