Correlation of RAS-Pathway Mutations and Spontaneous Myeloid Colony Growth with Progression and Transformation in Chronic Myelomonocytic Leukemia—A Retrospective Analysis in 337 Patients

 , , , , , and add
Show full author list
, , , , , and add
Show full author list
Abstract
:1. Introduction
2. Results
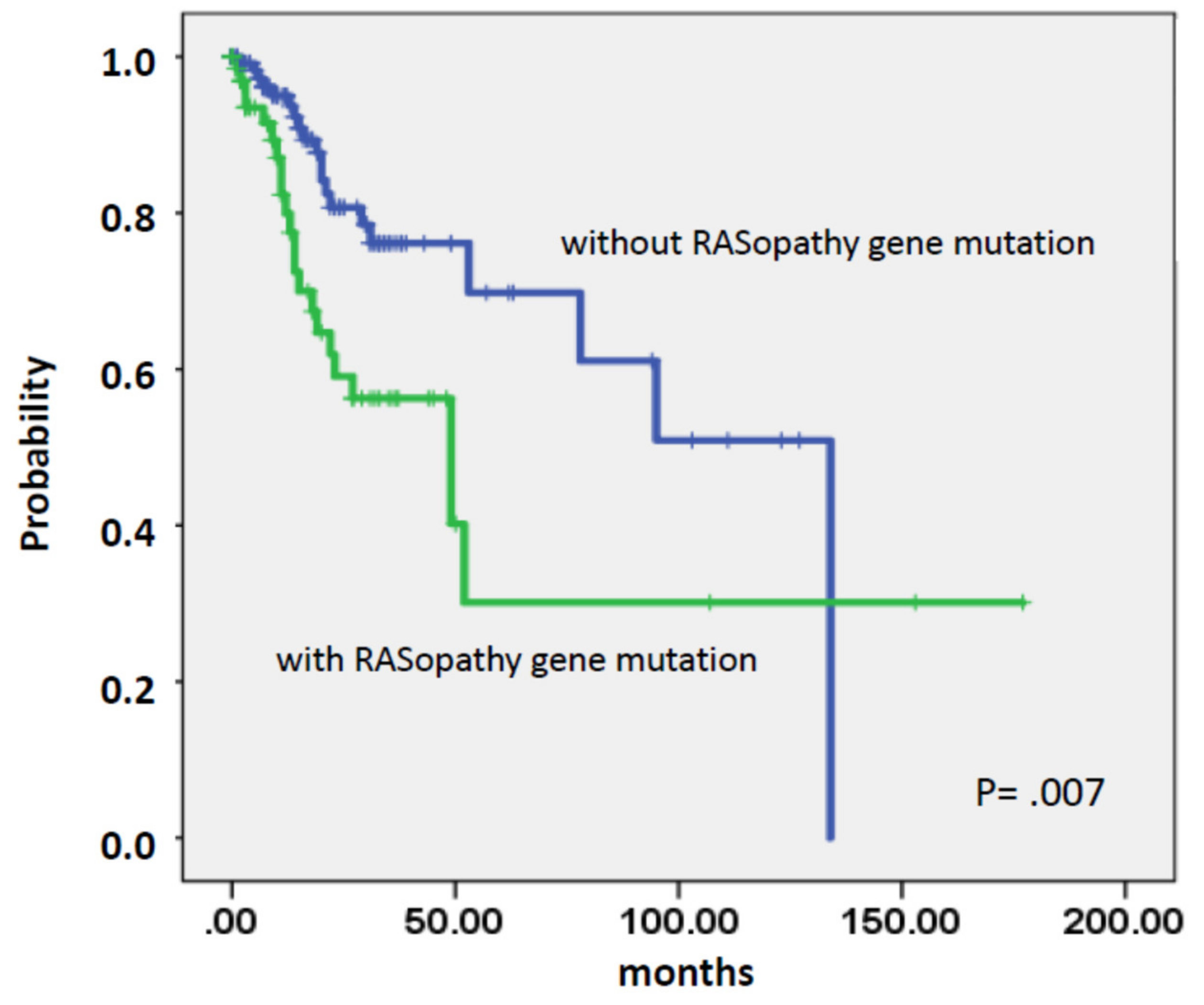
2.1. Impact of Disease Stage on Survival in Patients with CMML
2.2. Hematologic and Cytogenetic Characteristics in Patient-Subgroups
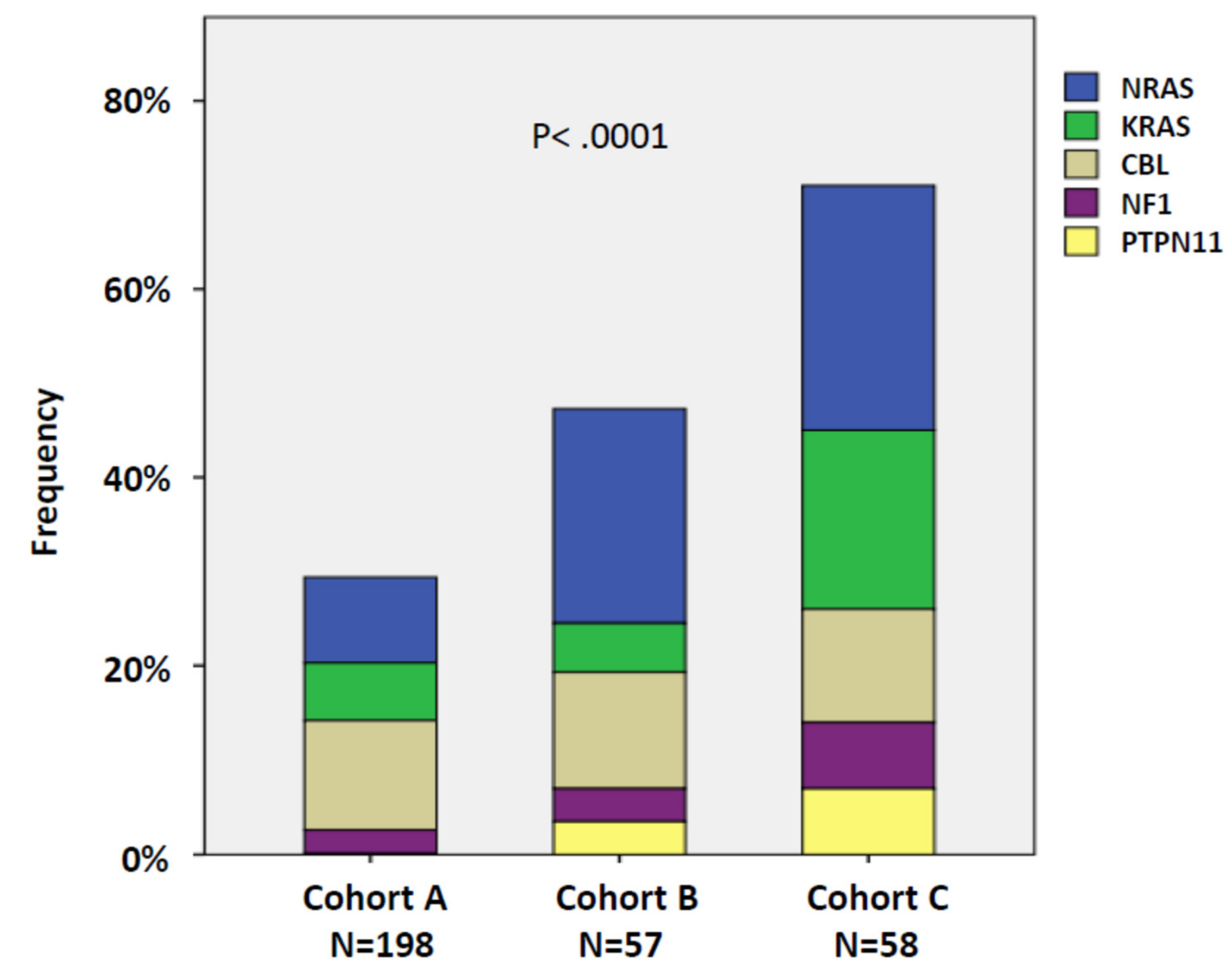
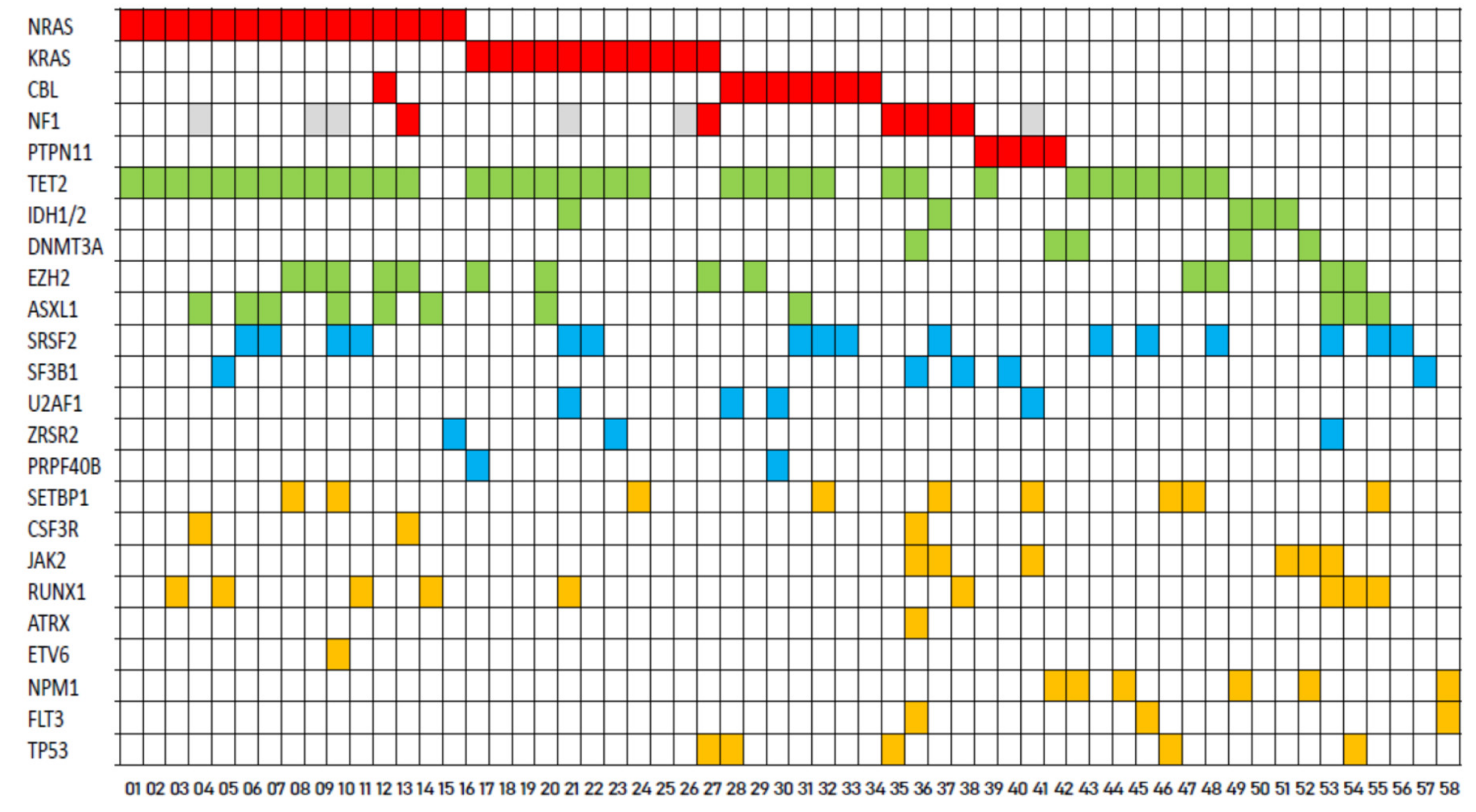
2.3. RAS-Pathway Mutations Correlate with AML Evolution in Patients with CMML
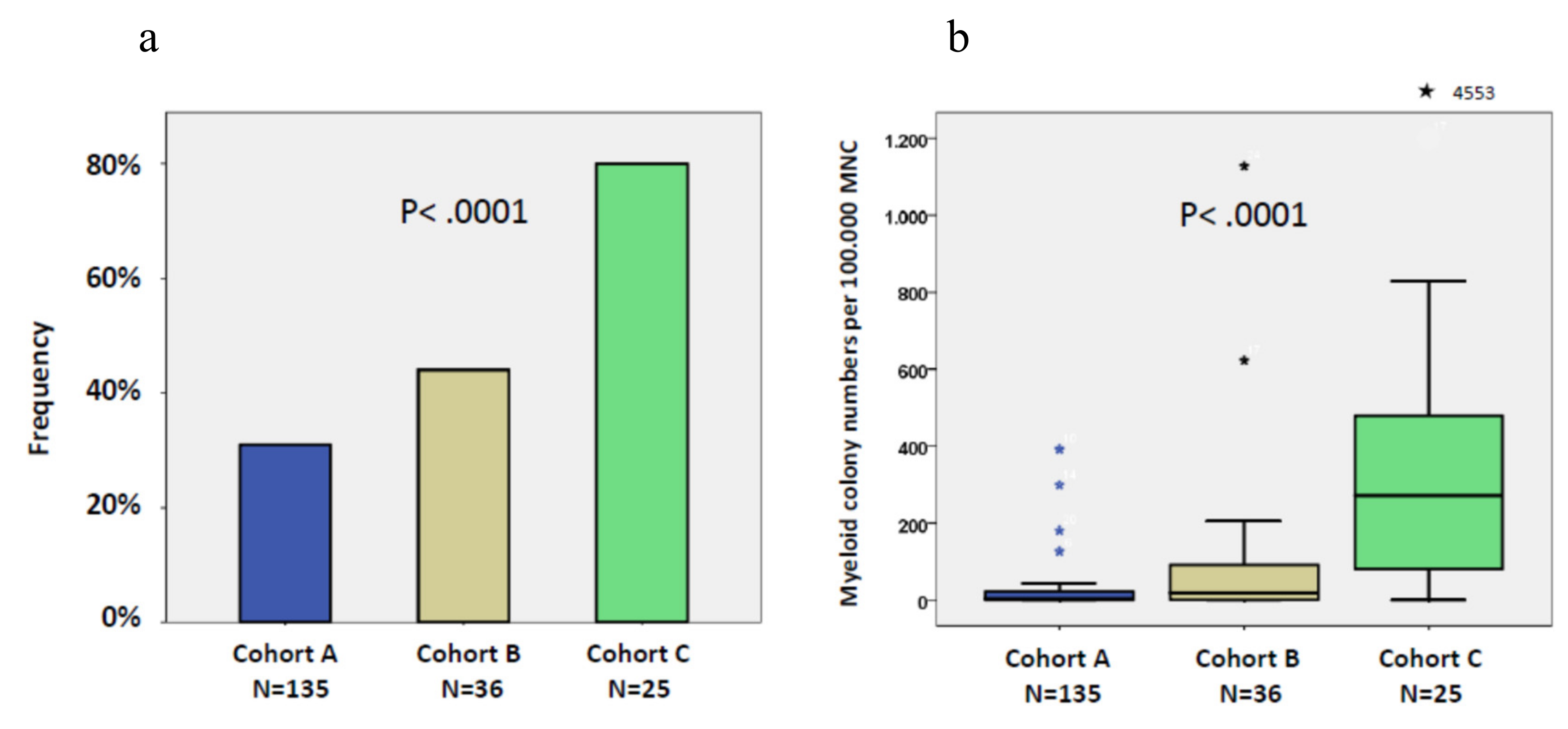
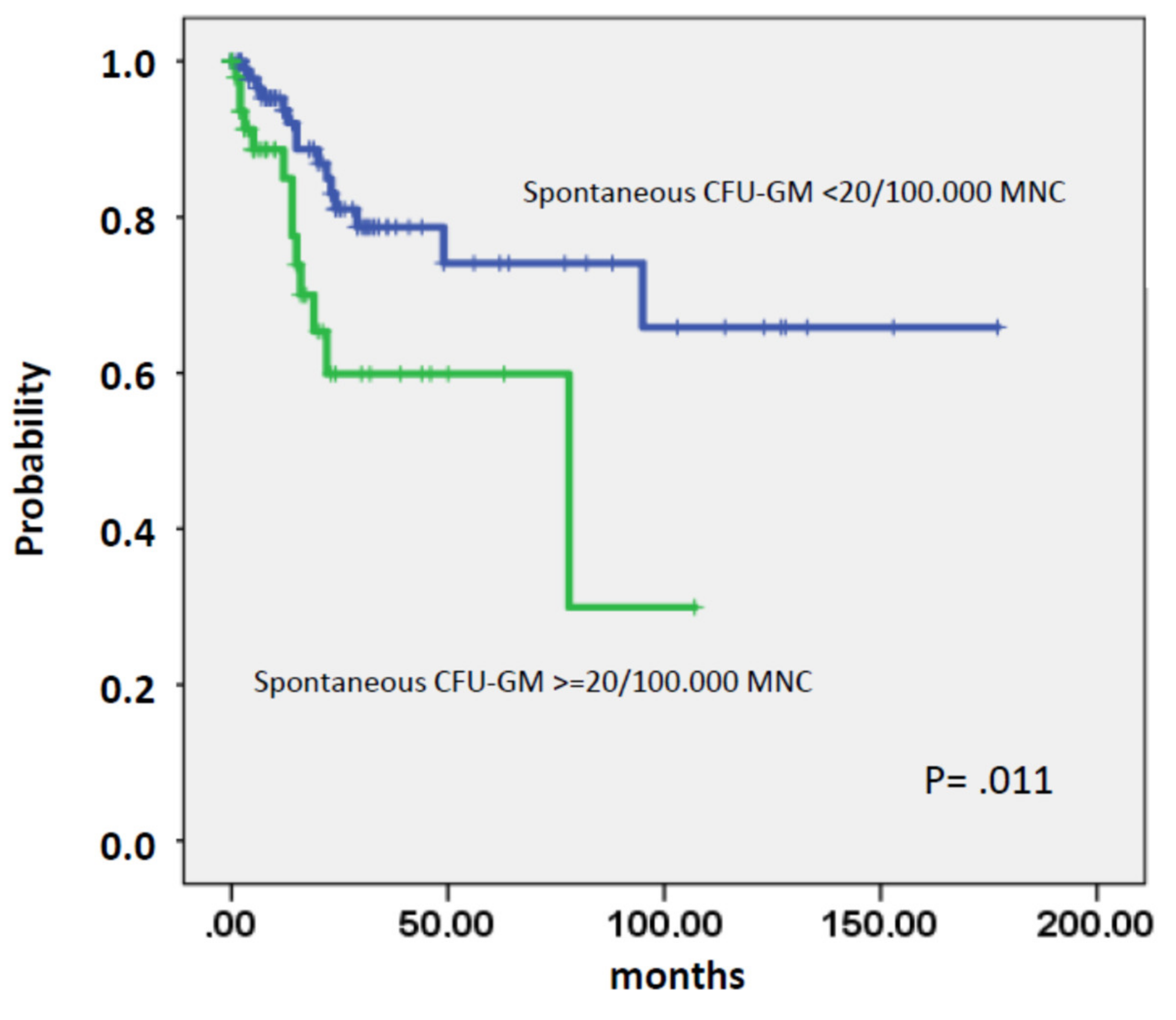
2.4. High Autonomous in Vitro Colony Formation Correlates with AML Evolution in Patients with CMML
3. Discussion
4. Patients and Methods
4.1. Patients
4.2. Cytogenetic Analysis
4.3. Molecular Studies
4.4. Colony Assay
4.5. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Bennett, J.M.; Catovsky, D.; Daniel, M.T.; Flandrin, G.; Galton, D.A.; Gralnick, H.R.; Sultan, C. Proposals for the Classification of the Myelodysplastic Syndromes. Br. J. Haematol. 1982, 51, 189–199. [Google Scholar] [CrossRef] [PubMed]
- Vardiman, J.W.; Harris, N.L.; Brunning, R.D. The World Health Organization (WHO) Classification of the Myeloid Neoplasms. Blood 2002, 100, 2292–2302. [Google Scholar] [CrossRef] [PubMed]
- Vardiman, J.W.; Thiele, J.; Arber, D.A.; Brunning, R.D.; Borowitz, M.J.; Porwit, A.; Harris, N.L.; Le Beau, M.M.; Hellström-Lindberg, E.; Tefferi, A.; et al. The 2008 Revision of the World Health Organization (WHO) Classification of Myeloid Neoplasms and Acute Leukemia: Rationale and Important Changes. Blood 2009, 114, 937–951. [Google Scholar] [CrossRef] [Green Version]
- Arber, D.A.; Orazi, A.; Hasserjian, R.; Thiele, J.; Borowitz, M.J.; Le Beau, M.M.; Bloomfield, C.D.; Cazzola, M.; Vardiman, J.W. The 2016 Revision to the World Health Organization Classification of Myeloid Neoplasms and Acute Leukemia. Blood 2016, 127, 2391–2405. [Google Scholar] [CrossRef]
- Padron, E.; Steensma, D.P. Cutting the Cord from Myelodysplastic Syndromes: Chronic Myelomonocytic Leukemia-Specific Biology and Management Strategies. Curr. Opin. Hematol. 2015, 22, 163–170. [Google Scholar] [CrossRef]
- Itzykson, R.; Fenaux, P.; Bowen, D.; Cross, N.C.P.; Cortes, J.; De Witte, T.; Germing, U.; Onida, F.; Padron, E.; Platzbecker, U.; et al. Diagnosis and Treatment of Chronic Myelomonocytic Leukemias in Adults: Recommendations From the European Hematology Association and the European LeukemiaNet. HemaSphere 2018, 1. [Google Scholar] [CrossRef]
- Valent, P.; Orazi, A.; Savona, M.R.; Patnaik, M.M.; Onida, F.; van de Loosdrecht, A.A.; Haase, D.; Haferlach, T.; Elena, C.; Pleyer, L.; et al. Proposed Diagnostic Criteria for Classical Chronic Myelomonocytic Leukemia (CMML), CMML Variants and Pre-CMML Conditions. Haematologica 2019, 104, 1935–1949. [Google Scholar] [CrossRef]
- Wattel, E.; Guerci, A.; Hecquet, B.; Economopoulos, T.; Copplestone, A.; Mahé, B.; Couteaux, M.E.; Resegotti, L.; Voglova, V.; Foussard, C.; et al. A Randomized Trial of Hydroxyurea versus VP16 in Adult Chronic Myelomonocytic Leukemia. Groupe Français Des Myélodysplasies and European CMML Group. Blood 1996, 88, 2480–2487. [Google Scholar] [CrossRef]
- Fenaux, P.; Mufti, G.J.; Hellstrom-Lindberg, E.; Santini, V.; Finelli, C.; Giagounidis, A.; Schoch, R.; Gattermann, N.; Sanz, G.; List, A.; et al. Efficacy of Azacitidine Compared with That of Conventional Care Regimens in the Treatment of Higher-Risk Myelodysplastic Syndromes: A Randomised, Open-Label, Phase III Study. Lancet Oncol. 2009, 10, 223–232. [Google Scholar] [CrossRef] [Green Version]
- Aribi, A.; Borthakur, G.; Ravandi, F.; Shan, J.; Davisson, J.; Cortes, J.; Kantarjian, H. Activity of Decitabine, a Hypomethylating Agent, in Chronic Myelomonocytic Leukemia. Cancer 2007, 109, 713–717. [Google Scholar] [CrossRef]
- Ciriello, G.; Cerami, E.; Sander, C.; Schultz, N. Mutual Exclusivity Analysis Identifies Oncogenic Network Modules. Genome Res. 2012, 22, 398–406. [Google Scholar] [CrossRef] [Green Version]
- Patnaik, M.M.; Tefferi, A. Cytogenetic and Molecular Abnormalities in Chronic Myelomonocytic Leukemia. Blood Cancer J. 2016, 6, e393. [Google Scholar] [CrossRef] [PubMed]
- Ricci, C.; Fermo, E.; Corti, S.; Molteni, M.; Faricciotti, A.; Cortelezzi, A.; Lambertenghi Deliliers, G.; Beran, M.; Onida, F. RAS Mutations Contribute to Evolution of Chronic Myelomonocytic Leukemia to the Proliferative Variant. Clin. Cancer Res. 2010, 16, 2246–2256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Itzykson, R.; Kosmider, O.; Renneville, A.; Gelsi-Boyer, V.; Meggendorfer, M.; Morabito, M.; Berthon, C.; Adès, L.; Fenaux, P.; Beyne-Rauzy, O.; et al. Prognostic Score Including Gene Mutations in Chronic Myelomonocytic Leukemia. JCO 2013, 31, 2428–2436. [Google Scholar] [CrossRef] [PubMed]
- Patnaik, M.M.; Itzykson, R.; Lasho, T.L.; Kosmider, O.; Finke, C.M.; Hanson, C.A.; Knudson, R.A.; Ketterling, R.P.; Tefferi, A.; Solary, E. ASXL1 and SETBP1 Mutations and Their Prognostic Contribution in Chronic Myelomonocytic Leukemia: A Two-Center Study of 466 Patients. Leukemia 2014, 28, 2206–2212. [Google Scholar] [CrossRef] [PubMed]
- Elena, C.; Gallì, A.; Such, E.; Meggendorfer, M.; Germing, U.; Rizzo, E.; Cervera, J.; Molteni, E.; Fasan, A.; Schuler, E.; et al. Integrating Clinical Features and Genetic Lesions in the Risk Assessment of Patients with Chronic Myelomonocytic Leukemia. Blood 2016, 128, 1408–1417. [Google Scholar] [CrossRef]
- Patnaik, M.M.; Wassie, E.A.; Lasho, T.L.; Hanson, C.A.; Ketterling, R.; Tefferi, A. Blast Transformation in Chronic Myelomonocytic Leukemia: Risk Factors, Genetic Features, Survival, and Treatment Outcome: Blast Transformation in Chronic Myelomonocytic Leukemia. Am. J. Hematol. 2015, 90, 411–416. [Google Scholar] [CrossRef]
- Geissler, K.; Hinterberger, W.; Bettelheim, P.; Haas, O.; Lechner, K. Colony Growth Characteristics in Chronic Myelomonocytic Leukemia. Leuk. Res. 1988, 12, 373–377. [Google Scholar] [CrossRef]
- Geissler, K.; Ohler, L.; Födinger, M.; Virgolini, I.; Leimer, M.; Kabrna, E.; Kollars, M.; Skoupy, S.; Bohle, B.; Rogy, M.; et al. Interleukin 10 Inhibits Growth and Granulocyte/Macrophage Colony-Stimulating Factor Production in Chronic Myelomonocytic Leukemia Cells. J. Exp. Med. 1996, 184, 1377–1384. [Google Scholar] [CrossRef]
- Padron, E.; Painter, J.S.; Kunigal, S.; Mailloux, A.W.; McGraw, K.; McDaniel, J.M.; Kim, E.; Bebbington, C.; Baer, M.; Yarranton, G.; et al. GM-CSF–Dependent PSTAT5 Sensitivity Is a Feature with Therapeutic Potential in Chronic Myelomonocytic Leukemia. Blood 2013, 121, 5068–5077. [Google Scholar] [CrossRef]
- Wang, J.; Liu, Y.; Li, Z.; Du, J.; Ryu, M.-J.; Taylor, P.R.; Fleming, M.D.; Young, K.H.; Pitot, H.; Zhang, J. Endogenous Oncogenic Nras Mutation Promotes Aberrant GM-CSF Signaling in Granulocytic/Monocytic Precursors in a Murine Model of Chronic Myelomonocytic Leukemia. Blood 2010, 116, 5991–6002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Meter, M.E.M.; Díaz-Flores, E.; Archard, J.A.; Passegué, E.; Irish, J.M.; Kotecha, N.; Nolan, G.P.; Shannon, K.; Braun, B.S. K-RasG12D Expression Induces Hyperproliferation and Aberrant Signaling in Primary Hematopoietic Stem/Progenitor Cells. Blood 2007, 109, 3945–3952. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Q.; Haigis, K.M.; McDaniel, A.; Harding-Theobald, E.; Kogan, S.C.; Akagi, K.; Wong, J.C.Y.; Braun, B.S.; Wolff, L.; Jacks, T.; et al. Hematopoiesis and Leukemogenesis in Mice Expressing Oncogenic NrasG12D from the Endogenous Locus. Blood 2011, 117, 2022–2032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, R.J.; Leedy, M.B.; Munugalavadla, V.; Voorhorst, C.S.; Li, Y.; Yu, M.; Kapur, R. Human Somatic PTPN11 Mutations Induce Hematopoietic-Cell Hypersensitivity to Granulocyte-Macrophage Colony-Stimulating Factor. Blood 2005, 105, 3737–3742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le, D.T.; Kong, N.; Zhu, Y.; Lauchle, J.O.; Aiyigari, A.; Braun, B.S.; Wang, E.; Kogan, S.C.; Le Beau, M.M.; Parada, L.; et al. Somatic Inactivation of Nf1 in Hematopoietic Cells Results in a Progressive Myeloproliferative Disorder. Blood 2004, 103, 4243–4250. [Google Scholar] [CrossRef] [Green Version]
- Geissler, K.; Jäger, E.; Barna, A.; Alendar, T.; Ljubuncic, E.; Sliwa, T.; Valent, P. Chronic Myelomonocytic Leukemia Patients with RAS Pathway Mutations Show High in Vitro Myeloid Colony Formation in the Absence of Exogenous Growth Factors. Leukemia 2016, 30, 2280–2281. [Google Scholar] [CrossRef]
- Geissler, K.; Jäger, E.; Barna, A.; Gurbisz, M.; Marschon, R.; Graf, T.; Graf, E.; Borjan, B.; Jilch, R.; Geissler, C.; et al. The Austrian Biodatabase for Chronic Myelomonocytic Leukemia (ABCMML): A Representative and Useful Real-Life Data Source for Further Biomedical Research. Wien Klin Wochenschr 2019, 131, 410–418. [Google Scholar] [CrossRef] [Green Version]
- Savona, M.R.; Malcovati, L.; Komrokji, R.; Tiu, R.V.; Mughal, T.I.; Orazi, A.; Kiladjian, J.-J.; Padron, E.; Solary, E.; Tibes, R.; et al. An International Consortium Proposal of Uniform Response Criteria for Myelodysplastic/Myeloproliferative Neoplasms (MDS/MPN) in Adults. Blood 2015, 125, 1857–1865. [Google Scholar] [CrossRef] [Green Version]
- Oehler, L.; Foedinger, M.; Koeller, M.; Kollars, M.; Reiter, E.; Bohle, B.; Skoupy, S.; Fritsch, G.; Lechner, K.; Geissler, K. Interleukin-10 Inhibits Spontaneous Colony-Forming Unit-Granulocyte-Macrophage Growth from Human Peripheral Blood Mononuclear Cells by Suppression of Endogenous Granulocyte-Macrophage Colony-Stimulating Factor Release. Blood 1997, 89, 1147–1153. [Google Scholar] [CrossRef]
- Hirsch-Ginsberg, C.; LeMaistre, A.C.; Kantarjian, H.; Talpaz, M.; Cork, A.; Freireich, E.J.; Trujillo, J.M.; Lee, M.S.; Stass, S.A. RAS Mutations Are Rare Events in Philadelphia Chromosome-Negative/Bcr Gene Rearrangement-Negative Chronic Myelogenous Leukemia, but Are Prevalent in Chronic Myelomonocytic Leukemia. Blood 1990, 76, 1214–1219. [Google Scholar] [CrossRef]
- Gelsi-Boyer, V.; Trouplin, V.; Adélaïde, J.; Aceto, N.; Remy, V.; Pinson, S.; Houdayer, C.; Arnoulet, C.; Sainty, D.; Bentires-Alj, M.; et al. Genome Profiling of Chronic Myelomonocytic Leukemia: Frequent Alterations of RAS and RUNX1genes. BMC Cancer 2008, 8, 299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tyner, J.W.; Erickson, H.; Deininger, M.W.N.; Willis, S.G.; Eide, C.A.; Levine, R.L.; Heinrich, M.C.; Gattermann, N.; Gilliland, D.G.; Druker, B.J.; et al. High-Throughput Sequencing Screen Reveals Novel, Transforming RAS Mutations in Myeloid Leukemia Patients. Blood 2009, 113, 1749–1755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orazi, A.; Chiu, R.; O’Malley, D.P.; Czader, M.; Allen, S.L.; An, C.; Vance, G.H. Chronic Myelomonocytic Leukemia: The Role of Bone Marrow Biopsy Immunohistology. Mod. Pathol. 2006, 19, 1536–1545. [Google Scholar] [CrossRef] [PubMed]
- Mossner, M.; Jann, J.-C.; Wittig, J.; Nolte, F.; Fey, S.; Nowak, V.; Obländer, J.; Pressler, J.; Palme, I.; Xanthopoulos, C.; et al. Mutational Hierarchies in Myelodysplastic Syndromes Dynamically Adapt and Evolve upon Therapy Response and Failure. Blood 2016, 128, 1246–1259. [Google Scholar] [CrossRef] [Green Version]
- Constantinidou, M.; Chalevelakis, G.; Economopoulos, T.; Koffa, M.; Liloglou, T.; Anastassiou, C.; Yalouris, A.; Spandidos, D.A.; Raptis, S. Codon 12 Ras Mutations in Patients with Myelodysplastic Syndrome: Incidence and Prognostic Value. Ann. Hematol. 1997, 74, 11–14. [Google Scholar] [CrossRef]
- De Souza Fernandez, T.; Menezes de Souza, J.; Macedo Silva, M.L.; Tabak, D.; Abdelhay, E. Correlation of N-Ras Point Mutations with Specific Chromosomal Abnormalities in Primary Myelodysplastic Syndrome. Leuk. Res. 1998, 22, 125–134. [Google Scholar] [CrossRef]
- Shih, L.-Y.; Huang, C.-F.; Wang, P.-N.; Wu, J.-H.; Lin, T.-L.; Dunn, P.; Kuo, M.-C. Acquisition of FLT3 or N-Ras Mutations Is Frequently Associated with Progression of Myelodysplastic Syndrome to Acute Myeloid Leukemia. Leukemia 2004, 18, 466–475. [Google Scholar] [CrossRef]
- Kunimoto, H.; Meydan, C.; Nazir, A.; Whitfield, J.; Shank, K.; Rapaport, F.; Maher, R.; Pronier, E.; Meyer, S.C.; Garrett-Bakelman, F.E.; et al. Cooperative Epigenetic Remodeling by TET2 Loss and NRAS Mutation Drives Myeloid Transformation and MEK Inhibitor Sensitivity. Cancer Cell 2018, 33, 44–59.e8. [Google Scholar] [CrossRef] [Green Version]
- Jin, X.; Qin, T.; Zhao, M.; Bailey, N.; Liu, L.; Yang, K.; Ng, V.; Higashimoto, T.; Coolon, R.; Ney, G.; et al. Oncogenic N-Ras and Tet2 Haploinsufficiency Collaborate to Dysregulate Hematopoietic Stem and Progenitor Cells. Blood Adv. 2018, 2, 1259–1271. [Google Scholar] [CrossRef]
- Watzinger, F.; Gaiger, A.; Karlic, H.; Becher, R.; Pillwein, K.; Lion, T. Absence of N-Ras Mutations in Myeloid and Lymphoid Blast Crisis of Chronic Myeloid Leukemia. Cancer Res. 1994, 54, 3934–3938. [Google Scholar]
- Tenedini, E.; Bernardis, I.; Artusi, V.; Artuso, L.; Roncaglia, E.; Guglielmelli, P.; Pieri, L.; Bogani, C.; Biamonte, F.; Rottuno, G.; et al. Targeted Cancer Exome Sequencing Reveals Recurrent Mutations in Myeloproliferative Neoplasms. Leukemia 2014, 28, 1052–1059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuo, M.-C.; Liang, D.-C.; Huang, C.-F.; Shih, Y.-S.; Wu, J.-H.; Lin, T.-L.; Shih, L.-Y. RUNX1 Mutations Are Frequent in Chronic Myelomonocytic Leukemia and Mutations at the C-Terminal Region Might Predict Acute Myeloid Leukemia Transformation. Leukemia 2009, 23, 1426–1431. [Google Scholar] [CrossRef] [PubMed]
- Gelsi-Boyer, V.; Trouplin, V.; Roquain, J.; Adélaïde, J.; Carbuccia, N.; Esterni, B.; Finetti, P.; Murati, A.; Arnoulet, C.; Zerazhi, H.; et al. ASXL1 Mutation Is Associated with Poor Prognosis and Acute Transformation in Chronic Myelomonocytic Leukaemia: Gene Mutations in CMML. Br. J. Haematol. 2010, 151, 365–375. [Google Scholar] [CrossRef] [Green Version]
- Khozin, S.; Blumenthal, G.M.; Pazdur, R. Real-World Data for Clinical Evidence Generation in Oncology. JNCI J. Natl. Cancer Inst. 2017, 109. [Google Scholar] [CrossRef] [Green Version]
- Patnaik, M.M.; Pierola, A.A.; Vallapureddy, R.; Yalniz, F.F.; Kadia, T.M.; Jabbour, E.J.; Lasho, T.; Hanson, C.A.; Ketterling, R.P.; Kantarjian, H.M.; et al. Blast Phase Chronic Myelomonocytic Leukemia: Mayo-MDACC Collaborative Study of 171 Cases. Leukemia 2018, 32, 2512–2518. [Google Scholar] [CrossRef]
- Borthakur, G.; Popplewell, L.; Boyiadzis, M.; Foran, J.; Platzbecker, U.; Vey, N.; Walter, R.B.; Olin, R.; Raza, A.; Giagounidis, A.; et al. Activity of the Oral Mitogen-Activated Protein Kinase Kinase Inhibitor Trametinib in RAS-Mutant Relapsed or Refractory Myeloid Malignancies: Trametinib in RAS-Mutant Malignancies. Cancer 2016, 122, 1871–1879. [Google Scholar] [CrossRef] [Green Version]
- Such, E.; Germing, U.; Malcovati, L.; Cervera, J.; Kuendgen, A.; Della Porta, M.G.; Nomdedeu, B.; Arenillas, L.; Luño, E.; Xicoy, B.; et al. Development and Validation of a Prognostic Scoring System for Patients with Chronic Myelomonocytic Leukemia. Blood 2013, 121, 3005–3015. [Google Scholar] [CrossRef]
- Malcovati, L.; Gallì, A.; Travaglino, E.; Ambaglio, I.; Rizzo, E.; Molteni, E.; Elena, C.; Ferretti, V.V.; Catricalà, S.; Bono, E.; et al. Clinical Significance of Somatic Mutation in Unexplained Blood Cytopenia. Blood 2017, 129, 3371–3378. [Google Scholar] [CrossRef]
- Öhler, L.; Geissler, K.; Hinterberger, W. Diagnostic and Prognostic Value of Colony Formation of Hematopoietic Progenitor Cells in Myeloid Malignancies. Wien. Klin. Wochenschr. 2003, 115, 537–546. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Genotype | WBC G/L Pretransform. (%PB blasts) | WBC G/L Posttransform. (%PB blasts) | CFU–GM/105 MNC Pretransform. | CFU-GM/105 MNC Posttransform. |
|---|---|---|---|---|---|
| UPN1-026 | CBL | 12.3 (2%) | 178 (60%) | 35 | 302 |
| PN1-033 | NRAS | 7.8 (4%) | 160 (10%) | 200 | 533 |
| UPN1-038 | NA | 93.8 (1%) | 50.7 (30%) | 622 | 4553 |
| UPN1-071 | PTPN11 | 74.0 (8%) | 161 (18%) | 11 | 48 |
| UPN1-128 | NRAS | 57.5 (3%) | 155 (13%) | 59 | 272 |
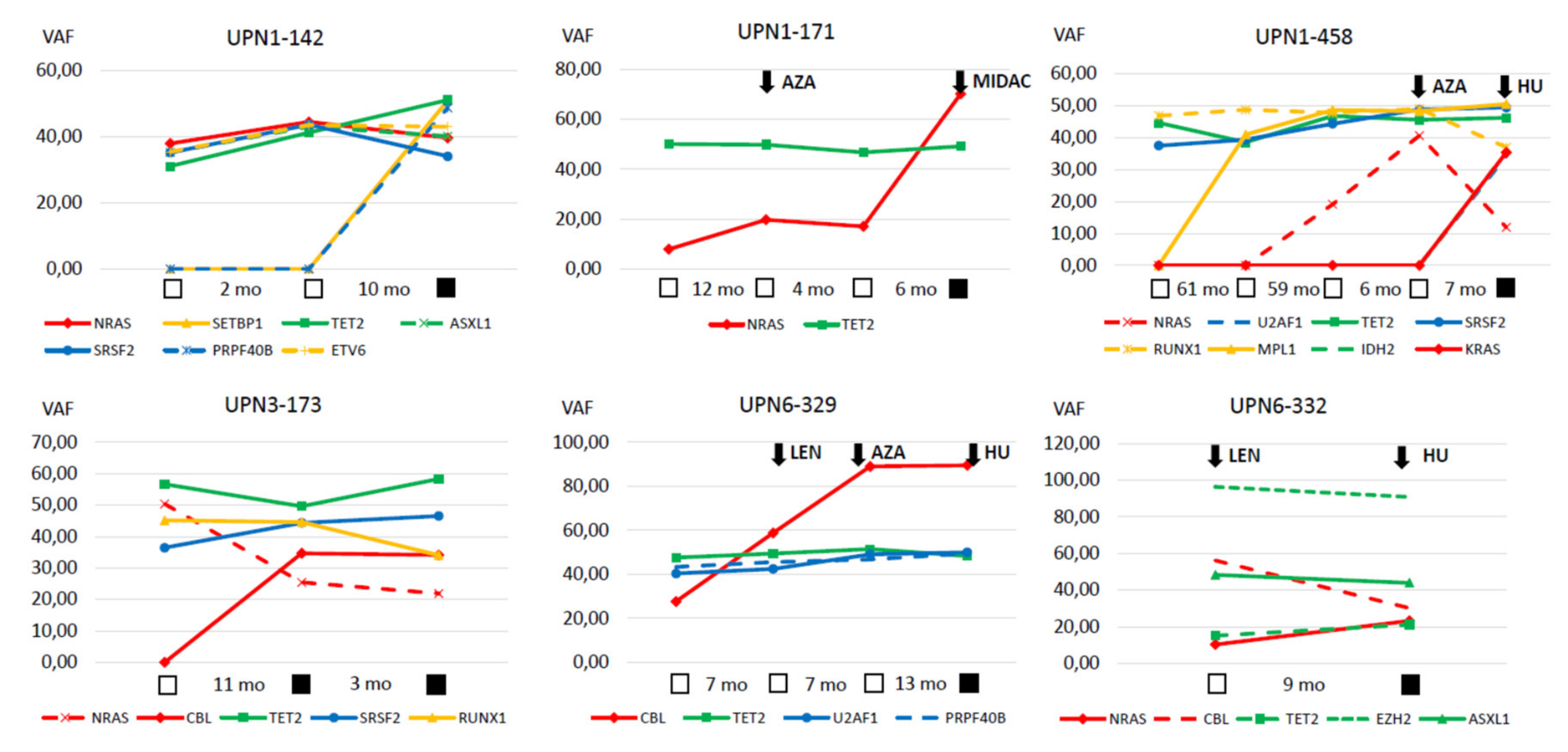
| UPN1-142 | NRAS | 20.3 (0%) | 80.7 (1%) | 48 | 202 |
| UPN1-171 | NRAS | 55.5 (0%) | 50.0 (54%) | 1 | 254 |
| UPN1-468 | NRAS | 8.5 (0%) | 24.5 (57%) | 8 | 381 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Geissler, K.; Jäger, E.; Barna, A.; Gurbisz, M.; Graf, T.; Graf, E.; Nösslinger, T.; Pfeilstöcker, M.; Tüchler, H.; Sliwa, T.; et al. Correlation of RAS-Pathway Mutations and Spontaneous Myeloid Colony Growth with Progression and Transformation in Chronic Myelomonocytic Leukemia—A Retrospective Analysis in 337 Patients. Int. J. Mol. Sci. 2020, 21, 3025. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21083025
Geissler K, Jäger E, Barna A, Gurbisz M, Graf T, Graf E, Nösslinger T, Pfeilstöcker M, Tüchler H, Sliwa T, et al. Correlation of RAS-Pathway Mutations and Spontaneous Myeloid Colony Growth with Progression and Transformation in Chronic Myelomonocytic Leukemia—A Retrospective Analysis in 337 Patients. International Journal of Molecular Sciences. 2020; 21(8):3025. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21083025
Chicago/Turabian StyleGeissler, Klaus, Eva Jäger, Agnes Barna, Michael Gurbisz, Temeida Graf, Elmir Graf, Thomas Nösslinger, Michael Pfeilstöcker, Heinz Tüchler, Thamer Sliwa, and et al. 2020. "Correlation of RAS-Pathway Mutations and Spontaneous Myeloid Colony Growth with Progression and Transformation in Chronic Myelomonocytic Leukemia—A Retrospective Analysis in 337 Patients" International Journal of Molecular Sciences 21, no. 8: 3025. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21083025