Increased Stromal Infiltrating Lymphocytes Are Associated with the Risk of Disease Progression in Mesenchymal Circulating Tumor Cell-Positive Primary Breast Cancer Patients

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
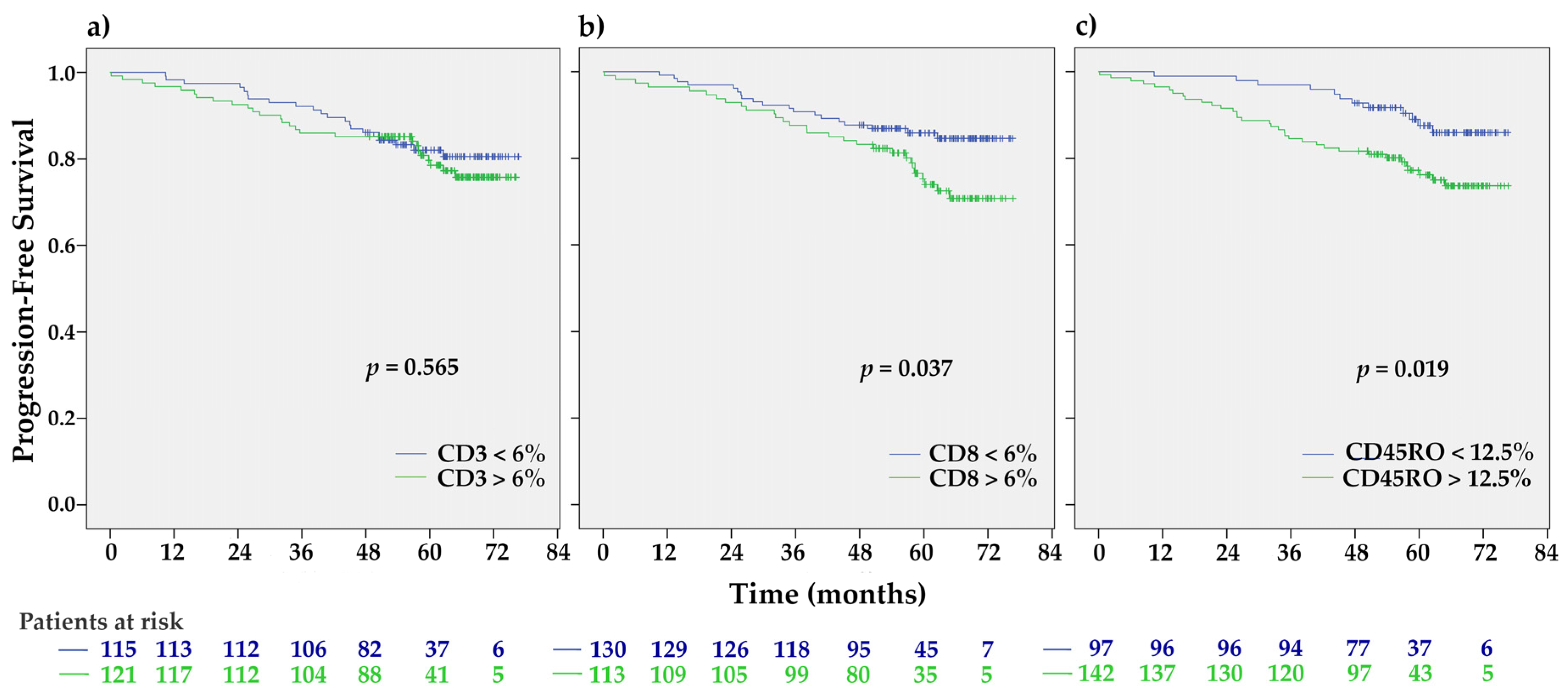
2.1. Association of TILs with Clinical Characteristics and Progression-Free Survival
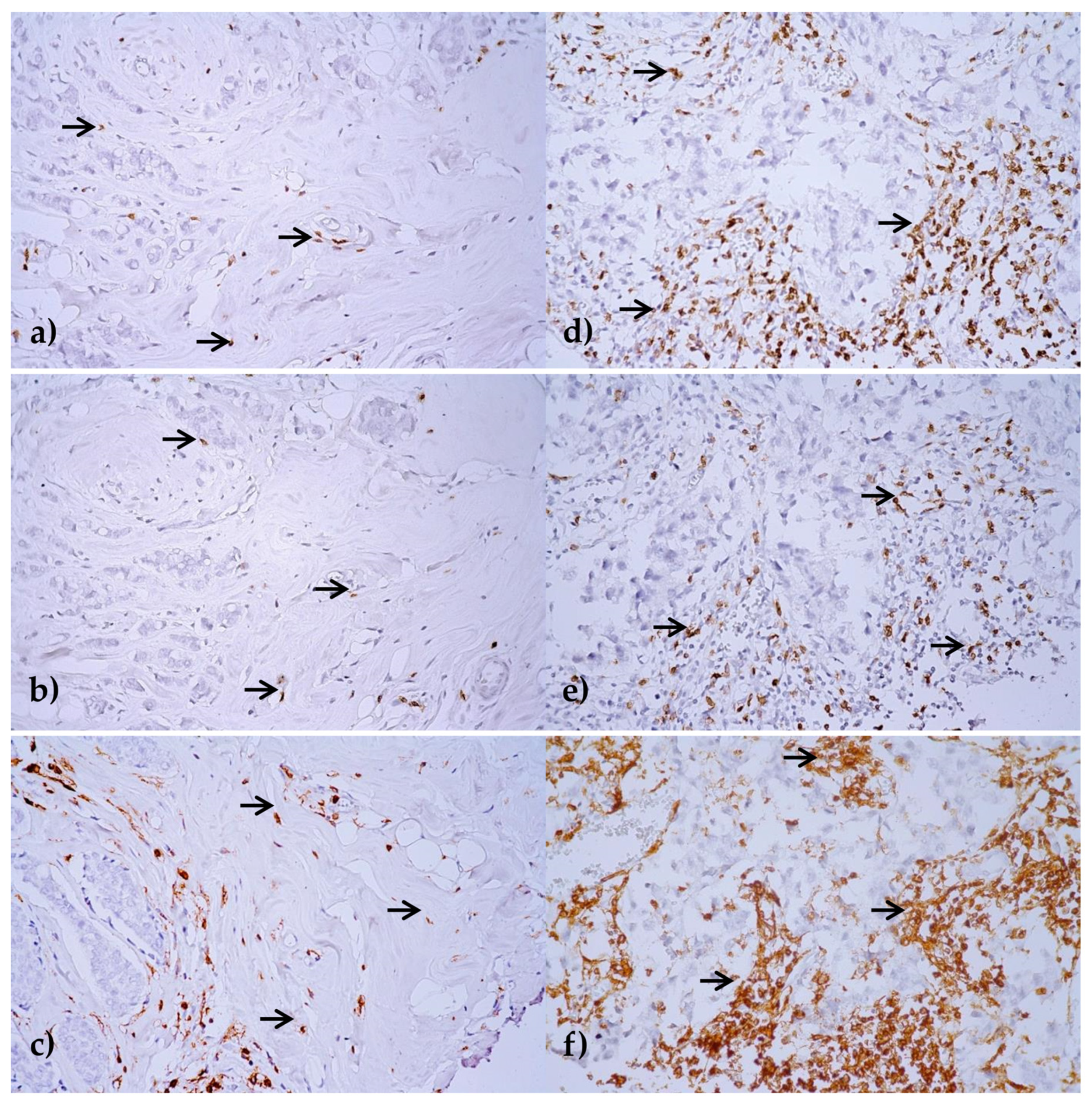
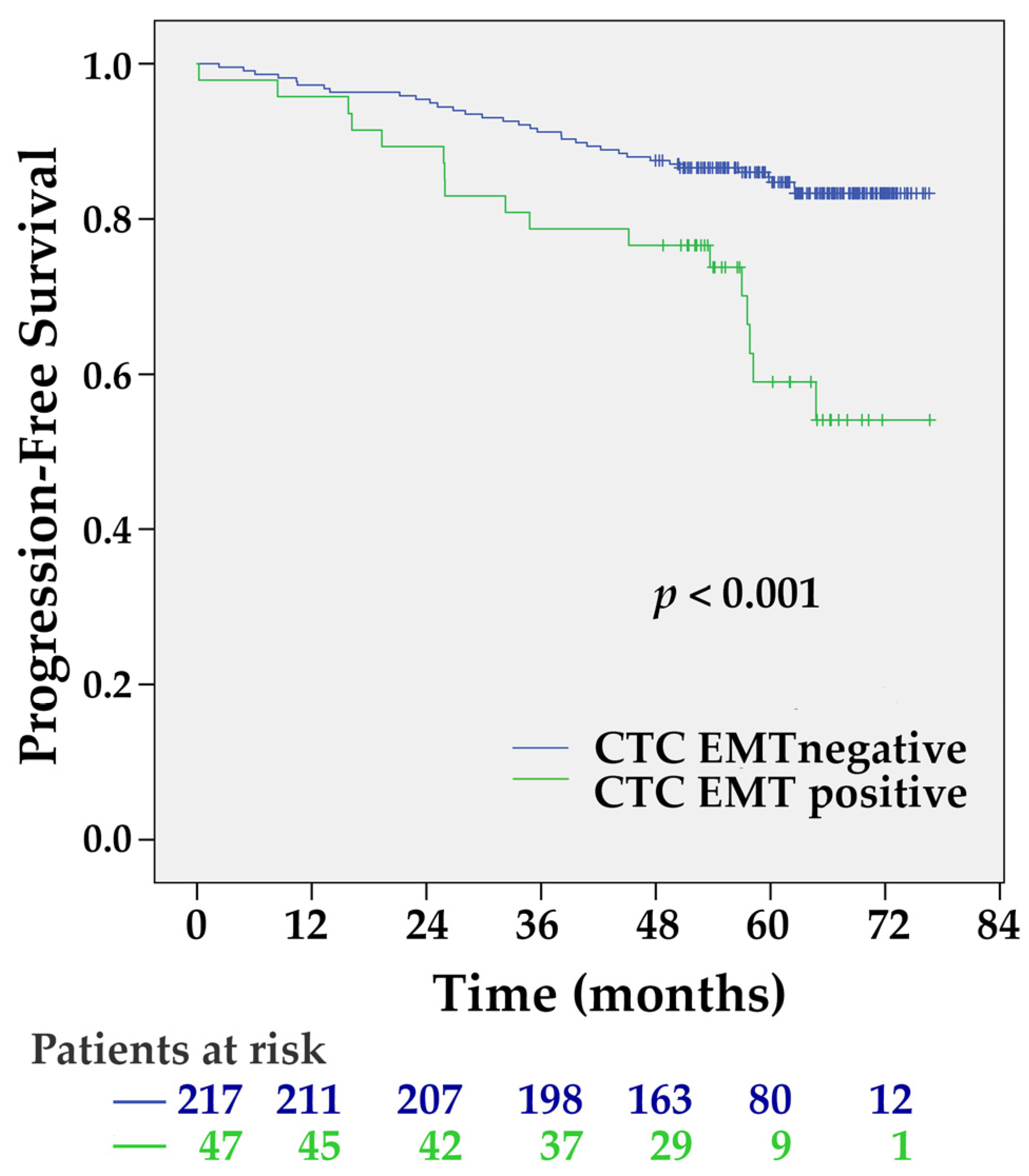
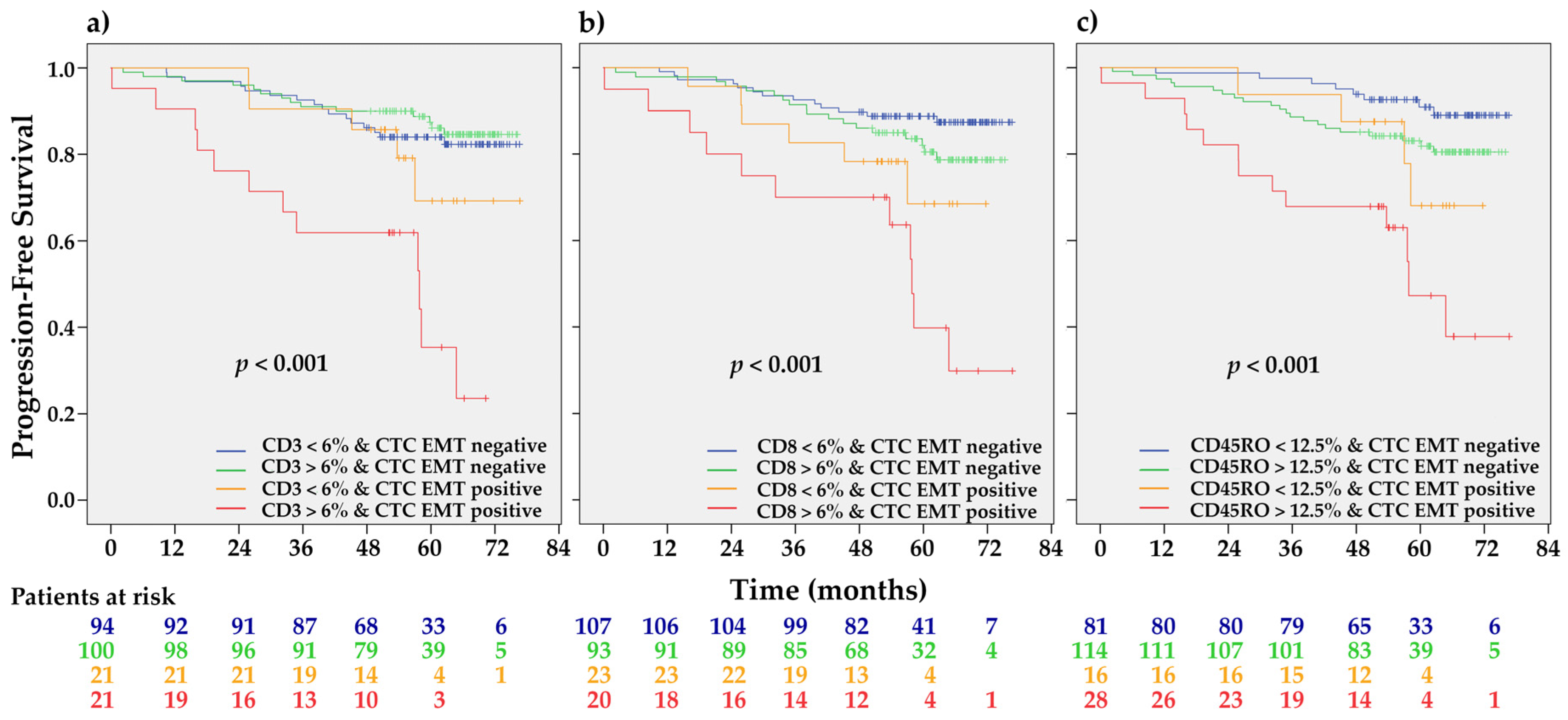
2.2. Association between TILs and CTCs and Their Prognostic Significance
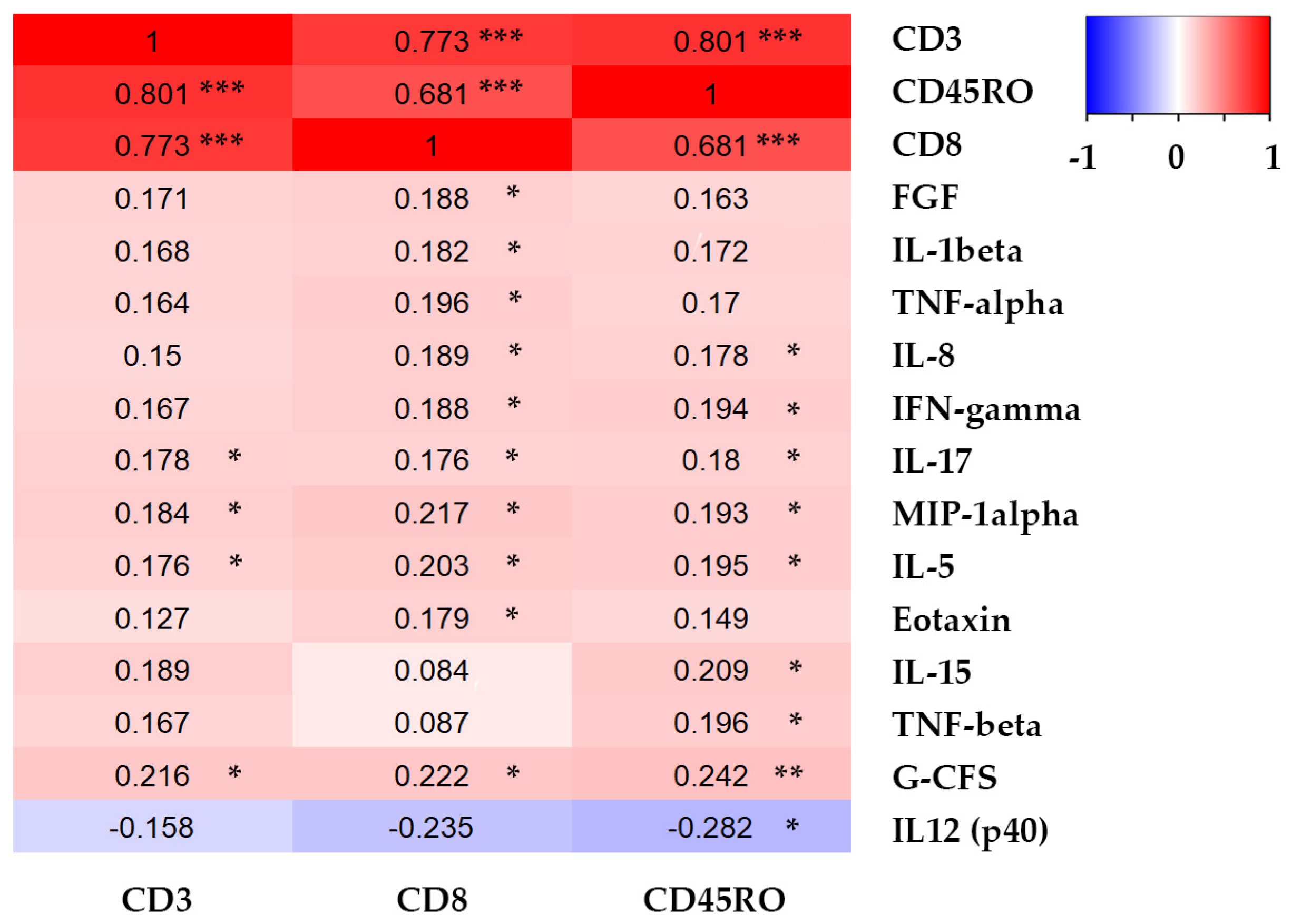
2.3. Association between TIL Infiltration and Plasma Cytokine Levels
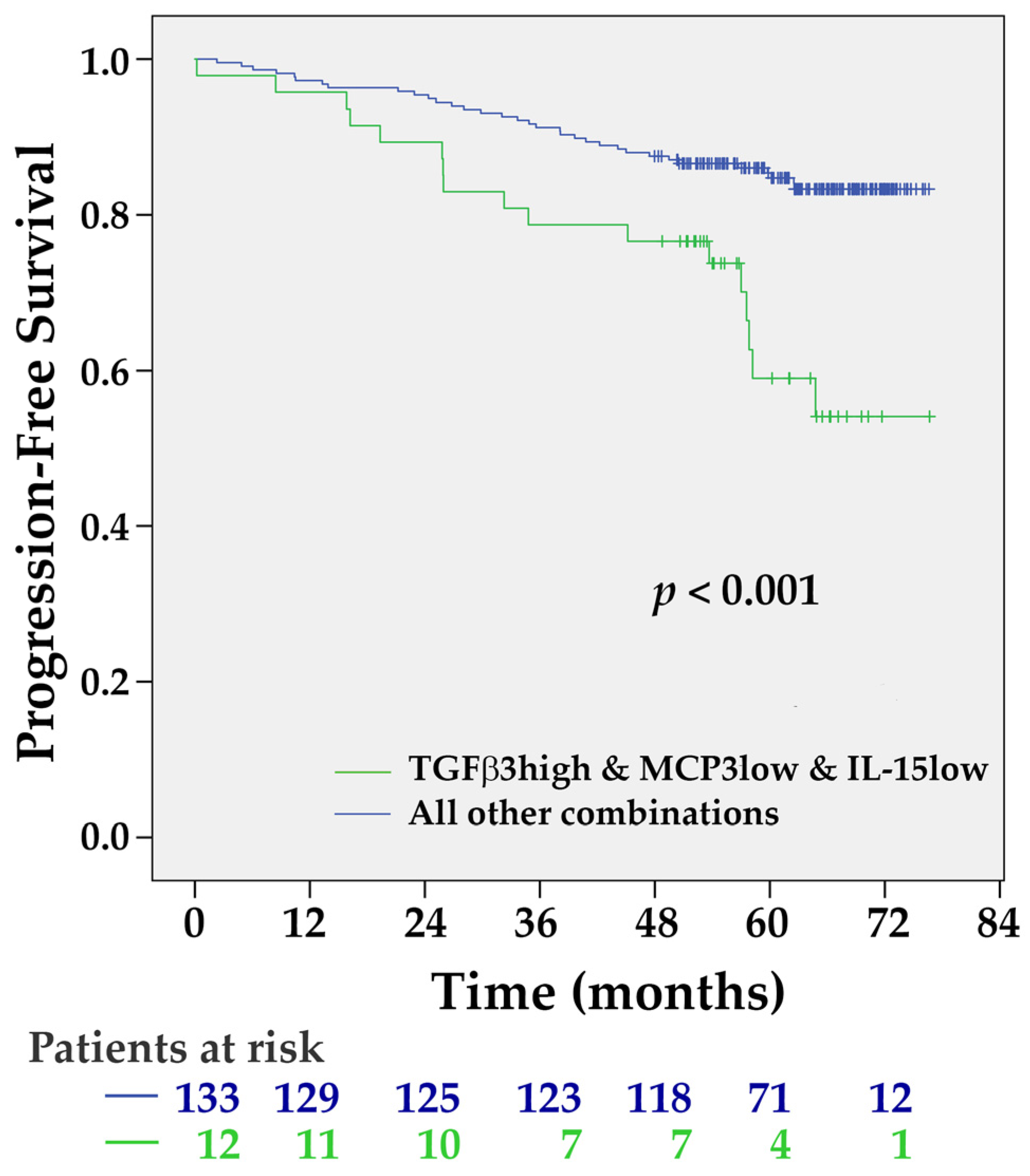
2.4. Variables with the Most Significant Impact on Progression-Free Survival
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Detection of CTCs
4.3. Tumor Pathology
4.4. Plasma Cytokines Assessment
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| BC | Breast cancer |
| CAF | Cancer-associated fibroblast |
| CTC | Circulating tumor cell |
| ECM | Extracellular matrix |
| EMT | Epithelial-mesenchymal transition |
| EpCAM | Epithelial cell adhesion molecule |
| Basic FGF | basic fibroblast growth factor |
| G-CSF | Granulocyte colony-stimulating factor |
| IDC | Invasive ductal carcinoma |
| IFN-gamma | Interferon gamma |
| IL | Interleukin |
| LVI | Lymphovascular invasion |
| MCP-3 | Monocyte chemotactic protein 3 |
| MDSC | Myeloid-derived suppressor cell |
| MET | Mesenchymal-epithelial transition |
| MIP-1alpha | Macrophage inflammatory protein-1α |
| OS | Overall survival |
| PFS | Progression-free survival |
| TAM | Tumor-associated macrophage |
| TGF-beta | Transforming growth factor-beta |
| TIL | Tumor-infiltrating lymphocyte |
| TNF-alpha | Tumor necrosis factor-alpha |
| TNF-beta | Tumor necrosis factor-beta |
References
- Harbeck, N.; Penault-Llorca, F.; Cortes, J.; Gnant, M.; Houssami, N.; Poortmans, P.; Ruddy, K.; Tsang, J.; Cardoso, F. Breast cancer. Nat. Rev. Dis. Primers 2019, 5, 66. [Google Scholar] [CrossRef]
- Loi, S.; Sirtaine, N.; Piette, F.; Salgado, R.; Viale, G.; Van Eenoo, F.; Rouas, G.; Francis, P.; Crown, J.P.; Hitre, E.; et al. Prognostic and predictive value of tumor-infiltrating lymphocytes in a phase III randomized adjuvant breast cancer trial in node-positive breast cancer comparing the addition of docetaxel to doxorubicin with doxorubicin-based chemotherapy: BIG 02-98. J. Clin. Oncol. 2013, 31, 860–867. [Google Scholar] [CrossRef]
- Althobiti, M.; Aleskandarany, M.A.; Joseph, C.; Toss, M.; Mongan, N.; Diez-Rodriguez, M.; Nolan, C.C.; Ashankyty, I.; Ellis, I.O.; Green, A.R.; et al. Heterogeneity of tumour-infiltrating lymphocytes in breast cancer and its prognostic significance. Histopathology 2018, 73, 887–896. [Google Scholar] [CrossRef]
- Adams, S.; Gray, R.J.; Demaria, S.; Goldstein, L.; Perez, E.A.; Shulman, L.N.; Martino, S.; Wang, M.; Jones, V.E.; Saphner, T.J.; et al. Prognostic value of tumor-infiltrating lymphocytes in triple-negative breast cancers from two phase III randomized adjuvant breast cancer trials: ECOG 2197 and ECOG 1199. J. Clin. Oncol. 2014, 32, 2959–2966. [Google Scholar] [CrossRef]
- Ali, H.R.; Provenzano, E.; Dawson, S.J.; Blows, F.M.; Liu, B.; Shah, M.; Earl, H.M.; Poole, C.J.; Hiller, L.; Dunn, J.A.; et al. Association between CD8+ T-cell infiltration and breast cancer survival in 12,439 patients. Ann. Oncol. 2014, 25, 1536–1543. [Google Scholar] [CrossRef]
- Loi, S.; Michiels, S.; Salgado, R.; Sirtaine, N.; Jose, V.; Fumagalli, D.; Kellokumpu-Lehtinen, P.L.; Bono, P.; Kataja, V.; Desmedt, C.; et al. Tumor infiltrating lymphocytes are prognostic in triple negative breast cancer and predictive for trastuzumab benefit in early breast cancer: Results from the FinHER trial. Ann. Oncol. 2014, 25, 1544–1550. [Google Scholar] [CrossRef]
- Ingold Heppner, B.; Untch, M.; Denkert, C.; Pfitzner, B.M.; Lederer, B.; Schmitt, W.; Eidtmann, H.; Fasching, P.A.; Tesch, H.; Solbach, C.; et al. Tumor-Infiltrating Lymphocytes: A Predictive and Prognostic Biomarker in Neoadjuvant-Treated HER2-Positive Breast Cancer. Clin. Cancer Res. 2016, 22, 5747–5754. [Google Scholar] [CrossRef] [Green Version]
- Issa-Nummer, Y.; Loibl, S.; von Minckwitz, G.; Denkert, C. Tumor-infiltrating lymphocytes in breast cancer: A new predictor for responses to therapy. Oncoimmunology 2014, 3, e27926. [Google Scholar] [CrossRef]
- Liu, J.; Xu, Y.; Yu, M.; Liu, Z.; Xu, Y.; Ma, G.; Zhou, W.; Kong, P.; Ling, L.; Wang, S.; et al. Increased Stromal Infiltrating Lymphocytes are Associated with Circulating Tumor Cells and Metastatic Relapse in Breast Cancer Patients After Neoadjuvant Chemotherapy. Cancer Manag. Res. 2019, 11, 10791–10800. [Google Scholar] [CrossRef]
- Weigelt, B.; Bosma, A.J.; Hart, A.A.; Rodenhuis, S.; van’t Veer, L.J. Marker genes for circulating tumour cells predict survival in metastasized breast cancer patients. Br. J. Cancer 2003, 88, 1091–1094. [Google Scholar] [CrossRef] [Green Version]
- Cristofanilli, M.; Budd, G.T.; Ellis, M.J.; Stopeck, A.; Matera, J.; Miller, M.C.; Reuben, J.M.; Doyle, G.V.; Allard, W.J.; Terstappen, L.W.; et al. Circulating tumor cells, disease progression, and survival in metastatic breast cancer. N. Engl. J. Med. 2004, 351, 781–791. [Google Scholar] [CrossRef] [Green Version]
- Molloy, T.J.; Bosma, A.J.; Baumbusch, L.O.; Synnestvedt, M.; Borgen, E.; Russnes, H.G.; Schlichting, E.; van’t Veer, L.J.; Naume, B. The prognostic significance of tumour cell detection in the peripheral blood versus the bone marrow in 733 early-stage breast cancer patients. Breast Cancer Res. 2011, 13, R61. [Google Scholar] [CrossRef] [Green Version]
- Krawczyk, N.; Meier-Stiegen, F.; Banys, M.; Neubauer, H.; Ruckhaeberle, E.; Fehm, T. Expression of stem cell and epithelial-mesenchymal transition markers in circulating tumor cells of breast cancer patients. BioMed Res. Int. 2014, 2014, 415721. [Google Scholar] [CrossRef]
- Mego, M.; Karaba, M.; Minarik, G.; Benca, J.; Silvia, J.; Sedlackova, T.; Manasova, D.; Kalavska, K.; Pindak, D.; Cristofanilli, M.; et al. Circulating Tumor Cells With Epithelial-to-mesenchymal Transition Phenotypes Associated With Inferior Outcomes in Primary Breast Cancer. Anticancer Res. 2019, 39, 1829–1837. [Google Scholar] [CrossRef]
- Liu, M.C.; Mego, M.; Nakamura, S.; Nole, F.; Pierga, J.; Toi, M. Clinical validity of circulating tumor cell (CTC) enumeration in 841 subjects with metastatic breast cancer (MBC). J. Clin. Oncol. 1059, 29 (Suppl. 15), 10592. [Google Scholar] [CrossRef]
- Bidard, F.C.; Peeters, D.J.; Fehm, T.; Nole, F.; Gisbert-Criado, R.; Mavroudis, D.; Grisanti, S.; Generali, D.; Garcia-Saenz, J.A.; Stebbing, J.; et al. Clinical validity of circulating tumour cells in patients with metastatic breast cancer: A pooled analysis of individual patient data. Lancet. Oncol. 2014, 15, 406–414. [Google Scholar] [CrossRef]
- Beerling, E.; Seinstra, D.; de Wit, E.; Kester, L.; van der Velden, D.; Maynard, C.; Schäfer, R.; van Diest, P.; Voest, E.; van Oudenaarden, A.; et al. Plasticity between Epithelial and Mesenchymal States Unlinks EMT from Metastasis-Enhancing Stem Cell Capacity. Cell Rep. 2016, 14, 2281–2288. [Google Scholar] [CrossRef] [Green Version]
- Papadaki, M.A.; Stoupis, G.; Theodoropoulos, P.A.; Mavroudis, D.; Georgoulias, V.; Agelaki, S. Circulating tumor cells with stemness and epithelial-to-mesenchymal transition features are chemoresistant and predictive of poor outcome in metastatic breast cancer. Mol. Cancer Ther. 2019, 18, 437–447. [Google Scholar] [CrossRef] [Green Version]
- Guan, X.; Ma, F.; Li, C.; Wu, S.; Hu, S.; Huang, J.; Sun, X.; Wang, J.; Luo, Y.; Cai, R. The prognostic and therapeutic implications of circulating tumor cell phenotype detection based on epithelial–mesenchymal transition markers in the first-line chemotherapy of HER2-negative metastatic breast cancer. Cancer Commun. 2019, 39, 1–10. [Google Scholar] [CrossRef]
- Zhang, S.; Wu, T.; Peng, X.; Liu, J.; Liu, F.; Wu, S.; Liu, S.; Dong, Y.; Xie, S.; Ma, S. Mesenchymal phenotype of circulating tumor cells is associated with distant metastasis in breast cancer patients. Cancer Manag. Res. 2017, 9, 691. [Google Scholar] [CrossRef] [Green Version]
- Miklikova, S.; Minarik, G.; Sedlackova, T.; Plava, J.; Cihova, M.; Jurisova, S.; Kalavska, K.; Karaba, M.; Benca, J.; Smolkova, B.; et al. Inflammation-Based Scores Increase the Prognostic Value of Circulating Tumor Cells in Primary Breast Cancer. Cancers 2020, 12, 1134. [Google Scholar] [CrossRef]
- Aceto, N. Bring along your friends: Homotypic and heterotypic circulating tumor cell clustering to accelerate metastasis. Biomed. J. 2020, 43, 18–23. [Google Scholar] [CrossRef]
- Saini, M.; Szczerba, B.M.; Aceto, N. Circulating Tumor Cell-Neutrophil Tango along the Metastatic Process. Cancer Res. 2019, 79, 6067–6073. [Google Scholar] [CrossRef] [Green Version]
- Fridlender, Z.G.; Albelda, S.M. Tumor-associated neutrophils: Friend or foe? Carcinogenesis 2012, 33, 949–955. [Google Scholar] [CrossRef] [Green Version]
- Fares, J.; Fares, M.Y.; Khachfe, H.H.; Salhab, H.A.; Fares, Y. Molecular principles of metastasis: A hallmark of cancer revisited. Signal Transduct. Target. Ther. 2020, 5, 28. [Google Scholar] [CrossRef]
- Garner, H.; de Visser, K.E. Immune crosstalk in cancer progression and metastatic spread: A complex conversation. Nat. Rev. Immunol. 2020, 20, 483–497. [Google Scholar] [CrossRef]
- Jabeen, S.; Espinoza, J.A.; Torland, L.A.; Zucknick, M.; Kumar, S.; Haakensen, V.D.; Lüders, T.; Engebraaten, O.; Børresen-Dale, A.-L.; Kyte, J.A.; et al. Noninvasive profiling of serum cytokines in breast cancer patients and clinicopathological characteristics. Oncoimmunology 2018, 8, e1537691. [Google Scholar] [CrossRef] [Green Version]
- Aaltomaa, S.; Lipponen, P.; Eskelinen, M.; Kosma, V.M.; Marin, S.; Alhava, E.; Syrjanen, K. Lymphocyte infiltrates as a prognostic variable in female breast cancer. Eur. J. Cancer 1992, 28A, 859–864. [Google Scholar] [CrossRef]
- Dushyanthen, S.; Beavis, P.A.; Savas, P.; Teo, Z.L.; Zhou, C.; Mansour, M.; Darcy, P.K.; Loi, S. Relevance of tumor-infiltrating lymphocytes in breast cancer. BMC Med. 2015, 13, 202. [Google Scholar] [CrossRef] [Green Version]
- Denkert, C.; Loibl, S.; Noske, A.; Roller, M.; Muller, B.M.; Komor, M.; Budczies, J.; Darb-Esfahani, S.; Kronenwett, R.; Hanusch, C.; et al. Tumor-associated lymphocytes as an independent predictor of response to neoadjuvant chemotherapy in breast cancer. J. Clin. Oncol. 2010, 28, 105–113. [Google Scholar] [CrossRef]
- Kurozumi, S.; Matsumoto, H.; Kurosumi, M.; Inoue, K.; Fujii, T.; Horiguchi, J.; Shirabe, K.; Oyama, T.; Kuwano, H. Prognostic significance of tumour-infiltrating lymphocytes for oestrogen receptor-negative breast cancer without lymph node metastasis. Oncol. Lett. 2019, 17, 2647–2656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ravelli, A.; Roviello, G.; Cretella, D.; Cavazzoni, A.; Biondi, A.; Cappelletti, M.R.; Zanotti, L.; Ferrero, G.; Ungari, M.; Zanconati, F. Tumor-infiltrating lymphocytes and breast cancer: Beyond the prognostic and predictive utility. Tumor Biol. 2017, 39, 1010428317695023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ingangi, V.; Minopoli, M.; Ragone, C.; Motti, M.L.; Carriero, M.V. Role of Microenvironment on the Fate of Disseminating Cancer Stem Cells. Front. Oncol. 2019, 9, 82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salgado, R.; Denkert, C.; Demaria, S.; Sirtaine, N.; Klauschen, F.; Pruneri, G.; Wienert, S.; Van den Eynden, G.; Baehne, F.L.; Penault-Llorca, F.; et al. Harmonization of the evaluation of tumor infiltrating lymphocytes (TILs) in breast cancer: Recommendations by an international TILs-working group 2014. Ann. Oncol. 2015, 26, 259–271. [Google Scholar] [CrossRef] [PubMed]
- Loi, S.; Drubay, D.; Adams, S.; Pruneri, G.; Francis, P.A.; Lacroix-Triki, M.; Joensuu, H.; Dieci, M.V.; Badve, S.; Demaria, S.; et al. Tumor-Infiltrating Lymphocytes and Prognosis: A Pooled Individual Patient Analysis of Early-Stage Triple-Negative Breast Cancers. J. Clin. Oncol. 2019, 37, 559–569. [Google Scholar] [CrossRef]
- Rathore, A.S.; Kumar, S.; Konwar, R.; Makker, A.; Negi, M.P.S.; Goel, M.M. CD3+, CD4+ & CD8+ tumour infiltrating lymphocytes (TILs) are predictors of favourable survival outcome in infiltrating ductal carcinoma of breast. Indian J. Med. Res. 2014, 140, 361–369. [Google Scholar]
- Koletsa, T.; Kotoula, V.; Koliou, G.A.; Manousou, K.; Chrisafi, S.; Zagouri, F.; Sotiropoulou, M.; Pentheroudakis, G.; Papoudou-Bai, A.; Christodoulou, C.; et al. Prognostic impact of stromal and intratumoral CD3, CD8 and FOXP3 in adjuvantly treated breast cancer: Do they add information over stromal tumor-infiltrating lymphocyte density? Cancer Immunol. Immunother. 2020, 69, 1549–1564. [Google Scholar] [CrossRef]
- Burstein, H.J.; Curigliano, G.; Loibl, S.; Dubsky, P.; Gnant, M.; Poortmans, P.; Colleoni, M.; Denkert, C.; Piccart-Gebhart, M.; Regan, M. Estimating the benefits of therapy for early-stage breast cancer: The St. Gallen International Consensus Guidelines for the primary therapy of early breast cancer 2019. Ann. Oncol. 2019, 30, 1541–1557. [Google Scholar] [CrossRef] [Green Version]
- Kos, Z.; Roblin, E.; Kim, R.S.; Michiels, S.; Gallas, B.D.; Chen, W.; van de Vijver, K.K.; Goel, S.; Adams, S.; Demaria, S.; et al. Pitfalls in assessing stromal tumor infiltrating lymphocytes (sTILs) in breast cancer. NPJ Breast Cancer 2020, 6, 17. [Google Scholar] [CrossRef]
- Chebouti, I.; Bankfalvi, A.; Friedrich, C.; Kimmig, R.; Kasimir-Bauer, S. Association between tumor infiltrating immune cells, circulating tumor cells in blood and disseminated tumor cells in the bone marrow in patients with primary ovarian cancer. Cancer Res. 2015, 75, 369. [Google Scholar]
- Xue, D.; Xia, T.; Wang, J.; Chong, M.; Wang, S.; Zhang, C. Role of regulatory T cells and CD8(+) T lymphocytes in the dissemination of circulating tumor cells in primary invasive breast cancer. Oncol. Lett. 2018, 16, 3045–3053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mego, M.; Cholujova, D.; Minarik, G.; Sedlackova, T.; Gronesova, P.; Karaba, M.; Benca, J.; Cingelova, S.; Cierna, Z.; Manasova, D.; et al. CXCR4-SDF-1 interaction potentially mediates trafficking of circulating tumor cells in primary breast cancer. BMC Cancer 2016, 16, 127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zarzynska, J.M. Two faces of TGF-beta1 in breast cancer. Mediat. Inflamm. 2014, 2014, 141747. [Google Scholar] [CrossRef] [PubMed]
- Hao, Y.; Baker, D.; Ten Dijke, P. TGF-β-Mediated Epithelial-Mesenchymal Transition and Cancer Metastasis. Int. J. Mol. Sci. 2019, 20, 2767. [Google Scholar] [CrossRef] [Green Version]
- Panis, C.; Herrera, A.C.; Victorino, V.J.; Aranome, A.M.; Cecchini, R. Screening of circulating TGF-β levels and its clinicopathological significance in human breast cancer. Anticancer Res. 2013, 33, 737–742. [Google Scholar]
- Labelle, M.; Begum, S.; Hynes, R.O. Direct signaling between platelets and cancer cells induces an epithelial-mesenchymal-like transition and promotes metastasis. Cancer Cell 2011, 20, 576–590. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Cai, Y.; Liu, L.; Wu, Y.; Xiong, X. Crucial biological functions of CCL7 in cancer. PeerJ 2018, 6, e4928. [Google Scholar] [CrossRef]
- Carlsson, A.; Wingren, C.; Ingvarsson, J.; Ellmark, P.; Baldertorp, B.; Fernö, M.; Olsson, H.; Borrebaeck, C.A. Serum proteome profiling of metastatic breast cancer using recombinant antibody microarrays. Eur. J. Cancer 2008, 44, 472–480. [Google Scholar] [CrossRef]
- Kubo, H.; Mensurado, S.; Gonçalves-Sousa, N.; Serre, K.; Silva-Santos, B. Primary Tumors Limit Metastasis Formation through Induction of IL15-Mediated Cross-Talk between Patrolling Monocytes and NK Cells. Cancer Immunol. Res. 2017, 5, 812–820. [Google Scholar] [CrossRef] [Green Version]
- Jabri, B.; Abadie, V. IL-15 functions as a danger signal to regulate tissue-resident T cells and tissue destruction. Nat. Rev. Immunol. 2015, 15, 771–783. [Google Scholar] [CrossRef]
- Mego, M.; Mani, S.A.; Lee, B.N.; Li, C.; Evans, K.W.; Cohen, E.N.; Gao, H.; Jackson, S.A.; Giordano, A.; Hortobagyi, G.N.; et al. Expression of epithelial-mesenchymal transition-inducing transcription factors in primary breast cancer: The effect of neoadjuvant therapy. Int. J. Cancer 2012, 130, 808–816. [Google Scholar] [CrossRef] [PubMed]
- Lakhani, S.R.; Ellis, I.O.; Schnitt, S.J.; Tan, P.H.; van de Vijver, M.J. WHO Classification of Tumours of the Breast; IARC Press: Lyon, France, 2012. [Google Scholar]
- Baker, K.; Lachapelle, J.; Zlobec, I.; Bismar, T.A.; Terracciano, L.; Foulkes, W.D. Prognostic significance of CD8+ T lymphocytes in breast cancer depends upon both oestrogen receptor status and histological grade. Histopathology 2011, 58, 1107–1116. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Chen, X.; Zhou, E.; Chen, G.; Qian, K.; Wu, X.; Miao, X.; Tang, Z. Intratumoral CD8(+) cytotoxic lymphocyte is a favorable prognostic marker in node-negative breast cancer. PLoS ONE 2014, 9, e95475. [Google Scholar] [CrossRef] [PubMed]
- Mego, M.; Gao, H.; Cohen, E.N.; Anfossi, S.; Giordano, A.; Sanda, T.; Fouad, T.M.; De Giorgi, U.; Giuliano, M.; Woodward, W.A.; et al. Circulating Tumor Cells (CTC) Are Associated with Defects in Adaptive Immunity in Patients with Inflammatory Breast Cancer. J. Cancer 2016, 7, 1095–1104. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Categories | N | % | CD3 Mean% ± SD | p | CD8 Mean% ± SD | p | CD45RO Mean% ± SD | p |
|---|---|---|---|---|---|---|---|---|---|
| All patients | 282 | 100 | 13.00 ± 15.30 | 12.29 ± 14.89 | 30.48 ± 27.18 | ||||
| Age (years) | ≤50 | 65 | 23.0 | 15.38 ± 17.95 | 0.478 | 14.97 ± 17.71 | 0.405 | 34.28 ± 30.44 | 0.369 |
| >50 | 217 | 77.0 | 12.33 ± 14.46 | 11.45 ± 13.85 | 29.32 ± 26.08 | ||||
| T-stage | T1 | 193 | 68.4 | 11.14 ± 13.16 | 0.101 | 11.81 ± 14.61 | 0.368 | 27.60 ± 24.60 | 0.086 |
| T2 and more | 89 | 31.6 | 16.97 ± 18.58 | 13.29 ± 15.52 | 36.51 ± 31.22 | ||||
| Histology | IDC | 247 | 87.6 | 13.86 ± 15.87 | 0.020 | 13.18 ± 15.53 | 0.035 | 31.99 ± 27.66 | 0.016 |
| Others | 35 | 12.4 | 6.46 ± 7.35 | 5.68 ± 5.39 | 18.62 ± 19.63 | ||||
| Grade | Low and intermediate | 174 | 62.8 | 9.08 ± 11.38 | <0.001 | 10.13 ± 13.02 | 0.003 | 23.79 ± 22.66 | <0.001 |
| High | 103 | 37.2 | 19.88 ± 18.48 | 16.15 ± 17.10 | 42.05 ± 30.31 | ||||
| N stage | N0 | 180 | 64.3 | 12.27 ± 15.46 | 0.124 | 11.80 ± 15.05 | 0.247 | 28.61 ± 27.33 | 0.046 |
| N+ | 100 | 35.7 | 14.31 ± 15.13 | 12.91 ± 14.68 | 33.97 ± 27.00 | ||||
| LVI | Absent | 175 | 76.4 | 11.91 ± 14.88 | 0.068 | 11.95 ± 14.89 | 0.024 | 28.05 ± 26.19 | 0.034 |
| Present | 54 | 23.6 | 16.72 ± 17.27 | 14.94 ± 16.13 | 37.48 ± 29.43 | ||||
| HR status $ | Negative | 38 | 13.5 | 24.74 ± 19.34 | <0.001 | 18.19 ± 16.66 | 0.005 | 54.54 ± 29.85 | <0.001 |
| Positive | 244 | 86.5 | 11.251 ± 13.82 | 11.31 ± 14.39 | 26.43 ± 24.55 | ||||
| HER2 status | Negative | 242 | 85.8 | 12.00 ± 14.80 | 0.018 | 11.69 ± 14.70 | 0.061 | 28.63 ± 26.31 | 0.013 |
| Amplified | 40 | 14.2 | 18.43 ± 16.96 | 15.92 ± 15.72 | 41.49 ± 29.92 | ||||
| p53 | Negative | 177 | 63.0 | 11.27 ± 13.69 | 0.124 | 11.60 ± 14.96 | 0.227 | 28.92 ± 26.39 | 0.281 |
| Positive | 104 | 37.0 | 15.65 ± 17.35 | 13.52 ± 14.84 | 33.03 ± 28.52 | ||||
| bcl2 | Negative | 80 | 28.4 | 17.85 ± 18.90 | 0.033 | 14.08 ± 15.46 | 0.133 | 39.67 ± 31.88 | 0.008 |
| Positive | 202 | 71.6 | 11.10 ± 13.23 | 11.58 ± 14.65 | 26.90 ± 24.28 | ||||
| Ki-67 & | Low | 180 | 63.8 | 8.94 ± 11.35 | <0.001 | 10.36 ± 14.10 | 0.001 | 22.81 ± 21.67 | <0.001 |
| High | 102 | 36.2 | 19.83 ± 18.43 | 15.59 ± 15.70 | 43.56 ± 30.54 | ||||
| Tumor subtypes | Luminal A | 150 | 53.2 | 8.87 ± 10.90 | <0.001 | 10.53 ± 14.13 | 0.006 | 22.08 ± 20.80 | <0.001 |
| Luminal B | 60 | 21.3 | 13.35 ± 16.48 | 10.51 ± 13.54 | 30.39 ± 26.80 | ||||
| HER2 positive | 40 | 14.2 | 18.43 ± 16.96 | 15.92 ± 15.72 | 41.49 ± 29.92 | ||||
| Triple-negative | 32 | 11.3 | 24.38 ± 20.43 | 18.66 ± 17.38 | 53.06 ± 31.64 | ||||
| CTC EMT | Negative | 220 | 82.4 | 12.98 ± 15.33 | 0.806 | 12.47 ± 15.20 | 0.774 | 29.69 ± 27.23 | 0.414 |
| Positive | 47 | 17.6 | 13.07 ± 15.31 | 11.74 ± 14.60 | 31.55 ± 26.76 | ||||
| Cytokines * | Low risk | 133 | 91.7 | 12.54 ± 14.36 | 0.548 | 11.40 ± 13.58 | 0.056 | 27.77 ± 24.84 | 0.655 |
| High risk | 12 | 8.3 | 13.60 ± 19.64 | 9.40 ± 18.73 | 27.30 ± 31.98 |
| Model | Variable | HR | 95% CI | p |
|---|---|---|---|---|
| 1 | LN+ | 6.446 | 2.56–16.24 | <0.001 |
| Ki-67 > 20% | 12.00 | 4.22–34.11 | <0.001 | |
| Cytokines * | 5.928 | 2.12–16.58 | 0.001 | |
| CD3high and CTC EMT positivity | 5.277 | 2.09–13.30 | <0.001 | |
| 2 | LN+ | 4.256 | 1.79–10.10 | 0.001 |
| Ki-67 > 20% | 8.482 | 3.25–22.13 | <0.001 | |
| Cytokines * | 6.387 | 2.35–17.38 | <0.001 | |
| CD8high and CTC EMT positivity | 3.655 | 1.49–9.00 | 0.005 | |
| 3 | LN+ | 3.796 | 1.50–9.58 | 0.005 |
| Ki-67 > 20% | 7.251 | 2.59–20.30 | <0.001 | |
| Cytokines * | 5.172 | 1.80–14.87 | 0.002 | |
| CD45ROhigh and CTC EMT positivity | 4.922 | 1.83–13.23 | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smolkova, B.; Cierna, Z.; Kalavska, K.; Miklikova, S.; Plava, J.; Minarik, G.; Sedlackova, T.; Cholujova, D.; Gronesova, P.; Cihova, M.; et al. Increased Stromal Infiltrating Lymphocytes Are Associated with the Risk of Disease Progression in Mesenchymal Circulating Tumor Cell-Positive Primary Breast Cancer Patients. Int. J. Mol. Sci. 2020, 21, 9460. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21249460
Smolkova B, Cierna Z, Kalavska K, Miklikova S, Plava J, Minarik G, Sedlackova T, Cholujova D, Gronesova P, Cihova M, et al. Increased Stromal Infiltrating Lymphocytes Are Associated with the Risk of Disease Progression in Mesenchymal Circulating Tumor Cell-Positive Primary Breast Cancer Patients. International Journal of Molecular Sciences. 2020; 21(24):9460. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21249460
Chicago/Turabian StyleSmolkova, Bozena, Zuzana Cierna, Katarina Kalavska, Svetlana Miklikova, Jana Plava, Gabriel Minarik, Tatiana Sedlackova, Dana Cholujova, Paulina Gronesova, Marina Cihova, and et al. 2020. "Increased Stromal Infiltrating Lymphocytes Are Associated with the Risk of Disease Progression in Mesenchymal Circulating Tumor Cell-Positive Primary Breast Cancer Patients" International Journal of Molecular Sciences 21, no. 24: 9460. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21249460