1. Introduction
The human
SCN4A gene encodes the alpha-subunit of the voltage-gated sodium channel Na
v1.4, which is the pore-forming subunit. The Na
v1.4 channel is expressed in skeletal muscles, and its related channelopathies affect skeletal muscle excitability [
1,
2,
3]. There are two prevalent clinical symptoms: (1) muscle stiffness with hypertonia (myotonia) episodes (non-dystrophic myotonia, NDM); and (2) muscle weakness leading to recurrent paralysis episodes (periodic paralysis, PP). According to clinical and electromyographical (EMG) features, there are at least two disease entities for NDM: sodium channel myotonia (SCM) and paramyotonia congenita (PMC). The clinical features of dominant SCM are not significantly cold-sensitive and do not significantly decrease the compound motor action potential in an EMG test. SCM can manifest as paramyotonia, potassium-aggravated myotonia, myotonia permanens, acetazolamide-responsive myotonia, painful myotonia and severe neonatal episodic laryngospasm [
4]. Patients with SCM may sometimes present with exercise-induced, delayed-onset myotonia or acetazolamide-responsive myotonia [
5]. An EMG examination will show a progressive decrease of compound motor action potential in a post-repetitive short effort test. Furthermore, PP caused by Na
v1.4 channelopathy can be divided into hypokalemic PP (hypoPP) and hyperkalemic PP (hyperPP), which are associated with the blood potassium level. Generally, overlap, borderline or mixed clinical features between NDM and PP can be identified in patients with a Na
v1.4 mutation [
6,
7,
8,
9]. The age of onset is from early to late childhood. The prevalence of Na
v1.4 channelopathies involving skeletal muscle has been estimated to be 0.4~1.4 : 100,000 [
5]. As of today, more than seventy mutations in the
SCN4A gene have been identified as pathogenic, and twelve are likely pathogenic [
10]. Most
SCN4A mutations are transmitted dominantly. The penetrance of the mutations among pedigrees is variable. Thus, the variable genotypes and phenotypes render it difficult to identify a correlation among Na
v1.4 channelopathies.
Changes of the electrophysiological features with a Na
v1.4 mutation in functional expression models have been investigated for two decades. The repertoire of biophysical defects of mutant channel behavior that predisposes the affected muscle affect both activation and inactivation gating mechanisms [
10]. Basically, a Na
v1.4 gain of function mutation results in myotonia, hyperPP and hypoPP; however, some defects predispose to myotonia, while others increase susceptibility to PP. Previous studies on Na
v1.4 mutations in SCM patients have demonstrated that the kinetics of channel inactivation are altered with a slower rate of onset and, sometimes, with faster recovery as well [
11,
12]. Nevertheless, the most characteristic phenotype, myotonia, as shown in EMG, demonstrates repetitive firing of action potentials. Considering the repetitive discharge, clinical phenotypes such as ataxia in
Scn8a-deficient mice, and recurrent attacks of erythromelalgia in patients with an
SCN9A mutation have been proposed to be ascribed to resurgent Na
+ currents elicited during the repolarization stage [
13,
14]. The genesis of resurgent current occurred at repolarization stage with reopening of the voltage-gated sodium channel. It has been proposed that there is competition between the Na
vβ4 peptides and the inactivating molecules to block the reopened channel [
14,
15,
16,
17]. Nevertheless, how the mutations in voltage-gated sodium channel facilitate the occurrence of resurgent current remains elusive.
As of today, the resurgent Na
+ currents found in the Na
v1.4 channel and the impact of a Na
v1.4 mutation on SCM have yet to be characterized, aside from a single study on PMC in dorsal root ganglion (DRG) neurons [
18]. Studying a known mutation in the Na
v1.4 channel in two individual families with SCM, our research aims to determine the changes of the resurgent Na
+ current caused by the mutation in the Na
v1.4 channel and correlate the phenotype with its aberrant electrophysiological features.
3. Discussion
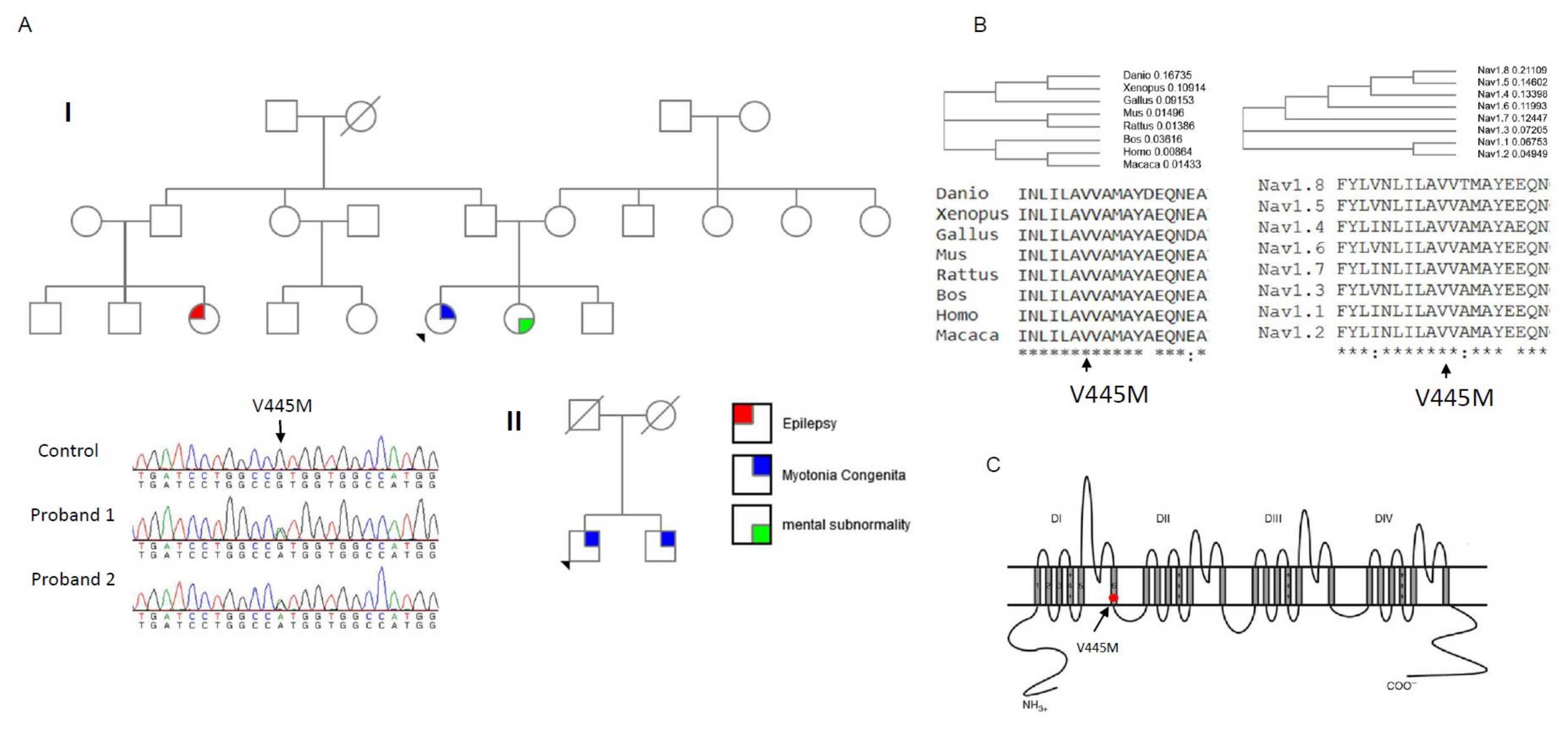
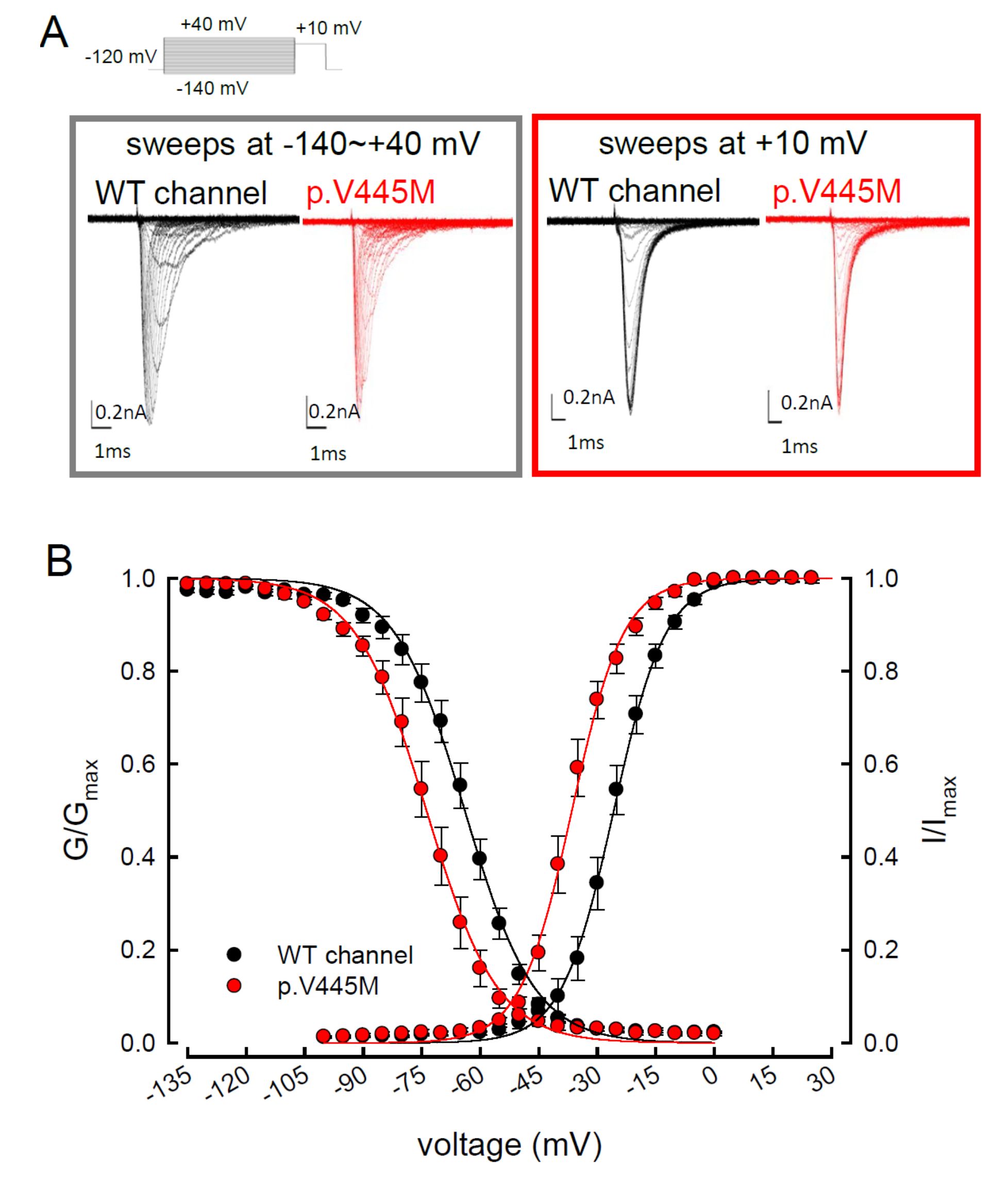
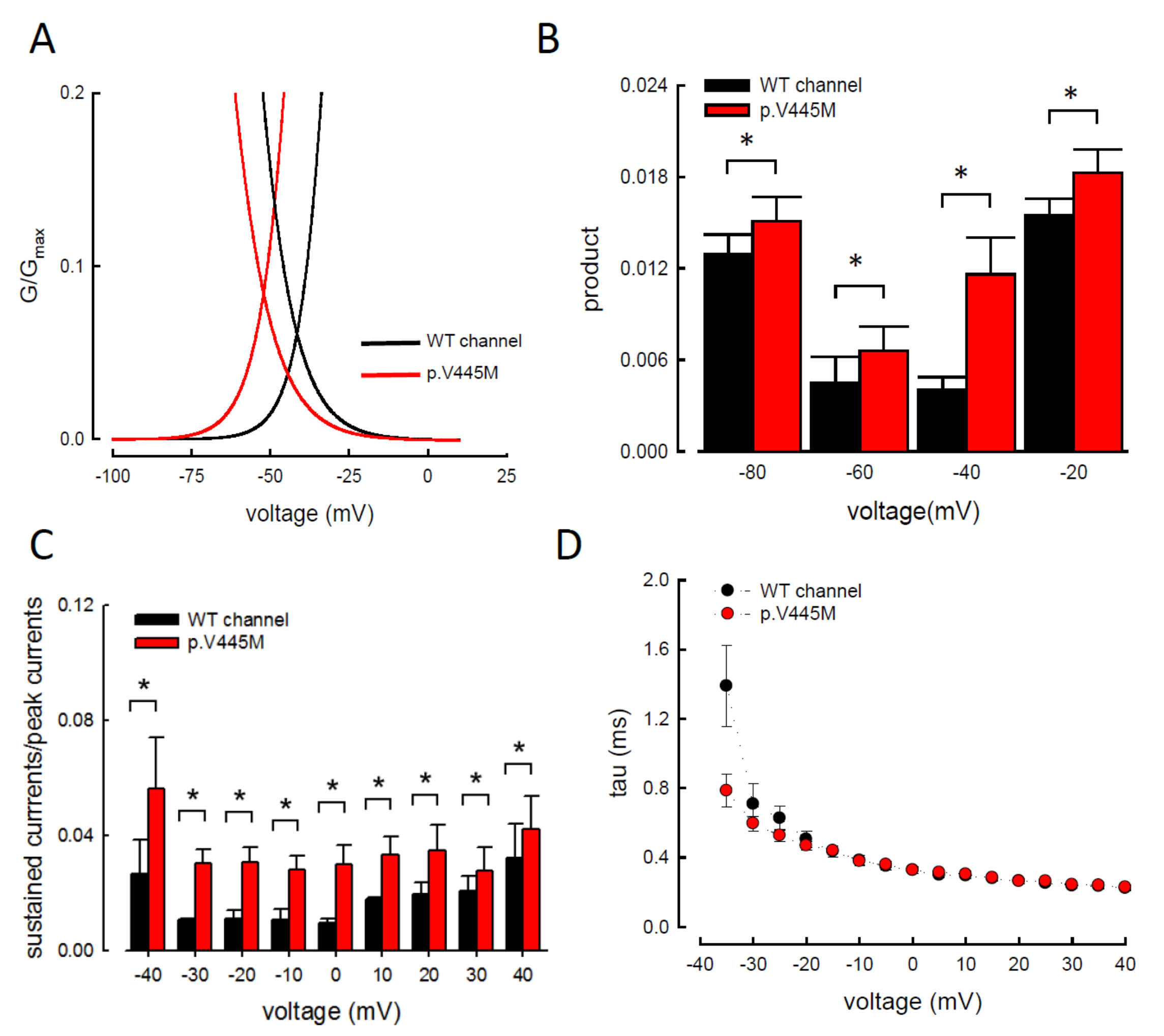
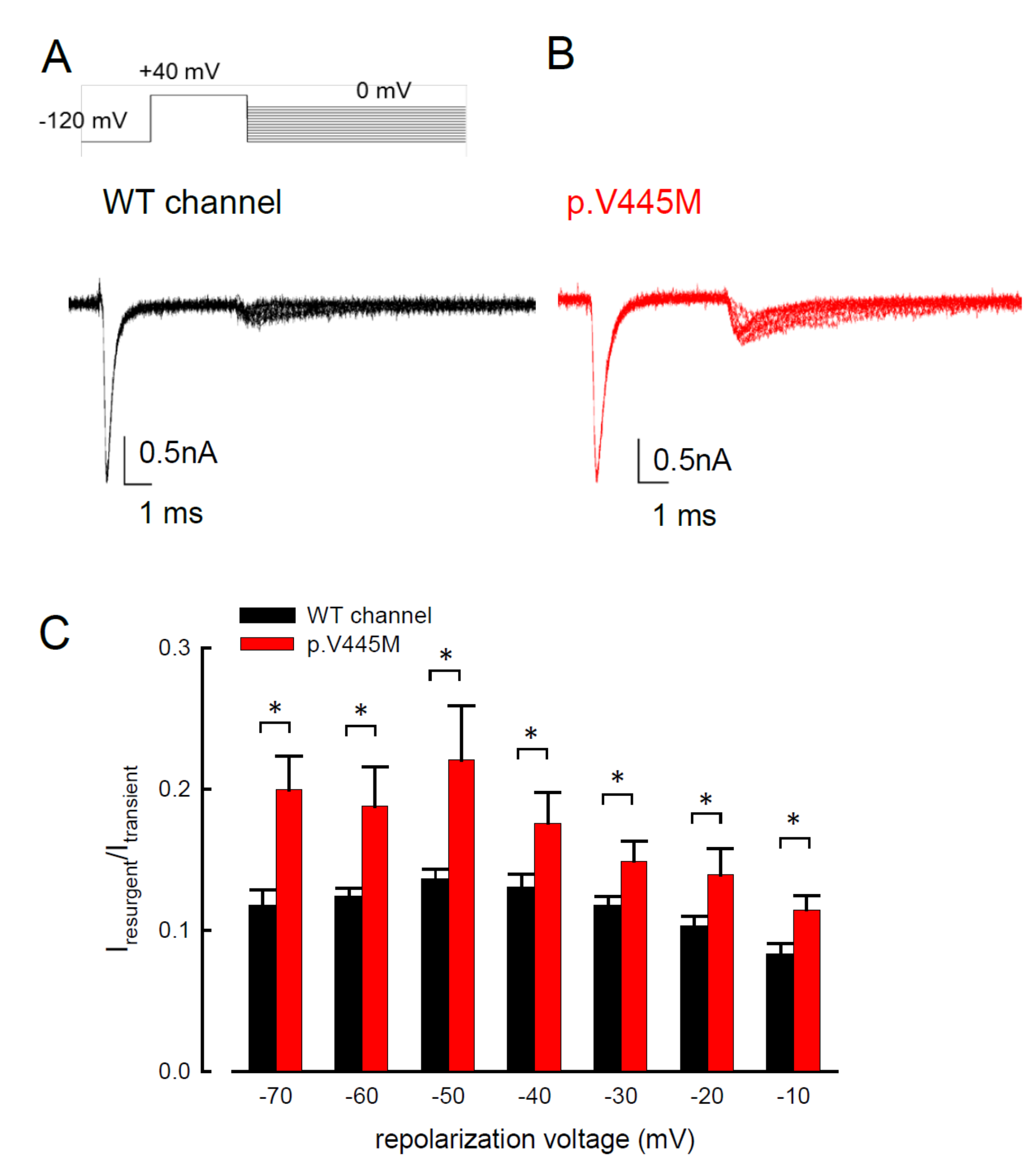
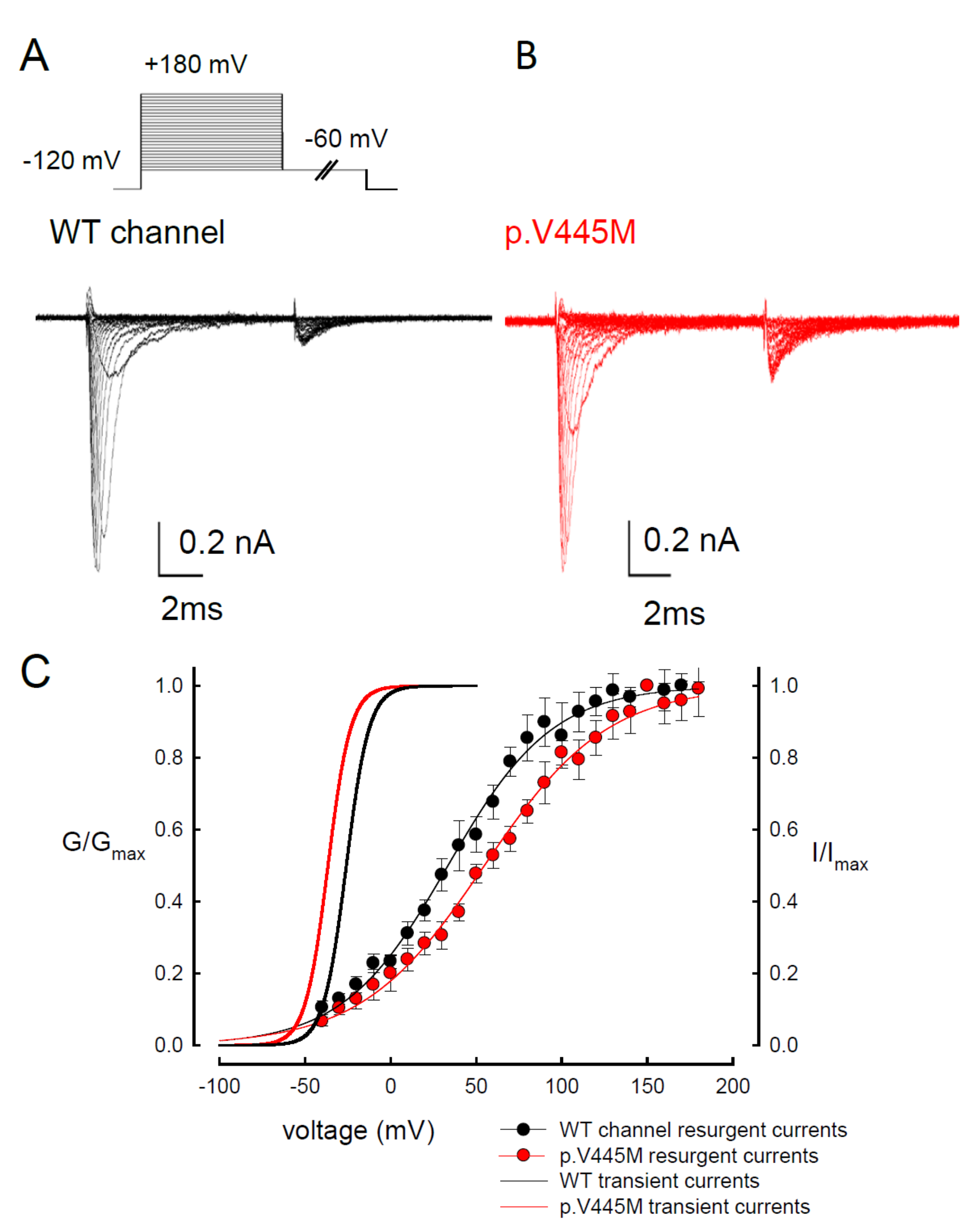
In summary, we identified the missense mutation p.V445M of the SCN4A gene from two patients with SCM who were recruited from two individual families. To determine the electrophysiological function of this mutation, a transfected CHO-K1 cell model was employed for the whole-cell patch-clamp recording. Evaluation of the transient Na+ current showed a hyperpolarizing shift in both the activation and inactivation curves of the mutant channel as compared with the WT channel. The window and sustained Na+ currents of the mutant channel were larger than those of the WT. Upon transfection of both Nav1.4 and a Navβ4 peptide, resurgent Na+ currents could be obtained 3~5 ms after a prepulse of depolarization. Compared with that of the WT channel, the magnitude of the resurgent Na+ currents were conspicuously larger in the mutant channel. Moreover, the time to peak of the resurgent Na+ currents in the mutant channel was slower than that of the WT channel, although no difference was found between them in the decay kinetics.
Myotonia results from an involuntary muscle contraction that persists for several seconds after the cessation of voluntary effect [
22]. The hyperexcitability of muscles with a burst of muscle action potentials leads to an after-contraction that can last for several seconds. The spontaneous, painless discharges show a waxing and waning pattern upon EMG study. A sustained burst of discharges can be elicited by a brief voluntary contraction, and the firing frequency is usually 20~80 Hz, which means the interval of the depolarizing potentials is between 12.5 and 50 ms [
23]. The repetitive, high-frequency discharges in myotonia suggest that resurgent Na
+ currents may be a critical factor involving the phenotype. Channels are usually refractory to be activated after inactivation until the membrane potential has been sufficiently hyperpolarized. Nevertheless, channels can reopen, allowing a surge of inward current during repolarization, i.e., resurgent Na
+ currents. Raman and Bean first described resurgent Na
+ currents in cerebellar Purkinje neurons [
16]. In the cerebellum, the resurgent Na
+ currents following relief of an ultra-fast open-channel block by an endogenous blocking particle, probably the C-terminal portion of the Na
vβ4 subunit [
24], may contribute to high-frequency firing [
16,
25]. The Na
v1.6 channel is the major carrier of resurgent Na
+ currents in cerebellar [
26] and DRG [
27] neurons. In the whole-cell configuration of transfected CHO-K1 cells expressing the Na
v1.7 channel, resurgent Na
+ currents after a long depolarizing prepulse have also been identified [
13]. Resurgent Na
+ currents from the mutant Na
v1.7 channel may play an important role in the episodic attacks of severe neuropathic pain found in both erythromelalgia and paroxysmal extreme pain disorders [
28]. Enhancement of resurgent Na
+ currents has even been proposed to be highly correlated with the severity of neuropathic pain [
28]. In the present study, a hyperpolarizing shift was found in both activation and inactivation curves between the mutant and WT channels. Although the window currents increased in the mutant channel, the hyperexcitability with repetitive recurrent discharges could not be fully explained by the changes in the transient Na
+ current alone. Here, we described the resurgent Na
+ currents in the Na
v1.4 channel. Compared with the WT channel, the larger magnitude and slowing of the time to peak of the resurgent Na
+ currents in the mutant channel may be one of the crucial factors of the functional disturbances of SCM. It has been proposed that impaired inactivation is a major determinant of resurgent Na
+ currents in Na
v1.7 channels [
28]. Future research should investigate whether mediation of the inactivation process governs the functional consequences resulting from a mutation in the Na
v1.4 channel, although prolonged recovery of slow inactivation has been observed in the p.V445M mutant channel [
20].
In our study, resurgent currents of Nav1.4 channel are discernible only in the presence of the Na
vβ4 peptides (
Figure S1). According to the prevailing model, this is ascribable to the competition between the Na
vβ4 peptides and the inactivating peptide for the open channel pore [
14,
15,
16,
17]. However, quite other biophysical characteristics, including (1) the concomitant increase of resurgent and sustained currents with the p.V445M mutant channels (
Figure 3A–C and
Figure 4), (2) the very much different activation curves for the transient and resurgent currents (
Figure 5C) all strongly argue against that the Na
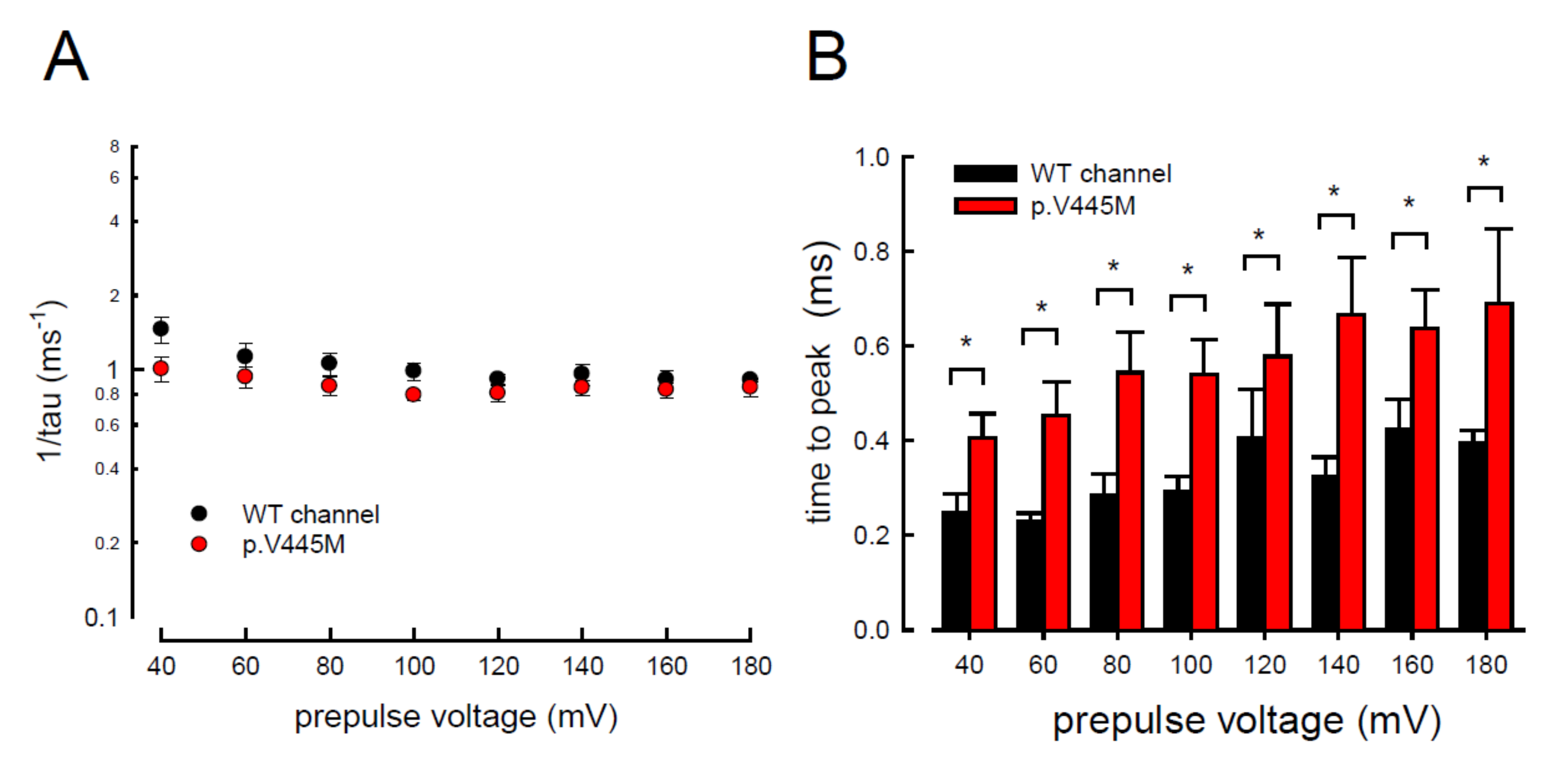
vβ4 peptide competes with the inactivating molecule for the same single open state, (3) the slower time to peak but unchanged decay kinetics of the resurgent currents with p.V445M mutant channels also contradicts that Na
vβ4 peptide competes with the inactivating molecule for the same single open state to generate the resurgent currents. We therefore propose that there may be two distinct open states (with two corresponding inactivated states) of the Na
v1.4 channel (
Figure 5), each responsible for the transient (O
1) and resurgent (O
2) currents, respectively. Significant occupancy of O
2 is possible only in the presence of the Na
vβ4 peptides, which is thus chiefly a gating modifier inducing new gating conformations rather than a pore blocker competing with the inactivating peptides.
The activation curves of the resurgent Na
+ currents in both the WT and p.V445M mutant channels markedly moved to a more positive voltage range, with a much less steep slope than those of the transient currents (
Figure 5C). We proposed that there may be two open states of the channel and that the gating modification illustrates the electrophysiological changes of the genesis of resurgent Na
+ currents [
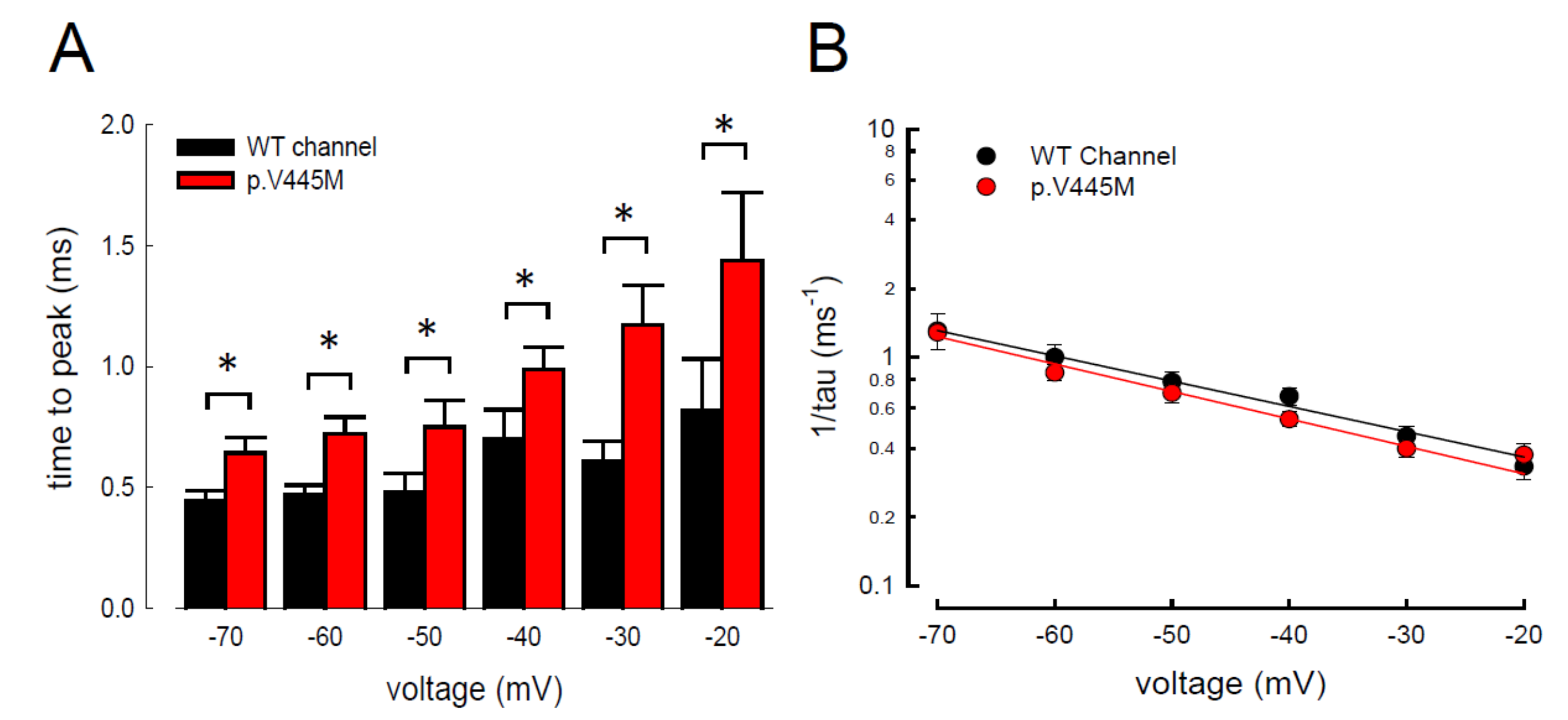
13]. This study showed that either after a depolarizing prepulse (
Figure 6B) or under a variable extent of repolarization (
Figure 7A), the time to peak of the resurgent Na
+ currents in the mutant channel was extended significantly compared with that in the WT channel; however, the decay kinetics (1/tau) remained similar between the channels. The p.V445M mutation significantly accelerated the entry and protracted the duration of the new open (activation) state, leading to an increase in the magnitude of the resurgent Na
+ currents. The reopening of the fast inactivated channels was probably accompanied by conformational changes of the domain I/S6 (DI/S6), where V445M is located.
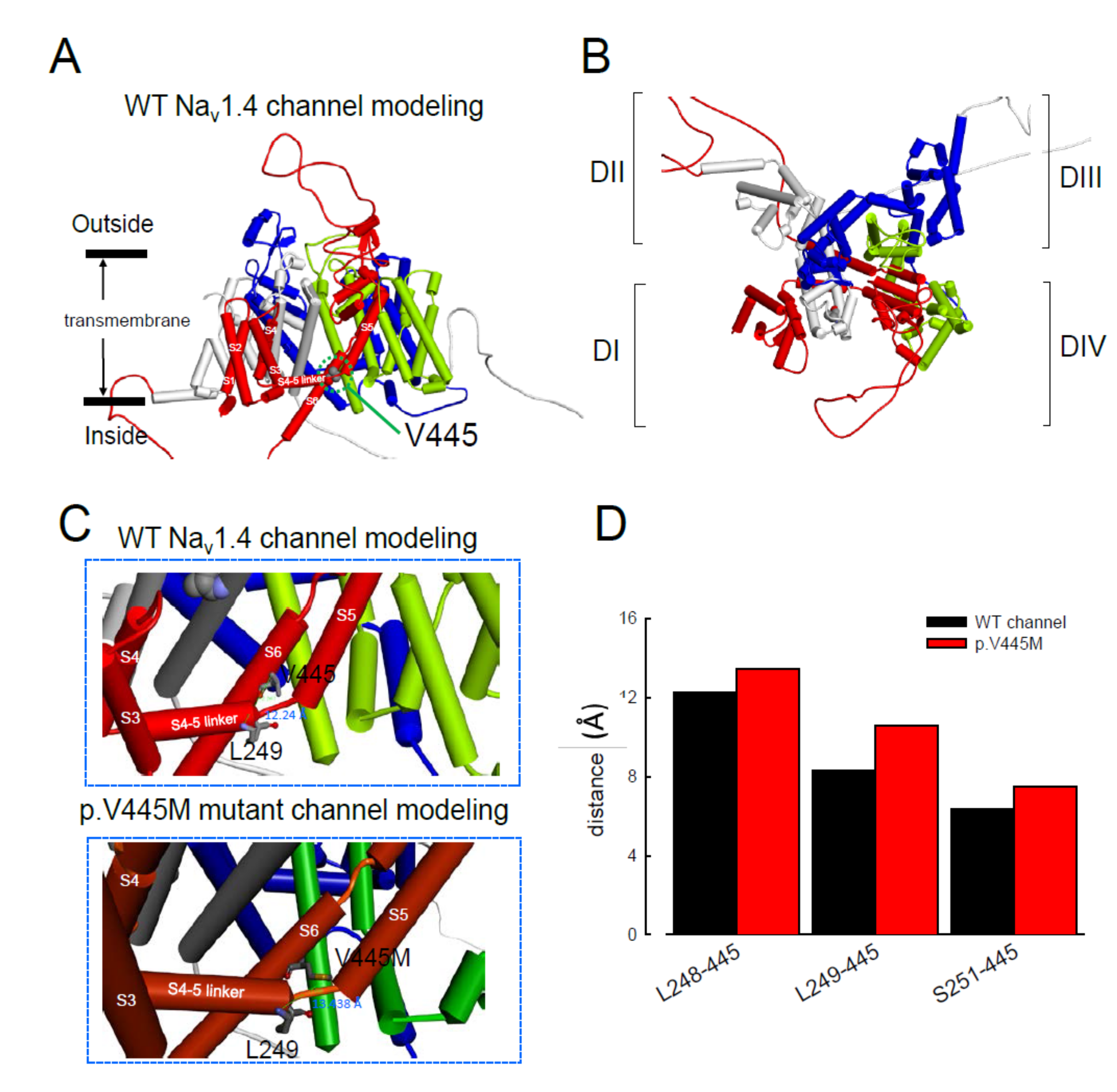
The computer homology model of the WT Na
v1.4 channel evaluated the topological structure change caused by the p.V445M mutation (
Figure 8A,B). The model estimated that the change of Val445 to Met may increase the distance between V445 and the residues at the S4–S5 linker (DI/S4-5 linker) (e.g., L248, L249 and S251;
Figure 8). While the S4–S5 linker plays an imperative role in governing the activation/inactivation of resurgent Na
+ currents [
13], such a distance change could contribute to the attenuation of inactivation and uncoupling between activation and inactivation. In the previous study, genesis of resurgent Na
+ currents in the Na
v1.7 channel was found to be possibly due to the existence of two open states in activation [
13]. Through modulating the transitional kinetics between these two states, the S4–S5 linker in Domain III seems to play an important role in activation–inactivation coupling. Mutations involving the linker and relevant nearby regions may, therefore, enhance the sustained and resurgent Na
+ currents, leading to marked hyperexcitability and repetitive firing in the corresponding tissues. Herein, we postulated that the change of distance between V445 and the residues of the S4–S5 linker may be one of the critical factors for the coupling effect. Aberrations in modulation of the coupling facilitate the generation of resurgent Na
+ currents and increase both the magnitude and time to peak, augmenting the repetitive firing. The mutation causes slowing of the time to peak of the resurgent Na
+ currents elicited in the Na
v1.4 channel, which increases the firing frequency of the muscle membrane. The action potential propagates to the T-tubule, which induces the opening of the voltage-gated calcium channel from the sarcoplasmic reticulum. The released calcium ion binds to troponin C, which induces the cross bridge to contract. The resurgent Na
+ currents introduce repetitive high-frequency firing, facilitating the binding leading to muscle stiffness. The essential tremors and chronic seizures found in the family members with a p.G1537S mutation in the
SCN4A gene [
29] may also have been attributable to the disturbance of the resurgent Na
+ currents in the Na
v1.4 channel.
In addition to SCM, mutations in Na
v1.4 are also responsible for PMC. Clinically, mutations involving the Arg1448 of the
SCN4A gene are frequently found in patients with PMC [
30]. The resurgent Na
+ currents in the Na
v1.4 channel were first described using rat DRG neurons transfected with Na
v1.4r-R1448P. Jarecki et al. reported that the resurgent Na
+ currents could be obtained and that the average relative amplitude was 4.8± 0.7% [
18], much lower than our findings (~10% in the WT and approximately 15–20% in mutant channels,
Figure 4C). Furthermore, the Arg1448 locates at DIV/S4, which is the outermost extracellular charged residue in the sodium channel voltage sensor that modulates the activation/inactivation coupling of the channel. The study showed that the Na
v1.4r-R1448P channels slow the inactivation and generate resurgent Na
+ currents, suggesting that the mutation slows the rate of open-channel fast inactivation and may be able to induce resurgent Na
+ currents. In another study, large resurgent Na
+ currents could be observed in nearly 62% of Na
v1.8-null DRG neurons using Biolistic transfected with Na
v1.6r during the repolarization stage; however, no resurgent Na
+ currents were identified in neurons transfected with a TTX-R version of the rat skeletal muscle sodium channel Na
v1.4, although they generated a larger peak sodium current amplitude than the Na
v1.6 channels [
27]. The discrepancy may have been due to the different expression systems and the modification of the channel to become TTX-resistant since resurgent Na
+ currents are difficult to obtain using DRG neurons or WT skeletal muscles [
27]. In a recent report, a p.G1306E mutation of SCN4A gene caused NDM and Brugada syndrome after treated with flecainide. The different isoforms of Nav1.4 expressed in the skeletal and cardiac muscles may result in such a rare phenotype [
31].
In conclusion, mutations in SCN4A are responsible for SCM. The hyperpolarizing shifting of the activation and inactivation curves, which results in an increase of window and sustained Na+ currents, may contribute to the hyperexcitability of neural-muscle tissues. The Nav1.4 channel can generate resurgent Na+ currents, which may further increase repetitive firing of the action potential in skeletal muscle, one of the hallmarks of SCM in EMG. In addition to myotonia, patients with SCM frequently experience episodes of muscle weakness. Overall, SCN4A mutations resulting in defects of slow inactivation and delay of time to peak in resurgent Na+ currents are likely factors contributing to constant myotonia and weakness in SCM patients.
4. Materials and Methods
4.1. Genetic Analysis of Two Families with Non-Dystrophic Myotonia (NDM)
Two probands with NDM from two individual Taiwanese–Chinese families visited the neurology clinic of the National Taiwan University Hospital, Taipei, Taiwan. Leukocyte DNA from the probands and their relatives was collected for genetic diagnosis. The genetic studies were approved by the Institutional Review Board (NTUH-REC No.: 201802049RINB) and written inform consent was obtained. Genetic analysis of two families with non-dystrophic myotonia (NDM). All methods and procedures were performed in accordance with the guideline and regulations.
4.2. Preparation for DNA Constructs
The cDNA of the wild-type (WT) human Nav1.4 channel (SCN4A) was purchased from OriGene Technologies Company (Cat. No. RC218290; Rockville, MD, USA). For mutagenesis, p.V445M mutant channel cDNA was created using the QuikChange Site-Directed Mutagenesis System Kit (Stratagene, La Jolla, CA, USA), and a c.1333G>A sequence variant was introduced. The cDNA sequence was confirmed by automatic DNA sequencing (3730xl DNA Analyzer; Applied Biosystems, Foster, CA, USA).
4.3. CHO-K1 Cell Cultures for WT and p.V445M Mutant cDNA Transfection
The Chinese hamster ovary (CHO-K1) cells used were approved by the Food Industry Research and Development Institute, Hsinchu, Taiwan. The cells were maintained in F12-K medium (Thermo Fisher Scientific, Waltham, MA, USA) under humidified conditions with 5% CO2|95% O2 at 37 °C. The medium was supplemented with 10% fetal bovine serum (Thermo Fisher Scientific) and 0.5% penicillin-streptomycin antibiotics (Thermo Fisher Scientific). A total of 1 × 106 CHO-K1 cells were seeded into a 35-mm culture dish (Greenpia Technology, Seoul, Korea). Briefly, Lipofectamine™ 3000 (Thermo Fisher Scientific, USA) DNA mix with 5.0 μg WT or p.V445M SCN4A cDNA construct and 0.1 μg green fluorescent protein was added to CHO-K1 cells in the F12-K medium at 37 °C with 5% CO2|95% O2 for one to two days. For the whole-cell patch-clamp recording, 0.1 mg/mL trypsin (Sigma-Aldrich, St. Louis, MO, USA) was added to the transfected cDNA CHO-K1 cells and let the cells to be dissociated in F12–K medium with 10% FBS. Then, the cells were plated on coverslips under 37 °C for ~60 min. Usually the patch-clamp recordings were carried out within 2–3 days following cDNA transfection, and the isolated single cells for electrophysiology recording were used within ~4 h of preparation.
4.4. Whole-cell Patch-Clamp Recordings of CHO-K1 Cells Expressing WT and p.V445M Mutant SCN4A Constructs
Whole-cell patch-clamp recordings of CHO-K1 cells expressing WT and p.V445M mutant SCN4A cDNA constructs were performed two to three days after the transfection. The recordings were carried out using an Axopatch 700B amplifier (Axon Instruments, Sunnyvale, CA, USA) and the pClamp 9.2 acquisition software package (Molecular Devices, San Jose, CA, USA). The currents were digitized with the Digidata-1322A interface (Axon Instruments, USA). A glass electrode pipette was fabricated with a tip of approximate diameter 1.0 μm and fired to a resistance of 1.0–2.0 mΩ using the Sutter P-97 puller (Sutter Instrument Company, USA). The glass electrode pipette was filled with an internal solution containing 75 mM CsCl, 75 mM CsF, 5 mM HEPES, 2 mM CaCl2 and 2.5 mM EGTA (pH = 7.4 – 7.6). The whole-cell configuration was immersed in an external solution of 145 mM NaCl, 10 mM HEPES, 2 mM CaCl2 and 2.5 mM MgCl2 (pH = 7.4 – 7.6). Then, the whole-cell configuration was moved in front of square glass barrel micropipes (Drummond Scientific, Broomall, PA, USA) emitting the extracellular solutions. A short intracellular Navβ4 peptide (KKLITFILKKTREK−OH, 0.1 mM) was also added to the internal solution to generate resurgent Na+ currents. One micromolar of tetrodotoxin (TTX) (Tocris, Bristol, UK) was used to block TTX-sensitive (TTX-s) Na+ channels. By subtracting the TTX-s currents, the resurgent Na+ currents could be obtained. To estimate the conductance, the data were fitted into the following Boltzmann sigmoid equation: Y = 1/1 + exp[(Vh − X)/k], where Y is the conductance, X is the membrane potential, Vh is the membrane potential with half of the conductance, and k is the slope of the curve.
4.5. Homology Modeling
The homology modeling procedure was performed using methods similar to those used in our previous study [
13,
21]. A homology model of the WT Na
v1.4 channel encoded by the
SCN4A gene was built from X-ray crystal structure data of the human voltage-gated Na
v1.4 channel (human Na
v1.4; PDB code: 6AGF). The amino acid sequence of the WT Na
v1.4 channel was obtained from the UniProt database (P35499). Sequences of the three inter-domain linkers of the WT Na
v1.4 channel (DI–DII linker, A447-P578; DII–DIII linker, L798–W1032; and DIII–DIV linker, G1292-A1354) were inserted into positions between the domains (DI–DIV) via homology modeling based on the WT human Na
v1.4 channel. The aligned sequences were then processed using Discovery Studio 2018 (Dassault Systèmes, Vélizy–Villacoublay, France) to assign the relative positions and generate the secondary structure of the WT human Na
v1.4 channel [
13,
21].
4.6. Data Analysis
All statistical data were described as mean ± standard error mean. Statistical significance was assessed and analyzed using the Student’s independent t-test and accepted at p < 0.05.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}







