Association Analysis in Children Born from Normal and Complicated Pregnancies—Cardiovascular Disease Associated microRNAs and the Incidence of Prehypertension/Hypertension, Overweight/Obesity, Valve Problems and Heart Defects



Abstract
:1. Introduction
2. Results
2.1. Abnormal microRNA Expression Profile in Children Born from Complicated Pregnancies
2.2. No Association between the Presence of Prehypertension/Hypertension and Expression of Examined microRNAs
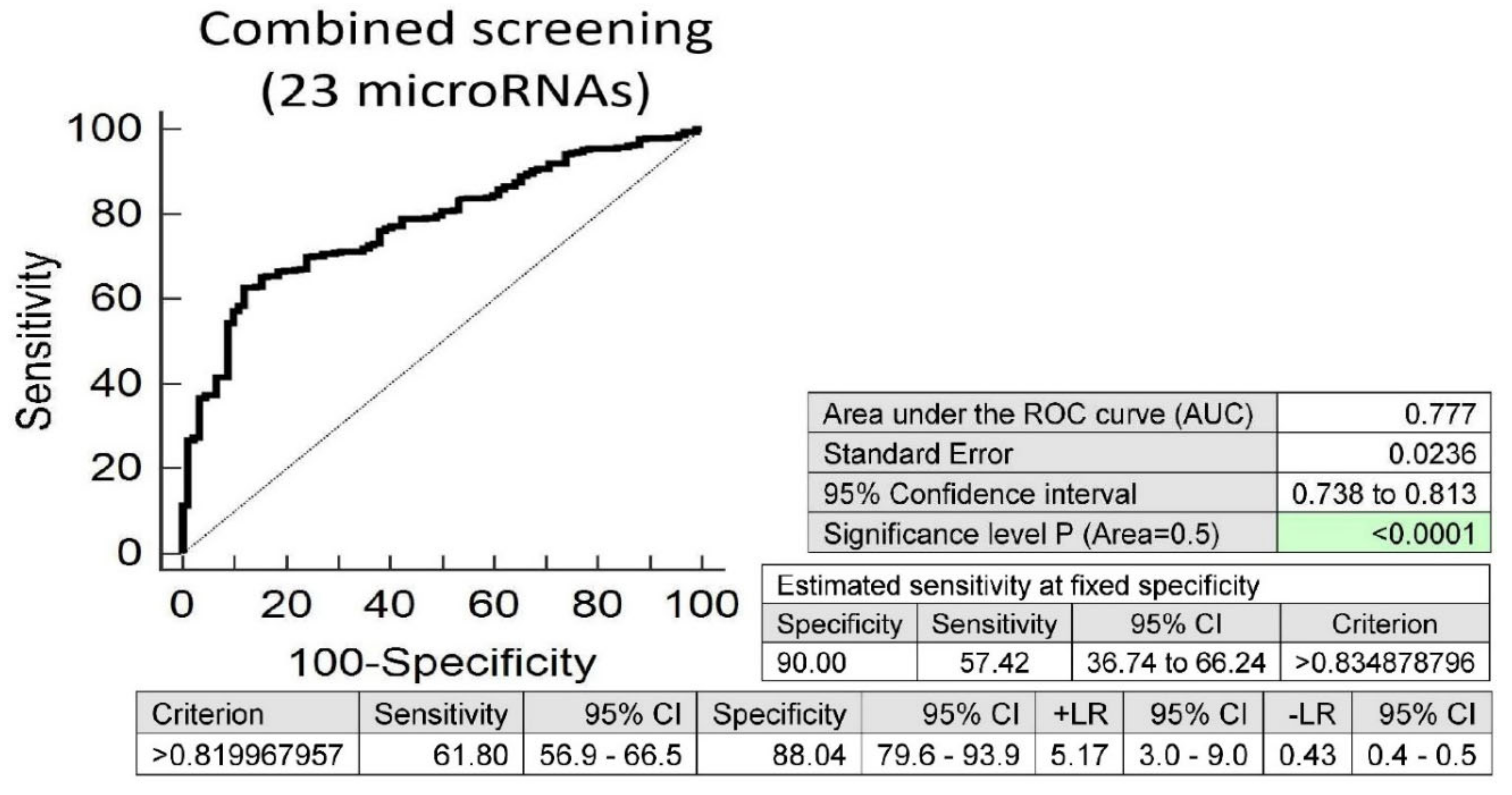
2.3. Postnatal Expression Profile of 19 Tested microRNAs Differentiates between Overweight/Obese Children and Children with Nomal BMI Values
2.4. Postnatal Expression Profile of 10 Tested microRNAs Differentiates between Children with Abnormal and Normal Values of Echocardiographic Measurements
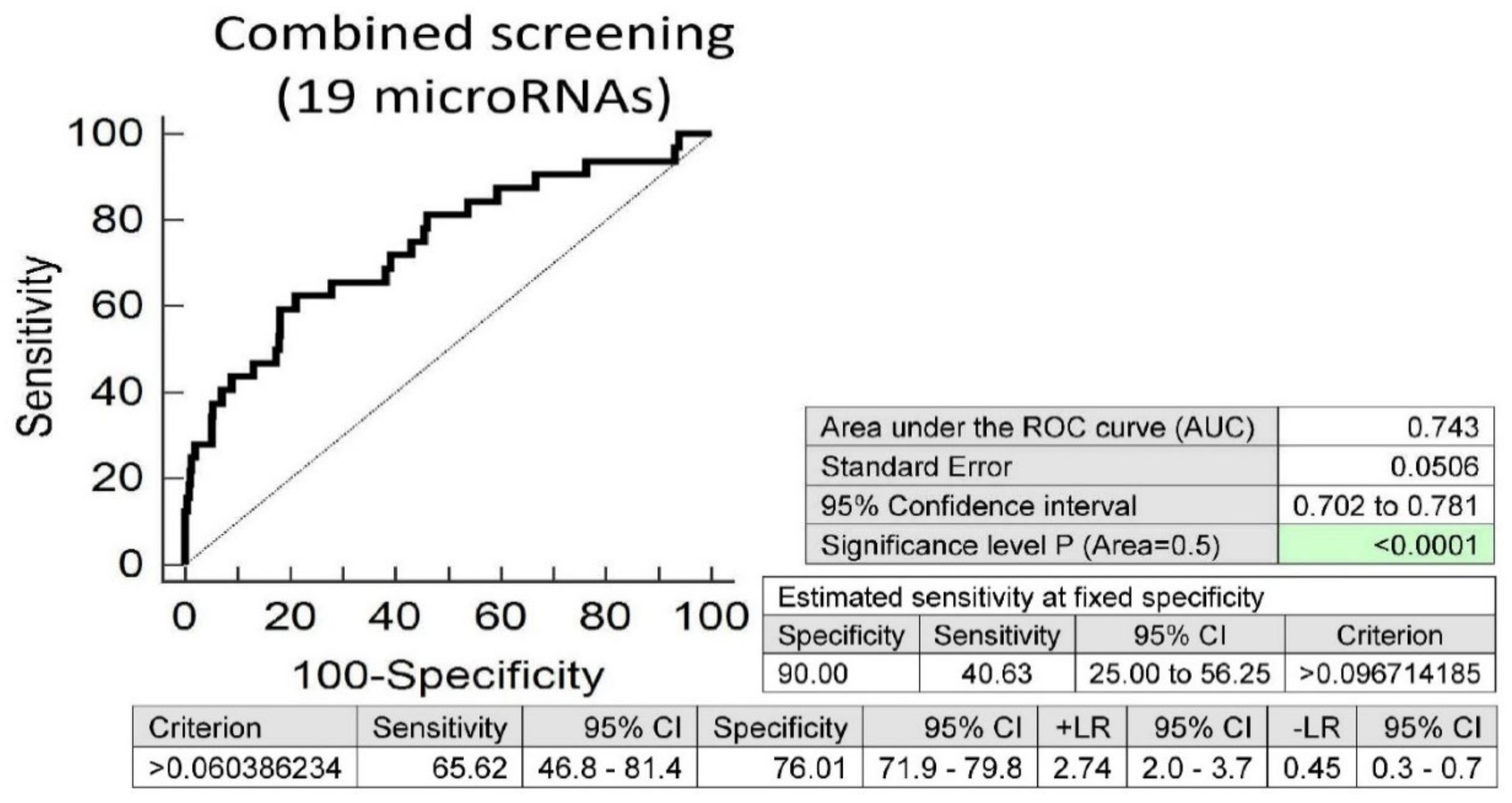
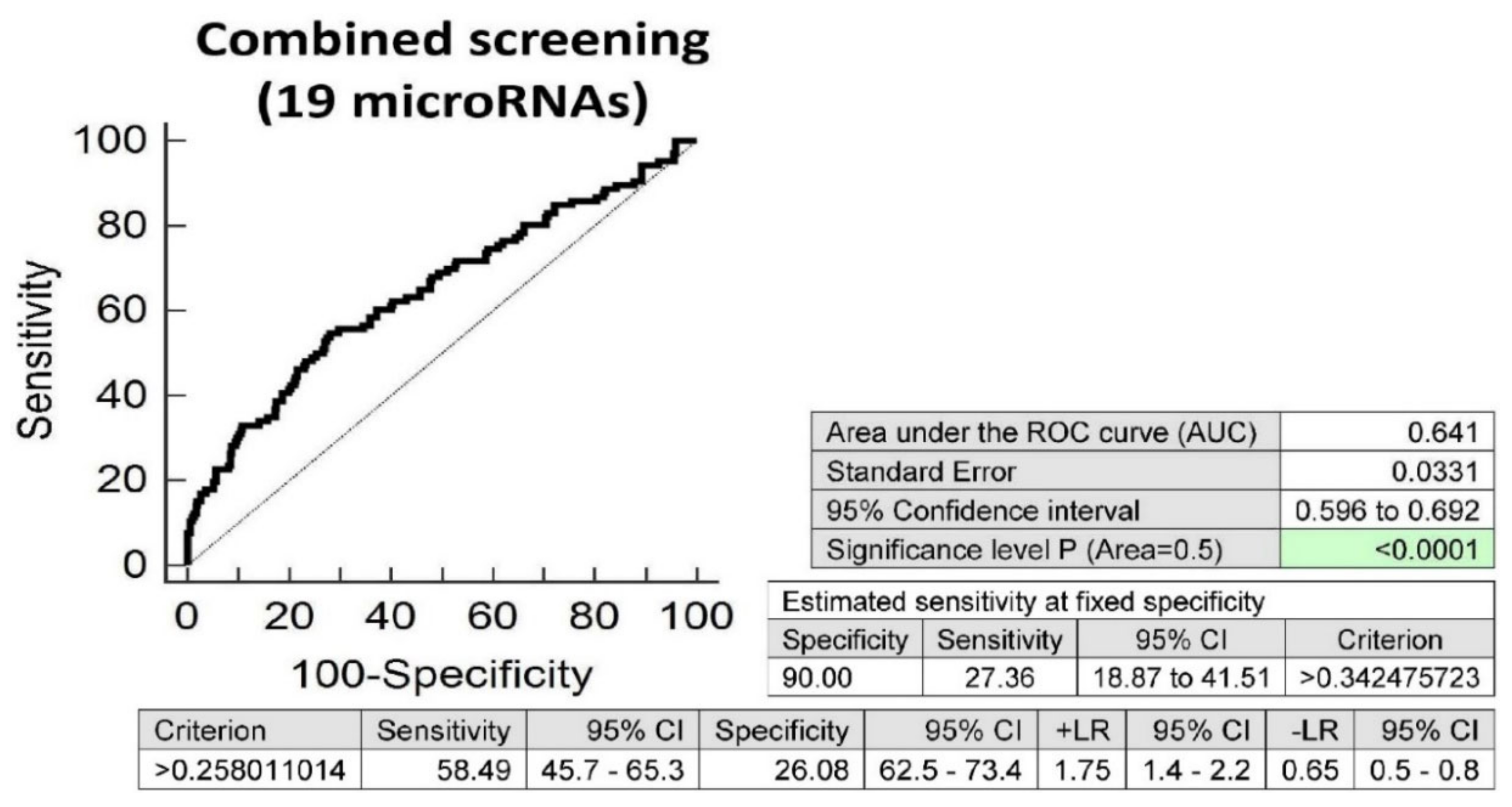
2.5. Postnatal Expression Profile of 19 Tested microRNAs Differentiates between Overweight/Obese and Normal Weight Children Born from Normal Pregnancies
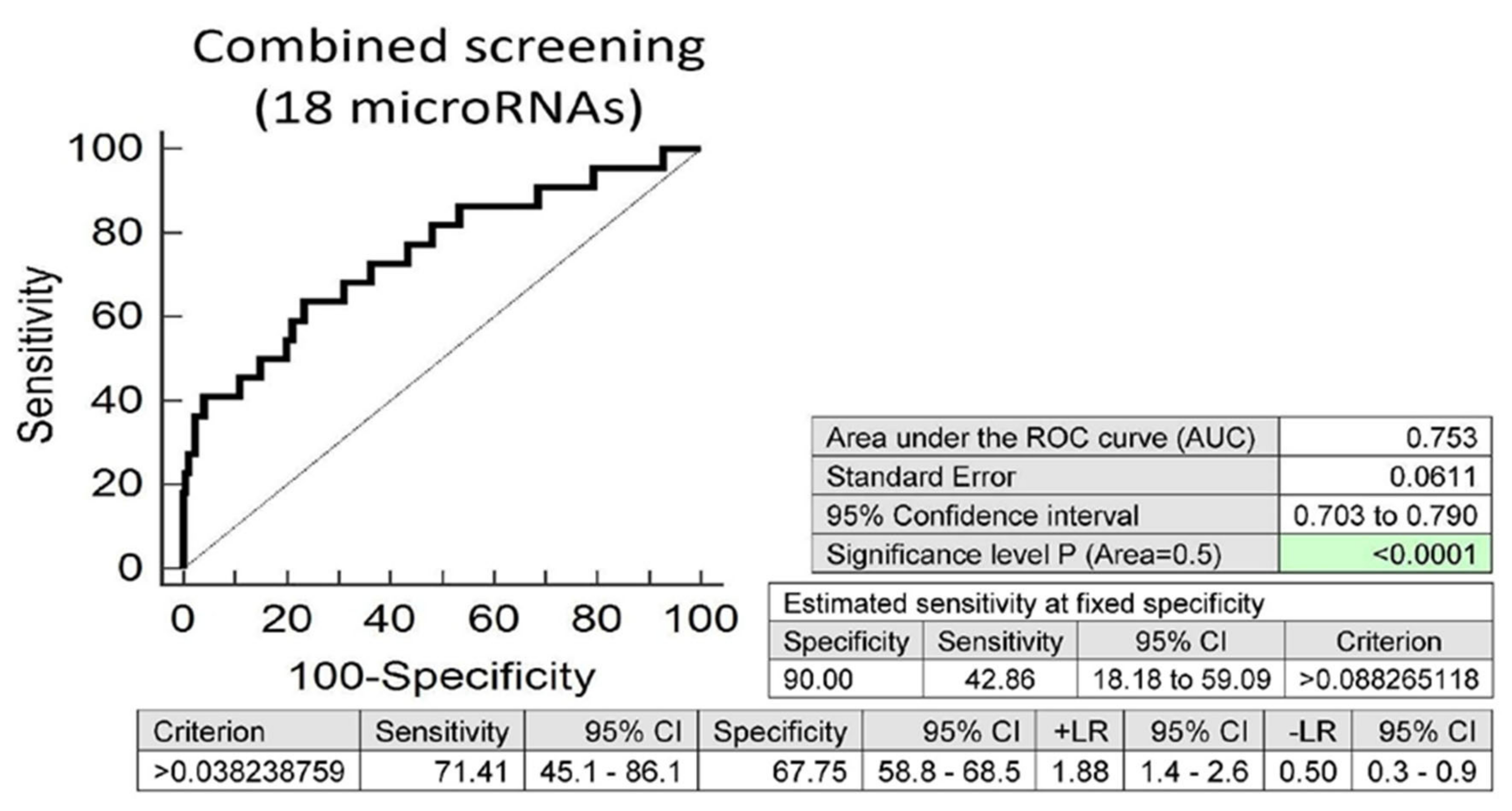
2.6. Postnatal Expression Profile of 18 Tested microRNAs Differentiates between Overweight/Obese and Normal Weight Children Born from Complicated Gestation
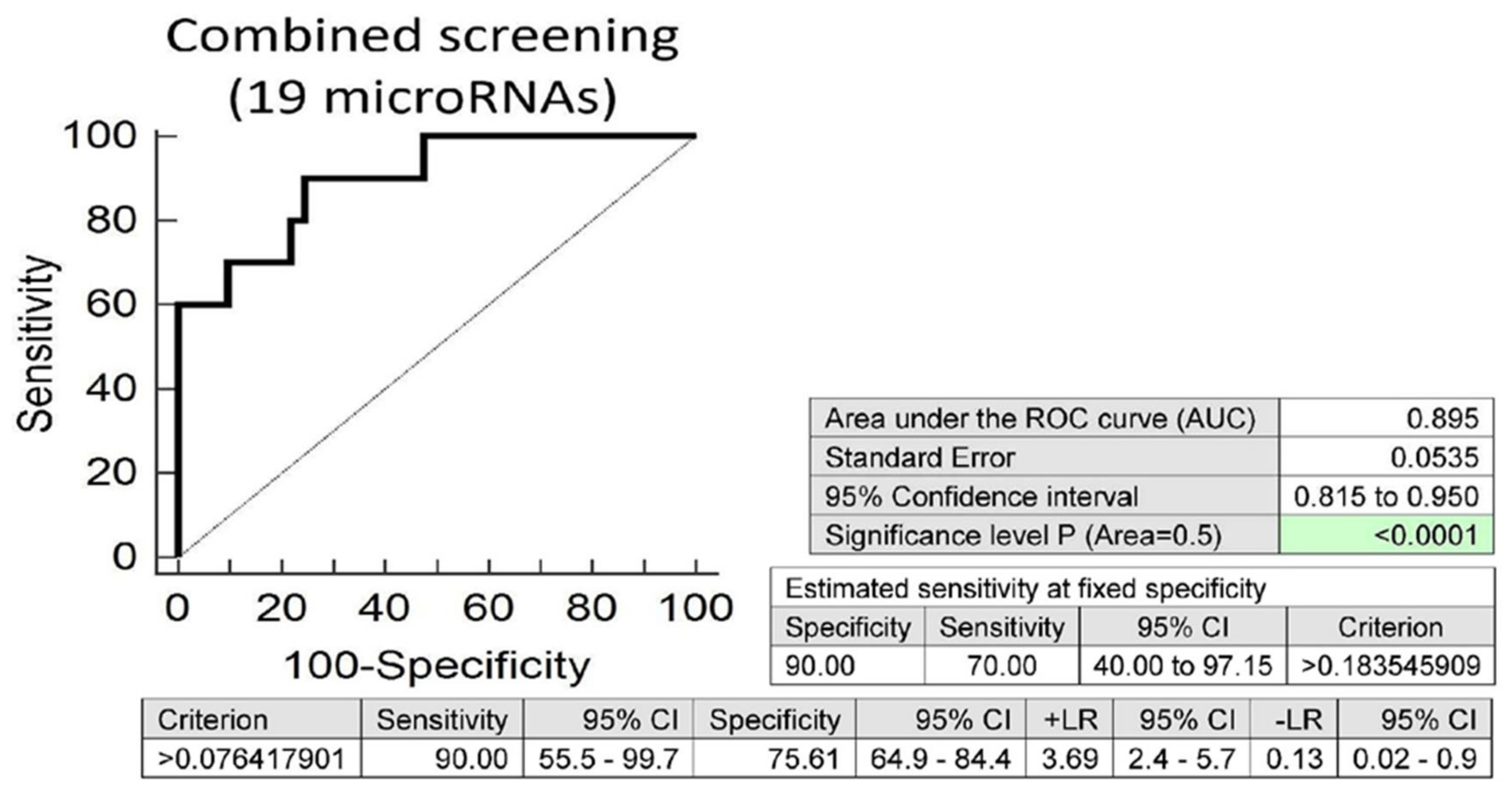
2.7. Postnatal Expression Profile of 19 microRNAs Differentiates between Children with Abnormal and Normal Values of Echocardiographic Measurements Descending from Complicated Pregnancies
3. Discussion
4. Materials and Methods
4.1. Participants
4.2. Blood Pressure and Echocardiography Measurements, and Body Mass Index Assessment
4.3. Processing of Samples, Reverse Transcription, and Relative Quantification of microRNAs
4.4. Statistical Analysis
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| GDM | Gestational diabetes mellitus |
| PE | Preeclampsia |
| FGR | Fetal growth restriction |
| GH | Gestational hypertension |
| AUC | Area under the Curve |
| ROC | Receive Operating Characteristic |
| FPR | False Positive Rate |
| CI | Confidence Interval |
| LR+ | Positive Likelihood Ratio |
| LR- | Negative Likelihood Ratio |
| NP | Normal Pregnancies |
| BP | Blood Pressure |
| OGTT | Oral glucose tolerance test |
| IADPSG | International Association of Diabetes and Pregnancy Study Groups |
| BMI | Body Mass Index |
| SBP | Systolic Blood Pressure |
| DBP | Diastolic Blood Pressure |
| GA | Gestational age |
| CS | Caesarean Section |
References
- Davis, E.F.; Lazdam, M.; Lewandowski, A.J.; Worton, S.A.; Kelly, B.; Kenworthy, Y.; Adwani, S.; Wilkinson, A.R.; McCormick, K.; Sargent, I.; et al. Cardiovascular Risk Factors in Children and Young Adults Born to Preeclamptic Pregnancies: A Systematic Review. Pediatrics 2012, 129, e1552–e1561. [Google Scholar] [CrossRef] [PubMed]
- Alsnes, I.V.; Vatten, L.J.; Fraser, A.; Bjørngaard, J.H.; Rich-Edwards, J.; Romundstad, P.R.; Asvold, B.O. Hypertension in Pregnancy and Offspring Cardiovascular Risk in Young Adulthood. Hypertension 2017, 69, 591–598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawasaki, M.; Arata, N.; Miyazaki, C.; Mori, R.; Kikuchi, T.; Ogawa, Y.; Ota, E. Obesity and abnormal glucose tolerance in offspring of diabetic mothers: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0190676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hammoud, N.M.; Visser, G.H.A.; Van Rossem, L.; Biesma, D.H.; Wit, J.M.; De Valk, H.W. Long-term BMI and growth profiles in offspring of women with gestational diabetes. Diabetologia 2018, 61, 1037–1045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bianco, M.E.; Josefson, J.L. Hyperglycemia During Pregnancy and Long-Term Offspring Outcomes. Curr. Diabetes Rep. 2019, 19, 143. [Google Scholar] [CrossRef]
- Lee, H.; Jang, H.C.; Park, H.K.; Cho, N.H. Early manifestation of cardiovascular disease risk factors in offspring of mothers with previous history of gestational diabetes mellitus. Diabetes Res. Clin. Pr. 2007, 78, 238–245. [Google Scholar] [CrossRef]
- Tam, W.H.; Ma, R.C.W.; Ozaki, R.; Li, A.M.; Chan, M.H.M.; Yuen, L.Y.; Lao, T.T.H.; Yang, X.; Ho, C.S.; Tutino, G.E.; et al. In Utero Exposure to Maternal Hyperglycemia Increases Childhood Cardiometabolic Risk in Offspring. Diabetes Care 2017, 40, 679–686. [Google Scholar] [CrossRef] [Green Version]
- Tsadok, M.A.; Friedlander, Y.; Paltiel, O.; Manor, O.; Meiner, V.; Hochner, H.; Sagy, Y.; Sharon, N.; Yazdgerdi, S.; Siscovick, D.; et al. Obesity and Blood Pressure in 17-Year-Old Offspring of Mothers with Gestational Diabetes: Insights from the Jerusalem Perinatal Study. Exp. Diabetes Res. 2011, 2011, 1–6. [Google Scholar] [CrossRef]
- Chen, Y.-L.; Han, L.-L.; Shi, X.-L.; Su, W.-J.; Liu, W.; Wang, L.-Y.; Huang, P.-Y.; Lin, M.-Z.; Song, H.-Q.; Li, X. Adverse pregnancy outcomes on the risk of overweight offspring: A population-based retrospective study in Xiamen, China. Sci. Rep. 2020, 10, 1549. [Google Scholar] [CrossRef]
- Josefson, J.L.; Catalano, P.M.; Lowe, W.L.; Scholtens, D.M.; Kuang, A.; Dyer, A.R.; Lowe, L.P.; Metzger, B.E. The Joint Associations of Maternal BMI and Glycemia with Childhood Adiposity. J. Clin. Endocrinol. Metab. 2020, 105, 2177–2188. [Google Scholar] [CrossRef]
- Liang, Z.; Liu, H.; Wang, L.; Song, Q.; Sun, D.; Li, W.; Leng, J.; Gao, R.; Hu, G.; Qi, L. Maternal Gestational Diabetes Mellitus Modifies the Relationship between Genetically Determined Body Mass Index during Pregnancy and Childhood Obesity. Mayo Clin. Proc. 2020, 95, 1877–1887. [Google Scholar] [CrossRef] [PubMed]
- Tenhola, S.; Rahiala, E.; Martikainen, A.; Halonen, P.; Voutilainen, R. Blood Pressure, Serum Lipids, Fasting Insulin, and Adrenal Hormones in 12-Year-Old Children Born with Maternal Preeclampsia. J. Clin. Endocrinol. Metab. 2003, 88, 1217–1222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogland, B.; Forman, M.R.; Romundstad, P.R.; Nilsen, S.T.; Vatten, L.J. Blood pressure in early adolescence in the offspring of preeclamptic and normotensive pregnancies. J. Hypertens. 2009, 27, 2051–2054. [Google Scholar] [CrossRef] [PubMed]
- Fraser, A.; Nelson, S.M.; Macdonald-Wallis, C.; Sattar, N.; Lawlor, D.A. Hypertensive Disorders of Pregnancy and Cardiometabolic Health in Adolescent Offspring. Hypertension 2013, 62, 614–620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Staley, J.R.; Bradley, J.; Silverwood, R.J.; Howe, L.D.; Tilling, K.M.; Lawlor, D.A.; Macdonald-Wallis, C. Associations of Blood Pressure in Pregnancy With Offspring Blood Pressure Trajectories During Childhood and Adolescence: Findings From a Prospective Study. J. Am. Hear. Assoc. 2015, 4, 4. [Google Scholar] [CrossRef] [Green Version]
- Lazdam, M.; De La Horra, A.; Diesch, J.; Kenworthy, Y.; Davis, E.; Lewandowski, A.J.; Szmigielski, C.; Shore, A.C.; MacKillop, L.; Kharbanda, R.K.; et al. Unique Blood Pressure Characteristics in Mother and Offspring After Early Onset Preeclampsia. Hypertension 2012, 60, 1338–1345. [Google Scholar] [CrossRef] [Green Version]
- Lim, W.-Y.; Lee, Y.-S.; Yap, F.K.-P.; Aris, I.M.; Lek, N.; Meaney, M.; Gluckman, P.D.; Godfrey, K.M.; Kwek, K.; Chong, Y.-S.; et al. Maternal Blood Pressure During Pregnancy and Early Childhood Blood Pressures in the Offspring. Medicine 2015, 94, e1981. [Google Scholar] [CrossRef]
- Rostand, S.G.; Cliver, S.P.; Goldenberg, R.L. Racial disparities in the association of foetal growth retardation to childhood blood pressure. Nephrol. Dial. Transplant. 2005, 20, 1592–1597. [Google Scholar] [CrossRef] [Green Version]
- Lu, J.; Zhang, S.; Li, W.; Leng, J.; Wang, L.; Liu, H.; Li, W.; Zhang, C.; Qi, L.; Tuomilehto, J.; et al. Maternal Gestational Diabetes Is Associated With Offspring’s Hypertension. Am. J. Hypertens. 2019, 32, 335–342. [Google Scholar] [CrossRef] [Green Version]
- Wright, C.S.; Rifas-Shiman, S.L.; Rich-Edwards, J.W.; Taveras, E.M.; Gillman, M.W.; Oken, E. Intrauterine Exposure to Gestational Diabetes, Child Adiposity, and Blood Pressure. Am. J. Hypertens. 2009, 22, 215–220. [Google Scholar] [CrossRef] [Green Version]
- Perng, W.; Hockett, C.W.; Sauder, K.A.; Dabelea, D. In utero exposure to gestational diabetes mellitus and cardiovascular risk factors in youth: A longitudinal analysis in the EPOCH cohort. Pediatr. Obes. 2020, 15, e12611. [Google Scholar] [CrossRef] [PubMed]
- Beukers, F.; Rotteveel, J.; Ganzevoort, W.; Van Weissenbruch, M.M.; Van Goudoever, J.B.; Van Wassenaer-Leemhuis, A.G. Blood pressure of 12-year-old children born after foetal growth restriction due to hypertensive disorders of pregnancy; relation to neonatal, life style, and family characteristics. Early Hum. Dev. 2019, 130, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Perng, W.; Ringham, B.M.; Smith, H.A.; Michelotti, G.; Kechris, K.M.; Dabelea, D. A prospective study of associations between in utero exposure to gestational diabetes mellitus and metabolomic profiles during late childhood and adolescence. Diabetologia 2020, 63, 296–312. [Google Scholar] [CrossRef] [PubMed]
- Lowe, W.L.; Scholtens, D.M.; Kuang, A.; Linder, B.; Lawrence, J.M.; Lebenthal, Y.; McCance, D.R.; Hamilton, J.K.; Nodzenski, M.; Talbot, O.; et al. Hyperglycemia and Adverse Pregnancy Outcome Follow-up Study (HAPO FUS): Maternal Gestational Diabetes Mellitus and Childhood Glucose Metabolism. Diabetes Care 2019, 42, 372–380. [Google Scholar] [CrossRef] [Green Version]
- Jayet, P.-Y.; Rimoldi, S.F.; Stuber, T.; Salmoòn, C.S.; Hutter, D.; Rexhaj, E.; Thalmann, S.; Schwab, M.; Turini, P.; Sartori-Cucchia, C.; et al. Pulmonary and Systemic Vascular Dysfunction in Young Offspring of Mothers With Preeclampsia. Circulation 2010, 122, 488–494. [Google Scholar] [CrossRef] [Green Version]
- Sarvari, S.I.; Rodríguez-López, M.; Nunez-Garcia, M.; Sitges, M.; Sepúlveda-Martínez, A.; Camara, O.; Butakoff, C.; Gratacós, E.; Bijnens, B.; Crispi, F. Persistence of Cardiac Remodeling in Preadolescents with Fetal Growth Restriction. Circ. Cardiovasc. Imaging 2017, 10, e005270. [Google Scholar] [CrossRef] [Green Version]
- Yiallourou, S.R.; Wallace, E.M.; Whatley, C.; Odoi, A.; Hollis, S.; Weichard, A.J.; Muthusamy, J.S.; Varma, S.; Cameron, J.D.; Narayan, O.; et al. Sleep: A Window Into Autonomic Control in Children Born Preterm and Growth Restricted. Sleep 2017, 40. [Google Scholar] [CrossRef]
- Patey, O.; Carvalho, J.S.; Thilaganathan, B. Perinatal changes in cardiac geometry and function in growth-restricted fetuses at term. Ultrasound Obstet. Gynecol. 2019, 53, 655–662. [Google Scholar] [CrossRef]
- Cohen, E.; Whatley, C.; Wong, F.Y.; Wallace, E.M.; Mockler, J.C.; Odoi, A.; Hollis, S.; Horne, R.S.; Yiallourou, S.R. Effects of foetal growth restriction and preterm birth on cardiac morphology and function during infancy. Acta Paediatr. 2018, 107, 450–455. [Google Scholar] [CrossRef]
- Lunddorf, L.L.H.; Brix, N.; Ernst, A.; Arendt, L.H.; Støvring, H.; Clemmensen, P.J.; Olsen, J.; Ramlau-Hansen, C.H. Hypertensive disorders in pregnancy and timing of pubertal development in daughters and sons. Hum. Reprod. 2020, 35, 2124–2133. [Google Scholar] [CrossRef]
- Martinez, M.P.; Lin, J.; Chow, T.; Chung, J.; Wang, X.; Xiang, A.H. Maternal Gestational Diabetes and Type 2 Diabetes During Pregnancy and Risk of Childhood Asthma in Offspring. J. Pediatr. 2020, 219, 173–179.e1. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Xiong, T.; Hu, Y. Hypertensive disorders of pregnancy and risk of asthma in offspring: Protocol for a systematic review and meta-analysis. BMJ Open 2020, 10, e035145. [Google Scholar] [CrossRef]
- Berkelhamer, S.K.; Mestan, K.K.; Steinhorn, R.H. An update on the diagnosis and management of bronchopulmonary dysplasia (BPD)-associated pulmonary hypertension. Semin. Perinatol. 2018, 42, 432–443. [Google Scholar] [CrossRef] [PubMed]
- Lagatta, J.M.; Hysinger, E.B.; Zaniletti, I.; Wymore, E.M.; Vyas-Read, S.; Yallapragada, S.; Nelin, L.D.; Truog, W.E.; Padula, M.A.; Porta, N.F.; et al. The Impact of Pulmonary Hypertension in Preterm Infants with Severe Bronchopulmonary Dysplasia through 1 Year. J. Pediatr. 2018, 203, 218–224.e3. [Google Scholar] [CrossRef] [PubMed]
- Naumburg, E.; Söderström, L. Increased risk of pulmonary hypertension following premature birth. BMC Pediatr. 2019, 19, 1–7. [Google Scholar] [CrossRef]
- Libby, G.; Murphy, D.J.; McEwan, N.F.; Greene, S.A.; Forsyth, J.S.; Chien, P.W.; Morris, A.D.; DARTS/MEMO Collaboration. Pre-eclampsia and the later development of type 2 diabetes in mothers and their children: An intergenerational study from the Walker cohort. Diabetologia 2007, 50, 523–530. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Vargas, L.; Addison, S.S.; Nistala, R.; Kurukulasuriya, D.; Sowers, J.R. Gestational Diabetes and the Offspring: Implications in the Development of the Cardiorenal Metabolic Syndrome in Offspring. Cardiorenal Med. 2012, 2, 134–142. [Google Scholar] [CrossRef] [Green Version]
- Uemura, O.; Ishikura, K.; Kaneko, T.; Hirano, D.; Hamasaki, Y.; Ogura, M.; Mikami, N.; Gotoh, Y.; Sahashi, T.; Fujita, N.; et al. Perinatal factors contributing to chronic kidney disease in a cohort of Japanese children with very low birth weight. Pediatr. Nephrol. 2020, 1–8. [Google Scholar] [CrossRef]
- Hoogenboom, L.A.; Wolfs, T.G.A.M.; Hütten, M.C.; Peutz-Kootstra, C.J.; Schreuder, M.F. Prematurity, perinatal inflammatory stress, and the predisposition to develop chronic kidney disease beyond oligonephropathy. Pediatr. Nephrol. 2020, 1–9. [Google Scholar] [CrossRef]
- Leybovitz-Haleluya, N.; Wainstock, T.; Landau, D.; Sheiner, E. Maternal gestational diabetes mellitus and the risk of subsequent pediatric cardiovascular diseases of the offspring: A population-based cohort study with up to 18 years of follow up. Acta Diabetol. 2018, 55, 1037–1042. [Google Scholar] [CrossRef]
- Walter, E.; Tsumi, E.; Wainstock, T.; Spiegel, E.; Sheiner, E. Maternal gestational diabetes mellitus: Is it associated with long-term pediatric ophthalmic morbidity of the offspring? J. Matern. Neonatal Med. 2019, 32, 2529–2538. [Google Scholar] [CrossRef] [PubMed]
- Ornoy, A.; Ratzon, N.; Greenbaum, C.; Wolf, A.; Dulitzky, M. School-age Children Born to Diabetic Mothers and to Mothers with Gestational Diabetes Exhibit a High Rate of Inattention and Fine and Gross Motor Impairment. J. Pediatr. Endocrinol. Metab. 2001, 14, 681–690. [Google Scholar] [CrossRef] [PubMed]
- He, X.-J.; Dai, R.-X.; Tian, C.-Q.; Hu, C.-L. Neurodevelopmental outcome at 1 year in offspring of women with gestational diabetes mellitus. Gynecol. Endocrinol. 2020, 21, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Noda, M.; Yoshida, S.; Mishina, H.; Matsubayashi, K.; Kawakami, K. Association between maternal hypertensive disorders of pregnancy and child neurodevelopment at 3 years of age: A retrospective cohort study. J. Dev. Orig. Health Dis. 2020, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Marcelle, E.T.; Oliva, M.T.; Hinshaw, S.P. Gestational Smoking and Hypertension as Predictors of Working Memory Functioning in Childhood Attention-Deficit/Hyperactivity Disorder. Front. Psychol. 2020, 11, 1950. [Google Scholar] [CrossRef] [PubMed]
- Dachew, B.A.; Scott, J.G.; Betts, K.; Mamun, A.; Alati, R. Hypertensive disorders of pregnancy and the risk of offspring depression in childhood: Findings from the Avon Longitudinal Study of Parents and Children. Dev. Psychopathol. 2020, 32, 845–851. [Google Scholar] [CrossRef]
- Dachew, B.A.; Scott, J.G.; Mamun, A.; Alati, R. Hypertensive disorders of pregnancy and emotional and behavioural problems in children: A longitudinal population-based study. Eur. Child Adolesc. Psychiatry 2020, 29, 1–10. [Google Scholar] [CrossRef]
- Monteith, C.; Flood, K.; Pinnamaneni, R.; Levine, T.A.; Alderdice, F.A.; Unterscheider, J.; McAuliffe, F.M.; Dicker, P.; Tully, E.C.; Malone, F.D.; et al. An abnormal cerebroplacental ratio (CPR) is predictive of early childhood delayed neurodevelopment in the setting of fetal growth restriction. Am. J. Obstet. Gynecol. 2019, 221, 273.e1–273.e9. [Google Scholar] [CrossRef]
- Delorme, P.; Kayem, G.; Lorthe, E.; Sentilhes, L.; Zeitlin, J.; Subtil, D.; Rozé, J.C.; Vayssière, C.; Durox, M.; Ancel, P.Y.; et al. Neurodevelopment at 2 years and umbilical artery Doppler in cases of very preterm birth after prenatal hypertensive disorder or suspected fetal growth restriction: EPIPAGE -2 prospective population-based cohort study. Ultrasound Obstet. Gynecol. 2020, 56, 557–565. [Google Scholar] [CrossRef]
- Tomlinson, M.S.; Santos, H.P.; Stewart, J.; Joseph, R.; Leviton, A.; Onderdonk, A.B.; Kuban, K.C.K.; Heeren, T.; O’Shea, T.M.; Fry, R.C.; et al. Neurocognitive and social-communicative function of children born very preterm at 10 years of age: Associations with microorganisms recovered from the placenta parenchyma. J. Perinatol. 2020, 40, 306–315. [Google Scholar] [CrossRef] [Green Version]
- Räikkönen, K.; Gissler, M.; Kajantie, E. Associations Between Maternal Antenatal Corticosteroid Treatment and Mental and Behavioral Disorders in Children. JAMA 2020, 323, 1924–1933. [Google Scholar] [CrossRef] [PubMed]
- Hromadnikova, I.; Kotlabova, K.; Dvorakova, L.; Krofta, L.; Sirc, J. Postnatal Expression Profile of microRNAs Associated with Cardiovascular and Cerebrovascular Diseases in Children at the Age of 3 to 11 Years in Relation to Previous Occurrence of Pregnancy-Related Complications. Int. J. Mol. Sci. 2019, 20, 654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hromadnikova, I.; Kotlabova, K.; Dvorakova, L.; Krofta, L.; Sirc, J. Substantially Altered Expression Profile of Diabetes/Cardiovascular/Cerebrovascular Disease Associated microRNAs in Children Descending from Pregnancy Complicated by Gestational Diabetes Mellitus—One of Several Possible Reasons for an Increased Cardiovascular Risk. Cells 2020, 9, 1557. [Google Scholar] [CrossRef]
- Inzaghi, E.; Kistner, A.; Germani, D.; Deodati, A.; Vanpee, M.; Legnevall, L.; Berinder, K.; Cianfarani, S. A prospective case-control study on miRNA circulating levels in subjects born small for gestational age (SGA) evaluated from childhood into young adulthood. PLoS ONE 2020, 15, e0228075. [Google Scholar] [CrossRef] [Green Version]
- Chen, R.; Xin, G.; Zhang, X. Long non-coding RNA HCP5 serves as a ceRNA sponging miR-17-5p and miR-27a/b to regulate the pathogenesis of childhood obesity via the MAPK signaling pathway. J. Pediatr. Endocrinol. Metab. 2019, 32, 1327–1339. [Google Scholar] [CrossRef]
- Benite-Ribeiro, S.A.; Putt, D.A.; Soares-Filho, M.C.; Santos, J.M. The link between hypothalamic epigenetic modifications and long-term feeding control. Appetite 2016, 107, 445–453. [Google Scholar] [CrossRef]
- Liao, J.; Huang, J.; Wang, S.; Xiang, M.; Wang, D.; Deng, H.; Yin, H.; Xu, F.; Hu, M. Effects of exercise and diet intervention on appetite-regulating hormones associated with miRNAs in obese children. Eat. Weight. Disord. 2020, 1–9. [Google Scholar] [CrossRef]
- Marzano, F.; Faienza, M.F.; Caratozzolo, M.F.; Brunetti, G.; Chiara, M.; Horner, D.S.; Annese, A.; D’Erchia, A.M.; Consiglio, A.; Pesole, G.; et al. Pilot study on circulating miRNA signature in children with obesity born small for gestational age and appropriate for gestational age. Pediatr. Obes. 2018, 13, 803–811. [Google Scholar] [CrossRef]
- Khalyfa, A.; Kheirandish-Gozal, L.; Bhattacharjee, R.; Khalyfa, A.A.; Gozal, D. Circulating microRNAs as Potential Biomarkers of Endothelial Dysfunction in Obese Children. Chest 2016, 149, 786–800. [Google Scholar] [CrossRef] [Green Version]
- International Association of Diabetes and Pregnancy Study Groups Consensus Panel; Metzger, B.E.; Gabbe, S.G.; Persson, B.; Buchanan, T.A.; Catalano, P.A.; Damm, P.; Dyer, A.R.; Leiva, A.D.; Hod, M.; et al. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care 2010, 33, 676–682. [Google Scholar] [CrossRef] [Green Version]
- ACOG Practice Bulletin No. 33. Diagnosis and Management of Preeclampsia and Eclampsia. Obstet. Gynecol. 2002, 99, 159–167. [CrossRef]
- Figueras, F.; Gratacos, E. Stage-based approach to the management of fetal growth restriction. Prenat. Diagn. 2014, 34, 655–659. [Google Scholar] [CrossRef] [PubMed]
- Baschat, A.A. Neurodevelopment following fetal growth restriction and its relationship with antepartum parameters of placental dysfunction. Ultrasound Obstet. Gynecol. 2011, 37, 501–514. [Google Scholar] [CrossRef] [PubMed]
- Nardozza, L.M.M.; Caetano, A.C.R.; Zamarian, A.C.P.; Mazzola, J.B.; Silva, C.P.; Marçal, V.M.G.; Lobo, T.F.; Peixoto, A.B.; Júnior, E.A. Fetal growth restriction: Current knowledge. Arch. Gynecol. Obstet. 2017, 295, 1061–1077. [Google Scholar] [CrossRef]
- Goldenberg, R.L.; Culhane, J.F.; Iams, J.D.; Romero, R. Epidemiology and causes of preterm birth. Lancet 2008, 371, 75–84. [Google Scholar] [CrossRef]
- Moutquin, J.M.; Milot Roy, V.; Irion, O. Preterm prevention: Effectivenss of current strategies. J. Soc. Obstet. Gynaecol. Can. 1996, 18, 571–588. [Google Scholar] [CrossRef]
- Romero, R.; Espinoza, J.; Kusanovic, J.P.; Gotsch, F.; Hassan, S.; Erez, O.; Chaiworapongsa, T.; Mazor, M. The preterm parturition syndrome. BJOG 2006, 113, 17–42. [Google Scholar] [CrossRef]
- National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics 2004, 114, 555–576. [Google Scholar] [CrossRef]
- Livak, K.J.; Schmittgen, T.D. Analysis of relative gene expression data using real-time quantitative PCR and the 2(-Delta Delta C(T)) method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef]
- Vandesompele, J.; De Preter, K.; Pattyn, F.; Poppe, B.; Van Roy, N.; De Paepe, A.; Speleman, F. Accurate normalization of real-time quantitative RT-PCR data by geometric averaging of multiple internal control genes. Genome Biol. 2002, 3, 0034. [Google Scholar] [CrossRef] [Green Version]
- Shapiro, S.S.; Wilk, M.B. An analysis of variance test for normality (complete samples). Biometrika 1965, 52, 591–611. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| NP (n = 92) | PE (n = 135) | FGR (n = 35) | GH (n = 53) | GDM (n = 118) | PTB (n = 33) | PPROM (n = 37) | p-Value 1 | p-Value 2 | p-Value 3 | p-Value 4 | p-Value 5 | p-Value 6 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| At follow-up | |||||||||||||
| Age (years) | 5 (3–11) | 5 (3–11) | 4 (3–10) | 5 (3–10) | 5 (3–10) | 5 (3–8) | 5 (3–9) | 1.000 | 0.302 | 1.000 | 1.000 | 1.000 | 1.000 |
| Height (cm) | 116.5 (98–153) | 114.0 (97–155) | 106.0 (93–152) | 112.0 (96–159.5) | 113.75 (98–153) | 115.0 (101–138) | 113.5 (102–145) | 1.000 | <0.001 | 1.000 | 1.000 | 1.000 | 1.000 |
| Weight (kg) | 21.25 14–40.8) | 19.25 (11.85–54.9) | 16.00 (12–37) | 19.70 (14–47.5) | 19.50 (14.4–47.1) | 19.70 (14.1–29.6) | 20.20 (14.7–47.9) | 0.331 | <0.001 | 1.000 | 1.000 | 1.000 | 1.000 |
| BMI (kg/m2) | 15.54 (13.22–20) | 14.90 (12.34–22.81) | 14.24 (12.7–19.24) | 15.42 (13.42–19.7) | 15.32 (12.97–20.08) | 14.75 (12.09–19.89) | 15.86 (13.23–26.28) | 0.399 | <0.001 | 1.000 | 1.000 | 0.461 | 1.000 |
| Systolic BP (mmHg) | 100.5 (84–123) | 99 (84–132) | 97 (82–123) | 99 (80–129) | 100 (82–125) | 100 (87–118) | 102 (88–125) | 1.000 | 0.812 | 1.000 | 1.000 | 1.000 | 1.000 |
| Diastolic BP (mmHg) | 61 (38–81) | 61 (41–88) | 60 (42–73) | 62 (49–83) | 61 (64–122) | 61 (43–72) | 64 (48–76) | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 |
| Heart rate (n/min) | 90 (51–120) | 92 (64–117) | 95.5 (62–112) | 94 (65–129) | 97 (64–122) | 95 (76–120) | 96 (74–114) | 1.000 | 1.000 | 1.000 | 0.002 | 0.331 | 0.551 |
| Abnormal echocardiographic findings | |||||||||||||
| Yes | 17 (18.48%) | 18 (13.33%) | 9 (25.71%) | 12 (22.64%) | 42 (35.59%) | 10 (30.30%) | 15 (40.54%) | 0.292 | 0.367 | 0.546 | 0.006 | 0.157 | 0.009 |
| No | 75 (81.52%) | 117 (86.66%) | 26 (74.29%) | 41 (77.36%) | 76 (64.41%) | 23 (69.70%) | 22 (59.46%) | ||||||
| During gestation | |||||||||||||
| Maternal age at delivery (years) | 32 (20–46) | 32 (21–44) | 32 (22–41) | 32 (27–51) | 34 (27–45) | 32 (20–39) | 32 (22–42) | 1.000 | 1.000 | 1.000 | 0.569 | 1.000 | 1.000 |
| GA at delivery (weeks) | 39.86 (37.71–41.86) | 35.86 (26–41.72) | 35.14 (28–41) | 38.68 (33.43–41.28) | 39.57 (37–41.18) | 31.0 (24–36.43) | 33.43 (24.71–35.86) | <0.001 | <0.001 | 0.002 | 1.000 | <0.001 | <0.001 |
| Mode of delivery | |||||||||||||
| Vaginal | 81 (88.04%) | 15 (11.11%) | 6 (17.14%) | 24 (45.28%) | 75 (63.56%) | 23 (69.70%) | 17 (45.95%) | <0.001 | <0.001 | <0.001 | <0.001 | 0.016 | <0.001 |
| CS | 11 (11.96%) | 120 (88.88%) | 29 (82.86%) | 29 (54.72%) | 43 (36.44%) | 10 (30.30%) | 20 (54.05%) | ||||||
| Fetal birth weight (g) | 3410 (2530–4450) | 2360 (660–4490) | 1630 (650–3010) | 3150 (1940–4310) | 3485 (2700–4400) | 1570 (542–2820) | 2100 (600–2710) | <0.001 | <0.001 | 0.318 | 1.000 | <0.001 | <0.001 |
| Fetal sex | |||||||||||||
| Boy | 47 (51.09%) | 57 (42.22%) | 18 (51.43%) | 26 (49.06%) | 74 (62.71%) | 20 (60.60%) | 15 (40.54%) | 0.188 | 0.973 | 0.814 | 0.091 | 0.347 | 0.278 |
| Girl | 45 (48.91%) | 78 (57.77%) | 17 (48.57%) | 27 (50.94%) | 44 (37.29%) | 13 (39.40%) | 22 (59.46%) | ||||||
| Primiparity | |||||||||||||
| Yes | 49 (53.26%) | 109 (80.74%) | 34 (97.14%) | 36 (67.92%) | 54 (45.76%) | 23 (69.70%) | 28 (75.68%) | <0.001 | <0.001 | 0.084 | 0.281 | 0.101 | 0.019 |
| No | 43 (46.74%) | 26 (19.26%) | 1 (2.86%) | 17 (32.08%) | 64 (54.24%) | 10 (30.30%) | 9 (24.32%) | ||||||
| Birth order of index pregnancy | |||||||||||||
| 1st | 39 (42.39%) | 87 (64.44%) | 29 (82.86%) | 28 (52.83%) | 42 (35.59%) | 14 (42.42%) | 17 (45.95%) | 0.007 | <0.001 | 0.471 | 0.179 | 0.202 | 0.790 |
| 2nd | 34 (36.96%) | 28 (20.74%) | 2 (5.71%) | 13 (24.53%) | 45 (38.14%) | 9 (27.27%) | 12 (32.43%) | ||||||
| 3rd | 15 (16.30%) | 13 (9.63%) | 2 (5.71%) | 9 (16.98%) | 16 (13.56%) | 5 (15.15%) | 5 (13.51%) | ||||||
| 4th+ | 4 (4.35%) | 7 (5.19%) | 2 (5.71%) | 3 (5.66%) | 15 (12.71%) | 5 (15.15%) | 3 (8.11%) | ||||||
| Infertility treatment | |||||||||||||
| Yes | 3 (3.26%) | 34 (25.19%) | 9 (25.71%) | 7 (13.21%) | 16 (13.56%) | 4 (12.12%) | 6 (16.22%) | <0.001 | <0.001 | 0.023 | 0.010 | 0.058 | 0.009 |
| No | 89 (96.74%) | 101 (74.81%) | 26 (74.29%) | 46 (86.79%) | 102 (86.44%) | 29 (87.88%) | 31 (83.78%) | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hromadnikova, I.; Kotlabova, K.; Krofta, L.; Sirc, J. Association Analysis in Children Born from Normal and Complicated Pregnancies—Cardiovascular Disease Associated microRNAs and the Incidence of Prehypertension/Hypertension, Overweight/Obesity, Valve Problems and Heart Defects. Int. J. Mol. Sci. 2020, 21, 8413. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21218413
Hromadnikova I, Kotlabova K, Krofta L, Sirc J. Association Analysis in Children Born from Normal and Complicated Pregnancies—Cardiovascular Disease Associated microRNAs and the Incidence of Prehypertension/Hypertension, Overweight/Obesity, Valve Problems and Heart Defects. International Journal of Molecular Sciences. 2020; 21(21):8413. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21218413
Chicago/Turabian StyleHromadnikova, Ilona, Katerina Kotlabova, Ladislav Krofta, and Jan Sirc. 2020. "Association Analysis in Children Born from Normal and Complicated Pregnancies—Cardiovascular Disease Associated microRNAs and the Incidence of Prehypertension/Hypertension, Overweight/Obesity, Valve Problems and Heart Defects" International Journal of Molecular Sciences 21, no. 21: 8413. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21218413