Speckle Tracking Echocardiography: New Ways of Translational Approaches in Preeclampsia to Detect Cardiovascular Dysfunction

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
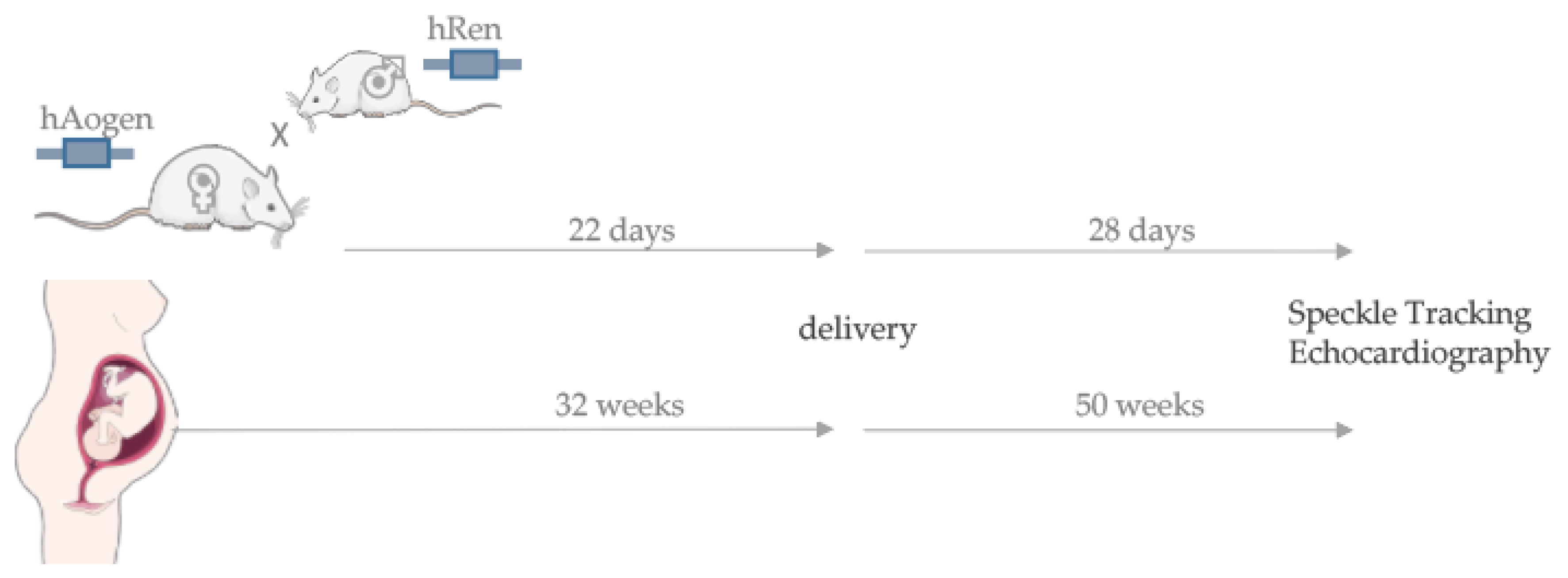
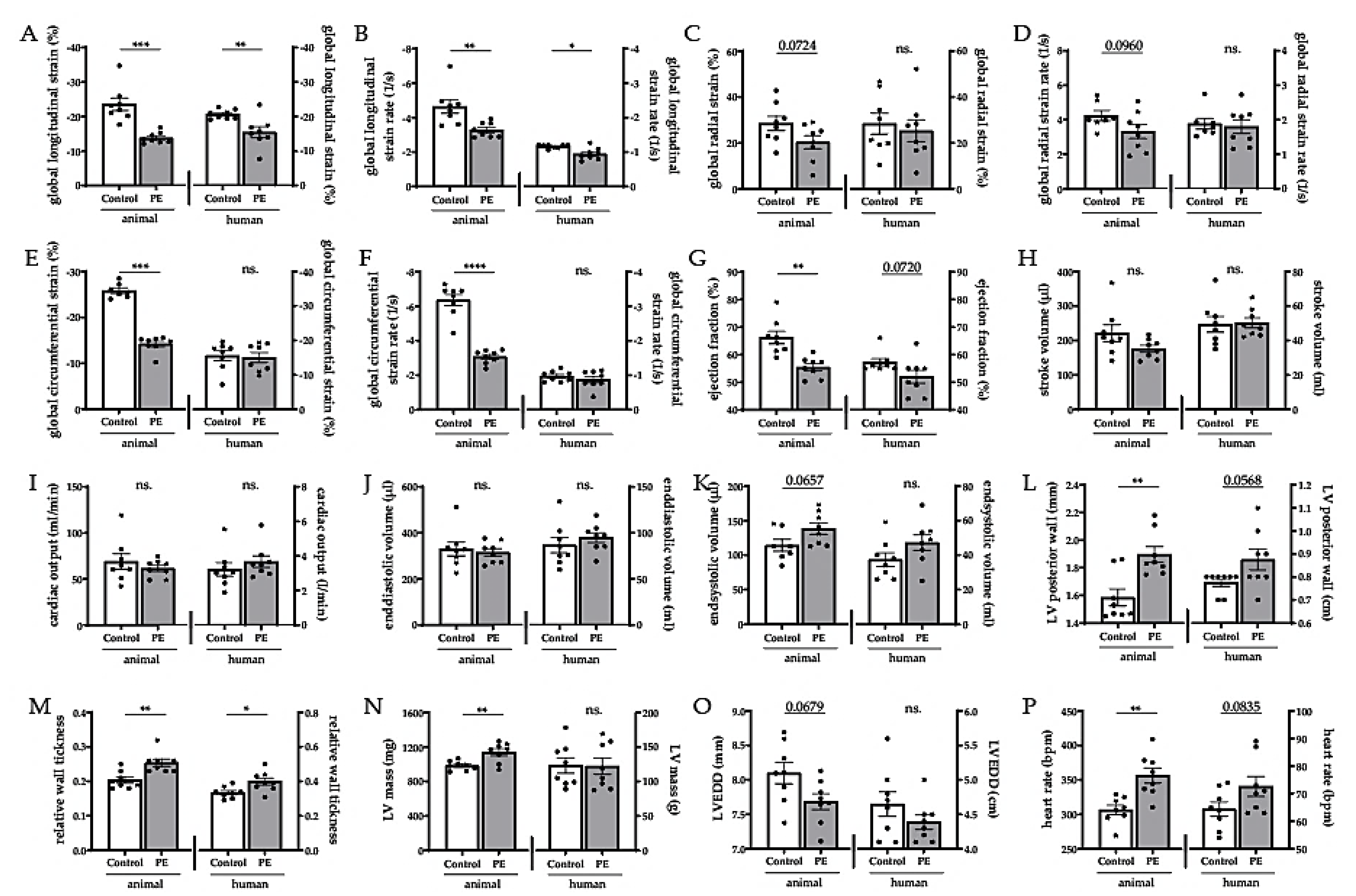
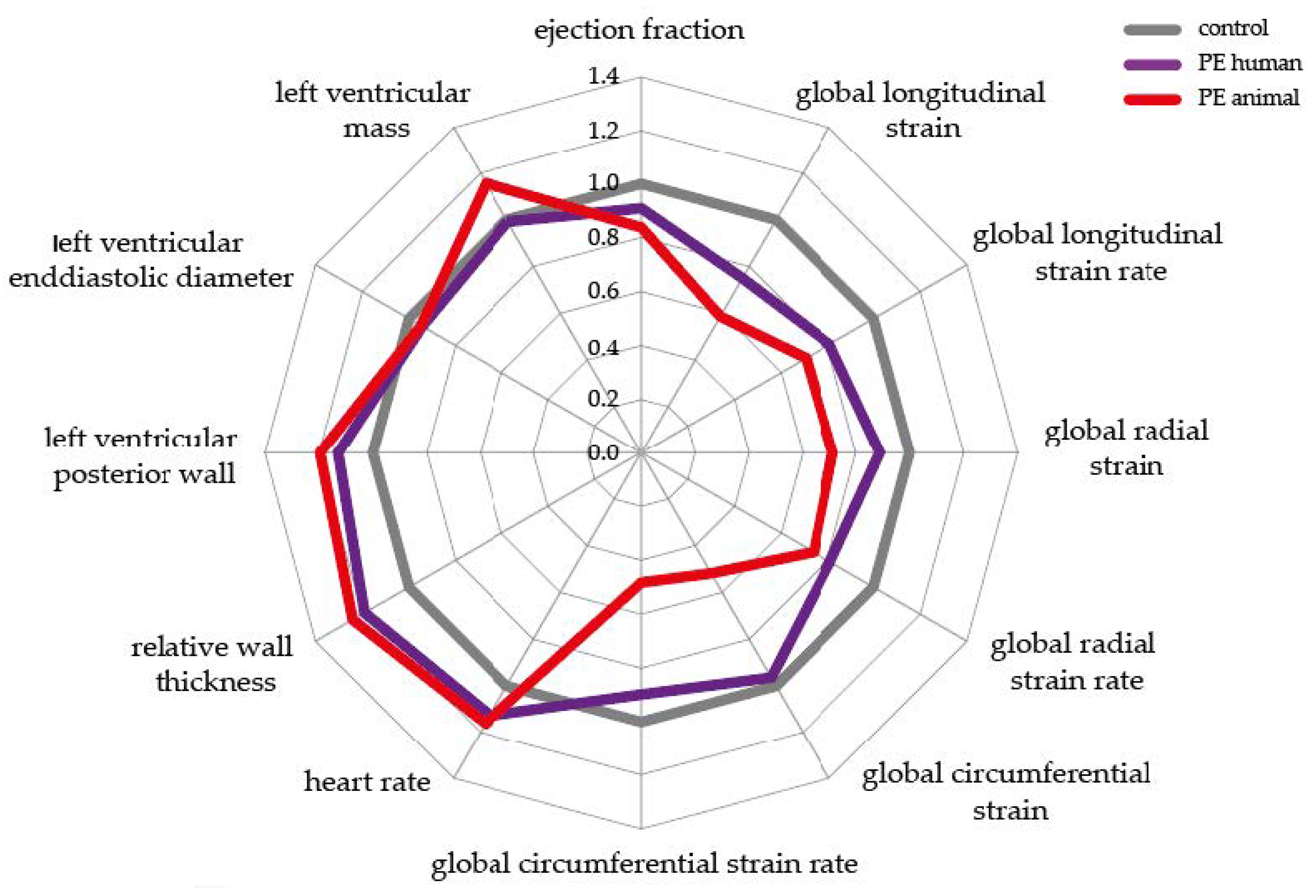
2.1. Speckle Tracking Echocardiography in the Transgenic Animal Model Simulates the Human Situation
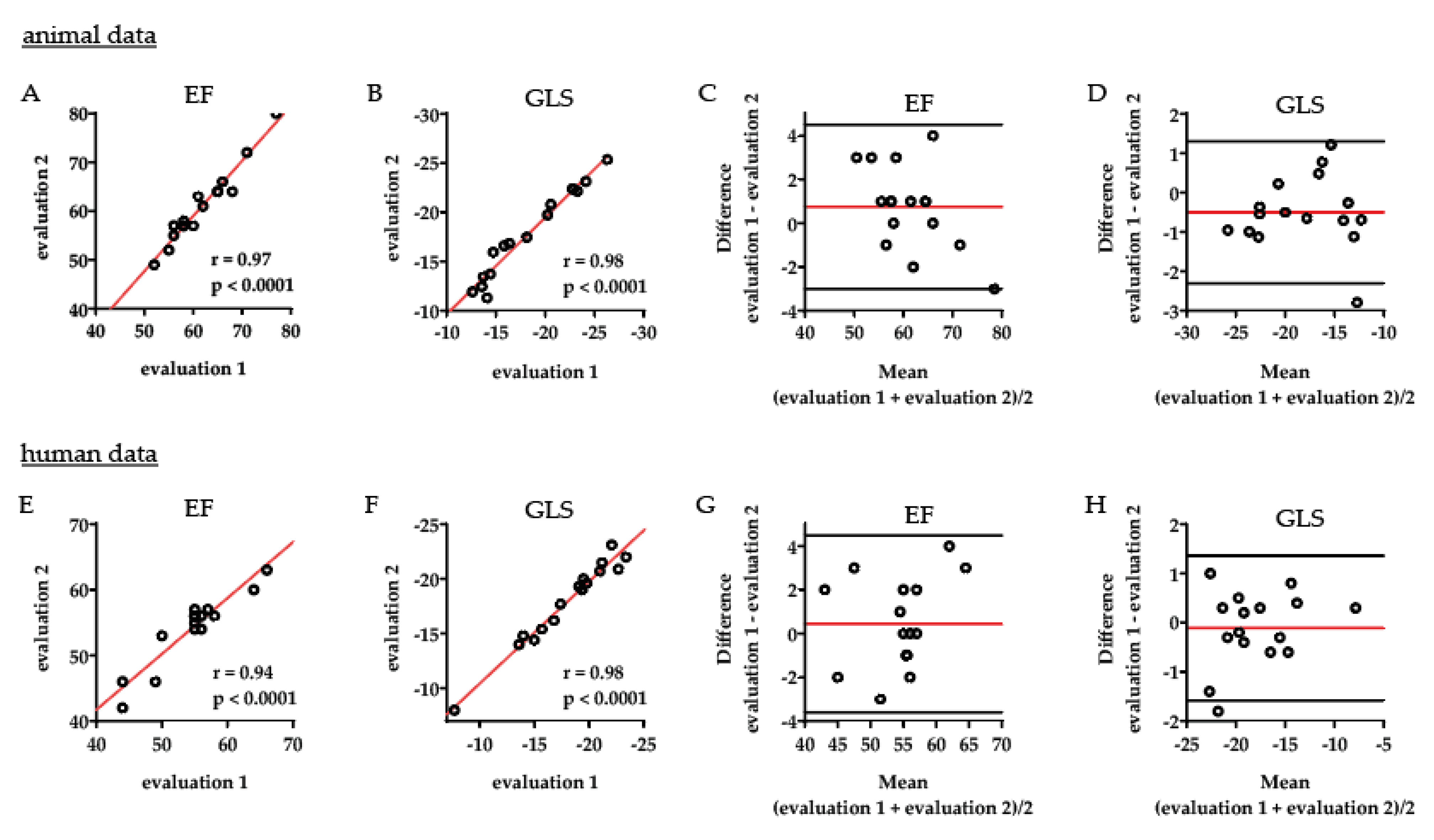
2.2. Intraobserver Variability Shows an Excellent Correlation within One Observer
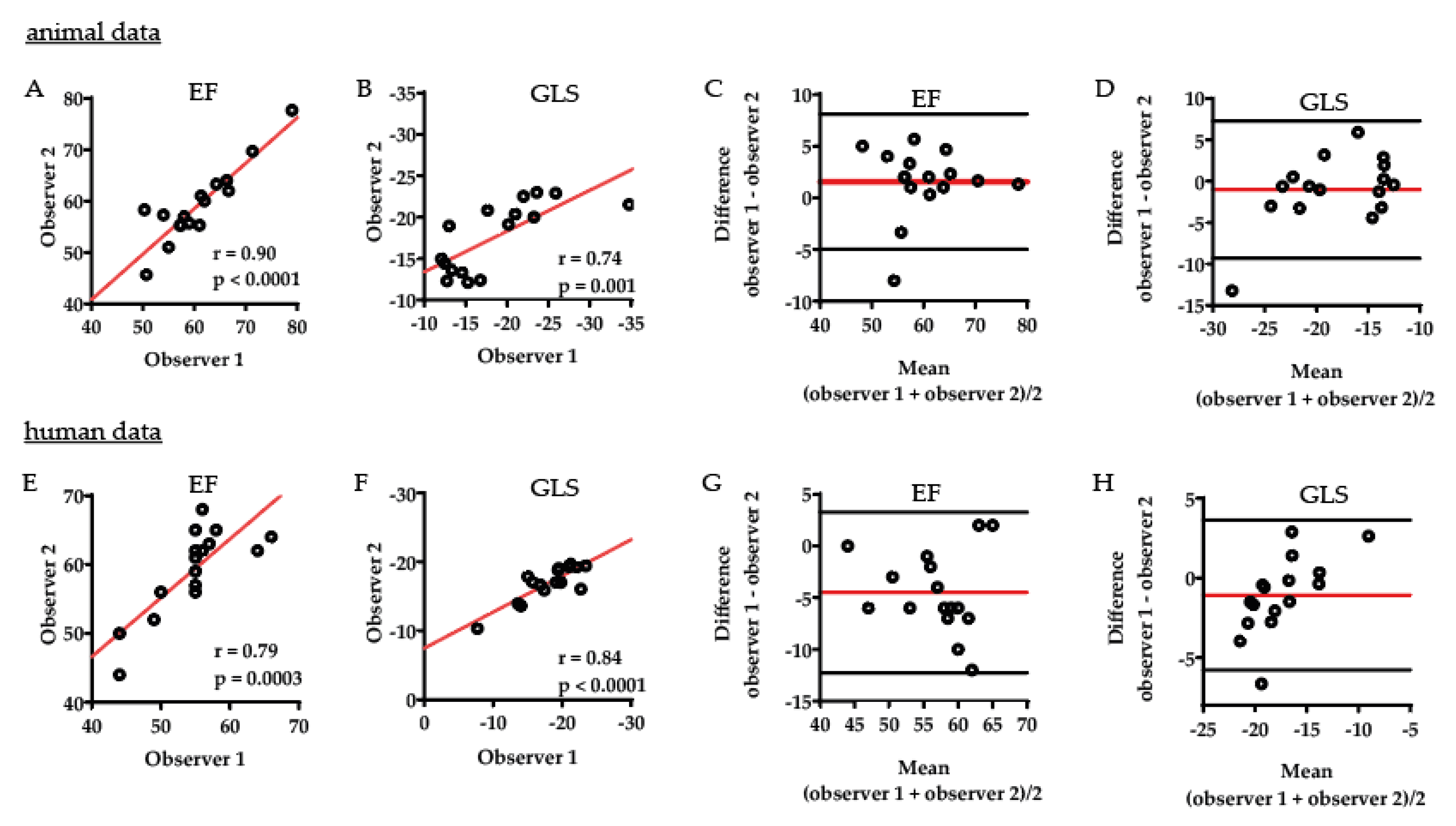
2.3. Interobserver Comparison Displays Strong Correlation between Two Different Observers
3. Discussion
4. Materials and Methods
4.1. Animal Cohort
4.2. Animal Echocardiography
4.3. Human Cohort
4.4. Human Echocardiography
4.5. Statistics
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| CVD | Cardiovascular disease |
| EF | Ejection fraction |
| GLS | Global longitudinal strain |
| hAogen | Human angiotensinogen |
| hRen | Human renin |
| ICC | Intraclass correlation coefficient |
| IVSd | Intraventricular septum diastole |
| LV | Left ventricle |
| LVEDD | Left ventricle end diastolic diameter |
| ns | Non-significant |
| PE | Preeclampsia |
| PWd | Posterior wall diastole |
| SEM | Standard error mean |
| sFlt-1 | Soluble fms-like tyrosine kinase I |
| STE | Speckle Tracking Echocardiography |
References
- Mosca, L.; Benjamin, E.J.; Berra, K.; Bezanson, J.L.; Dolor, R.J.; Lloyd-Jones, D.M.; Newby, L.K.; Pina, I.L.; Roger, V.L.; Shaw, L.J.; et al. Effectiveness-based guidelines for the prevention of cardiovascular disease in women--2011 update: A guideline from the american heart association. Circulation 2011, 123, 1243–1262. [Google Scholar] [CrossRef] [Green Version]
- Bellamy, L.; Casas, J.P.; Hingorani, A.D.; Williams, D.J. Pre-eclampsia and risk of cardiovascular disease and cancer in later life: Systematic review and meta-analysis. BMJ 2007, 335, 974. [Google Scholar] [CrossRef] [Green Version]
- Melchiorre, K.; Sharma, R.; Thilaganathan, B. Cardiovascular implications in preeclampsia: An overview. Circulation 2014, 130, 703–714. [Google Scholar] [CrossRef]
- Melchiorre, K.; Sutherland, G.R.; Liberati, M.; Thilaganathan, B. Preeclampsia is associated with persistent postpartum cardiovascular impairment. Hypertension 2011, 58, 709–715. [Google Scholar] [CrossRef] [Green Version]
- Strobl, I.; Windbichler, G.; Strasak, A.; Weiskopf-Schwendinger, V.; Schweigmann, U.; Ramoni, A.; Scheier, M. Left ventricular function many years after recovery from pre-eclampsia. BJOG 2011, 118, 76–83. [Google Scholar] [CrossRef] [Green Version]
- Ghossein-Doha, C.; van Neer, J.; Wissink, B.; Breetveld, N.M.; de Windt, L.J.; van Dijk, A.P.; van der Vlugt, M.J.; Janssen, M.C.; Heidema, W.M.; Scholten, R.R.; et al. Pre-eclampsia: An important risk factor for asymptomatic heart failure. Ultrasound. Obstet. Gynecol. 2017, 49, 143–149. [Google Scholar] [CrossRef] [Green Version]
- Lampinen, K.H.; Ronnback, M.; Kaaja, R.J.; Groop, P.H. Impaired vascular dilatation in women with a history of pre-eclampsia. J. Hypertens 2006, 24, 751–756. [Google Scholar] [CrossRef]
- Krabbendam, I.; Maas, M.L.; Thijssen, D.H.; Oyen, W.J.; Lotgering, F.K.; Hopman, M.T.; Spaanderman, M.E. Exercise-induced changes in venous vascular function in nonpregnant formerly preeclamptic women. Reprod. Sci. 2009, 16, 414–420. [Google Scholar] [CrossRef]
- Spaan, J.J.; Ekhart, T.; Spaanderman, M.E.; Peeters, L.L. Remote hemodynamics and renal function in formerly preeclamptic women. Obstet. Gynecol. 2009, 113, 853–859. [Google Scholar] [CrossRef]
- Foo, F.L.; Mahendru, A.A.; Masini, G.; Fraser, A.; Cacciatore, S.; MacIntyre, D.A.; McEniery, C.M.; Wilkinson, I.B.; Bennett, P.R.; Lees, C.C. Association Between Prepregnancy Cardiovascular Function and Subsequent Preeclampsia or Fetal Growth Restriction. Hypertension 2018, 72, 442–450. [Google Scholar] [CrossRef]
- Bohlender, J.; Ganten, D.; Luft, F.C. Rats transgenic for human renin and human angiotensinogen as a model for gestational hypertension. J. Am. Soc. Nephrol. 2000, 11, 2056–2061. [Google Scholar]
- Hering, L.; Herse, F.; Geusens, N.; Verlohren, S.; Wenzel, K.; Staff, A.C.; Brosnihan, K.B.; Huppertz, B.; Luft, F.C.; Muller, D.N.; et al. Effects of circulating and local uteroplacental angiotensin II in rat pregnancy. Hypertension 2010, 56, 311–318. [Google Scholar] [CrossRef] [Green Version]
- Geusens, N.; Verlohren, S.; Luyten, C.; Taube, M.; Hering, L.; Vercruysse, L.; Hanssens, M.; Dudenhausen, J.W.; Dechend, R.; Pijnenborg, R. Endovascular trophoblast invasion, spiral artery remodelling and uteroplacental haemodynamics in a transgenic rat model of pre-eclampsia. Placenta 2008, 29, 614–623. [Google Scholar] [CrossRef]
- Andersen, L.B.; Golic, M.; Przybyl, L.; Sorensen, G.L.; Jorgensen, J.S.; Fruekilde, P.; von Versen-Hoynck, F.; Herse, F.; Hojskov, C.S.; Dechend, R.; et al. Vitamin D depletion does not affect key aspects of the preeclamptic phenotype in a transgenic rodent model for preeclampsia. J. Am. Soc. Hypertens. 2016, 10, 597–607. [Google Scholar] [CrossRef]
- Dechend, R.; Gratze, P.; Wallukat, G.; Shagdarsuren, E.; Plehm, R.; Brasen, J.H.; Fiebeler, A.; Schneider, W.; Caluwaerts, S.; Vercruysse, L.; et al. Agonistic autoantibodies to the AT1 receptor in a transgenic rat model of preeclampsia. Hypertension 2005, 45, 742–746. [Google Scholar] [CrossRef] [Green Version]
- Kraker, K.; O’Driscoll, J.M.; Schutte, T.; Herse, F.; Patey, O.; Golic, M.; Geisberger, S.; Verlohren, S.; Birukov, A.; Heuser, A.; et al. Statins Reverse Postpartum Cardiovascular Dysfunction in a Rat Model of Preeclampsia. Hypertension 2020, 75, 202–210. [Google Scholar] [CrossRef]
- Sengupta, P. The Laboratory Rat: Relating Its Age With Human’s. Int. J. Prev. Med. 2013, 4, 624–630. [Google Scholar]
- Melchiorre, K.; Sutherland, G.R.; Baltabaeva, A.; Liberati, M.; Thilaganathan, B. Maternal cardiac dysfunction and remodeling in women with preeclampsia at term. Hypertension 2011, 57, 85–93. [Google Scholar] [CrossRef] [Green Version]
- Melchiorre, K.; Sutherland, G.R.; Watt-Coote, I.; Liberati, M.; Thilaganathan, B. Severe myocardial impairment and chamber dysfunction in preterm preeclampsia. Hypertens. Pregnancy 2012, 31, 454–471. [Google Scholar] [CrossRef]
- An, X.; Wang, J.; Li, H.; Lu, Z.; Bai, Y.; Xiao, H.; Zhang, Y.; Song, Y. Speckle Tracking Based Strain Analysis Is Sensitive for Early Detection of Pathological Cardiac Hypertrophy. PLoS ONE 2016, 11, e0149155. [Google Scholar] [CrossRef]
- Bauer, M.; Cheng, S.; Jain, M.; Ngoy, S.; Theodoropoulos, C.; Trujillo, A.; Lin, F.C.; Liao, R. Echocardiographic speckle-tracking based strain imaging for rapid cardiovascular phenotyping in mice. Circ. Res. 2011, 108, 908–916. [Google Scholar] [CrossRef] [Green Version]
- Peng, Y.; Popovic, Z.B.; Sopko, N.; Drinko, J.; Zhang, Z.; Thomas, J.D.; Penn, M.S. Speckle tracking echocardiography in the assessment of mouse models of cardiac dysfunction. Am. J. Physiol. Heart. Circ. Physiol. 2009, 297, H811–H820. [Google Scholar] [CrossRef]
- De Lucia, C.; Wallner, M.; Eaton, D.M.; Zhao, H.; Houser, S.R.; Koch, W.J. Echocardiographic Strain Analysis for the Early Detection of Left Ventricular Systolic/Diastolic Dysfunction and Dyssynchrony in a Mouse Model of Physiological Aging. J. Gerontol. A Biol. Sci. Med. Sci. 2019, 74, 455–461. [Google Scholar] [CrossRef]
- Imbalzano, E.; Zito, C.; Carerj, S.; Oreto, G.; Mandraffino, G.; Cusma-Piccione, M.; Di Bella, G.; Saitta, C.; Saitta, A. Left ventricular function in hypertension: New insight by speckle tracking echocardiography. Echocardiography 2011, 28, 649–657. [Google Scholar] [CrossRef]
- Cong, J.; Fan, T.; Yang, X.; Squires, J.W.; Cheng, G.; Zhang, L.; Zhang, Z. Structural and functional changes in maternal left ventricle during pregnancy: A three-dimensional speckle-tracking echocardiography study. Cardiovasc. Ultrasound. 2015, 13, 6. [Google Scholar] [CrossRef] [Green Version]
- Orabona, R.; Vizzardi, E.; Sciatti, E.; Bonadei, I.; Valcamonico, A.; Metra, M.; Frusca, T. Insights into cardiac alterations after pre-eclampsia: An echocardiographic study. Ultrasound. Obstet. Gynecol. 2017, 49, 124–133. [Google Scholar] [CrossRef] [Green Version]
- Orabona, R.; Sciatti, E.; Vizzardi, E.; Prefumo, F.; Bonadei, I.; Valcamonico, A.; Metra, M.; Lorusso, R.; Ghossein-Doha, C.; Spaanderman, M.E.A.; et al. Inappropriate left ventricular mass after preeclampsia: Another piece of the puzzle Inappropriate LVM and PE. Hypertens Res. 2019, 42, 522–529. [Google Scholar] [CrossRef]
- Main, E.K.; Cape, V.; Abreo, A.; Vasher, J.; Woods, A.; Carpenter, A.; Gould, J.B. Reduction of severe maternal morbidity from hemorrhage using a state perinatal quality collaborative. Am. J. Obstet. Gynecol. 2017, 216, 298.e1–298.e11. [Google Scholar] [CrossRef]
- Regitz-Zagrosek, V.; Roos-Hesselink, J.W.; Bauersachs, J.; Blomstrom-Lundqvist, C.; Cifkova, R.; De Bonis, M.; Iung, B.; Johnson, M.R.; Kintscher, U.; Kranke, P.; et al. 2018 ESC Guidelines for the management of cardiovascular diseases during pregnancy. Eur. Heart J. 2018, 39, 3165–3241. [Google Scholar] [CrossRef]
- Tranquilli, A.L.; Brown, M.A.; Zeeman, G.G.; Dekker, G.; Sibai, B.M. The definition of severe and early-onset preeclampsia. Statements from the International Society for the Study of Hypertension in Pregnancy (ISSHP). Pregnancy Hypertens. 2013, 3, 44–47. [Google Scholar] [CrossRef]
- Tranquilli, A.L.; Dekker, G.; Magee, L.; Roberts, J.; Sibai, B.M.; Steyn, W.; Zeeman, G.G.; Brown, M.A. The classification, diagnosis and management of the hypertensive disorders of pregnancy: A revised statement from the ISSHP. Pregnancy Hypertens. 2014, 4, 97–104. [Google Scholar] [CrossRef]
- National High Blood Pressure Education Program Working Group on High Blood Pressure in Pregnancy. Report of the National High Blood Pressure Education Program Working Group on High Blood Pressure in Pregnancy. Am. J. Obstet. Gynecol. 2000, 183, S1–S22. [Google Scholar] [CrossRef]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F., 3rd; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 1321–1360. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control (n = 8) | Preeclamptic (n = 8) | p-Value | |
|---|---|---|---|
| Age (years) | 36.3 ± 1.71 | 35.0 ± 1.45 | 0.5860 |
| Weight (kg) | 70.9 ± 5.2 | 77.8 ± 7.3 | 0.4569 |
| Height (m) | 1.7 ± 0.0 | 1.6 ± 0.0 | 0.2014 |
| BMI (kg/m²) | 25.1 ± 1.58 | 28.8 ± 2.17 | 0.1870 |
| Gestational age of delivery (weeks) | 40.4 ± 0.60 | 31.5 ± 1.49 | <0.0001 |
| Scan after delivery (weeks) | 45.5 ± 5.45 | 49.8 ± 3.34 | 0.5169 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kräker, K.; Schütte, T.; O’Driscoll, J.; Birukov, A.; Patey, O.; Herse, F.; Müller, D.N.; Thilaganathan, B.; Haase, N.; Dechend, R. Speckle Tracking Echocardiography: New Ways of Translational Approaches in Preeclampsia to Detect Cardiovascular Dysfunction. Int. J. Mol. Sci. 2020, 21, 1162. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21031162
Kräker K, Schütte T, O’Driscoll J, Birukov A, Patey O, Herse F, Müller DN, Thilaganathan B, Haase N, Dechend R. Speckle Tracking Echocardiography: New Ways of Translational Approaches in Preeclampsia to Detect Cardiovascular Dysfunction. International Journal of Molecular Sciences. 2020; 21(3):1162. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21031162
Chicago/Turabian StyleKräker, Kristin, Till Schütte, Jamie O’Driscoll, Anna Birukov, Olga Patey, Florian Herse, Dominik N. Müller, Basky Thilaganathan, Nadine Haase, and Ralf Dechend. 2020. "Speckle Tracking Echocardiography: New Ways of Translational Approaches in Preeclampsia to Detect Cardiovascular Dysfunction" International Journal of Molecular Sciences 21, no. 3: 1162. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21031162