The Impact of Lidocaine on Adipose-Derived Stem Cells in Human Adipose Tissue Harvested by Liposuction and Used for Lipotransfer

 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Basic Demographics and Clinical Data of the Patients
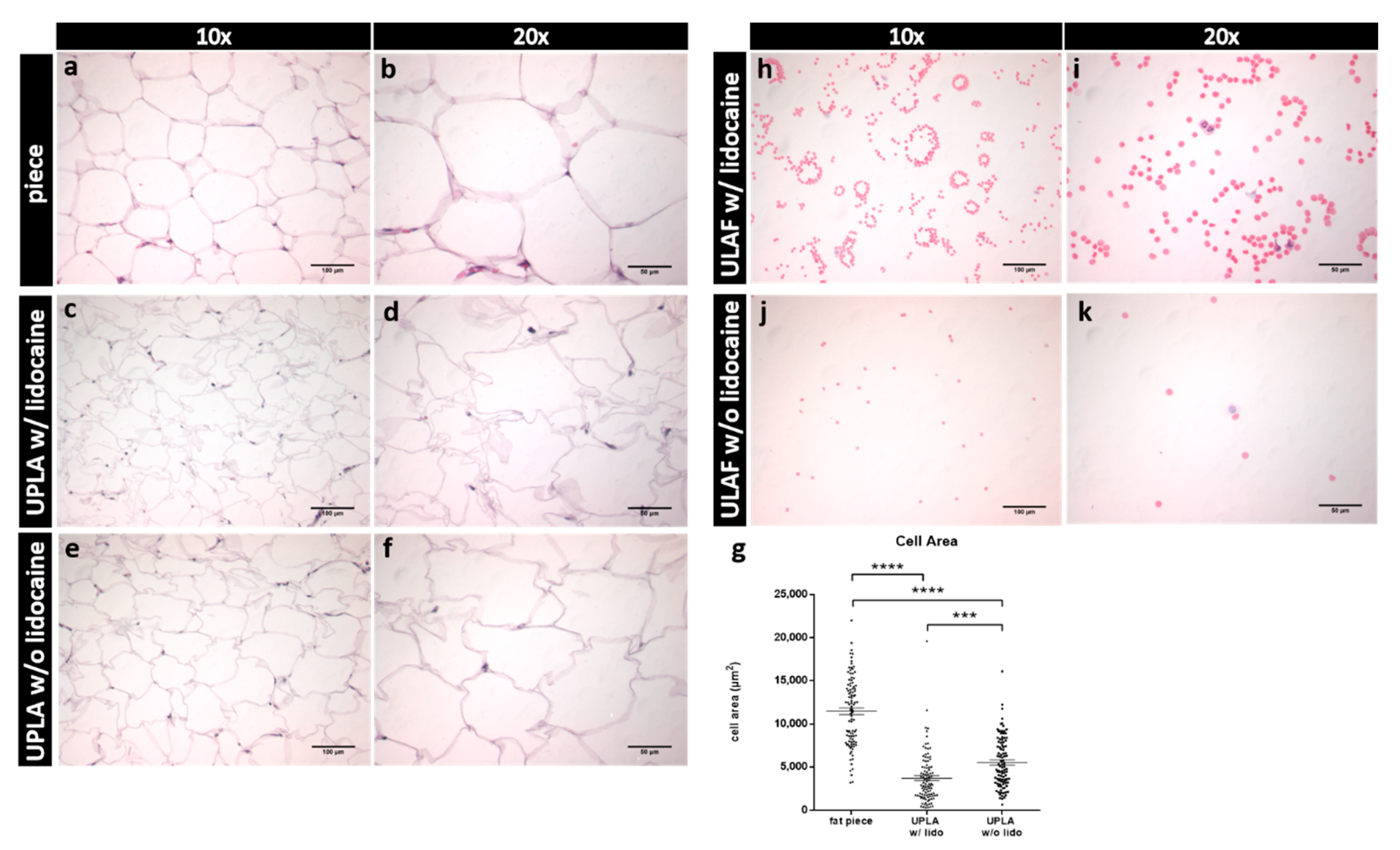
2.2. Hematoxylin-Eosin (HE) Staining of Unprocessed Lipoaspirate and Surgically Resected Fat Tissue
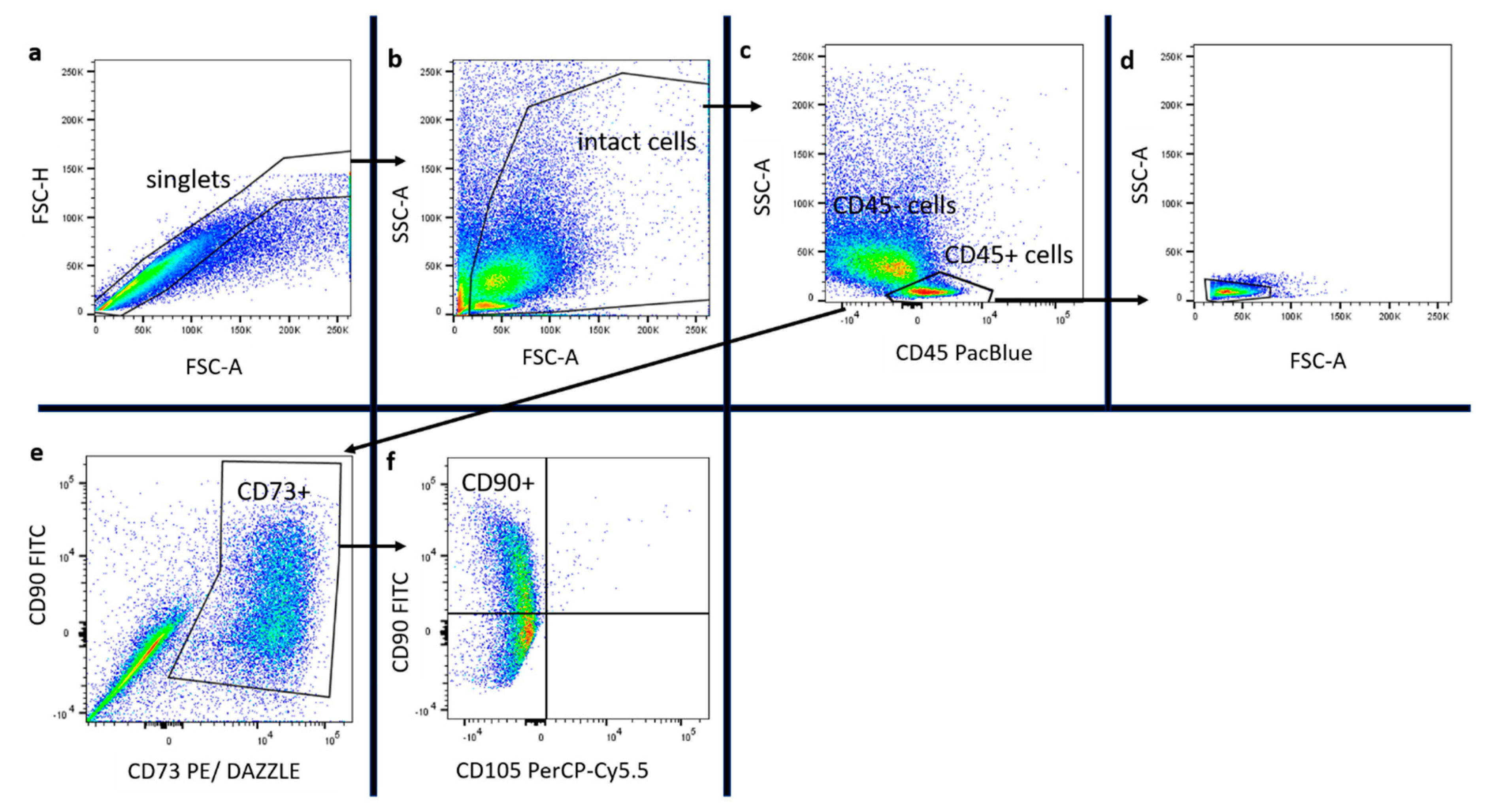
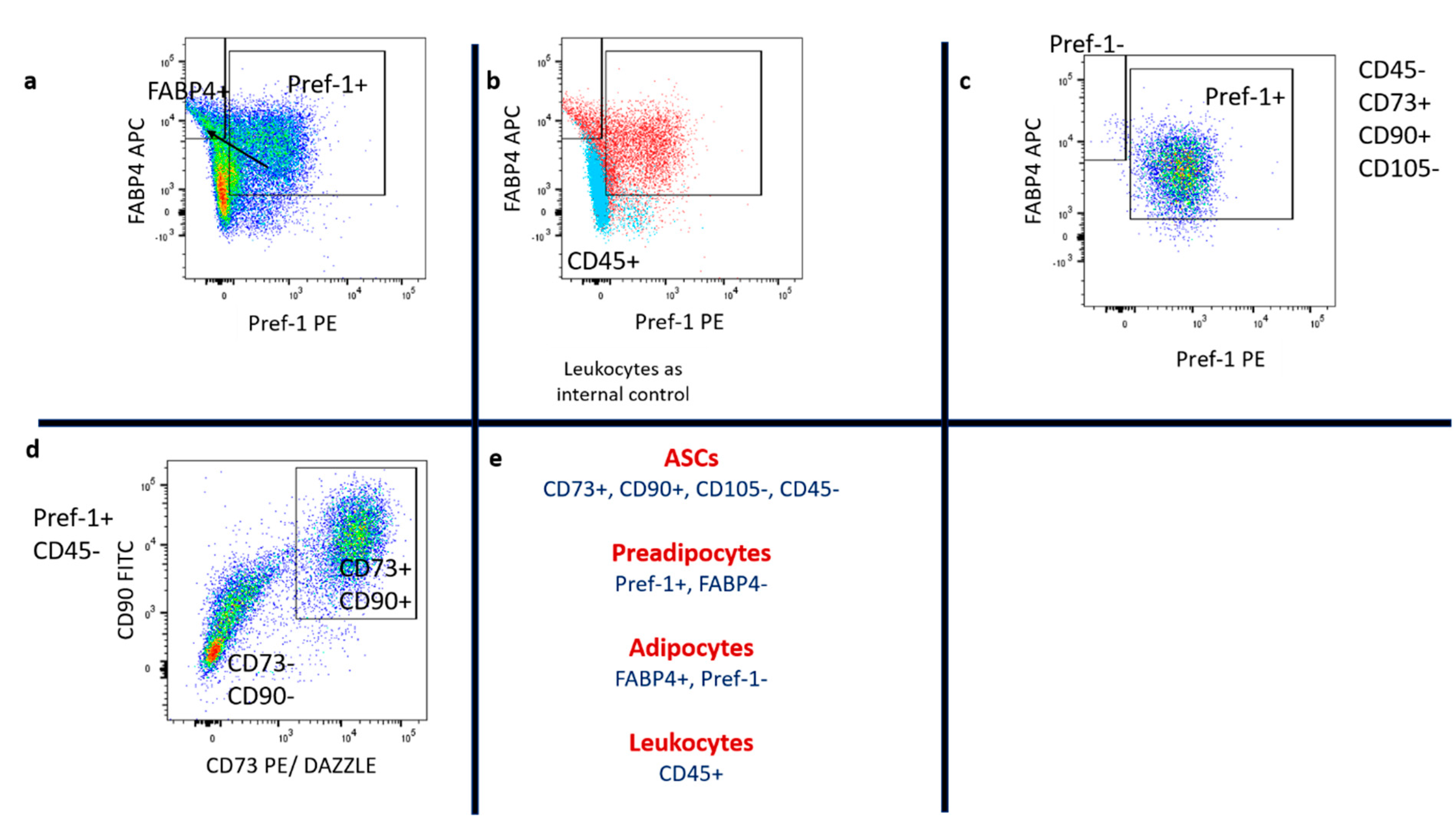
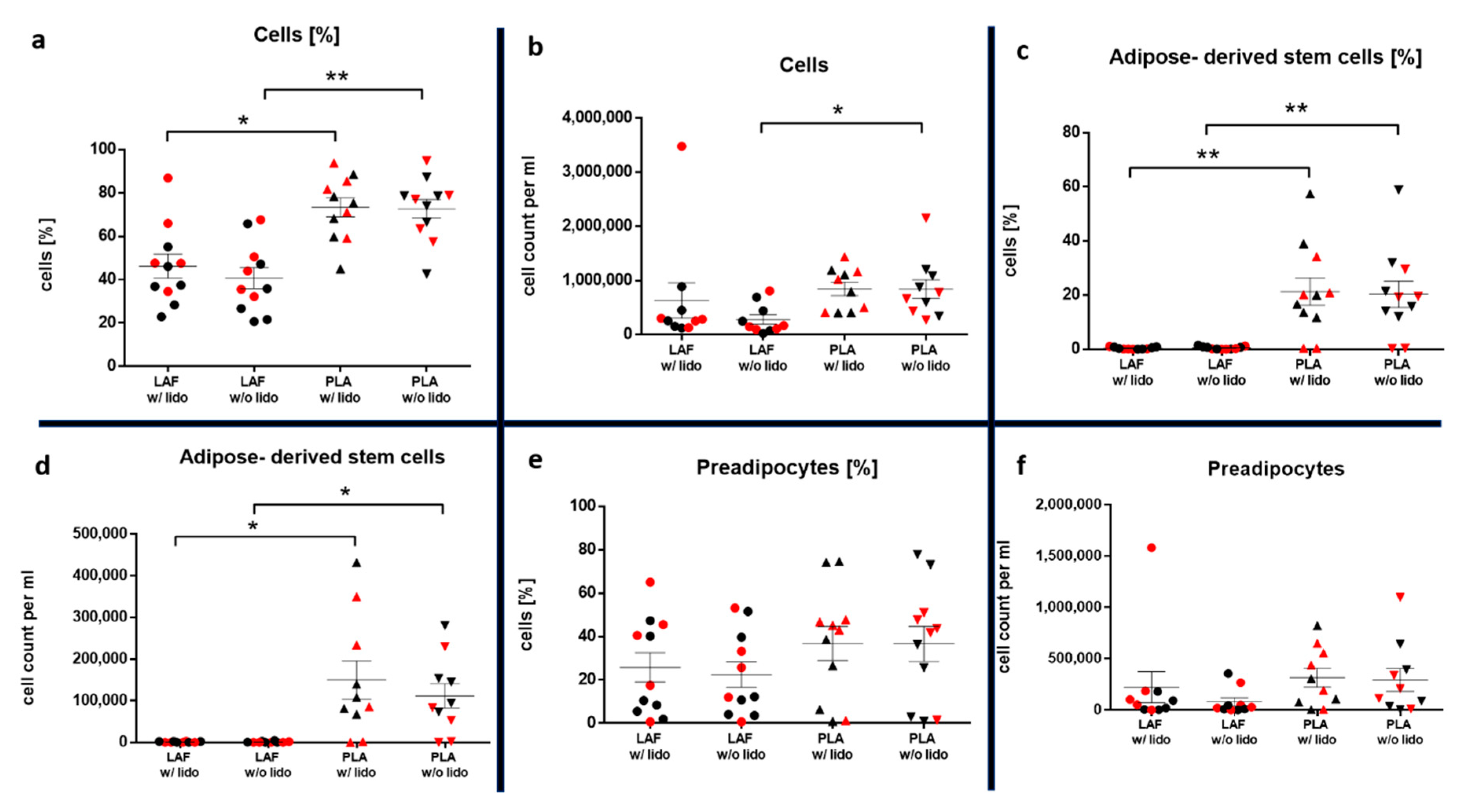
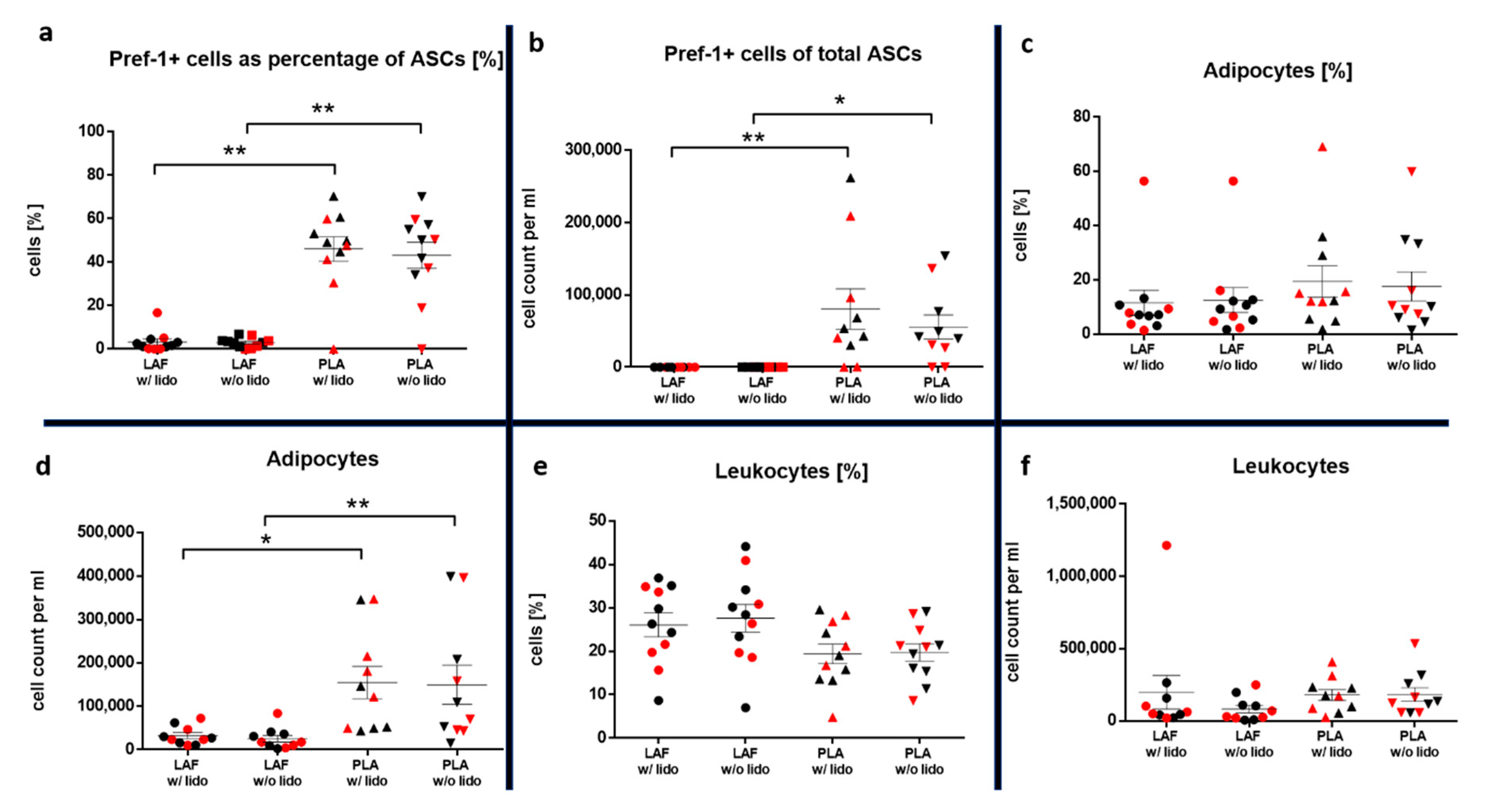
2.3. Hematoxylin-Eosin (HE) Staining, Immunostaining and Flow Cytometry of Processed Lipoaspirate
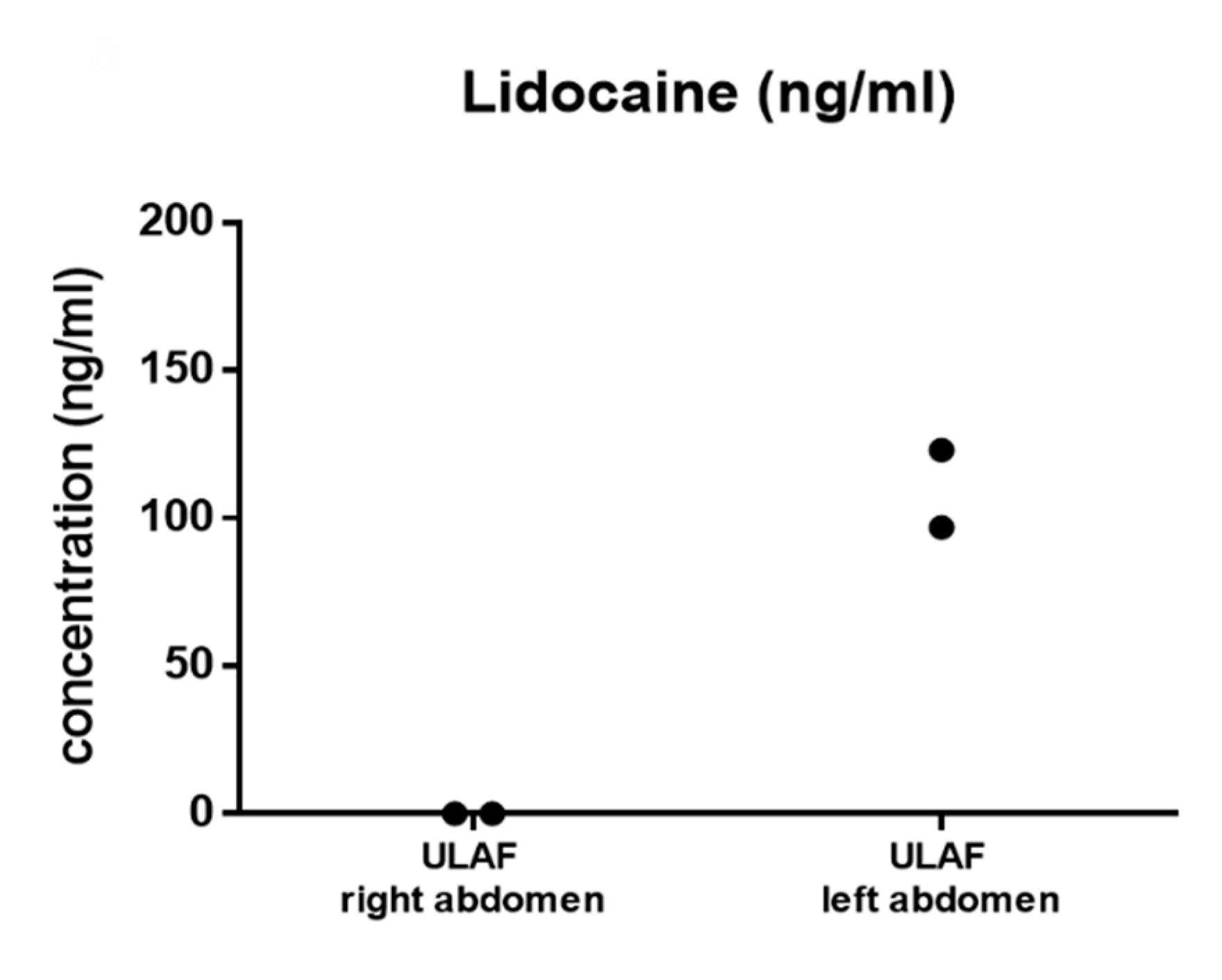
2.4. Evaluation of Lidocaine Distribution Using GC-MS
3. Discussion
4. Methods
4.1. Written Informed Consent and Ethical Approval
4.2. Tissue Harvesting by Liposuction and Abdominoplasty
4.3. Hematoxylin-Eosin (HE) Staining of Unprocessed Lipoaspirate and Fat Piece
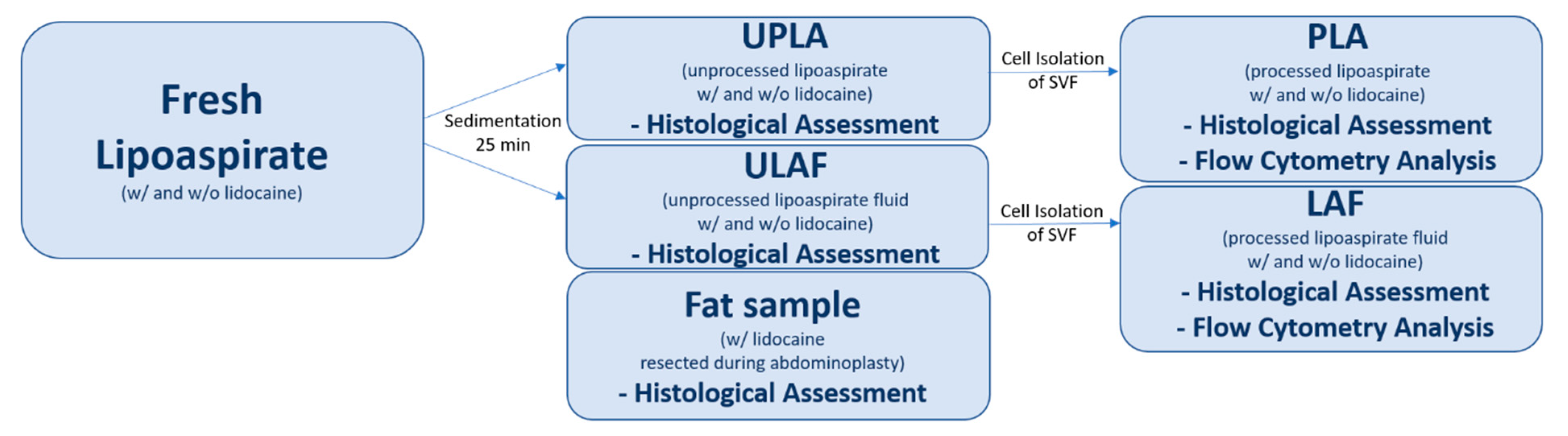
4.4. Processing of Lipoaspirate
4.4.1. Cell Isolation from ULAF and UPLA
4.4.2. HE Staining of a Single Cell Suspension
4.4.3. Immunostaining and Measurement by Flow Cytometry
4.5. GC-MS Evaluation of Method
4.6. Statistics
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ULAF | Unprocessed liposuction aspirate fluid |
| UPLA | Unprocessed lipoaspirate |
| LAF | Processed liposuction aspirate fluid |
| PLA | Processed lipoaspirate |
| MSC | Mesenchymal stem cells |
| ASC | Adipose derived stem cells |
| SVF | Stromal-vascular fraction |
| SEM | Standard error of the mean |
| GC-MS | Gas chromatography mass spectroscopy |
References
- Szychta, P.; Zadrozny, M.; Rykala, J.; Banasiak, L.; Witmanowski, H. Autologous fat transfer to the subcutaneous tissue in the context of breast reconstructive procedures. Postepy Dermatol. Alergol. 2016, 33, 323–328. [Google Scholar] [CrossRef] [Green Version]
- Mazzola, I.C.; Cantarella, G.; Mazzola, R.F. Management of tracheostomy scar by autologous fat transplantation: A minimally invasive new approach. J. Craniofac. Surg. 2013, 24, 1361–1364. [Google Scholar] [CrossRef]
- Salgarello, M.; Visconti, G.; Barone-Adesi, L. Fat grafting and breast reconstruction with implant: Another option for irradiated breast cancer patients. Plast. Reconstr. Surg. 2012, 129, 317–329. [Google Scholar] [CrossRef]
- Klinger, M.; Marazzi, M.; Vigo, D.; Torre, M. Fat injection for cases of severe burn outcomes: A new perspective of scar remodeling and reduction. Aesthetic Plast. Surg. 2008, 32, 465–469. [Google Scholar] [CrossRef] [PubMed]
- Uzzan, C.; Boccara, D.; Lacheré, A.; Mimoun, M.; Chaouat, M. Traitement de la lipoatrophie faciale par lipofilling chez les patients infectés par le VIH: Étude rétrospective de 317 patients sur neuf ans. Ann. Chir. Plast. Esthet. 2012, 57, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.S.; Lanni, M.A.; Lamelas, A.M.; Tecce, M.G.; Bucky, L.P. Abstract: Identifying Risk Factors for Fat Necrosis After Autologous Fat Transplantation to the Breast. Plast. Reconstr. Surg. Glob. Open 2016, 4. [Google Scholar] [CrossRef]
- Katzel, E.B.; Bucky, L.P. Fat Grafting to the Breast: Clinical Applications and Outcomes for Reconstructive Surgery. Plast. Reconstr. Surg. 2017, 140, 69S–76S. [Google Scholar] [CrossRef] [PubMed]
- Tiryaki, T.; Findikli, N.; Tiryaki, D. Staged stem cell-enriched tissue (SET) injections for soft tissue augmentation in hostile recipient areas: A preliminary report. Aesthetic Plast. Surg. 2011, 35, 965–971. [Google Scholar] [CrossRef] [PubMed]
- Gir, P.; Brown, S.A.; Oni, G.; Kashefi, N.; Mojallal, A.; Rohrich, R.J. Fat grafting: Evidence-based review on autologous fat harvesting, processing, reinjection, and storage. Plast. Reconstr. Surg. 2012, 130, 249–258. [Google Scholar] [CrossRef]
- Ross, R.J.; Shayan, R.; Mutimer, K.L.; Ashton, M.W. Autologous fat grafting: Current state of the art and critical review. Ann. Plast. Surg. 2014, 73, 352–357. [Google Scholar] [CrossRef] [PubMed]
- Strong, A.L.; Cederna, P.S.; Rubin, J.P.; Coleman, S.R.; Levi, B. The Current State of Fat Grafting: A Review of Harvesting, Processing, and Injection Techniques. Plast. Reconstr. Surg. 2015, 136, 897–912. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Wu, Y. Assessment of the clinical efficacy of cell-assisted lipotransfer and conventional fat graft: A meta-analysis based on case-control studies. J. Orthop. Surg. Res. 2017, 12, 155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurita, M.; Matsumoto, D.; Shigeura, T.; Sato, K.; Gonda, K.; Harii, K.; Yoshimura, K. Influences of centrifugation on cells and tissues in liposuction aspirates: Optimized centrifugation for lipotransfer and cell isolation. Plast. Reconstr. Surg. 2008, 121, 1033–1041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Condé-Green, A.; de Amorim, N.F.G.; Pitanguy, I. Influence of decantation, washing and centrifugation on adipocyte and mesenchymal stem cell content of aspirated adipose tissue: A comparative study. J. Plast. Reconstr. Aesthet. Surg. 2010, 63, 1375–1381. [Google Scholar] [CrossRef]
- Wronska, A.; Kmiec, Z. Structural and biochemical characteristics of various white adipose tissue depots. Acta Physiol. (Oxf) 2012, 205, 194–208. [Google Scholar] [CrossRef] [PubMed]
- Zuk, P.A.; Zhu, M.; Ashjian, P.; de Ugarte, D.A.; Huang, J.I.; Mizuno, H.; Alfonso, Z.C.; Fraser, J.K.; Benhaim, P.; Hedrick, M.H. Human adipose tissue is a source of multipotent stem cells. Mol. Biol. Cell 2002, 13, 4279–4295. [Google Scholar] [CrossRef] [PubMed]
- Zhu, M.; Zhou, Z.; Chen, Y.; Schreiber, R.; Ransom, J.T.; Fraser, J.K.; Hedrick, M.H.; Pinkernell, K.; Kuo, H.-C. Supplementation of fat grafts with adipose-derived regenerative cells improves long-term graft retention. Ann. Plast. Surg. 2010, 64, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Zuk, P.A.; Zhu, M.; Mizuno, H.; Huang, J.; Futrell, J.W.; Katz, A.J.; Benhaim, P.; Lorenz, H.P.; Hedrick, M.H. Multilineage cells from human adipose tissue: Implications for cell-based therapies. Tissue Eng. 2001, 7, 211–228. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez, A.-M.; Elabd, C.; Amri, E.-Z.; Ailhaud, G.; Dani, C. The human adipose tissue is a source of multipotent stem cells. Biochimie 2005, 87, 125–128. [Google Scholar] [CrossRef]
- Rada, T.; Reis, R.L.; Gomes, M.E. Distinct stem cells subpopulations isolated from human adipose tissue exhibit different chondrogenic and osteogenic differentiation potential. Stem Cell Rev. 2011, 7, 64–76. [Google Scholar] [CrossRef] [Green Version]
- Kraus, A.; Woon, C.; Raghavan, S.; Megerle, K.; Pham, H.; Chang, J. Co-culture of human adipose-derived stem cells with tenocytes increases proliferation and induces differentiation into a tenogenic lineage. Plast. Reconstr. Surg. 2013, 132, 754e–766e. [Google Scholar] [CrossRef] [PubMed]
- Dykstra, J.A.; Facile, T.; Patrick, R.J.; Francis, K.R.; Milanovich, S.; Weimer, J.M.; Kota, D.J. Concise Review: Fat and Furious: Harnessing the Full Potential of Adipose-Derived Stromal Vascular Fraction. Stem Cells Transl. Med. 2017, 6, 1096–1108. [Google Scholar] [CrossRef] [PubMed]
- Rosen, E.D.; MacDougald, O.A. Adipocyte differentiation from the inside out. Nat. Rev. Mol. Cell Biol. 2006, 7, 885–896. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, M.R.; Bradley, J.P.; Dickinson, B.; Heller, J.B.; Wasson, K.; O’Hara, C.; Huang, C.; Gabbay, J.; Ghadjar, K.; Miller, T.A. Autologous fat transfer national consensus survey: Trends in techniques for harvest, preparation, and application, and perception of short- and long-term results. Plast. Reconstr. Surg. 2007, 119, 323–331. [Google Scholar] [CrossRef]
- Klein, J.A. Tumescent technique for regional anesthesia permits lidocaine doses of 35 mg/kg for liposuction. J. Dermatol. Surg. Oncol. 1990, 16, 248–263. [Google Scholar] [CrossRef]
- Klein, J.A. Intravenous fluids and bupivacaine are contraindicated in tumescent liposuction. Plast. Reconstr. Surg. 1998, 102, 2516–2519. [Google Scholar] [CrossRef]
- AC, G. Local Anesthetics: Use and Effects in Autologous fat Grafting. Surgery 2013, 3. [Google Scholar] [CrossRef] [Green Version]
- Keck, M.; Zeyda, M.; Gollinger, K.; Burjak, S.; Kamolz, L.-P.; Frey, M.; Stulnig, T.M. Local anesthetics have a major impact on viability of preadipocytes and their differentiation into adipocytes. Plast. Reconstr. Surg. 2010, 126, 1500–1505. [Google Scholar] [CrossRef]
- McLure, H.A.; Rubin, A.P. Review of local anaesthetic agents. Minerva Anestesiol. 2005, 71, 59–74. [Google Scholar]
- Koh, Y.J.; Koh, B.I.; Kim, H.; Joo, H.J.; Jin, H.K.; Jeon, J.; Choi, C.; Lee, D.H.; Chung, J.H.; Cho, C.-H.; et al. Stromal vascular fraction from adipose tissue forms profound vascular network through the dynamic reassembly of blood endothelial cells. Arterioscler. Thromb. Vasc. Biol. 2011, 31, 1141–1150. [Google Scholar] [CrossRef] [Green Version]
- Shin, S.; Choi, J.-W.; Lim, S.; Lee, S.; Jun, E.-Y.; Sun, H.-M.; Kim, I.-K.; Lee, H.-B.; Kim, S.W.; Hwang, K.-C. Anti-apoptotic effects of adipose-derived adherent stromal cells in mesenchymal stem cells exposed to oxidative stress. Cell Biochem. Funct. 2018, 36, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Girard, A.-C.; Atlan, M.; Bencharif, K.; Gunasekaran, M.K.; Delarue, P.; Hulard, O.; Lefebvre-d’Hellencourt, C.; Roche, R.; Hoareau, L.; Festy, F. New insights into lidocaine and adrenaline effects on human adipose stem cells. Aesthetic Plast. Surg. 2013, 37, 144–152. [Google Scholar] [CrossRef] [PubMed]
- Shoshani, O.; Berger, J.; Fodor, L.; Ramon, Y.; Shupak, A.; Kehat, I.; Gilhar, A.; Ullmann, Y. The effect of lidocaine and adrenaline on the viability of injected adipose tissue--an experimental study in nude mice. J. Drugs Dermatol. 2005, 4, 311–316. [Google Scholar] [PubMed]
- Livaoğlu, M.; Buruk, C.K.; Uraloğlu, M.; Ersöz, S.; Livaogğlu, A.; Sözen, E.; Agdoğan, Ö. Effects of lidocaine plus epinephrine and prilocaine on autologous fat graft survival. J. Craniofac. Surg. 2012, 23, 1015–1018. [Google Scholar] [CrossRef]
- Moore, J.H.; Kolaczynski, J.W.; Morales, L.M.; Considine, R.V.; Pietrzkowski, Z.; Noto, P.F.; Caro, J.F. Viability of fat obtained by syringe suction lipectomy: Effects of local anesthesia with lidocaine. Aesthetic Plast. Surg. 1995, 19, 335–339. [Google Scholar] [CrossRef]
- Becker, D.E.; Reed, K.L. Local Anesthetics: Review of Pharmacological Considerations. Anesth. Prog. 2012, 59, 90–102. [Google Scholar] [CrossRef] [Green Version]
- Goldman, J.J.; Wang, W.Z.; Fang, X.-H.; Williams, S.J.; Baynosa, R.C. Tumescent Liposuction without Lidocaine. Plast. Reconstr. Surg. Glob. Open 2016, 4, e829. [Google Scholar] [CrossRef]
- Harris, M.; Chung, F. Complications of general anesthesia. Clin. Plast. Surg. 2013, 40, 503–513. [Google Scholar] [CrossRef]
- Sood, J.; Jayaraman, L.; Sethi, N. Liposuction: Anaesthesia challenges. Indian J. Anaesth. 2011, 55, 220–227. [Google Scholar] [CrossRef]
- Alaaeddine, N.; El Atat, O.; Saliba, N.; Feghali, Z.; Nasr, M.; Tarabey, B.; Hilal, G.; Hashim, H. Effect of age and body mass index on the yield of stromal vascular fraction. J. Cosmet. Dermatol. 2018, 17, 1233–1239. [Google Scholar] [CrossRef]
- Rohrich, R.J.; Sorokin, E.S.; Brown, S.A. In search of improved fat transfer viability: A quantitative analysis of the role of centrifugation and harvest site. Plast. Reconstr. Surg. 2004, 113, 391–395. [Google Scholar] [CrossRef] [PubMed]
- Aust, L.; Devlin, B.; Foster, S.J.; Halvorsen, Y.D.C.; Hicok, K.; Du Laney, T.; Sen, A.; Willingmyre, G.D.; Gimble, J.M. Yield of human adipose-derived adult stem cells from liposuction aspirates. Cytotherapy 2004, 6, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Nikoletopoulou, V.; Markaki, M.; Palikaras, K.; Tavernarakis, N. Crosstalk between apoptosis, necrosis and autophagy. Biochim. Biophys. Acta 2013, 1833, 3448–3459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keck, M.; Zeyda, M.; Burjak, S.; Kamolz, L.-P.; Selig, H.; Stulnig, T.M.; Frey, M. Coenzyme Q10 does not enhance preadipocyte viability in an in vitro lipotransfer model. Aesthetic Plast. Surg. 2012, 36, 453–457. [Google Scholar] [CrossRef]
- Perfetto, S.P.; Chattopadhyay, P.K.; Lamoreaux, L.; Nguyen, R.; Ambrozak, D.; Koup, R.A.; Roederer, M. Amine-Reactive Dyes for Dead Cell Discrimination in Fixed Samples. Curr. Protoc. Cytom. 2010, 53, 9.34.1–9.34.14. [Google Scholar] [CrossRef] [Green Version]
- Cawthorn, W.P.; Scheller, E.L.; MacDougald, O.A. Adipose tissue stem cells meet preadipocyte commitment: Going back to the future. J. Lipid Res. 2012, 53, 227–246. [Google Scholar] [CrossRef] [Green Version]
- Sidney, L.E.; Branch, M.J.; Dunphy, S.E.; Dua, H.S.; Hopkinson, A. Concise review: Evidence for CD34 as a common marker for diverse progenitors. Stem Cells 2014, 32, 1380–1389. [Google Scholar] [CrossRef] [Green Version]
- Dominici, M.; Le Blanc, K.; Mueller, I.; Slaper-Cortenbach, I.; Marini, F.; Krause, D.; Deans, R.; Keating, A.; Prockop, D.; Horwitz, E. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy 2006, 8, 315–317. [Google Scholar] [CrossRef]
- Corselli, M.; Chen, C.-W.; Sun, B.; Yap, S.; Rubin, J.P.; Péault, B. The tunica adventitia of human arteries and veins as a source of mesenchymal stem cells. Stem Cells Dev. 2012, 21, 1299–1308. [Google Scholar] [CrossRef] [Green Version]
- Zimmerlin, L.; Donnenberg, V.S.; Pfeifer, M.E.; Meyer, E.M.; Péault, B.; Rubin, J.P.; Donnenberg, A.D. Stromal vascular progenitors in adult human adipose tissue. Cytometry A 2010, 77, 22–30. [Google Scholar] [CrossRef]
- Chen, C.-W.; Montelatici, E.; Crisan, M.; Corselli, M.; Huard, J.; Lazzari, L.; Péault, B. Perivascular multi-lineage progenitor cells in human organs: Regenerative units, cytokine sources or both? Cytokine Growth Factor Rev. 2009, 20, 429–434. [Google Scholar] [CrossRef] [PubMed]
- Zimmerlin, L.; Donnenberg, V.S.; Rubin, J.P.; Donnenberg, A.D. Mesenchymal markers on human adipose stem/progenitor cells. Cytometry A 2013, 83, 134–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crisan, M.; Yap, S.; Casteilla, L.; Chen, C.-W.; Corselli, M.; Park, T.S.; Andriolo, G.; Sun, B.; Zheng, B.; Zhang, L.; et al. A perivascular origin for mesenchymal stem cells in multiple human organs. Cell Stem Cell 2008, 3, 301–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshimura, K.; Shigeura, T.; Matsumoto, D.; Sato, T.; Takaki, Y.; Aiba-Kojima, E.; Sato, K.; Inoue, K.; Nagase, T.; Koshima, I.; et al. Characterization of freshly isolated and cultured cells derived from the fatty and fluid portions of liposuction aspirates. J. Cell. Physiol. 2006, 208, 64–76. [Google Scholar] [CrossRef] [PubMed]
- Hudak, C.S.; Gulyaeva, O.; Wang, Y.; Park, S.-M.; Lee, L.; Kang, C.; Sul, H.S. Pref-1 marks very early mesenchymal precursors required for adipose tissue development and expansion. Cell Rep. 2014, 8, 678–687. [Google Scholar] [CrossRef] [Green Version]
- Hudak, C.S.; Sul, H.S. Pref-1, a gatekeeper of adipogenesis. Front. Endocrinol. (Lausanne) 2013, 4, 79. [Google Scholar] [CrossRef] [Green Version]
- Mitterberger, M.C.; Lechner, S.; Mattesich, M.; Kaiser, A.; Probst, D.; Wenger, N.; Pierer, G.; Zwerschke, W. DLK1(PREF1) is a negative regulator of adipogenesis in CD105⁺/CD90⁺/CD34⁺/CD31⁻/FABP4⁻ adipose-derived stromal cells from subcutaneous abdominal fat pats of adult women. Stem Cell Res. 2012, 9, 35–48. [Google Scholar] [CrossRef] [Green Version]
- Aldridge, A.; Kouroupis, D.; Churchman, S.; English, A.; Ingham, E.; Jones, E. Assay validation for the assessment of adipogenesis of multipotential stromal cells--a direct comparison of four different methods. Cytotherapy 2013, 15, 89–101. [Google Scholar] [CrossRef] [Green Version]
- Parlee, S.D.; Lentz, S.I.; Mori, H.; MacDougald, O.A. Quantifying Size and Number of Adipocytes in Adipose Tissue. Meth. Enzymol. 2014, 537, 93–122. [Google Scholar] [CrossRef] [Green Version]
- Anderson, E.K.; Gutierrez, D.A.; Hasty, A.H. Adipose tissue recruitment of leukocytes. Curr. Opin. Lipidol. 2010, 21, 172–177. [Google Scholar] [CrossRef]
- Wu, T.; Smith, J.; Nie, H.; Wang, Z.; Erwin, P.J.; van Wijnen, A.J.; Qu, W. Cytotoxicity of Local Anesthetics in Mesenchymal Stem Cells. Am. J. Phys. Med. Rehabil. 2018, 97, 50–55. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Age | BMI | Weight Gain/Loss in Last 6 Months | W:H Ratio | Diabetes |
|---|---|---|---|---|---|
| 1 | 43 | 26 | no | 0.854 | no |
| 2 | 44 | 35 | yes, −5 kg | 1.026 | no |
| 3 | 35 | 48 | no | 0.91 | no |
| 4 | 30 | 30 | yes, −5 kg | 0.63 | no |
| 5 | 41 | 26 | yes, −5 kg | 0.78 | no |
| 6 | 27 | 26 | yes, −5 kg | 0.85 | no |
| 7 | 48 | 29 | no | 0.85 | no |
| 8 | 37 | 25 | no | 0.97 | no |
| 9 | 52 | 34 | no | 0.96 | no |
| 10 | 60 | 25 | yes, −5 kg | 0.83 | no |
| 11 | 19 | 32 | no | 0.8 | no |
| Mean | 42 | 30.2 | 0.86 | ||
| SEM | 3.54 | 2.06 | 0.03 |
| w/Lido | w/o Lido | ||||
|---|---|---|---|---|---|
| ASCs (viable) | PLA | % | 25.5 | 28.9 | |
| SEM | 15.6 | 18.1 | |||
| Cells/mL | 25,109 | 32,113 | |||
| SEM | 15,828 | 23,670 | |||
| Preadipocyte (viable) | LAF | % | 93 | 93 | |
| SEM | 3.4 | 2.59 | |||
| Cells/mL | 38,380 | 15,848 | |||
| SEM | 21,419 | 7851 | |||
| PLA | % | 70 | 77.9 | ||
| SEM | 15 | 8.5 | |||
| Cells/mL | 88,756 | 87,814 | |||
| SEM | 44,411 | 58,406 | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grambow, F.; Rutkowski, R.; Podmelle, F.; Schmoeckel, K.; Siegerist, F.; Domanski, G.; Schuster, M.W.; Domanska, G. The Impact of Lidocaine on Adipose-Derived Stem Cells in Human Adipose Tissue Harvested by Liposuction and Used for Lipotransfer. Int. J. Mol. Sci. 2020, 21, 2869. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21082869
Grambow F, Rutkowski R, Podmelle F, Schmoeckel K, Siegerist F, Domanski G, Schuster MW, Domanska G. The Impact of Lidocaine on Adipose-Derived Stem Cells in Human Adipose Tissue Harvested by Liposuction and Used for Lipotransfer. International Journal of Molecular Sciences. 2020; 21(8):2869. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21082869
Chicago/Turabian StyleGrambow, Felix, Rico Rutkowski, Fred Podmelle, Katrin Schmoeckel, Florian Siegerist, Grzegorz Domanski, Matthias W. Schuster, and Grazyna Domanska. 2020. "The Impact of Lidocaine on Adipose-Derived Stem Cells in Human Adipose Tissue Harvested by Liposuction and Used for Lipotransfer" International Journal of Molecular Sciences 21, no. 8: 2869. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21082869