Rheumatic Manifestations in Patients Treated with Immune Checkpoint Inhibitors

 ,
,
Abstract
:1. Introduction
2. Methods
3. Results
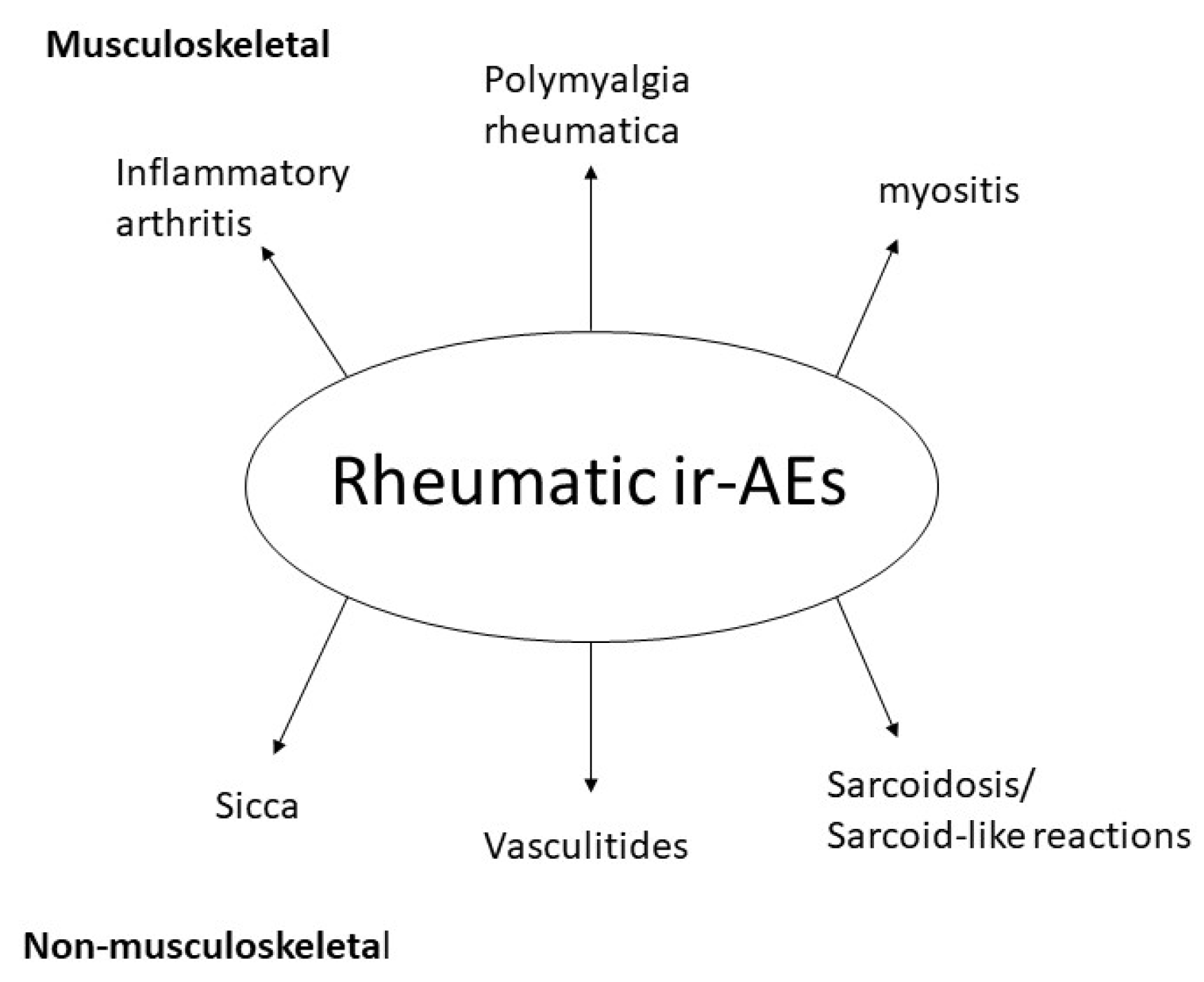
3.1. Musculoskeletal Immune-Related Adverse Events
3.1.1. Inflammatory Arthritis
3.1.2. Polymyalgia Rheumatica
3.1.3. Myositis
3.1.4. Association of Immune Checkpoint Inhibitor (ICI)-Induced Musculoskeletal Manifestations and Oncological Response
3.2. Non-Musculoskeletal Rheumatic Manifestations Induced by ICIs
3.2.1. Vasculitis
3.2.2. Sarcoidosis and Sarcoid-Like Reactions
3.3. Sicca and Sjogren’s Syndrome
3.4. Systemic Connective Tissue Diseases
3.4.1. Systemic Lupus Erythematosus (SLE)
3.4.2. Systemic Sclerosis (SSc)
4. Discussion
Funding
Acknowledgments
Conflicts of Interest
References
- Topalian, S.L.; Wolchok, J.D.; Chan, T.A.; Mellman, I.; Palucka, K.; Banchereau, J.; Rosenberg, S.A.; Wittrup, K.D. Immunotherapy: The path to win the war on cancer? Cell 2015, 161, 185–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Topalian, S.L.; Drake, C.G.; Pardoll, D.M. Immune checkpoint blockade: A common denominator approach to cancer therapy. Cancer Cell 2015, 27, 450–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, J.; Yu, J.X.; Hubbard-Lucey, V.M.; Neftelinov, S.T.; Hodge, J.P.; Lin, Y. The clinical trial landscape for PD1/PDl1 immune checkpoint inhibitors. Nat. Rev. Drug Discov. 2018, 17, 854–855. [Google Scholar] [CrossRef] [PubMed]
- Xu, C.; Chen, Y.P.; Du, X.J.; Liu, J.Q.; Huang, C.L.; Chen, L.; Zhou, G.Q.; Li, W.F.; Mao, Y.P.; Hsu, C.; et al. Comparative safety of immune checkpoint inhibitors in cancer: Systematic review and network meta-analysis. BMJ 2018, 363. [Google Scholar] [CrossRef]
- Postow, M.A.; Sidlow, R.; Hellmann, M.D. Immune-related adverse events associated with immune checkpoint blockade. N. Engl. J. Med. 2018, 378, 158–168. [Google Scholar] [CrossRef]
- Brahmer, J.R.; Lacchetti, C.; Schneider, B.J.; Atkins, M.B.; Brassil, K.J.; Caterino, J.M.; Chau, I.; Ernstoff, M.S.; Gardner, J.M.; Ginex, P.; et al. Management of Immune-Related Adverse Events in Patients Treated with Immune Checkpoint Inhibitor Therapy: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2018, 36, 1714–1768. [Google Scholar] [CrossRef]
- Calabrese, L.H.; Calabrese, C.; Cappelli, L.C. Rheumatic immune-related adverse events from cancer immunotherapy. Nat. Rev. Rheumatol. 2018, 14, 569–579. [Google Scholar] [CrossRef]
- Cappelli, L.C.; Gutierrez, A.K.; Bingham, C.O.; Shah, A.A. Rheumatic and Musculoskeletal Immune-Related Adverse Events Due to Immune Checkpoint Inhibitors: A Systematic Review of the Literature. Arthritis Care Res. 2017, 69, 1751–1763. [Google Scholar] [CrossRef] [Green Version]
- Abdel-Wahab, N.; Suarez-Almazor, M.E. Frequency and distribution of various rheumatic disorders associated with checkpoint inhibitor therapy. Rheumatology 2019, 58, vii40–vii48. [Google Scholar] [CrossRef] [Green Version]
- Daoussis, D.; Kraniotis, P.; Filippopoulou, A.; Argiriadi, R.; Theodoraki, S.; Makatsoris, T.; Koutras, A.; Kehagias, I.; Papachristou, D.J.; Solomou, A.; et al. An MRI study of immune checkpoint inhibitor–induced musculoskeletal manifestations myofasciitis is the prominent imaging finding. Rheumatology 2019. [Google Scholar] [CrossRef]
- Kostine, M.; Rouxel, L.; Barnetche, T.; Veillon, R.; Martin, F.; Dutriaux, C.; Dousset, L.; Pham-Ledard, A.; Prey, S.; Beylot-Barry, M.; et al. Rheumatic disorders associated with immune checkpoint inhibitors in patients with cancer-clinical aspects and relationship with tumour response: A single-centre prospective cohort study. Ann. Rheum. Dis. 2018, 77, 393–398. [Google Scholar] [CrossRef] [PubMed]
- Narváez, J.; Juarez-López, P.; LLuch, J.; Narváez, J.A.; Palmero, R.; García del Muro, X.; Nolla, J.M.; Domingo-Domenech, E. Rheumatic immune-related adverse events in patients on anti-PD-1 inhibitors: Fasciitis with myositis syndrome as a new complication of immunotherapy. Autoimmun. Rev. 2018, 1040–1045. [Google Scholar] [CrossRef] [PubMed]
- Kostine, M.; Truchetet, M.-E.; Schaeverbeke, T. Clinical characteristics of rheumatic syndromes associated with checkpoint inhibitors therapy. Rheumatology 2019, 58 (Suppl. 7), vii68–vii74. [Google Scholar] [CrossRef] [Green Version]
- Pundole, X.; Abdel-Wahab, N.; Suarez-Almazor, M.E. Arthritis risk with immune checkpoint inhibitor therapy for cancer. Curr. Opin. Rheumatol. 2019, 31, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O.; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef] [PubMed]
- Ngo, L.; Miller, E.; Valen, P.; Gertner, E. Nivolumab induced remitting seronegative symmetrical synovitis with pitting edema in a patient with melanoma: A case report. J. Med. Case Rep. 2018, 12, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amini-Adle, M.; Piperno, M.; Tordo, J.; Thomas, L.; Dalle, S.; Dubois, V.; Marabelle, A. Remitting Seronegative Symmetric Synovitis With Pitting Edema Associated With Partial Melanoma Response Under Anti-CTLA-4 and Anti-Programmed Death 1 Combination Treatment. Arthritis Rheumatol. 2018, 70, 1358. [Google Scholar] [CrossRef] [Green Version]
- Gauci, M.L.; Baroudjian, B.; Laly, P.; Madelaine, I.; Da Meda, L.; Vercellino, L.; Bagot, M.; Lioté, F.; Pages, C.; Lebbé, C. Remitting seronegative symmetrical synovitis with pitting edema (RS3PE) syndrome induced by nivolumab. Semin. Arthritis Rheum. 2017, 47, 281–287. [Google Scholar] [CrossRef]
- Wada, N.; Uchi, H.; Furue, M. Case of remitting seronegative symmetrical synovitis with pitting edema (RS3PE) syndrome induced by nivolumab in a patient with advanced malignant melanoma. J. Dermatol. 2017, 44, e196–e197. [Google Scholar] [CrossRef]
- Cappelli, L.C.; Gutierrez, A.K.; Baer, A.N.; Albayda, J.; Manno, R.L.; Haque, U.; Lipson, E.J.; Bleich, K.B.; Shah, A.A.; Naidoo, J.; et al. Inflammatory arthritis and sicca syndrome induced by nivolumab and ipilimumab. Ann. Rheum. Dis. 2017, 76, 43–50. [Google Scholar] [CrossRef]
- Cappelli, L.C.; Brahmer, J.R.; Forde, P.M.; Le, D.T.; Lipson, E.J.; Naidoo, J.; Zheng, L.; Bingham, C.O.; Shah, A.A. Clinical presentation of immune checkpoint inhibitor-induced inflammatory arthritis differs by immunotherapy regimen. Semin. Arthritis Rheum. 2018, 48, 553–557. [Google Scholar] [CrossRef] [PubMed]
- Braaten, T.J.; Brahmer, J.R.; Forde, P.M.; Le, D.; Lipson, E.J.; Naidoo, J.; Schollenberger, M.; Zheng, L.; Bingham, C.O.; Shah, A.A.; et al. Immune checkpoint inhibitor-induced inflammatory arthritis persists after immunotherapy cessation. Ann. Rheum. Dis. 2019. [Google Scholar] [CrossRef]
- Albayda, J.; Dein, E.; Shah, A.A.; Bingham, C.O.; Cappelli, L. Sonographic Findings in Inflammatory Arthritis Secondary to Immune Checkpoint Inhibition: A Case Series. ACR Open Rheumatol. 2019, 1, 303–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Subedi, A.; Williams, S.G.; Yao, L.; Maharjan, S.; Strauss, J.; Sharon, E.; Thomas, A.; Apolo, A.B.; Gourh, P.; Hasni, S.A.; et al. Use of Magnetic Resonance Imaging to Identify Immune Checkpoint Inhibitor–Induced Inflammatory Arthritis. JAMA Netw. Open 2020, 3, e200032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dasgupta, B.; Cimmino, M.A.; Maradit-Kremers, H.; Schmidt, W.A.; Schirmer, M.; Salvarani, C.; Bachta, A.; Dejaco, C.; Duftner, C.; Jensen, H.S.; et al. 2012 provisional classification criteria for polymyalgia rheumatica: A European League Against Rheumatism/American College of Rheumatology collaborative initiative. Ann. Rheum. Dis. 2012, 71, 484–492. [Google Scholar] [CrossRef] [Green Version]
- Richter, M.D.; Crowson, C.; Kottschade, L.A.; Finnes, H.D.; Markovic, S.N.; Thanarajasingam, U. Rheumatic Syndromes Associated With Immune Checkpoint Inhibitors: A Single-Center Cohort of Sixty-One Patients. Arthritis Rheumatol. 2019, 71, 468–475. [Google Scholar] [CrossRef] [Green Version]
- Belkhir, R.; Le Burel, S.; Dunogeant, L.; Marabelle, A.; Hollebecque, A.; Besse, B.; Leary, A.; Voisin, A.-L.; Pontoizeau, C.; Coutte, L.; et al. Rheumatoid arthritis and polymyalgia rheumatica occurring after immune checkpoint inhibitor treatment. Ann. Rheum. Dis. 2017, 76, 1747–1750. [Google Scholar] [CrossRef]
- Le Burel, S.; Champiat, S.; Mateus, C.; Marabelle, A.; Michot, J.-M.; Robert, C.; Belkhir, R.; Soria, J.-C.; Laghouati, S.; Voisin, A.-L.; et al. Prevalence of immune-related systemic adverse events in patients treated with anti-Programmed cell Death 1/anti-Programmed cell Death-Ligand 1 agents: A single-centre pharmacovigilance database analysis. Eur. J. Cancer 2017, 82, 34–44. [Google Scholar] [CrossRef]
- Mitchell, E.L.; Lau, P.K.H.; Khoo, C.; Liew, D.; Leung, J.; Liu, B.; Rischin, A.; Frauman, A.G.; Kee, D.; Smith, K.; et al. Rheumatic immune-related adverse events secondary to anti–programmed death-1 antibodies and preliminary analysis on the impact of corticosteroids on anti-tumour response: A case series. Eur. J. Cancer 2018, 105, 88–102. [Google Scholar] [CrossRef]
- Calabrese, C.; Kirchner, E.; Kontzias, K.; Velcheti, V.; Calabrese, L.H. Rheumatic immune-related adverse events of checkpoint therapy for cancer: Case series of a new nosological entity. RMD Open 2017. [Google Scholar] [CrossRef] [Green Version]
- Mooradian, M.J.; Nasrallah, M.; Gainor, J.F.; Reynolds, K.L.; Cohen, J.V.; Lawrence, D.P.; Miloslavsky, E.M.; Kohler, M.J.; Sullivan, R.J.; Schoenfeld, S.R. Musculoskeletal rheumatic complications of immune checkpoint inhibitor therapy: A single center experience. Semin. Arthritis Rheum. 2019, 48, 1127–1132. [Google Scholar] [CrossRef] [PubMed]
- Calabrese, C.; Cappelli, L.C.; Kostine, M.; Kirchner, E.; Braaten, T.; Calabrese, L. Polymyalgia rheumatica-like syndrome from checkpoint inhibitor therapy: Case series and systematic review of the literature. RMD Open 2019, 5, e000906. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, B.L.; Gedmintas, L.; Todd, D.J. Drug-associated polymyalgia rheumatica/giant cell arteritis occurring in two patients after treatment with ipilimumab, an antagonist of ctla-4. Arthritis Rheumatol. 2014, 66, 768–769. [Google Scholar] [CrossRef]
- Dalakas, M.C.; Hohlfeld, R. Polymyositis and dermatomyositis. Lancet 2003, 362, 971–982. [Google Scholar] [CrossRef]
- Shibata, C.; Kato, J.; Toda, N.; Imai, M.; Fukumura, Y.; Arai, J.; Kurokawa, K.; Kondo, M.; Takagi, K.; Kojima, K.; et al. Paraneoplastic dermatomyositis appearing after nivolumab therapy for gastric cancer: A case report. J. Med. Case Rep. 2019, 13, 168. [Google Scholar] [CrossRef] [PubMed]
- Anquetil, C.; Salem, J.E.; Lebrun-Vignes, B.; Johnson, D.B.; Mammen, A.L.; Stenzel, W.; Léonard-Louis, S.; Benveniste, O.; Moslehi, J.J.; Allenbach, Y. Immune checkpoint inhibitor–associated myositis: Expanding the spectrum of cardiac complications of the immunotherapy revolution. Circulation 2018, 138, 743–745. [Google Scholar] [CrossRef]
- Nguyễn, T.; Maria, A.T.J.; Ladhari, C.; Palassin, P.; Quantin, X.; Lesage, C.; Taïeb, G.; Ayrignac, X.; Rullier, P.; Hillaire-Buys, D.; et al. Rheumatic disorders associated with immune checkpoint inhibitors: What about myositis? An analysis of the WHO’s adverse drug reactions database. Ann. Rheum. Dis. 2020. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, S.; Ishikawa, N.; Konoeda, F.; Seki, N.; Fukushima, S.; Takahashi, K.; Uhara, H.; Hasegawa, Y.; Inomata, S.; Otani, Y.; et al. Nivolumab-related myasthenia gravis with myositis and myocarditis in Japan. Neurology 2017, 89, 1127–1134. [Google Scholar] [CrossRef]
- Touat, M.; Maisonobe, T.; Knauss, S.; Ben Hadj Salem, O.; Hervier, B.; Auré, K.; Szwebel, T.-A.; Kramkimel, N.; Lethrosne, C.; Bruch, J.-F.; et al. Immune checkpoint inhibitor-related myositis and myocarditis in patients with cancer. Neurology 2018, 91, e985–e994. [Google Scholar] [CrossRef]
- Shah, M.; Tayar, J.H.; Abdel-Wahab, N.; Suarez-Almazor, M.E. Myositis as an adverse event of immune checkpoint blockade for cancer therapy. Semin. Arthritis Rheum. 2019, 48, 736–740. [Google Scholar] [CrossRef]
- Moreira, A.; Loquai, C.; Pföhler, C.; Kähler, K.C.; Knauss, S.; Heppt, M.V.; Gutzmer, R.; Dimitriou, F.; Meier, F.; Mitzel-Rink, H.; et al. Myositis and neuromuscular side-effects induced by immune checkpoint inhibitors. Eur. J. Cancer 2019, 106, 12–23. [Google Scholar] [CrossRef] [PubMed]
- Matas-García, A.; Milisenda, J.C.; Selva-O’Callaghan, A.; Prieto-González, S.; Padrosa, J.; Cabrera, C.; Reguart, N.; Castrejón, N.; Solé, M.; Ros, J.; et al. Emerging PD-1 and PD-1L inhibitors-associated myopathy with a characteristic histopathological pattern. Autoimmun. Rev. 2020, 19, 102455. [Google Scholar] [CrossRef] [PubMed]
- Safa, H.; Johnson, D.H.; Trinh, V.A.; Rodgers, T.E.; Lin, H.; Suarez-Almazor, M.E.; Fa’ak, F.; Saberian, C.; Yee, C.; Davies, M.A.; et al. Immune checkpoint inhibitor related myasthenia gravis: Single center experience and systematic review of the literature. J. Immunother. Cancer 2019, 7, 319. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.B.; Balko, J.M.; Compton, M.L.; Chalkias, S.; Gorham, J.; Xu, Y.; Hicks, M.; Puzanov, I.; Alexander, M.R.; Bloomer, T.L.; et al. Fulminant Myocarditis with Combination Immune Checkpoint Blockade. N. Engl. J. Med. 2016, 375, 1749–1755. [Google Scholar] [CrossRef]
- Norwood, T.G.; Westbrook, B.C.; Johnson, D.B.; Litovsky, S.H.; Terry, N.L.; McKee, S.B.; Gertler, A.S.; Moslehi, J.J.; Conry, R.M. Smoldering myocarditis following immune checkpoint blockade. J. Immunother. Cancer 2017, 5, 91. [Google Scholar] [CrossRef]
- Daoussis, D.; Kraniotis, P.; Liossis, S.-N.; Solomou, A. Immune checkpoint inhibitor-induced myo-fasciitis. Rheumatology 2017, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delyon, J.; Brunet-Possenti, F.; Leonard-Louis, S.; Arangalage, D.; Baudet, M.; Baroudjian, B.; Lebbe, C.; Hervier, B. Immune checkpoint inhibitor rechallenge in patients with immune-related myositis. Ann. Rheum. Dis. 2019, 78, e129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Psimaras, D.; Velasco, R.; Birzu, C.; Tamburin, S.; Lustberg, M.; Bruna, J.; Argyriou, A.A. Immune checkpoint inhibitors-induced neuromuscular toxicity: From pathogenesis to treatment. J. Peripher. Nerv. Syst. 2019, 24. [Google Scholar] [CrossRef] [PubMed]
- Das, S.; Johnson, D.B. Immune-related adverse events and anti-tumor efficacy of immune checkpoint inhibitors. J. Immunother. Cancer 2019, 7, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Weyand, C.M.; Berry, G.J.; Goronzy, J.J. The immunoinhibitory PD-1/PD-L1 pathway in inflammatory blood vessel disease. J. Leukoc. Biol. 2018, 103, 565–575. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, R.; Zhang, H.; Berry, G.; Goronzy, J.J.; Weyand, C.M. Immune checkpoint dysfunction in large and medium vessel vasculitis. Am. J. Physiol. Heart Circ. Physiol. 2017, 312, H1052–H1059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, H.; Watanabe, R.; Berry, G.J.; Vaglio, A.; Liao, Y.J.; Warrington, K.J.; Goronzi, J.J.; Weyand, C.M. Immunoinhibitory checkpoint deficiency in medium & large vessel vasculitis. Proc. Natl. Acad. Sci. USA 2017, 114, E970–E979. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cadena, R.H.; Reitsema, R.D.; Huitema, M.G.; van Sleen, Y.; van der Geest, K.S.M.; Heeringa, P.; Boots, A.M.H.; Abdulahad, W.H.; Brower, E. Decreased expression of negative immune checkpoint VistA by CD4+ T cells facilitates T helper 1, T helper 17, and T follicular helper lineage differentiation in GCA. Front. Immunol. 2019, 10, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Daxini, A.; Cronin, K.; Sreih, A.G. Vasculitis associated with immune checkpoint inhibitors—A systematic review. Clin. Rheumatol. 2018, 37. [Google Scholar] [CrossRef] [PubMed]
- Hersh, E.M.; O’Day, S.J.; Powderly, J.; Khan, K.D.; Pavlik, A.C.; Cranmer, L.D.; Samlowski, W.E.; Nichol, G.M.; Yellin, M.J.; Weber, J.S. A phase II multicenter study of ipilimumab with or without dacarbazine in chemotherapy-naive patients with advanced melanoma. Invest. New Drugs 2011, 29, 489–498. [Google Scholar] [CrossRef] [PubMed]
- Hodi, F.S.; Lawrence, D.; Lezcano, C.; Wu, X.; Zhou, J.; Sasada, T.; Zeng, W.; Giobbie-Hurder, A.; Atkins, M.B.; Ibrahim, N.; et al. Bevacizumab plus Ipilimumab in Patients with Metastatic Melanoma. Cancer Immunol. Res. 2014, 2, 632–642. [Google Scholar] [CrossRef] [Green Version]
- Cadena, R.H.; Abdulahad, W.H.; Hospers, G.A.P.; Wind, T.T.; Boots, A.M.H.; Heeringa, P.; Brouwer, E. Checks and balances in autoimmune vasculitis. Front. Immunol. 2018, 9, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Roy, A.K.; Tathireddy, H.R.; Roy, M. Aftermath of induced inflammation: Acute periaortitis due to nivolumab therapy. Case Rep. 2017, 3–5. [Google Scholar] [CrossRef] [Green Version]
- Van den Brom, R.R.H.; Abdulahad, W.H.; Rutgers, A.; Kroesen, B.J.; Roozendaal, C.; de Groot, D.J.; Schröder, C.P.; Hospers, G.A.; Brouwer, E. Rapid granulomatosis with polyangiitis induced by immune checkpoint inhibition. Rheumatology 2016, 55, 1143–1145. [Google Scholar] [CrossRef] [Green Version]
- Sibille, A.; Alfieri, R.; Malaise, O.; Detrembleur, N.; Pirotte, M.; Louis, R.; Duysinx, B. Granulomatosis with polyangiitis in a patient on programmed death-1 inhibitor for advanced non-small-cell lung cancer. Front. Oncol. 2019, 9, 1–4. [Google Scholar] [CrossRef]
- Roger, A.; Groh, M.; Lorillon, G.; Le Pendu, C.; Maillet, J.; Arangalage, D.; Tazi, A.; Lebbe, C.; Baroudjian, B.; Delyon, J.; et al. Eosinophilic granulomatosis with polyangiitis (Churg-Strauss) induced by immune checkpoint inhibitors. Ann. Rheum. Dis. 2019, 78, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Le Burel, S.; Champiat, S.; Routier, E.; Aspeslagh, S.; Albiges, L.; Szwebel, T.A.; Michot, J.M.; Chretien, P.; Mariette, X.; Voisin, A.L.; et al. Onset of connective tissue disease following anti-PD1/PD-L1 cancer immunotherapy. Ann. Rheum. Dis. 2018, 77, 468–470. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Wolfe, S.P.; Alloo, A.; Gottesman, S.P. Interstitial granulomatous dermatitis and granulomatous arteritis in the setting of PD-1 inhibitor therapy for metastatic melanoma. J. Cutan. Pathol. 2020, 47, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Arellano, K.; Mosley, J.C.; Moore, D.C. Case Report of Ipilimumab-Induced Diffuse, Nonnecrotizing Granulomatous Lymphadenitis and Granulomatous Vasculitis. J. Pharm. Pract. 2018, 31, 227–229. [Google Scholar] [CrossRef]
- Tomelleri, A.; Campochiaro, C.; De Luca, G.; Cavalli, G.; Dagna, L. Anti-PD1 therapy-associated cutaneous leucocytoclastic vasculitis: A case series. Eur. J. Intern. Med. 2018, 57, e11–e12. [Google Scholar] [CrossRef] [PubMed]
- Läubli, H.; Hench, J.; Stanczak, M.; Heijnen, I.; Papachristofilou, A.; Frank, S.; Zippelius, A.; Stenner-Liewen, F. Cerebral vasculitis mimicking intracranial metastatic progression of lung cancer during PD-1 blockade. J. Immunother. Cancer 2017, 5, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Bender, C.; Dimitrakopoulou-Strauss, A.; Enk, A.; Hassel, J.C. Safety of the PD-1 antibody pembrolizumab in patients with high-grade adverse events under ipilimumab treatment. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2016, 27, 1353–1354. [Google Scholar] [CrossRef] [PubMed]
- Khoja, L.; Maurice, C.; Chappell, M.; MacMillan, L.; Al-Habeeb, A.S.; Al-Faraidy, N.; Butler, M.O.; Rogalla, P.; Mason, W.; Joshua, A.M.; et al. Eosinophilic fasciitis and acute encephalopathy toxicity from pembrolizumab treatment of a patient with metastatic melanoma. Cancer Immunol. Res. 2016, 4, 175–178. [Google Scholar] [CrossRef] [Green Version]
- Kao, J.C.; Liao, B.; Markovic, S.N.; Klein, C.J.; Naddaf, E.; Staff, N.P.; Liewluck, T.; Hammack, J.E.; Sandroni, P.; Finnes, H.; et al. Neurological Complications Associated With Anti-Programmed Death 1 (PD-1) Antibodies. JAMA Neurol. 2017, 74, 1216–1222. [Google Scholar] [CrossRef]
- Aya, F.; Ruiz-Esquide, V.; Viladot, M.; Font, C.; Prieto-González, S.; Prat, A.; Arance, A. Vasculitic neuropathy induced by pembrolizumab. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2017, 28, 433–434. [Google Scholar] [CrossRef]
- Tsui, E.; Gonzales, J.A. Retinal Vasculitis Associated with Ipilimumab. Ocul. Immunol. Inflamm. 2019, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Manusow, J.S.; Khoja, L.; Pesin, N.; Joshua, A.M.; Mandelcorn, E.D. Retinal vasculitis and ocular vitreous metastasis following complete response to PD-1 inhibition in a patient with metastatic cutaneous melanoma. J. Immunother. Cancer 2015, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Emens, L.A.; Davis, S.L.; Oliver, S.C.N. Association of Cancer Immunotherapy with Acute Macular Neuroretinopathy and Diffuse Retinal Venulitis. JAMA Ophthalmol. 2019, 137, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Weiner, R.; Hanson, B.; Rehman, J.; Sun, B. Isolated testicular vasculitis due to immune checkpoint inhibitor. Eur. J. Rheumatol. 2020, 7, 35–36. [Google Scholar] [CrossRef] [PubMed]
- Minor, D.R.; Bunker, S.R.; Doyle, J. Lymphocytic Vasculitis of the Uterus in a Patient With Melanoma Receiving Ipilimumab. J. Clin. Oncol. 2015, 31. [Google Scholar] [CrossRef] [PubMed]
- Khaddour, K.; Singh, V.; Shayuk, M. Acral vascular necrosis associated with immune-check point inhibitors: Case report with literature review. BMC Cancer 2019, 19, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Gambichler, T.; Strutzmann, S.; Tannapfel, A.; Susok, L. Paraneoplastic acral vascular syndrome in a patient with metastatic melanoma under immune checkpoint blockade. BMC Cancer 2017, 17, 327. [Google Scholar] [CrossRef] [Green Version]
- Padda, A.; Schiopu, E.; Sovich, J.; Ma, V.; Alva, A.; Fecher, L. Ipilimumab induced digital vasculitis. J. Immunother. Cancer 2018, 3–7. [Google Scholar] [CrossRef] [Green Version]
- Comont, T.; Sibaud, V.; Mourey, L.; Cougoul, P.; Beyne-Rauzy, O. Immune checkpoint inhibitor-related acral vasculitis. J. Immunother. Cancer. 2018, 6, 120. [Google Scholar] [CrossRef] [Green Version]
- Park, H.J.; Ranganathan, P. Neoplastic and paraneoplastic vasculitis, vasculopathy, and hypercoagulability. Rheum. Dis. Clin. N. Am. 2011, 37, 593–606. [Google Scholar] [CrossRef]
- Cornejo, C.M.; Haun, P.; English, J., 3rd. Rosenbach, M. Immune checkpoint inhibitors and the development of granulomatous reactions. J. Am. Acad. Dermatol. 2019, 81, 1165–1175. [Google Scholar] [CrossRef] [PubMed]
- Broos, C.E.; van Nimwegen, M.; Int Veen, J.C.C.M.; Hoogsteden, H.C.; Hendriks, R.W.; van den Blink, B.; Kool, M. Decreased Cytotoxic T-Lymphocyte Antigen 4 Expression on Regulatory T Cells and Th17 Cells in Sarcoidosis: Double Trouble? Am. J. Respir. Crit. Care Med. 2015, 192, 763–765. [Google Scholar] [CrossRef] [PubMed]
- Von Euw, E.; Chodon, T.; Attar, N.; Jalil, J.; Koya, R.C.; Comin-Anduix, B.; Ribas, A. CTLA4 blockade increases Th17 cells in patients with metastatic melanoma. J. Transl. Med. 2009, 7, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perez-De-Lis, M.; Retamozo, S.; Flores-Chavez, A.; Kostov, B.; Perez-Alvarez, R.; Brito-Zerón, P.; Ramos-Casals, M. Autoimmune diseases induced by biological agents. A review of 12,731 cases (BIOGEAS Registry). Expert Opin. Drug Saf. 2017, 16, 1255–1271. [Google Scholar] [CrossRef]
- Birnbaum, M.R.; Ma, M.W.; Fleisig, S.; Packer, S.; Amin, B.D.; Jacobson, M.; McLellan, B.N. Nivolumab-related cutaneous sarcoidosis in a patient with lung adenocarcinoma. JAAD Case Rep. 2017, 3, 208–211. [Google Scholar] [CrossRef] [Green Version]
- Gkiozos, I.; Kopitopoulou, A.; Kalkanis, A.; Vamvakaris, I.N.; Judson, M.A.; Syrigos, K.N. Sarcoidosis-Like Reactions Induced by Checkpoint Inhibitors. J. Thorac. Oncol. 2018, 13, 1076–1082. [Google Scholar] [CrossRef]
- Dunn-Pirio, A.M.; Shah, S.; Eckstein, C. Neurosarcoidosis following Immune Checkpoint Inhibition. Case Rep. Oncol. 2018, 11, 521–526. [Google Scholar] [CrossRef]
- Tan, I.; Malinzak, M.; Salama, A.K.S. Delayed onset of neurosarcoidosis after concurrent ipilimumab/nivolumab therapy. J. Immunother. Cancer 2018, 6, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Lise, Q.K.; Audrey, A.G. Multifocal choroiditis as the first sign of systemic sarcoidosis associated with pembrolizumab. Am. J. Ophthalmol. Case Rep. 2017, 5, 92–93. [Google Scholar] [CrossRef]
- Zimmer, L.; Goldinger, S.M.; Hofmann, L.; Loquai, C.; Ugurel, S.; Thomas, I.; Schmidgen, M.I.; Gutzmer, R.; Utikal, J.S.; Göppner, D.; et al. Neurological, respiratory, musculoskeletal, cardiac and ocular side-effects of anti-PD-1 therapy. Eur. J. Cancer 2016, 60, 210–225. [Google Scholar] [CrossRef]
- Eckert, A.; Schoeffler, A.; Dalle, S.; Phan, A.; Kiakouama, L.; Thomas, L. Anti-CTLA4 monoclonal antibody induced sarcoidosis in a metastatic melanoma patient. Dermatology 2009, 218, 69–70. [Google Scholar] [CrossRef] [PubMed]
- Thajudeen, B.; Madhrira, M.; Bracamonte, E.; Cranmer, L.D. Ipilimumab granulomatous interstitial nephritis. Am. J. Ther. 2015, 22, e84–e87. [Google Scholar] [CrossRef] [PubMed]
- Berthod, G.; Lazor, R.; Letovanec, I.; Romano, E.; Noirez, L.; Mazza Stalder, J.; Speiser, D.E.; Peters, S.M.O. Pulmonary sarcoid-like granulomatosis induced by ipilimumab. J. Clin. Oncol. 2012, 10, e156–e159. [Google Scholar] [CrossRef]
- Benfaremo, D.; Manfredi, L.; Luchetti, M.M.; Gabrielli, A. Musculoskeletal and Rheumatic Diseases Induced by Immune Checkpoint Inhibitors: A Review of the Literature. Curr. Drug Saf. 2018, 13. [Google Scholar] [CrossRef] [PubMed]
- Chopra, A.; Nautiyal, A.; Kalkanis, A.; Judson, M.A. Drug-Induced Sarcoidosis-Like Reactions. Chest 2018, 154, 664–677. [Google Scholar] [CrossRef] [PubMed]
- Kluger, N. Tattoo Reactions Associated with Targeted Therapies and Immune Checkpoint Inhibitors for Advanced Cancers: A Brief Review. Dermatology 2019, 235, 522–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bronstein, Y.; Ng, C.S.; Hwu, P.; Hwu, W.-J. Radiologic manifestations of immune-related adverse events in patients with metastatic melanoma undergoing anti-CTLA-4 antibody therapy. AJR Am. J. Roentgenol. 2011, 197, W992–W1000. [Google Scholar] [CrossRef]
- Tirumani, S.H.; Ramaiya, N.H.; Keraliya, A.; Bailey, N.D.; Ott, P.A.; Hodi, F.S.; Nishino, M. Radiographic Profiling of Immune-Related Adverse Events in Advanced Melanoma Patients Treated with Ipilimumab. Cancer Immunol. Res. 2015, 3, 1185–1192. [Google Scholar] [CrossRef] [Green Version]
- Nishino, M.; Hatabu, H.; Sholl, L.M.; Ramaiya, N.H. Thoracic complications of precision cancer therapies: A practical guide for radiologists in the new era of cancer care1. Radiographics 2017, 37, 1371–1387. [Google Scholar] [CrossRef]
- Rodriguez, E.F.; Lipson, E.; Suresh, K.; Cappelli, L.C.; Monaco, S.E.; Maleki, Z. Immune checkpoint blocker-related sarcoid-like granulomatous inflammation: A rare adverse event detected in lymph node aspiration cytology of patients treated for advanced malignant melanoma. Hum. Pathol. 2019, 91, 69–76. [Google Scholar] [CrossRef]
- Montaudie, H.; Pradelli, J.; Passeron, T.; Lacour, J.-P.; Leroy, S. Pulmonary sarcoid-like granulomatosis induced by nivolumab. Br. J. Dermatol. 2017, 176, 1060–1063. [Google Scholar] [CrossRef] [PubMed]
- Reuss, J.E.; Kunk, P.R.; Stowman, A.M.; Gru, A.A.; Slingluff, C.L.; Gaughan, E.M. Sarcoidosis in the setting of combination ipilimumab and nivolumab immunotherapy: A case report & review of the literature. J. Immunother. Cancer 2016, 4, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Rambhia, P.H.; Reichert, B.; Scott, J.F.; Feneran, A.N.; Kazakov, J.A.; Honda, K.; Koon, H.; Gerstenblith, M.R. Immune checkpoint inhibitor-induced sarcoidosis-like granulomas. Int. J. Clin. Oncol. 2019, 24, 1171–1181. [Google Scholar] [CrossRef] [PubMed]
- Tetzlaff, M.T.; Nelson, K.C.; Diab, A.; Staerkel, G.A.; Nagarajan, P.; Torres-Cabala, C.A.; Chasen, B.A.; Wargo, J.A.; Prieto, V.G.; Amaria, R.N.; et al. Granulomatous/sarcoid-like lesions associated with checkpoint inhibitors: A marker of therapy response in a subset of melanoma patients. J. Immunother. Cancer 2018, 6, 1–11. [Google Scholar] [CrossRef]
- Moutsopoulos, H.M. Sjogren’s syndrome: A forty-year scientific journey. J. Autoimmun. 2014, 51, 1–9. [Google Scholar] [CrossRef]
- Goules, A.V.; Kapsogeorgou, E.K.; Tzioufas, A.G. Insight into pathogenesis of Sjogren’s syndrome: Dissection on autoimmune infiltrates and epithelial cells. Clin. Immunol. 2017, 182, 30–40. [Google Scholar] [CrossRef]
- Huang, C.; Zhu, H.X.; Yao, Y.; Bian, Z.-H.; Zheng, Y.-J.; Li, L.; Moutsopoulos, H.M.; Gershwin, M.E.; Lian, Z.-X. Immune checkpoint molecules. Possible future therapeutic implications in autoimmune diseases. J. Autoimmun. 2019, 104. [Google Scholar] [CrossRef]
- Downie-Doyle, S.; Bayat, N.; Rischmueller, M.; Lester, S. Influence of CTLA4 haplotypes on susceptibility and some extraglandular manifestations in primary Sjogren’s syndrome. Arthritis Rheum. 2006, 54, 2434–2440. [Google Scholar] [CrossRef]
- Gottenberg, J.-E.; Loiseau, P.; Azarian, M.; Chen, C.; Cagnard, N.; Hachulla, E.; Puechal, X.; Sibilia, J.; Charron, D.; Mariette, X.; et al. CTLA-4 +49A/G and CT60 gene polymorphisms in primary Sjogren syndrome. Arthritis Res. Ther. 2007, 9, R24. [Google Scholar] [CrossRef] [Green Version]
- Yin, H.; Nguyen, C.Q.; Samuni, Y.; Uede, T.; Peck, A.B.; Chiorini, J.A. Local delivery of AAV2-CTLA4IgG decreases sialadenitis and improves gland function in the C57BL/6.NOD-Aec1Aec2 mouse model of Sjogren’s syndrome. Arthritis Res. Ther. 2012, 14, R40. [Google Scholar] [CrossRef] [Green Version]
- Klocke, K.; Sakaguchi, S.; Holmdahl, R.; Wing, K. Induction of autoimmune disease by deletion of CTLA-4 in mice in adulthood. Proc. Natl. Acad. Sci. USA 2016, 113, E2383–E2392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, J.; Jin, J.-O.; Kawai, T.; Yu, Q. Endogenous programmed death ligand-1 restrains the development and onset of Sjgren’s syndrome in non-obese diabetic mice. Sci. Rep. 2016, 6, 39105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdel-Rahman, O.; Oweira, H.; Petrausch, U.; Helbling, D.; Schmidt, J.; Mannhart, M.; Mehrabi, A.; Schob, O.; Giryes, A. Immune-related ocular toxicities in solid tumor patients treated with immune checkpoint inhibitors: A systematic review. Expert Rev. Anticancer Ther. 2017, 17, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Warner, B.M.; Baer, A.N.; Lipson, E.J.; Allen, C.; Hinrichs, C.; Rajan, A.; Pelayo, E.; Beach, M.; Gulley, J.L.; Madan, R.A.; et al. Sicca Syndrome Associated with Immune Checkpoint Inhibitor Therapy. Oncologist 2019, 24, 1259–1269. [Google Scholar] [CrossRef] [Green Version]
- Ortiz Brugués, A.; Sibaud, V.; Herbault-Barrés, B.; Betrian, S.; Korakis, I.; De Bataille, C.; Gomez-Roca, C.; Epstein, J.; Vigarios, E. Sicca Syndrome Induced by Immune Checkpoint Inhibitor Therapy: Optimal Management Still Pending. Oncologist 2020, 25, 391–395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramos-Casals, M.; Maria, A.; Suarez-Almazor, M.E.; Lambotte, O.; Fisher, B.A.; Hernandez-Molina, G.; Guilpain, P.; Pundole, X.; Flores-Chavez, A.; Baldini, C.; et al. Sicca/Sjogren’s syndrome triggered by PD-1/PD-L1 checkpoint inhibitors. Data from the International ImmunoCancer Registry (ICIR). Clin. Exp. Rheumatol. 2019, 37 (Suppl. 1), 114–122. [Google Scholar]
- Nishimura, H.; Nose, M.; Hiai, H.; Minato, N.; Honjo, T. Development of lupus-like autoimmune diseases by disruption of the PD-1 gene encoding an ITIM motif-carrying immunoreceptor. Immunity. 1999, 11, 141–151. [Google Scholar] [CrossRef] [Green Version]
- Ceeraz, S.; Nowak, E.C.; Burns, C.M.; Noelle, R.J. Immune checkpoint receptors in regulating immune reactivity in rheumatic disease. Arthritis Res. Ther. 2014, 16, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Lu, K.-L.; Wu, M.-Y.; Wang, C.-H.; Wang, C.-H.; Hung, H.-L.; Cung, W.-H.; Chen, C.-B. The Role of Immune Checkpoint Receptors in Regulating Immune Reactivity in Lupus. Cells 2019, 8, 1213. [Google Scholar] [CrossRef] [Green Version]
- Arnaud, L.; Lebrun-Vignes, B.; Salem, J.-E. Checkpoint inhibitor-associated immune arthritis. Ann. Rheum. Dis. 2019, 78, e68. [Google Scholar] [CrossRef] [Green Version]
- Raschi, E.; Antonazzo, I.C.; Poluzzi, E.; De Ponti, F. Drug-induced systemic lupus erythematosus: Should immune checkpoint inhibitors be added to the evolving list? Ann. Rheum. Dis. 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michot, J.-M.; Fusellier, M.; Champiat, S.; Velter, C.; Baldini, C.; Voisin, A.-L.; Danlos, F.-X.; El Dakdouki, Y.; Annereau, M.; Mariette, X.; et al. Drug-induced lupus erythematosus following immunotherapy with anti-programmed death-(ligand) 1. Ann. Rheum. Dis. 2019, 78, e67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fadel, F.; El Karoui, K.; Knebelmann, B. Anti-CTLA4 antibody-induced lupus nephritis. N. Engl. J. Med. 2009, 361, 211–212. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, N.S.; Wetter, D.A.; Wieland, C.N.; Shenoy, N.K.; Markovic, S.N.; Thanarajasingam, U. Scleroderma Induced by Pembrolizumab: A Case Series. Mayo Clin. Proc. 2017, 92, 1158–1163. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| RA | ICI-Induced Arthritis |
| Usually involves small joints of the hands in a symmetrical fashion | May manifest as mono, oligo or polyarthritis |
| Synovium is primarily targeted | Apart from synovitis, myo-fasciitis may be prominent |
| Responds to steroids but treatment with DMARDs is always needed | Good response to steroids DMARD needed when relapse occurs during steroid tapering |
| PMR | ICI-Induced PMR |
| Aching and stiffness in the shoulder and pelvic girdles are typical symptoms | Joint involvement, including knees and hands, may occur |
| High inflammatory markers are a diagnostic criterion | Absence of increased inflammatory markers is reported in several cases |
| Responds to low dose of steroids (prednisolone, 20 mg/daily) | Aggressive treatment with higher doses of steroids may be needed |
| Polymyositis/Dermatomyositis | ICI-Induced Myositis |
| Typical clinical presentation involves proximal muscle weakness, without associated muscle pain, sparing facial muscles Dermatomyositis exhibits typical rash | May present with myalgia and oculomotor symptoms, while typical rash is usually absent |
| Increase in muscle enzymes and autoantibodies against nuclear or cytoplasmic antigens aid diagnosis | May exhibit significant increase in muscle enzymes, albeit normal in a subset of patients Autoantibodies are usually absent |
| High-dose steroids are the mainstay of treatment Additional immunosuppression is needed in resistant disease and extramuscular features such as ILD | High-dose steroids are usually required, even though milder clinical phenotypes respond well to moderate doses Increased frequency of concurrent myasthenia and/or cardiac involvement is reported and may warrant additional immunosuppression |
| Systemic Vasculitides | ICI-Induced Vasculitis |
| High inflammatory burden is typical Autoantibodies, such as ANCA, can aid diagnosis in subsets of the disease | Inflammatory markers are commonly increased, but autoantibody positivity is rare |
| Sjogren Syndrome | ICI-Induced Sicca |
| Striking female preponderance | Male predominance in some case series |
| Specific autoantibodies are typically positive | Absence of autoantibodies is reported in most cases |
| Dry eyes and dry mouth are the most frequent complaints | Dry mouth is the most prominent symptom |
| SLE | ICI-Induced Lupus |
| Typically affects females of childbearing age Antinuclear antibodies are almost always positive | Older age, lack of striking female predominance and absence of autoantibodies are reported |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Melissaropoulos, K.; Klavdianou, K.; Filippopoulou, A.; Kalofonou, F.; Kalofonos, H.; Daoussis, D. Rheumatic Manifestations in Patients Treated with Immune Checkpoint Inhibitors. Int. J. Mol. Sci. 2020, 21, 3389. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21093389
Melissaropoulos K, Klavdianou K, Filippopoulou A, Kalofonou F, Kalofonos H, Daoussis D. Rheumatic Manifestations in Patients Treated with Immune Checkpoint Inhibitors. International Journal of Molecular Sciences. 2020; 21(9):3389. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21093389
Chicago/Turabian StyleMelissaropoulos, Konstantinos, Kalliopi Klavdianou, Alexandra Filippopoulou, Fotini Kalofonou, Haralabos Kalofonos, and Dimitrios Daoussis. 2020. "Rheumatic Manifestations in Patients Treated with Immune Checkpoint Inhibitors" International Journal of Molecular Sciences 21, no. 9: 3389. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21093389