Current Synthesis and Systematic Review of Main Effects of Calf Blood Deproteinized Medicine (Actovegin®) in Ischemic Stroke

Abstract
:1. Background
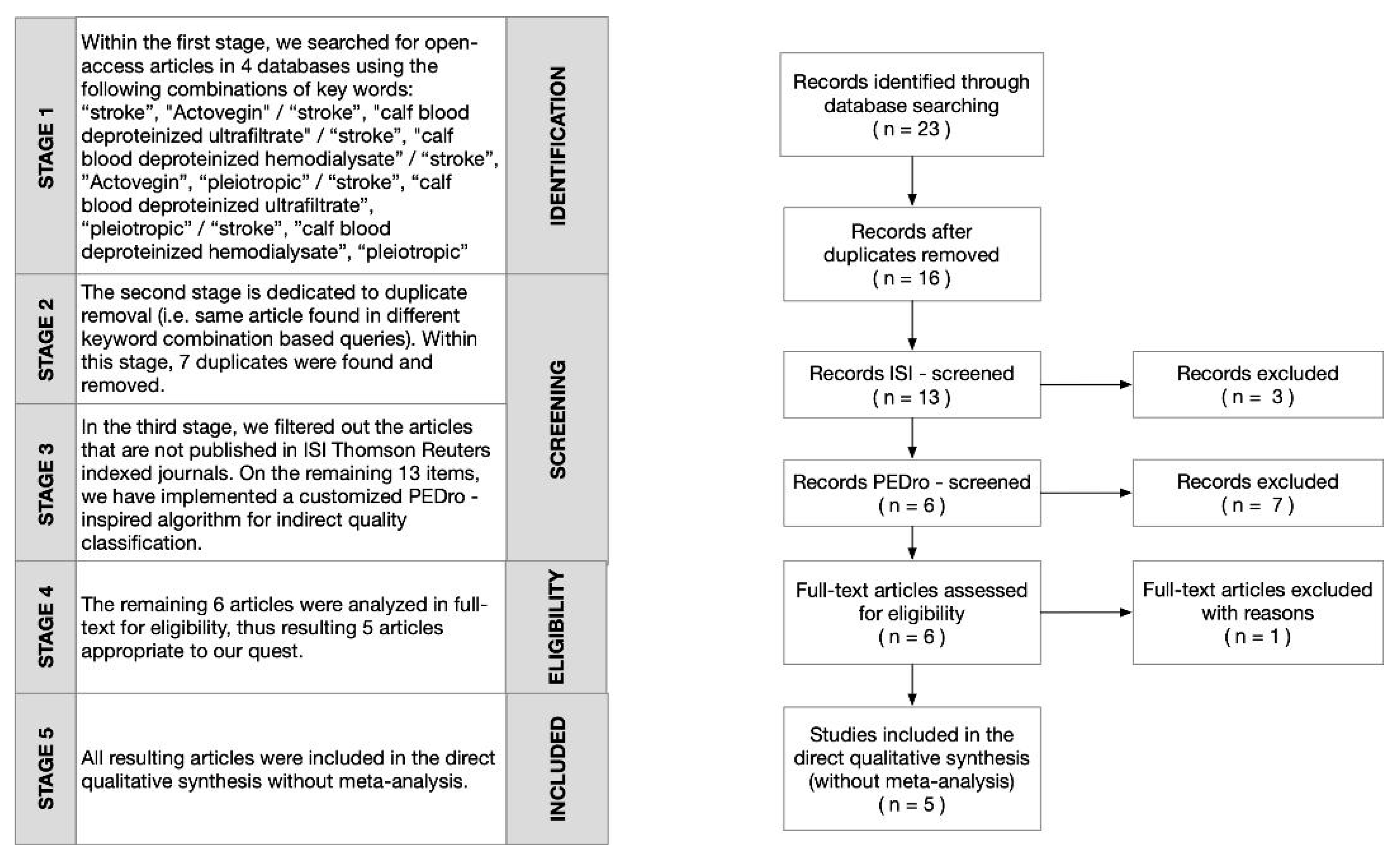
2. Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Article | Publ. Year | No. of Citations | No. of Citations/Year | PEDro Score |
|---|---|---|---|---|
| Mijajlović et al., Post-stroke dementia—A comprehensive review, BMC Med. 2017; 15: 11. Published online 2017 Jan 18. doi:10.1186/s12916-017-0779-7 | 2017 | 78 | 26 | 10 |
| Elmlinger et al., Neuroprotective and Anti-Oxidative Effects of the Hemodialysate Actovegin® on Primary Rat Neurons in Vitro, Neuromolecular Med. 2011 Dec; 13(4): 266–274. Published online 2011 Oct 9. doi:10.1007/s12017-011-8157-7 | 2011 | 124 | 13.78 | 8 |
| Guekht et. al, ARTEMIDA Trial (A Randomized Trial of Efficacy, 12 Months International Double-Blind Actovegin®): A Randomized Controlled Trial to Assess the Efficacy of Actovegin in Poststroke Cognitive Impairment, Stroke. 2017 May; 48(5): 1262-1270. Published online 2017 Apr 24.doi:10.1161/STROKEAHA.116.014321 | 2017 | 33 | 11 | 6 |
| Bordet et al., Towards the Concept of disease-modifier in post-stroke or vascular cognitive impairment: a consensus report, BMC Med. 2017; 15: 107. Published online 2017 May 24. doi:10.1186/s12916-017-0869-6 | 2017 | 23 | 7.66 | 4 |
| Liu et al., Curcumin Protects against Ischemic Stroke by Titrating Microglia/Macrophage Polarization, Front Aging Neurosci. 2017; 9: 233. Published online 2017 Jul 21. doi:10.3389/fnagi.2017.00233 | 2017 | 22 | 7.33 | 4 |
| Borstein et al., Diabetes and the brain: issues and unmet needs, Neurol Sci. 2014; 35(7): 995–1001. Published online 2014 Apr 29. doi:10.1007/s10072-014-1797-2 | 2014 | 43 | 7.17 | 4 |
| Meilin et al., Treatment with Actovegin improves spatial learning and memory in rats following transient forebrain ischaemia, J Cell Mol Med. 2014 Aug; 18(8): 1623–1630. Published online 2014 May 6. doi:10.1111/jcmm.12297 | 2014 | 31 | 5.17 | 3 |
| Voskoboeva et al., Homocystinuria due to cystathionine beta-synthase (CBS) deficiency in Russia: Molecular and clinical characterization, Mol Genet Metab Rep. 2018 Mar; 14: 47–54. Published online 2017 Dec 27. doi:10.1016/j.ymgmr.2017.11.001 | 2018 | 7 | 3.5 | 2 |
| Dong et al., Cerebrolysin improves sciatic nerve dysfunction in a mouse model of diabetic peripheral neuropathy, Neural Regen Res. 2016 Jan; 11(1): 156–162. doi:10.4103/1673-5374.175063 | 2016 | 12 | 3 | 2 |
| Krasnov et al., Early Aging in Chernobyl Clean-Up Workers: Long-Term Study, Biomed Res Int. 2015; 2015: 948473. Published online 2015 Jan 27. doi:10.1155/2015/948473 | 2015 | 10 | 2 | 1 |
| Mattyasovszky et al., Exposure to radial extracorporeal shock waves modulates viability and gene expression of human skeletal muscle cells: a controlled in vitro study, J Orthop Surg Res. 2018; 13: 75. Published online 2018 Apr 6. doi:10.1186/s13018-018-0779-0 | 2018 | 4 | 2 | 1 |
| Zhang et al., Isosteviol Sodium Protects against Ischemic Stroke by Modulating Microglia/Macrophage Polarization via Disruption of GAS5/miR-146a-5p sponge, Sci Rep. 2019; 9: 12221. Published online 2019 Aug 21. doi:10.1038/s41598-019-48759-0 | 2019 | 0 | 0 | 0 |
| Zhang et al., Progression in Vascular Cognitive Impairment: Pathogenesis, Neuroimaging Evaluation, and Treatment, Cell Transplant. 2019 Jan; 28(1): 18–25. Published online 2018 Nov 29. doi:10.1177/0963689718815820 | 2019 | 0 | 0 | 0 |
| Article |
|---|
| Guekht et al., A Randomised, Double-Blind, Placebo-Controlled Trial of Actovegin® in Patients with Post-Stroke Cognitive Impairment: ARTEMIDA Study Design, Dement Geriatr Cogn Dis Extra. 2013 Jan-Dec; 3(1): 459-467. Published online 2013 Dec 14. doi:10.1159/000357122 |
| Khandelwal et al., Cardiovascular autonomic functions & cerebral autoregulation in patients with orthostatic hypotension, Indian J Med Res. 2011 Oct; 134(4): 463–469 |
| Onose et al., Integrative emphases on intimate, intrinsic propensity/ pathological processes-causes of self-recovery limits and also, subtle related targets for neuroprotection/ pleiotropicity/ multimodal actions, by accessible therapeutic approaches-in spinal cord inj, J Med Life. 2010 Aug 15; 3(3): 262–274. Published online 2010 Aug 25 |
References
- Sacco, R.L.; Kasner, S.E.; Broderick, J.P.; Caplan, L.R.; Connors, J.; Culebras, A.; Elkind, M.S.; George, M.G.; Hamdan, A.D.; Higashida, R.T.; et al. An Updated Definition of Stroke for the 21st Century. Stroke 2013, 44, 2064–2089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boden-Albala, B.; Appleton, N.; Schram, B. Stroke Epidemiology and Prevention (Chapter 1). In Stroke Rehabilitation; Wilson, R., Raghavan, P., Eds.; Elsevier: St. Louis, MO, USA, 2019. [Google Scholar]
- Macdonald, B.K.; Cockerell, O.C.; Sander, J.W.; Shorvon, S.D. The incidence and lifetime prevalence of neurological disorders in a prospective community-based study in the UK. Brain 2000, 123, 665–676. [Google Scholar] [CrossRef] [Green Version]
- Feigin, V.L.; Forouzanfar, M.H.; Krishnamurthi, R.; Mensah, G.A.; Connor, M.; Bennett, D.A.; Moran, A.E.; Sacco, R.L.; Anderson, L.; Truelsen, T.; et al. Global and regional burden of stroke during 1990–2010: Findings from the Global Burden of Disease Study 2010. Lancet 2014, 383, 245–254. [Google Scholar] [CrossRef]
- Ropper, A.H.; Samuels, M.A.; Klein, J.P. Cerebrovascular Diseases (Chapter 34). In Adams and Victor’s: Principles of Neurology, 10th ed.; Mc Graw Hill Education: Boston, MA, USA, 2014; p. 781. [Google Scholar]
- Pulit, S.L.; Weng, L.-C.; McArdle, P.F.; Trinquart, L.; Choi, S.H.; Mitchell, B.; Rosand, J.; Bakker, P.I.W.D.; Benjamin, E.J.; Ellinor, P.T.; et al. Atrial Fibrillation Genetic Risk Differentiates Cardioembolic Stroke from other Stroke Subtypes. Neurol. Genet. 2018, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feigin, V.; Abajobir, A.A.; Abate, K.H.; Abd-Allah, F.; Abdulle, A.M.; Abera, S.F.; Abyu, G.Y.; Ahmed, M.; Aichour, A.N.; Aichour, I.; et al. Global, regional, and national burden of neurological disorders during 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Neurol. 2017, 16, 877–897. [Google Scholar] [CrossRef] [Green Version]
- Stack, C.A.; Cole, J. Ischemic stroke in young adults. Curr. Opin. Cardiol. 2018, 33, 594–604. [Google Scholar] [CrossRef]
- Frontera, W.R.; Silver, J.; Rizzo, T. Stroke in Young Adults. In Essentials of Physical Medicine and Rehabilitation: Musculoskeletal Disorders, Pain and Rehabilitation, 4th ed.; Elsevier: St. Louis, MO, USA, 2018; p. 937. [Google Scholar]
- Kanyal, N. The Science of Ischemic Stroke: Pathophysiology & Pharmacological Treatment. Int. J. Pharm. Sci. Rev. Res. 2015, 4, 65–84. [Google Scholar]
- Stevens, E.; Emmett, E.; Wang, Y.; McKevitt, W.C.; Wolfe, C. The Burden of Stroke in Europe. The Challenge for Policy Makers—King’s College London for the Stroke Alliance for Europe (SAFE), 2017. Available online: https://www.stroke.org.uk/sites/default/files/the_burden_of_stroke_in_europe_-_challenges_for_policy_makers.pdf (accessed on 29 April 2020).
- Manuelidis, L. Different central nervous system cell types display distinct and nonrandom arrangements of satellite DNA sequences. Proc. Natl. Acad. Sci. USA 1984, 81, 3123–3127. [Google Scholar] [CrossRef] [Green Version]
- Hall, J.E.; Guyton, A.C. Genetic Control of Protein Synthesis, Cell Function, and Cell Reproduction. In Guyton and Hall Textbook of Medical Physiology, 12th ed.; Saunders Elsevier: Philadelphia, PA, USA, 2011; p. 39. [Google Scholar]
- Onose, G.; Haras, M.; Anghelescu, A.; Muresanu, D.; Giuglea, C.; Daia Chendreanu, C. Integrative emphaizses an intimate intrinsic propensity/ pathological processes-causes of self recovery limits and also, subtle related targets for neuroprotection/ pleiotropicity/multimodal actions by accesible therapeutic approaches in spinal cord injuries. J. Med. Life 2010, 3, 262–274. [Google Scholar]
- Onose, G.; Daia, C.; Haras, B.; Spircu, T.; Anghelescu, A.; Ciurea; Mihaescu, A.S.; Onose, L. A long-term, complex, unitary appraisal regarding neurorestorative, including neurorehabilitative, outcomes in patients treated with Cerebrolysin®, following traumatic brain injury. J. Neurorestoratology 2014, 2, 85. [Google Scholar] [CrossRef] [Green Version]
- Ren, Y.; Zhou, X.; He, X. Function of microglia and macrophages in secondary damage after spinal cord injury. Neural Regen. Res. 2014, 9, 1787–1795. [Google Scholar] [CrossRef] [PubMed]
- Loane, D.J.; Faden, A.I. Neuroprotection for traumatic brain injury: Translational challenges and emerging therapeutic strategies. Trends Pharmacol. Sci. 2010, 31, 596–604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Onose, G.; Anghelescu, A.; Muresanu, D.F.; Padure, L.; Haras, M.A.; Chendreanu, C.O.; Onose, L.V.; Mirea, A.; Ciurea, A.V.; El Masri, W.S.; et al. A review of published reports on neuroprotection in spinal cord injury. Spinal Cord 2009, 47, 716–726. [Google Scholar] [CrossRef] [PubMed]
- Muresanu, D.F.; Radulescu, A.; Marginean, M.; Toldisan, I. Neuroprotection and Neuroplasticity in Traumatic Brain Injury. SNPCAR 2007, 10, 3–8. [Google Scholar]
- Frontera, W.R.; DeLisa, J.A.; Gans, B.M.; Robinson, L.R.; Bockeneck, W.; Chase, J. Stroke Rehabilitation (Chapter 18). In DeLisa’s Physical Medicine & Rehabilitation. Principles and Practice, 6th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2019; pp. 356–357. [Google Scholar]
- Cifu, D.X. Stroke Syndromes (Chapter 44). In Braddom’s Physical Medicine and Rehabilitation, 5th ed.; Elsevier: Philadelphia, PA, USA, 2016; p. 1001. [Google Scholar]
- Jin, J.Q.; Li, W.; Mu, Y.L.; Jiang, Y.; Zhang, Y.X.; Lu, Z.Y. [Study on the oral mucosal diseases in patients with cerebrovascular diseases]. Chin. J. Epidemiol. 2019, 40, 1003–1005. [Google Scholar] [CrossRef]
- Braddom, R.L. Physical Medicine & Rehabilitation, 3rd ed.; Elsevier: Philadephia, PA, USA, 2007; pp. 1176–1177. [Google Scholar]
- Schreiber, S.; Wilisch Neumann, A.; Assmann, A.; Scheumann, V.; Perosa, V.; Jandke, S.; Mawrin, C.; Carare, R.O.; Werring, D.J.; Schreiber, F. Invited Review: The spectrum of age related small vessel diseases: Potential overlap and interactions of amyloid and nonamyloid vasculopathies. Neuropathol. Appl. Neurobiol. 2019. [Google Scholar] [CrossRef]
- Rognoni, A.; Cavallino, C.; Veia, A.; Bacchini, S.; Rosso, R.; Facchini, M.; Secco, G.G.; Lupi, A.; Nardi, F.; Rametta, F.; et al. Pathophysiology of Atherosclerotic Plaque Development. Cardiovasc. Hematol. Agents Med. Chem. 2015, 13, 10–13. [Google Scholar] [CrossRef]
- Bernhardt, J.; Hayward, K.S.; Kwakkel, G.; Ward, N.S.; Wolf, S.L.; Borschmann, K.; Krakauer, J.W.; Boyd, L.A.; Carmichael, S.T.; Corbett, D.; et al. Agreed definitions and a shared vision for new standards in stroke recovery research: The Stroke Recovery and Rehabilitation Roundtable task-force. Int. J. Stroke 2017, 12, 444–450. [Google Scholar] [CrossRef]
- Xing, C.; Arai, K.; Lo, E.H.; Hommel, M. Pathophysiologic cascades in ischemic stroke. Int. J. Stroke 2012, 7, 378–385. [Google Scholar] [CrossRef]
- Prentice, H.; Modi, J.P.; Wu, J.-Y. Mechanisms of Neuronal Protection against Excitotoxicity, Endoplasmic Reticulum Stress, and Mitochondrial Dysfunction in Stroke and Neurodegenerative Diseases. Oxidative Med. Cell. Longev. 2015, 2015, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Ramón, R.; García, J.C. Excitotoxicity and Oxidative Stress in Acute Stroke. In Ischemic Stroke—Updates; IntechOpen Limited: London, UK, 2016. [Google Scholar]
- Liu, L.; Locascio, L.M.; Doré, S. Critical Role of Nrf2 in Experimental Ischemic Stroke. Front. Pharmacol. 2019, 10, 153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Namba, K.; Takeda, Y.; Sunami, K.; Hirakawa, M. Temporal Profiles of the Levels of Endogenous Antioxidants After Four-Vessel Occlusion in Rats. J. Neurosurg. Anesthesiol. 2001, 13, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Song, J.; Park, J.; Oh, Y.; Lee, W.T. Glutathione Suppresses Cerebral Infarct Volume and Cell Death after Ischemic Injury: Involvement of FOXO3 Inactivation and Bcl2 Expression. Oxidative Med. Cell. Longev. 2015, 2015, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Sun, M.-S.; Jin, H.; Sun, X.; Huang, S.; Zhang, F.-L.; Guo, Z.-N.; Yang, Y. Free Radical Damage in Ischemia-Reperfusion Injury: An Obstacle in Acute Ischemic Stroke after Revascularization Therapy. Oxidative Med. Cell. Longev. 2018, 2018, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Haddad, J.J.; Harb, H.L. L-gamma-Glutamyl-L-cysteinyl-glycine (glutathione; GSH) and GSH-related enzymes in the regulation of pro- and anti-inflammatory cytokines: A signaling transcriptional scenario for redox(y) immunologic sensor(s). Mol. Immunol. 2005, 42, 987–1014. [Google Scholar] [CrossRef]
- Bae, C.Y.-J.; Sun, H.-S. TRPM7 in cerebral ischemia and potential target for drug development in stroke. Acta Pharmacol. Sin. 2011, 32, 725–733. [Google Scholar] [CrossRef]
- Khoshnam, S.E.; Winlow, W.; Farzaneh, M.; Farbood, Y.; Moghaddam, H.F. Pathogenic mechanisms following ischemic stroke. Neurol. Sci. 2017, 38, 1167–1186. [Google Scholar] [CrossRef]
- Anrather, J.; Iadecola, C. Inflammation and Stroke: An Overview. Neurother. 2016, 13, 661–670. [Google Scholar] [CrossRef]
- Onwuekwe, I.; Ezeala-Adikaibe, B. Ischemic Stroke and Neuroprotection. Ann. Med Heal. Sci. Res. 2012, 2, 186–190. [Google Scholar] [CrossRef] [Green Version]
- Rodrigo, R.; Fernández-Gajardo, R.; Gutiérrez, R.; Matamala, J.M.; Carrasco, R.; Miranda-Merchak, A.; Feuerhake, W. Oxidative stress and pathophysiology of ischemic stroke: Novel therapeutic opportunities. CNS Neurol. Disord. DR 2013, 12, 698–714. [Google Scholar] [CrossRef]
- Andrews, A.M.; Gerhardt, G.A.; Daws, L.C.; Shoaib, M.; Mason, B.J.; Heyser, C.J.; De Lecea, L.; Balster, R.L.; Walsh, S.; Dahmen, M.M.; et al. Neurovascular Unit. In Encyclopedia of Psychopharmacology; Springer-Verlag GmbH: Heidelberg, Germany, 2010; p. 877. [Google Scholar]
- Arai, K.; Lok, J.; Guo, S.; Hayakawa, K.; Xing, C.; Lo, E.H. Cellular mechanisms of neurovascular damage and repair after stroke. J. Child Neurol. 2011, 26, 1193–1198. [Google Scholar] [CrossRef] [PubMed]
- Ropper, A.; Samuels, M. Intracranial Neoplasms and Parneoplastic Disorders (Chapter 31)—Brain Edema. In Adams and Victor’s Principles of Neurology, 9th ed.; McGraw-Hill Professional: New York City, NY, USA, 2009; pp. 618–619. [Google Scholar]
- Kim, J.Y.; Park, J.; Chang, J.Y.; Kim, S.-H.; Lee, W.T. Inflammation after Ischemic Stroke: The Role of Leukocytes and Glial Cells. Exp. Neurobiol. 2016, 25, 241–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qin, A.-P.; Zhang, H.-L.; Qin, Z.-H. Mechanisms of lysosomal proteases participating in cerebral ischemia-induced neuronal death. Neurosci. Bull. 2008, 24, 117–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Unal-Cevik, I.; Kiliņ, M.; Can, A.; Gürsoy-Ozdemir, Y.; Dalkara, T. Apoptotic and Necrotic Death Mechanisms Are Concomitantly Activated in the Same Cell After Cerebral Ischemia. Stroke 2004, 35, 2189–2194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mureşanu, D.F. Neuromodulation with Pleiotropic and Multimodal Drugs—Future Approaches to Treatment of Neurological Disorders. In Brain Edema XIV. Acta Neurochirurgica Supplementum; Springer: Vienna, Austria, 2010; Volume 106, pp. 291–294. [Google Scholar]
- Bröker, L.E.; Kruyt, F.A.E.; Giaccone, G. Cell Death Independent of Caspases: A Review. Clin. Cancer Res. 2005, 11, 3155–3162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, D.R.; Kroemer, G. The Pathophysiology of Mitochondrial Cell Death. Science 2004, 305, 626–629. [Google Scholar] [CrossRef] [PubMed]
- Lang, J.T.; McCullough, L.D. Pathways to ischemic neuronal cell death: Are sex differences relevant? J. Transl. Med. 2008, 6, 33. [Google Scholar] [CrossRef] [Green Version]
- Medical & Biological Laboratories (MBL). Life Science. Available online: https://www.mblbio.com/bio/g/dtl/A/?pcd=SY-001#u-pub (accessed on 28 April 2020).
- Nagata, S. Early work on the function of CD95, an interview with Shige Nagata. Cell Death Differ. 2004, 11, S23–S27. [Google Scholar] [CrossRef] [Green Version]
- Chaudhary, P.M.; Eby, M.; Jasmin, A.; Bookwalter, A.; Murray, J.; Hood, L. Death receptor 5, a new member of the TNFR family, and DR4 induce FADD-dependent apoptosis and activate the NF-kappaB pathway. Immunity 1997, 7, 821–830. [Google Scholar] [CrossRef] [Green Version]
- King, M.W. The Extracellular Matrix. The Medical Biochemistry Page. Available online: https://themedicalbiochemistrypage.org/extracellularmatrix.php (accessed on 28 April 2020).
- Muresanu, D.; Buzoianu, A.; Florian, A.I.; Von Wild, T. Towards a roadmap in brain protection and recovery. J. Cell. Mol. Med. 2012, 16, 2861–2871. [Google Scholar] [CrossRef]
- NCBI/PubMed, NCBI/PMC. Available online: https://www.ncbi.nlm.nih.gov (accessed on 28 April 2020).
- Elsevier. Available online: https://www.elsevier.com (accessed on 28 April 2020).
- PEDRO Score. Available online: https://www.strokengine.ca/glossary/pedro–score (accessed on 28 April 2020).
- Institute for Scientific Information (ISI) Web of Knowledge/Science. Available online: https://apps.webofknowledge.com (accessed on 28 April 2020).
- PRISMA 2009 Flow Diagram. Available online: http://prisma-statement.org/documents/PRISMA%202009%20flow%20diagram.pdf (accessed on 28 April 2020).
- Onose, G.; Popescu, N.; Munteanu, C.; Ciobanu, V.; Sporea, C.; Mirea, M.-D.; Daia, C.; Andone, I.; Spînu, A.; Mirea, A. Mobile Mechatronic/Robotic Orthotic Devices to Assist–Rehabilitate Neuromotor Impairments in the Upper Limb: A Systematic and Synthetic Review. Front. Mol. Neurosci. 2018, 12, 577. [Google Scholar] [CrossRef] [PubMed]
- Mijajlovic, M.D.; Pavlović, A.; Brainin, M.; Heiss, W.-D.; Quinn, T.J.; Ihle-Hansen, H.B.; Hermann, D.M.; Ben Assayag, E.; Richard, E.; Thiel, A.; et al. Post-stroke dementia—A comprehensive review. BMC Med. 2017, 15, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elmlinger, M.W.; Kriebel, M.; Ziegler, D. Neuroprotective and Anti-Oxidative Effects of the Hemodialysate Actovegin on Primary Rat Neurons in Vitro. Neuromol. Med. 2011, 13, 266–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guekht, A.; Skoog, I.; Edmundson, S.; Zakharov, V.; Korczyn, A.D. ARTEMIDA Trial (A Randomized Trial of Efficacy, 12 Months International Double-Blind Actovegin). Stroke 2017, 48, 1262–1270. [Google Scholar] [CrossRef]
- Bordet, R.; Ihl, R.; Korczyn, A.D.; Lanza, G.; Jansa, J.; Hoerr, R.; Guekht, A. Towards the concept of disease – modifier in post-stroke or vascular cognitive impairment: A consensus report. BMC Med. 2017, 15, 107. [Google Scholar] [CrossRef]
- Bornstein, N.M.; Brainin, M.; Guekht, A.; Skoog, I.; Korczyn, A.D. Diabetes and the brain: Issues and unmet needs. Neurol. Sci. 2014, 35, 995–1001. [Google Scholar] [CrossRef] [Green Version]
- Machicao, F.; Muresanu, D.F.; Hundsberger, H.; Pfluger, M.; Guekht, A. Pleiotropic neuroprotective and metabolic effects of Actovegi’ s mode of action. J. Neurol. Sci. 2012, 322, 222–227. [Google Scholar] [CrossRef]
- Skoog, I.; Korczyn, A.D.; Guekht, A. Neuroprotection in vascular dementia: A future path. J. Neurol. Sci. 2012, 322, 232–236. [Google Scholar] [CrossRef]
- Dieckmann, A.; Kriebel, M.; Andriambeloson, E.; Ziegler, D.; Elmlinger, M. Treatment with Actovegin® Improves Sensory Nerve Function and Pathology in Streptozotocin-Diabetic Rats via Mechanisms Involving Inhibition of PARP Activation. Exp. Clin. Endocrinol. Diabetes 2011, 120, 132–138. [Google Scholar] [CrossRef] [Green Version]
- Onose, G.; Teoias-Serban, D.; Popescu, C.; Andone, I.; Bruma, E.; Mihaescu, A.; Haras, M.; Bumbea, A.M.; Anghelescu, A.; Spircu, T.; et al. New approaches regarding the use of Actovegin in subacute/ postacute/subchronic Traumatic Brain Injury patients. Farmacia 2017, 65, 772–777. [Google Scholar]
- Onose, G.; Chendreanu, D.C.; Haras, M.; Ciurea, A.V.; Anghelescu, A. Traumatic brain injury: Current endeavours and trends for neuroprotections and related recovery. Rom. Neurosurg. 2011, XVII, 11–30. [Google Scholar]
- Buchmayer, F.; Pleiner, J.; Elmlinger, M.W.; Lauer, G.; Nell, G.; Sitte, H.H. Actovegin®: A biological drug for more than 5 decades. Wien. Med. Wochenschr. 2011, 161, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, D.; Movsesyan, L.; Mankovsky, B.; Gurieva, I.; Abylaiuly, Z.; Strokov, I. Treatment of symptomatic Polyneurophaty with Actovegin in type 2 Diabetic patients. Diabetes Care 2009, 32, 1479–1484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meilin, S.; Machicao, F.; Elmlinger, M. Treatment with Actovegin improves spatial learning and memory in rats following tansient forebrain ischaemia. J. Cell Mol. Med. 2014, 18, 1623–1630. [Google Scholar] [CrossRef] [Green Version]
- Ropper, A.; Samuels, M.; Klein, J. Cerebrovascular Diseases (Chapter 34). In Adams and Victor’s: Principles of Neurology, 10th ed.; Mc Graw Hill Education: Boston, MA, USA, 2014; p. 875. [Google Scholar]
- Actovegin®—Medicine Leaflet. Available online: https://www.anm.ro/_/_RCP/RCP_7336_30.01.15.pdf (accessed on 28 April 2020).
- Shi, H.; Hu, X.; Leak, R.K.; Shi, Y.; An, C.; Suenaga, J.; Chen, J.; Gao, Y. Demyelination as a rational therapeutic target for ischemic or traumatic brain injury. Exp. Neurol. 2015, 272, 17–25. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Xuan, W.; Zhu, Z.-Y.; Li, Y.; Zhu, H.; Zhu, L.; Fu, D.-Y.; Yang, L.-Q.; Li, P.; Yu, W. The evolving role of neuro-immune interaction in brain repair after cerebral ischemic stroke. CNS Neurosci. Ther. 2018, 24, 1100–1114. [Google Scholar] [CrossRef] [Green Version]
- Dobkin, B.H.; Carmichael, S.T. The Specific Requirements of Neural Repair Trials for Stroke. Neurorehabilit. Neural Repair 2015, 30, 470–478. [Google Scholar] [CrossRef] [Green Version]
- Watts, L.; Long, J.A.; Manga, V.H.; Huang, S.; Shen, Q.; Duong, T.Q. Normobaric oxygen worsens outcome after a moderate traumatic brain injury. Br. J. Pharmacol. 2015, 35, 1137–1144. [Google Scholar] [CrossRef]
- Fan, B.; Wei, Z.; Yao, X.; Shi, G.; Cheng, X.; Zhou, X.; Zhou, H.; Ning, G.; Kong, X.; Feng, S. Microenvironment Imbalance of Spinal Cord Injury. Cell Transplant. 2018, 27, 853–866. [Google Scholar] [CrossRef] [Green Version]
- Huang, H.; Young, W.; Ziad, A.; Hooshang, S.; Alok, S.; Dafin, M.; Shiqing, F.; Lin, C. Beijing Declaration of International Association of Neurorestoratology. J. Neurorestoratology 2015, 3, 121–122. [Google Scholar] [CrossRef] [Green Version]
| Keywords/Database | Elsevier | PubMed | PMC | PEDro |
|---|---|---|---|---|
| “stroke”, “Actovegin” | 0 | 0 | 16 | 0 |
| “stroke”, “calf blood deproteinized ultrafiltrate” | 0 | 0 | 0 | 0 |
| “stroke”, “calf blood deproteinized”, “hemodialysate” | 0 | 0 | 0 | 0 |
| “stroke”, “Actovegin”, “pleiotropic” | 0 | 0 | 7 | 0 |
| “stroke”, “calf blood deproteinized ultrafiltrate”, “pleiotropic” | 0 | 0 | 0 | 0 |
| “stroke”, “calf blood deproteinized”, “hemodialysate”, “pleiotropic” | 0 | 0 | 0 | 0 |
| Total | 0 | 0 | 23 | 0 |
| No. | Title | Authors | ISI | Year | Citations | Citations/Year | PEDro |
|---|---|---|---|---|---|---|---|
| 1 | Post-Stroke Dementia—A Comprehensive Review | Mijajlović et al. [61] (in the body text—see further) | Yes | 2017 | 78 | 26 | 10 |
| 2 | Neuroprotective and Anti-Oxidative Effects of the Hemodialysate Actovegin® on Primary Rat Neurons in Vitro | Elmlinger et al. [62] (in the body text—see further) | Yes | 2011 | 124 | ~14 | 8 |
| 3 | ARTEMIDA Trial (A Randomized Trial of Efficacy, 12 Months International Double-Blind Actovegin®): A Randomized Controlled Trial to Assess the Efficacy of Actovegin® in Poststroke Cognitive Impairment | Guekht et al. [63] (in the body text—see further) | Yes | 2017 | 33 | 11 | 6 |
| 4 | Towards the Concept of Disease-Modifier in Post-Stroke or Vascular Cognitive Impairment: A Consensus Report | Bordet et al. [64] (in the body text—see further) | Yes | 2017 | 23 | ~8 | 4 |
| 5 | Diabetes and the Brain: Issues and Unmet Needs | Bornstein et al. [65] (in the body text—see further) | Yes | 2014 | 43 | 7 | 4 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Firan, F.C.; Romila, A.; Onose, G. Current Synthesis and Systematic Review of Main Effects of Calf Blood Deproteinized Medicine (Actovegin®) in Ischemic Stroke. Int. J. Mol. Sci. 2020, 21, 3181. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21093181
Firan FC, Romila A, Onose G. Current Synthesis and Systematic Review of Main Effects of Calf Blood Deproteinized Medicine (Actovegin®) in Ischemic Stroke. International Journal of Molecular Sciences. 2020; 21(9):3181. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21093181
Chicago/Turabian StyleFiran, Florentina Carmen, Aurelia Romila, and Gelu Onose. 2020. "Current Synthesis and Systematic Review of Main Effects of Calf Blood Deproteinized Medicine (Actovegin®) in Ischemic Stroke" International Journal of Molecular Sciences 21, no. 9: 3181. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21093181