
Gender Differences in Diabetic Kidney Disease: Focus on Hormonal, Genetic and Clinical Factors

 ,
,  ,
,  , ,
, ,
Abstract
:1. Introduction
2. Gender Differences in the Prevalence of DKD and its Phenotypes
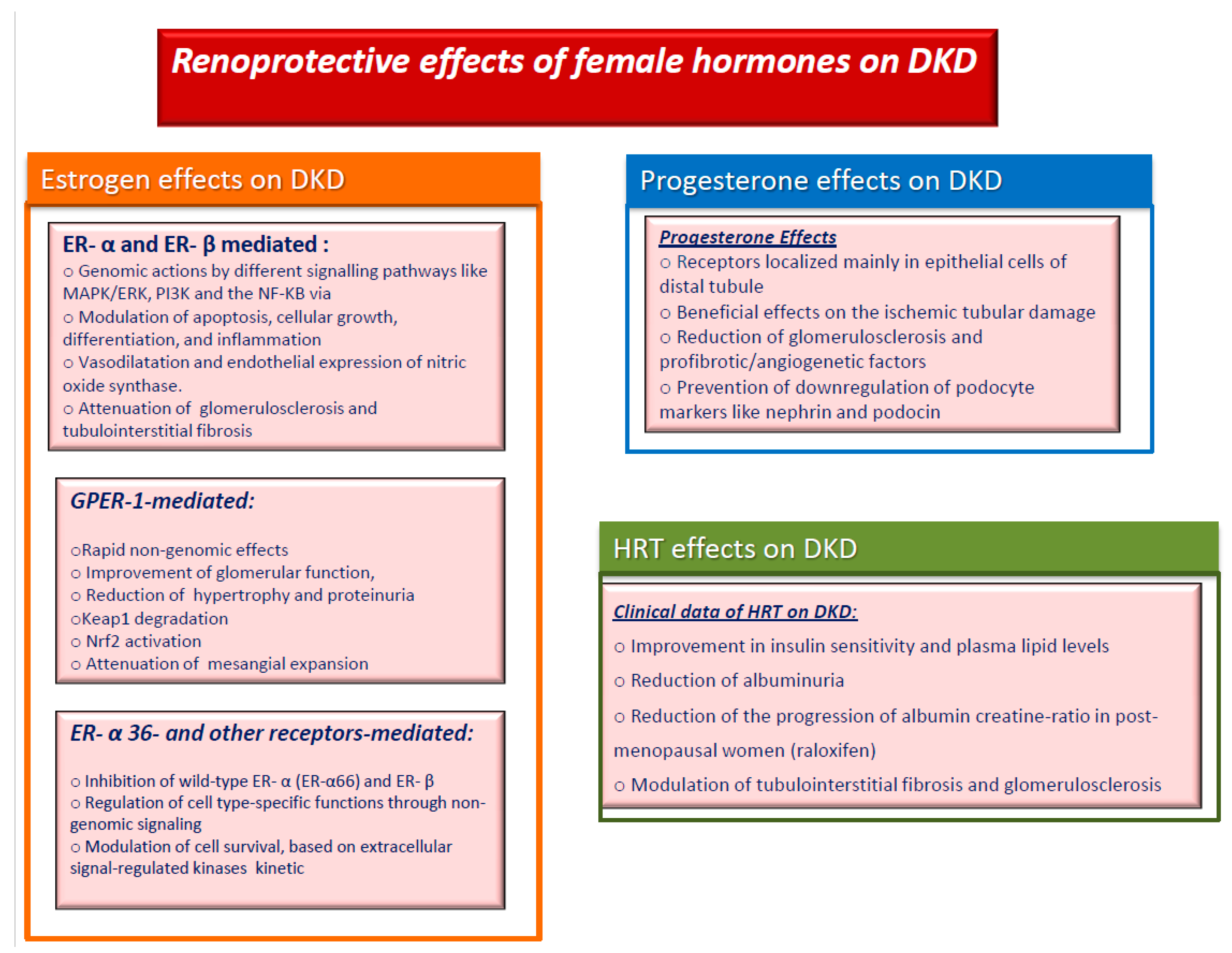
3. Impact of Female Sex Hormones on DKD
4. Impact of Sex Genes Interactions on DKD
5. Gender Differences in DKD Risk Factors and Renoprotective Drugs
6. Conclusions
Funding
Conflicts of Interest
References
- Rossi, M.C.; Cristofaro, M.R.; Gentile, S.; Lucisano, G.; Manicardi, V.; Mulas, M.F.; Napoli, A.; Nicolucci, A.; Pellegrini, F.; Suraci, C.; et al. Sex disparities in the quality of diabetes care: Biological and cultural factors may play a different role for different outcomes: A cross-sectional observational study from the AMD Annals initiative. Diabetes Care 2013, 36, 162–168. [Google Scholar] [CrossRef] [Green Version]
- De Boer, I.H.; Caramori, M.L.; Chan, J.C.N.; Heerspink, H.J.L.; Hurst, C.; Khunti, K.; Liew, A.; Michos, E.D.; Navaneethan, S.D.; Olowu, W.A.; et al. KDIGO 2020 clinical practice guideline for diabetes management in chronic kidney disease. Kidney Int. 2020, 98, S1–S115. [Google Scholar] [CrossRef]
- Bolignano, D.; Cernaro, V.; Gembillo, G.; Baggetta, R.; Buemi, M.; D’Arrigo, G. Antioxidant agents for delaying diabetic kidney disease progression: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0178699. [Google Scholar] [CrossRef]
- Viazzi, F.; Russo, G.T.; Ceriello, A.; Fioretto, P.; Giorda, C.; De Cosmo, S.; Pontremoli, R. Natural history and risk factors for diabetic kidney disease in patients with T2D: Lessons from the AMD-annals. J. Nephrol. 2019, 32, 517–525. [Google Scholar] [CrossRef]
- Pugliese, G.; Penno, G.; Natali, A.; Barutta, F.; Di Paolo, S.; Reboldi, G.; Gesualdo, L.; De Nicola, L. Italian Diabetes Society and the Italian Society of Nephrology. Diabetic kidney disease: New clinical and therapeutic issues. Joint position statement of the Italian Diabetes Society and the Italian Society of Nephrology on “The natural history of diabetic kidney disease and treatment of hyperglycemia in patients with type 2 diabetes and impaired renal function”. J. Nephrol. 2020, 9–35. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.K. Sex as an important biological variable in biomedical research. BMB Rep. 2018, 51, 167–173. [Google Scholar] [CrossRef] [Green Version]
- Gemmati, D.; Varani, K.; Bramanti, B.; Piva, R.; Bonaccorsi, G.; Trentini, A.; Manfrinato, M.C.; Tisato, V.; Carè, A.; Bellini, T. “Bridging the Gap” Everything that Could Have Been Avoided If We Had Applied Gender Medicine, Pharmacogenetics and Personalized Medicine in the Gender-Omics and Sex-Omics Era. Int. J. Mol. Sci. 2019, 21, 296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cañadas-Garre, M.; Anderson, K.; Cappa, R.; Skelly, R.; Smyth, L.J.; McKnight, A.J.; Maxwell, A.P. Genetic Susceptibility to Chronic Kidney Disease–Some More Pieces for the Heritability Puzzle. Front. Genet. 2019, 10, 453. [Google Scholar] [CrossRef]
- Siligato, R.; Gembillo, G.; Cernaro, V.; Torre, F.; Salvo, A.; Granese, R.; Santoro, D. Maternal and Fetal Outcomes of Pregnancy in Nephrotic Syndrome Due to Primary Glomerulonephritis. Front. Med. 2020, 7, 563094. [Google Scholar] [CrossRef] [PubMed]
- Bang, H.; Vupputuri, S.; Shoham, D.A.; Klemmer, P.J.; Falk, R.J.; Mazumdar, M.; Gipson, D.; Colindres, R.E.; Kshirsagar, A.V. SCreening for Occult REnal Disease (SCORED): A simple prediction model for chronic kidney disease. Arch. Intern. Med. 2007, 167, 374–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Süleymanlar, G.; Utaş, C.; Arinsoy, T.; Ateş, K.; Altun, B.; Altiparmak, M.R.; Ecder, T.; Yilmaz, M.E.; Çamsari, T.; Başçi, A.; et al. A population-based survey of Chronic REnal Disease In Turkey--the CREDIT study. Nephrol. Dial. Transplant. 2010, 26, 1862–1871. [Google Scholar] [CrossRef] [PubMed]
- Hill, N.R.; Fatoba, S.T.; Oke, J.L.; Hirst, J.A.; O’Callaghan, C.A.; Lasserson, D.S.; Hobbs, F.D. Global Prevalence of Chronic Kidney Disease-A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0158765. [Google Scholar] [CrossRef] [PubMed]
- Ricardo, A.C.; Yang, W.; Sha, D.; Appel, L.J.; Chen, J.; Krousel-Wood, M.; Manoharan, A.; Steigerwalt, S.; Wright, J.; Rahman, M.; et al. Sex-Related Disparities in CKD Progression. J. Am. Soc. Nephrol. 2019, 30, 137–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, W.; Xie, D.; Anderson, A.H.; Joffe, M.M.; Greene, T.; Teal, V.; Hsu, C.Y.; Fink, J.C.; He, J.; Lash, J.P.; et al. Association of kidney disease outcomes with risk factors for CKD: Findings from the Chronic Renal Insufficiency Cohort (CRIC) study. Am. J. Kidney Dis. 2014, 63, 236–243. [Google Scholar] [CrossRef] [Green Version]
- Swartling, O.; Rydell, H.; Stendahl, M.; Segelmark, M.; Lagerros, Y.T.; Evans, M. CKD Progression and Mortality Among Men and Women: A Nationwide Study in Sweden. Am. J. Kidney Dis. 2021, 9. [Google Scholar] [CrossRef]
- Neugarten, J.; Acharya, A.; Silbiger, S.R. Effect of gender on the progression of nondiabetic renal disease: A meta-analysis. J. Am. Soc. Nephrol. 2000, 11, 319–329. [Google Scholar] [CrossRef]
- Iseki, K. Gender differences in chronic kidney disease. Kidney Int. 2008, 74, 415–417. [Google Scholar] [CrossRef] [Green Version]
- Jafar, T.H.; Schmid, C.; Stark, P.C.; Toto, R.D.; Remuzzi, G.; Ruggenenti, P.; Marcantoni, C.; Becker, G.J.; Shahinfar, S.; De Jong, P.E.; et al. The rate of progression of renal disease may not be slower in women compared with men: A patient-level meta-analysis. Nephrol. Dial. Transplant. 2003, 18, 2047–2053. [Google Scholar] [CrossRef] [PubMed]
- Bash, L.D.; Coresh, J.; Köttgen, A.; Parekh, R.S.; Fulop, T.; Wang, Y.; Astor, B.C. Defining incident chronic kidney disease in the research setting: The ARIC Study. Am. J. Epidemiol. 2009, 170, 414–424. [Google Scholar] [CrossRef]
- Gall, M.A.; Hougaard, P.; Borch-Johnsen, K.; Parving, H.H. Risk factors for development of incipient and overt diabetic nephropathy in patients with non-insulin dependent diabetes mellitus: Prospective, observational study. BMJ 1997, 314, 783–788. [Google Scholar] [CrossRef] [Green Version]
- Lewis, E.J.; Hunsicker, L.G.; Rodby, R.A. A clinical trial in type 2 diabetic nephropathy. Am. J. Kidney Dis. 2001, 38 (Suppl. S1), S191–S194. [Google Scholar] [CrossRef] [PubMed]
- Keane, W.F.; Brenner, B.M.; de Zeeuw, D.; Grunfeld, J.P.; McGill, J.; Mitch, W.E.; Ribeiro, A.B.; Shahinfar, S.; Simpson, R.L.; Snapinn, S.M.; et al. The risk of developing end-stage renal disease in patients with type 2 diabetes and nephropathy: The RENAAL study. Kidney Int. 2003, 63, 1499–1507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rossing, K.; Christensen, P.K.; Hovind, P.; Tarnow, L.; Rossing, P.; Parving, H.H. Progression of nephropathy in type 2 diabetic patients. Kidney Int. 2004, 66, 1596–1605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Retnakaran, R.; Cull, C.A.; Thorne, K.I.; Adler, A.I.; Holman, R.R.; UKPDS Study Group. Risk factors for renal dysfunction in type 2 diabetes: U.K. Prospective Diabetes Study 74. Diabetes 2006, 55, 1832–1839. [Google Scholar] [CrossRef] [Green Version]
- Penno, G.; Solini, A.; Bonora, E.; Fondelli, C.; Orsi, E.; Zerbini, G.; Trevisan, R.; Vedovato, M.; Gruden, G.; Laviola, L.; et al. Gender differences in cardiovascular disease risk factors, treatments and complications in patients with type 2 diabetes: The RIACE Italian multicentre study. J. Intern. Med. 2013, 274, 176–191. [Google Scholar] [CrossRef]
- Yu, M.K.; Lyles, C.R.; Bent-Shaw, L.A.; Young, B.A. Pathways Authors. Risk factor, age and sex differences in chronic kidney disease prevalence in a diabetic cohort: The pathways study. Am. J. Nephrol. 2012, 36, 245–251. [Google Scholar] [CrossRef] [Green Version]
- Jardine, M.J.; Hata, J.; Woodward, M.; Perkovic, V.; Ninomiya, T.; Arima, H.; Zoungas, S.; Cass, A.; Patel, A.; Marre, M.; et al. Prediction of kidney-related outcomes in patients with type 2 diabetes. Am. J. Kidney Dis. 2012, 60, 770–778. [Google Scholar] [CrossRef]
- Zoppini, G.; Targher, G.; Chonchol, M.; Ortalda, V.; Negri, G.; Stoico, V.; Bonora, E. Predictors of Estimated GFR Decline in Patients withType 2 Diabetes and Preserved Kidney Function. Clin. J. Am. Soc. Nephrol. 2012, 7, 401–408. [Google Scholar] [CrossRef] [Green Version]
- Altemtam, N.; Russell, J.; El Nahas, M. A study of the natural history of diabetic kidney disease (DKD). Nephrol. Dial. Transplant. 2012, 27, 1847–1854. [Google Scholar] [CrossRef] [Green Version]
- Elley, C.R.; Robinson, T.; Moyes, S.A.; Kenealy, T.; Collins, J.; Robinson, E.; Orr-Walker, B.; Drury, P.L. Derivation and validation of a renal risk score for people with type 2 diabetes. Diabetes Care 2013, 36, 3113–3120. [Google Scholar] [CrossRef] [Green Version]
- De Hauteclocque, A.; Ragot, S.; Slaoui, Y.; Gand, E.; Miot, A.; Sosner, P.; Halimi, J.-M.; Zaoui, P.; Rigalleau, V.; Roussel, R.; et al. The influence of sex on renal function decline in people with type 2 diabetes. Diabet Med. 2014, 31, 1121–1128. [Google Scholar] [CrossRef] [PubMed]
- Kajiwara, A.; Kita, A.; Saruwatari, J.; Miyazaki, H.; Kawata, Y.; Morita, K.; Oniki, K.; Yoshida, A.; Jinnouchi, H.; Nakagawa, K. Sex differences in the renal function decline of patients with type 2 diabetes. J. Diabetes Res. 2016, 2016, 4626382. [Google Scholar] [CrossRef] [Green Version]
- Orchard, T.J.; Dorman, J.S.; Maser, R.E.; Becker, D.J.; Drash, A.L.; Ellis, D.; LaPorte, R.E.; Kuller, L.H. Prevalence of complications in IDDM by sex and duration. Pittsburgh Epidemiology of Diabetes Complications Study II. Diabetes 1990, 39, 1116–1124. [Google Scholar] [CrossRef]
- Lovshin, J.A.; Škrtić, M.; Bjornstad, P.; Moineddin, R.; Daneman, D.; Dunger, P.D.; Reich, H.N.; Mahmud, F.H.; Scholey, J.W.; Cherney, D.Z.I.; et al. Hyperfiltration, urinaryalbumin excretion, and ambulatory blood pressure in adolescents with Type 1 diabetes mellitus. Am. J. Physiol. Renal. Physiol. 2018, 314, F667–F674. [Google Scholar] [CrossRef] [Green Version]
- Holl, R.W.; Grabert, M.; Thon, A.; Heinze, E. Urinary excretion of albumin in adolescents with type 1 diabetes: Persistent versus intermittent microalbuminuria and relationship to duration of diabetes, sex, and metabolic control. Diabetes Care 1999, 22, 1555–1560. [Google Scholar] [CrossRef]
- Jacobsen, P.; Rossing, K.; Tarnow, L.; Rossing, P.; Mallet, C.; Poirier, O.; Cambien, F.; Parving, H.-H. Progression of diabetic nephropathy in normotensive type 1 diabetic patients. Kidney Int Suppl. 1999, 71, S101–S105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rossing, P.; Hougaard, P.; Parving, H.H. Risk factors for development of incipient and overt diabetic nephropathy in type 1 diabetic patients: A 10-year prospective observational study. Diabetes Care 2002, 25, 859–864. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Krzentowski, G.; Albert, A.; Lefebvre, P.J. Factors predictive of nephropathy in DCCT Type 1 diabetic patients with good or poor metabolic control. Diabet Med. 2003, 20, 580–585. [Google Scholar] [CrossRef] [PubMed]
- Hovind, P.; Tarnow, L.; Rossing, P.; Graae, M.; Torp, I.; Binder, C.; Parving, H.-H. Predictors for the development of microalbuminuria and macroalbuminuria in patients with type 1 diabetes: Inception cohort study. BMJ 2004, 328, 1105. [Google Scholar] [CrossRef] [Green Version]
- Finne, P.; Reunanen, A.; Stenman, S.; Groop, P.H.; GronhagenRiska, C. Incidence of end-stage renal disease in patients with type 1 diabetes. JAMA 2005, 294, 1782–1787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sibley, S.D.; Thomas, W.; de Boer, I.; Brunzell, J.D.; Steffes, M.W. Gender and elevated albumin excretion in the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications (DCCT/EDIC) cohort: Role of central obesity. Am. J. Kidney Dis. 2006, 47, 223–232. [Google Scholar] [CrossRef]
- Raile, K.; Galler, A.; Hofer, S.; Herbst, A.; Dunstheimer, D.; Busch, P.; Holl, R.W. Diabetic nephropathy in 27,805 children, adolescents, and adults with type 1 diabetes: Effect of diabetes duration, A1C, hypertension, dyslipidemia, diabetes onset, and sex. Diabetes Care 2007, 30, 2523–2528. [Google Scholar] [CrossRef] [Green Version]
- Monti, M.C.; Lonsdale, J.T.; Montomoli, C.; Montross, R.; Schlag, E.; Greenberg, D.A. Familial risk factors for microvascular complications and differential male-female risk in a large cohort of American families with type 1 diabetes. J. Clin. Endocrinol. Metab. 2007, 92, 4650–4655. [Google Scholar] [CrossRef]
- Mollsten, A.; Svensson, M.; Waernbaum, I.; Berhan, Y.; Schon, S.; Nystrom, L.; Arnqvist, H.J.; Dahlquist, G. Cumulative risk, age at onset and sex-specific differences for developing endstage renal disease in young patients with type 1 diabetes. A nationwide population based cohort study. Diabetes 2010, 59, 1803–1808. [Google Scholar]
- Costacou, T.; Fried, L.; Ellis, D.; Orchard, T.J. Sex differences in the development of kidney disease in individuals with type 1 diabetes mellitus: A contemporary analysis. Am. J. Kidney Dis. 2011, 58, 565–573. [Google Scholar] [CrossRef] [Green Version]
- Harjutsalo, V.; on behalf of the FinnDiane Study Group; Maric, C.; Forsblom, C.; Thorn, L.; Wadén, J.; Groop, P.H. Sex-related differences in the long-term risk of microvascular complications by age at onset of type 1 diabetes. Diabetologia 2011, 54, 1992–1999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kautzky-Willer, A.; Stich, K.; Hintersteiner, J.; Kautzky, A.; Kamyar, M.R.; Saukel, J.; Johnson, J.; Lemmens-Gruber, R. Sex-specificdifferences in cardiometabolic risk in type 1 diabetes: A cross-sectional study. Cardiovasc. Diabetol. 2013, 12, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skupien, J.; Smiles, A.M.; Valo, E.; Ahluwalia, T.S.; Gyorgy, B.; Sandholm, N.; Croall, S.; Lajer, M.; McDonnell, K.; Forsblom, C.; et al. Variations in Risk of EndStage Renal Disease and Risk of Mortality in an International Study of Patients With Type 1 Diabetes and Advanced Nephropathy. Diabetes Care 2019, 42, 93–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dyck, R.F.; Tan, L. Rates and outcomes of diabetic end-stage renal disease among registered native people in Saskatchewan. CMAJ 1994, 150, 203–208. [Google Scholar]
- Haroun, M.K.; Jaar, B.G.; Hoffman, S.C.; Comstock, G.W.; Klag, M.J.; Coresh, J. Risk factors for chronic kidney disease: A prospective study of 23,534 men and women in Washington County, Maryland. J. Am. Soc. Nephrol. 2003, 14, 2934–2941. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xue, J.L.; Eggers, P.W.; Agodoa, L.Y.; Foley, R.N.; Collins, A.J. Longitudinal study of racial and ethnic differences in developing end-stage renal disease among aged medicare beneficiaries. J. Am. Soc. Nephrol. 2007, 18, 1299–1306. [Google Scholar] [CrossRef] [Green Version]
- Yamagata, K.; Ishida, K.; Sairenchi, T.; Takahashi, H.; Ohba, S.; Shiigai, T.; Narita, M.; Koyama, A. Risk factors for chronic kidney disease in a community-based population: A 10-year follow-up study. Kidney Int. 2007, 71, 159–166. [Google Scholar] [CrossRef] [Green Version]
- Hippisley-Cox, J.; Coupland, C. Predicting the risk of chronic Kidney Disease in men and women in England and Wales: Prospective derivation and external validation of the QKidney Scores. BMC Fam. Pract. 2010, 11, 49. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, F.; Haastert, B.; Koch, M.; Giani, G.; Glaeske, G.; Icks, A. The effect of diabetes on incidence and mortality in end-stage renal disease in Germany. Nephrol. Dial. Transplant. 2011, 26, 1634–1640. [Google Scholar] [CrossRef] [Green Version]
- Johnson, E.S.; Smith, D.H.; Thorp, M.L.; Yang, X.; Juhaeri, J. Predicting the risk of end-stage renal disease in the population-based setting: A retrospective case-control study. BMC Nephrol. 2011, 12, 17. [Google Scholar] [CrossRef] [Green Version]
- Tohidi, M.; Hasheminia, M.; Mohebi, R.; Khalili, D.; Hosseinpanah, F.; Yazdani, B.; Nasiri, A.A.; Azizi, F.; Hadaegh, F. Incidence of chronic kidney disease and its risk factors, results of over 10 year follow up in an Iranian cohort. PLoS ONE 2012, 7, e45304. [Google Scholar] [CrossRef]
- Nagai, K.; Saito, C.; Watanabe, F.; Ohkubo, R.; Sato, C.; Kawamura, T.; Uchida, K.; Hiwatashi, A.; Kai, H.; Ishida, K.; et al. Annual incidence of persistent proteinuria in the general population from Ibaraki annual urinalysis study. Clin. Exp. Nephrol. 2013, 17, 255–260. [Google Scholar] [CrossRef] [PubMed]
- van Blijderveen, J.C.; Straus, S.M.; Zietse, R.; Stricker, B.H.; Sturkenboom, M.C.; Verhamme, K.M. A population-based study on the prevalence and incidence of chronic kidney disease in the Netherlands. Int. Urol. Nephrol. 2014, 46, 583–592. [Google Scholar] [CrossRef] [PubMed]
- Maric-Bilkan, C. Sex differences in diabetic kidney disease. Mayo Clin. Proc. 2020, 95, 587–599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shepard, B.D. Sex differences in diabetes and kidney disease: Mechanisms and consequences. Am. J. Physiol. Renal. Physiol. 2019, 317, F456–F462. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Cai, R.; Sun, J.; Dong, X.; Huang, R.; Tian, S.; Wang, S. Diabetes mellitus as a risk factor for incident chronic kidney disease and end-stage renal disease in women compared with men: A systematic review and meta-analysis. Endocrine 2017, 55, 66–76. [Google Scholar] [CrossRef]
- Nag, S.; Bilous, R.; Kelly, W.; Jones, S.; Roper, N.; Connolly, V. All-cause and cardiovascular mortality in diabetic subjects increases significantly with reduced estimated glomerular filtration rate (eGFR): 10 years’ data from the South Tees Diabetes Mortality study. Diabet Med. 2007, 24, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Pugliese, G.; Solini, A.; Bonora, E.; Fondelli, C.; Orsi, E.; Nicolucci, A.; Penno, G.; RIACE Study Group. Chronic kidney disease in type 2 diabetes: Lessons from the Renal Insufficiency and Cardiovascular Events (RIACE) Italian Multicentre Study. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 815–822. [Google Scholar] [CrossRef] [PubMed]
- Russo, G.T.; De Cosmo, S.; Viazzi, F.; Mirijello, A.; Ceriello, A.; Guida, P.; Giorda, C.; Cucinotta, D.; Pontremoli, R.; Fioretto, P.; et al. Diabetic kidney disease in the elderly: Prevalence and clinical correlates. BMC Geriatr. 2018, 18, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, M.K.; Katon, W.; Young, B.A. Associations between sex and incident chronic kidney disease in a prospective diabetic cohort. Nephrology 2015, 20, 451–458. [Google Scholar] [CrossRef] [PubMed]
- A-AMD Annals: A model of continuous monitoring and improvement of the quality of diabetes care. Epidemiol. Prev. 2011, 35, 18–26.
- Mirijello, A.; Viazzi, F.; Fioretto, P.; Giorda, C.; Ceriello, A.; Russo, G.T.; Guida, P.; Pontremoli, R.; De Cosmo, S. Association of kidney disease measures with risk of renal function worsening in patients with type 1 diabetes. BMC Nephrol. 2018, 19, 347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piscitelli, P.; Viazzi, F.; Fioretto, P.; Giorda, C.; Ceriello, A.; Genovese, S.; Russo, G.; Guida, P.; Pontremoli, R.; De Cosmo, S. Predictors of chronic kidney disease in type 1 diabetes: A longitudinal study from the AMD Annals initiative. Sci. Rep. 2017, 7, 3313. [Google Scholar] [CrossRef]
- Pacilli, A.; Viazzi, F.; Fioretto, P.; Giorda, C.; Ceriello, A.; Genovese, S.; Russo, G.; Guida, P.; Pontremoli, R.; De Cosmo, S.; et al. Epidemiology of diabetic kidney disease in adult patients with type 1 diabetes in Italy: The AMD-Annals initiative. Diabetes Metab. Res. Rev. 2017, 33. [Google Scholar] [CrossRef]
- Manicardi, V.; Russo, G.; Napoli, A.; Torlone, E.; Li Volsi, P.; Giorda, C.B.; Musacchio, N.; Nicolucci, A.; Suraci, C.; Lucisano, G.; et al. Gender- Disparities in Adults with Type 1 Diabetes: More Than a Quality of Care Issue. A Cross-Sectional Observational Study from the AMD Annals Initiative. PLoS ONE 2016, 11, e0162960. [Google Scholar] [CrossRef]
- Viazzi, F.; Piscitelli, P.; Giorda, C.; Ceriello, A.; Genovese, S.; Russo, G.T.; Fioretto, P.; Guida, P.; De Cosmo, S.; Pontremoli, R. Association of kidney disease measures with risk of renal function worsening in patients with hypertension and type 2 diabetes. J. Diabetes Complicat. 2017, 31, 419–426. [Google Scholar] [CrossRef]
- De Cosmo, S.; Viazzi, F.; Pacilli, A.; Giorda, C.; Ceriello, A.; Gentile, S.; Russo, G.; Rossi, M.C.; Nicolucci, A.; Guida, P.; et al. Predictors of chronic kidney disease in type 2 diabetes: A longitudinal study from the AMD Annals initiative. Medicine 2016, 95, e4007. [Google Scholar] [CrossRef]
- De Cosmo, S.; Rossi, M.C.; Pellegrini, F.; Lucisano, G.; Bacci, S.; Gentile, S.; Ceriello, A.; Russo, G.; Nicolucci, A.; Giorda, C.; et al. Kidney dysfunction and related cardiovascular risk factors among patients with type 2 diabetes. Nephrol. Dial. Transplant. 2014, 29, 657–662. [Google Scholar] [CrossRef] [Green Version]
- Acconcia, F.; Kumar, R. Signaling regulation of genomic and nongenomic functions of estrogen receptors. Cancer Lett. 2006, 238, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Prossnitz, E.R.; Arterburn, J.B. International Union of Basic and Clinical Pharmacology. XCVII. G protein-coupled estrogen receptor and its pharmacologic modulators. Pharmacol. Rev. 2015, 67, 505–540. [Google Scholar] [CrossRef] [Green Version]
- Kiyama, R.; Wada-Kiyama, Y. Estrogenic endocrine disruptors: Molecular mechanisms of action. Environ. Int. 2015, 83, 11–40. [Google Scholar] [CrossRef]
- Venkov, C.D.; Rankin, A.B.; Vaughan, D.E. Identification of authentic estrogen receptor in cultured endothelial cells—A potential mechanism for steroid hormone regulation of endothelial function. Circulation 1996, 94, 727–733. [Google Scholar] [CrossRef]
- Meyer, M.R.; Barton, M. Estrogens and coronary artery disease: New clinical perspectives. Adv. Pharmacol. 2016, 77, 307–360. [Google Scholar]
- Burns Katherine, A.; Korach Kenneth, S. Estrogen receptors and human disease: An update. Arch. Toxicol. 2012, 10, 1491–1504. [Google Scholar] [CrossRef] [Green Version]
- Ribeiro, J.R.; Freiman, R.N. Estrogen signaling crosstalk: Implications for endocrine resistance in ovarian cancer. J. Steroid. Biochem. Mol. Biol. 2014, 143, 160–173. [Google Scholar] [CrossRef] [Green Version]
- Xing, D.; Nozell, S.; Chen, Y.F.; Hage, F.; Oparil, S. Estrogen and mechanisms of vascular protection. Arterioscler. Thromb. Vasc. Biol. 2009, 29, 289–295. [Google Scholar] [CrossRef] [Green Version]
- Lewis-Wambi, J.S.; Jordan, V.C. Estrogen regulation of apoptosis: How can one hormone stimulate and inhibit? Breast Cancer Res. 2009, 11, 206. [Google Scholar] [CrossRef] [Green Version]
- Roepke, T.A. Oestrogen modulates hypothalamic control of energy homeostasis through multiple mechanisms. J. Neuroendocrinol. 2009, 21, 141–150. [Google Scholar] [CrossRef] [Green Version]
- Barros, R.P.; Machado, U.F.; Warner, M.; Gustafsson, J.A. Muscle GLUT4 regulation by estrogen receptors ERbeta and ERalpha. Proc. Natl. Acad. Sci. USA 2006, 103, 1605–1608. [Google Scholar] [CrossRef] [Green Version]
- Heine, P.A.; Taylor, J.A.; Iwamoto, G.A.; Lubahn, D.B.; Cooke, P.S. Increased adipose tissue in male and female estrogen receptor-alpha knockout mice. Proc. Natl. Acad. Sci. USA 2000, 97, 12729–12734. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Cuenca, S.; Monjo, M.; Frontera, M.; Gianotti, M.; Proenza, A.M.; Roca, P. Sex steroid receptor expression profile in brown adipose tissue. Effects of hormonal status. Cell Physiol. Biochem. 2007, 20, 877–886. [Google Scholar] [CrossRef]
- Casazza, K.; Page, G.P.; Fernandez, J.R. The Association Between the rs2234693 and rs9340799 Estrogen Receptor α Gene Polymorphisms and Risk Factors for Cardiovascular Disease: A Review. Biol. Res. For. Nurs. 2010, 12, 84–97. [Google Scholar] [CrossRef]
- Gao, H.; Fält, S.; Sandelin, A.; Gustafsson, J.A.; Dahlman-Wright, K. Genome-wide identification of estrogen receptor alpha-binding sites in mouse liver. Mol. Endocrinol. 2008, 22, 10–22. [Google Scholar] [CrossRef] [Green Version]
- Brandenberger, A.W.; Tee, M.K.; Lee, J.Y.; Chao, V.; Jaffe, R.B. Tissue distribution of estrogen receptors alpha (ER-alpha) and beta (ER-beta) mRNA in the midgestational human fetus. J. Clin. Endocrinol. Metab. 1997, 82, 3509–3512. [Google Scholar]
- Evans, M.J.; Lai, K.; Shaw, L.J.; Harnish, D.C.; Chadwick, C.C. Estrogen receptor α inhibits IL-1β induction of gene expression in the mouse liver. Endocrinology 2002, 7, 2559–2570. [Google Scholar] [CrossRef]
- Fliegner, D.; Schubert, C.; Penkalla, A.; Witt, H.; Kararigas, G.; Dworatzek, E.; Staub, E.; Martus, P.; Ruiz Noppinger, P.; Kintscher, U.; et al. Female sex and estrogen receptor-beta attenuate cardiac remodeling and apoptosis in pressure overload. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2010, 298, R1597–R1606. [Google Scholar] [CrossRef]
- Gürgen, D.; Hegner, B.; Kusch, A.; Catar, R.; Chaykovska, L.; Hoff, U.; Dragun, D. Estrogen receptor-β signals left ventricular hypertrophy sex differences in normotensive deoxycorticosterone acetate-salt mice. Hypertension 2011, 57, 648–654. [Google Scholar] [CrossRef] [Green Version]
- Lovegrove, A.S.; Sun, J.; Gould, K.A.; Lubahn, D.B.; Korach, K.S.; Lane, P.H. Estrogen receptor alpha-mediated events promote sex-specific diabetic glomerular hypertrophy. Am. J. Physiol. Renal. Physiol. 2004, 287, F586–F591. [Google Scholar] [CrossRef]
- Shimizu, Y. [Estrogen: Estrone (E1), estradiol (E2), estriol (E3) and estetrol (E4)]. Nihon Rinsho. 2005, 63 (Suppl. S8), 425–438. (In Japanese) [Google Scholar] [PubMed]
- Dantas, A.P.V.; Fortes, Z.B.; de Carvalho, M.H.C. Vascular disease in diabetic women: Why do they miss the female protection? Exp. Diabetes Res. 2012, 570598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maric, C.; Sandberg, K.; Hinojosa-Laborde, C. Glomerulosclerosis and tubulointerstitial fibrosis are attenuated with 17beta-estradiol in the aging Dahl salt sensitive rat. J. Am. Soc. Nephrol. 2004, 15, 1546–1556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stringer, K.D.; Komers, R.; Osman, S.A.; Oyama, T.T.; Lindsley, J.N.; Anderson, S. Gender hormones and the progression of experimental polycystic kidney disease. Kidney Int. 2005, 68, 1729–1739. [Google Scholar] [CrossRef] [Green Version]
- Elliot, S.J.; Berho, M.; Korach, K.; Doublier, S.; Lupia, E.; Striker, G.E.; Karl, M. Gender-specific effects of endogenous testosterone: Female alpha-estrogen receptor-deficient C57Bl/6J mice develop glomerulosclerosis. Kidney Int. 2007, 72, 464–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Metcalfe Peter, D.; Leslie, J.A.; Campbell, M.T.; Meldrum, D.R.; Hile, K.L.; Meldrum, K.K. Testosterone exacerbates obstructive renal injury by stimulating TNF-α production and increasing proapoptotic and profibrotic signaling. Am. J. Physiol. Endocrinol. Metab. 2008, 294, E435–E443. [Google Scholar] [CrossRef] [Green Version]
- Reckelhoff, J.F.; Zhang, H.; Srivastava, K. Gender differences in development of hypertension in spontaneously hypertensive rats: Role of the renin-angiotensin system. Hypertension 2000, 35 Pt 2, 480–483. [Google Scholar] [CrossRef] [Green Version]
- Monster, T.B.; Janssen, W.M.; de Jong, P.E.; de Jong-van den Berg, L.T. Prevention of Renal and Vascular End Stage Disease Study Group. Oral contraceptive use and hormone replacement therapy are associated with microalbuminuria. Arch. Intern. Med. 2001, 161, 2000–2005. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, S.B.; Culleton, B.F.; Tonelli, M.; Klarenbach, S.W.; Macrae, J.M.; Zhang, J.; Hemmelgarn, B.R.; Alberta Kidney Disease Network. Oral estrogen therapy in postmenopausal women is associated with loss of kidney function. Kidney Int. 2008, 74, 370–376. [Google Scholar] [CrossRef] [Green Version]
- Alexander, S.P.; Mathie, A.; Peters, J.A. Guide to Receptors and Channels (GRAC), 5th edition. Br. J. Pharmacol. 2011, 164 (Suppl. S1), S1-324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hazell, G.G.; Yao, S.T.; Roper, J.A.; Prossnitz, E.R.; O’Carroll, A.M.; Lolait, S.J. Localisation of GPR30, a novel G protein-coupled oestrogen receptor, suggests multiple functions in rodent brain and peripheral tissues. J. Endocrinol. 2009, 202, 223–236. [Google Scholar] [CrossRef] [PubMed]
- Soltysik, K.; Czekaj, P. Membrane estrogen receptors—Is it an alternative way of estrogen action? J. Physiol. Pharmacol. 2013, 64, 129–142. [Google Scholar]
- Cheng, S.B.; Graeber, C.T.; Quinn, J.A.; Filardo, E.J. Retrograde transport of the transmembrane estrogen receptor, G-protein-coupled-receptor-30 (GPR30/GPER) from the plasma membrane towards the nucleus. Steroids 2011, 76, 892–896. [Google Scholar] [CrossRef]
- Cheng, S.B.; Dong, J.; Pang, Y.; LaRocca, J.; Hixon, M.; Thomas, P.; Filardo, E.J. Anatomical location and redistribution of G protein-coupled estrogen receptor-1 during the estrus cycle in mouse kidney and specific binding to estrogens but not aldosterone. Mol. Cell Endocrinol. 2014, 382, 950–959. [Google Scholar] [CrossRef]
- Lindsey, S.H.; Yamaleyeva, L.M.; Brosnihan, K.B.; Gallagher, P.E.; Chappell, M.C. Estrogen receptor GPR30 reduces oxidative stress and proteinuria in the salt-sensitive female mRen2.Lewis rat. Hypertension 2011, 58, 665–671. [Google Scholar] [CrossRef] [Green Version]
- Wang, K.; Zheng, X.; Pan, Z.; Yao, W.; Gao, X.; Wang, X.; Ding, X. Icariin Prevents Extracellular Matrix Accumulation and Ameliorates Experimental Diabetic Kidney Disease by Inhibiting Oxidative Stress via GPER Mediated p62-Dependent Keap1 Degradation and Nrf2 Activation. Front Cell Dev Biol. 2020, 8, 559. [Google Scholar] [CrossRef]
- Li, Q.; Sullivan, N.R.; McAllister, C.E.; Van de Kar, L.D.; Muma, N.A. Estradiol accelerates the effects of fluoxetine on serotonin 1A receptor signaling. Psychoneuroendocrinology 2013, 38, 1145–1157. [Google Scholar] [CrossRef] [Green Version]
- Xu, H.; Qin, S.; Carrasco, G.A.; Dai, Y.; Filardo, E.J.; Prossnitz, E.R.; Battaglia, G.; Doncarlos, L.L.; Muma, N.A. Extra-nuclear estrogen receptor GPR30 regulates serotonin function in rat hypothalamus. Neuroscience 2009, 158, 1599–1607. [Google Scholar] [CrossRef] [Green Version]
- McAllister, C.E.; Creech, R.D.; Kimball, P.A.; Muma, N.A.; Li, Q. GPR30 is necessary for estradiol-induced desensitization of 5-HT1A receptor signaling in the paraventricular nucleus of the rat hypothalamus. Psychoneuroendocrinology 2012, 37, 1248–1260. [Google Scholar] [CrossRef] [Green Version]
- Akama, K.T.; Thompson, L.I.; Milner, T.A.; McEwen, B.S. Post-synaptic density95 (PSD-95) binding capacity of G-protein-coupled receptor 30 (GPR30), an estrogen receptor that can be identified in hippocampal dendritic spines. J. Biol. Chem. 2013, 288, 6438–6450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.C.; Ding, X.S.; Li, H.M.; Zhang, C. Icariin attenuates high glucose-induced type IV collagen and fibronectin accumulation in glomerular mesangial cells by inhibiting transforming growth factor-β production and signalling through G protein-coupled oestrogen receptor 1. Clin. Exp. Pharmacol. Physiol. 2013, 40, 635–643. [Google Scholar] [CrossRef]
- Rowlands, D.J.; Chapple, S.; Siow, R.C.; Mann, G.E. Equol-stimulated mitochondrial reactive oxygen species activate endothelial nitric oxide synthase and redox signaling in endothelial cells: Roles for F-actin and GPR30. Hypertension 2011, 57, 833–840. [Google Scholar] [CrossRef]
- Rao, J.; Jiang, X.; Wang, Y.; Chen, B. 2011. Advances in the understanding of the structure and function of ER-α36, a novel variant of human estrogen receptor-alpha. J. Steroid Biochem. Mol. Biol. 2011, 127, 231–237. [Google Scholar] [CrossRef]
- Lin, S.L.; Yan, L.Y.; Liang, X.W.; Wang, Z.B.; Wang, Z.Y.; Qiao, J.; Schatten, H.; Sun, Q.Y. A novel variant of ER-alpha, ER-alpha36 mediates testosterone-stimulated ERK and Akt activation in endometrial cancer Hec1A cells. Reprod. Biol. Endocrinol. 2009, 7, 102. [Google Scholar] [CrossRef] [Green Version]
- Wells, C.C.; Riazi, S.; Mankhey, R.W.; Bhatti, F.; Ecelbarger, C.; Maric, C. Diabetic nephropathy is associated with decreased circulating estradiol levels and imbalance in the expression of renal estrogen receptors. Gend. Med. 2005, 2, 227–237. [Google Scholar] [CrossRef]
- Inada, A.; Inada, O.; Fujii, N.L.; Nagafuchi, S.; Katsuta, H.; Yasunami, Y.; Matsubara, T.; Arai, H.; Fukatsu, A.; Nabeshima, Y.I. Adjusting the 17β-Estradiol-to-Androgen Ratio Ameliorates Diabetic Nephropathy. J. Am. Soc. Nephrol. 2016, 27, 3035–3050. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manigrasso, M.B.; Sawyer, R.T.; Marbury, D.C.; Flynn, E.R.; Maric, C. Inhibition of estradiol synthesis attenuates renal injury in male streptozotocin-induced diabetic rats. Am. J. Physiol. Renal Physiol. 2011, 301, F634–F640. [Google Scholar] [CrossRef] [Green Version]
- Maric, C.; Forsblom, C.; Thorn, L.; Waden, J.; Groop, P.H.; FinnDiane Study Group. Association between testosterone, estradiol and sex hormone binding globulin levels in men with type 1 diabetes with nephropathy. Steroids 2010, 75, 772–778. [Google Scholar] [CrossRef] [Green Version]
- Matsushita, M.; Tamura, K.; Osada, S.; Kogo, H. Effect of troglitazone on the excess testosterone and LH secretion in thyroidectomized, insulin-resistant, type 2 diabetic Goto-Kakizaki rats. Endocrine 2005, 27, 301–305. [Google Scholar] [CrossRef]
- Salonia, A.; Lanzi, R.; Scavini, M.; Pontillo, M.; Gatti, E.; Petrella, G.; Licata, G.; Nappi, R.E.; Bosi, E.; Briganti, A.; et al. Sexual function and endocrine profile in fertile women with type 1 diabetes. Diabetes Care 2006, 29, 312–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersson, B.; Mattsson, L.A.; Hahn, L.; Mårin, P.; Lapidus, L.; Holm, G.; Bengtsson, B.A.; Björntorp, P. Estrogen replacement therapy decreases hyperandrogenicity and improves glucose homeostasis and plasma lipids in postmenopausal women with noninsulin-dependent diabetes mellitus. J. Clin. Endocrinol. Metab. 1997, 82, 638–643. [Google Scholar] [CrossRef]
- Brussaard, H.E.; Gevers Leuven, J.A.; Frölich, M.; Kluft, C.; Krans, H.M. Short-term oestrogen replacement therapy improves insulin resistance, lipids and fibrinolysis in postmenopausal women with NIDDM. Diabetologia 1997, 40, 843–849. [Google Scholar] [CrossRef] [PubMed]
- Szekacs, B.; Vajo, Z.; Varbiro, S.; Kakucs, R.; Vaslaki, L.; Acs, N.; Mucsi, I.; Brinton, E.A. Postmenopausal hormone replacement improves proteinuria and impaired creatinine clearance in type 2 diabetes mellitus and hypertension. Br. J. Obstet. Gynaecol. 2000, 107, 1017–1021. [Google Scholar] [CrossRef]
- Maric, C.; Sullivan, S. Estrogens and the diabetic kidney. Gender Med. 2008, 5, S103–S113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mankhey, R.W.; Bhatti, F.; Maric, C. 17β-Estradiol replacement improves renal function and pathology associated with diabetic nephropathy. Am. J. Physiol. Renal Physiol. 2005, 288, F399–F405. [Google Scholar] [CrossRef] [Green Version]
- Chin, M.; Isono, M.; Isshiki, K.; Araki, S.; Sugimoto, T.; Guo, B.; Sato, H.; Haneda, M.; Kashiwagi, A.; Koya, D. Estrogen and raloxifene, a selective estrogen receptor modulator, ameliorate renal damage in db/db mice. Am. J. Pathol. 2005, 166, 1629–1636. [Google Scholar] [CrossRef] [Green Version]
- Hadjadj, S.; Gourdy, P.; Zaoui, P.; Guerci, B.; Roudaut, N.; Gautier, J.F.; Chabin, M.; Mauco, G.; Ragot, S.; RADIAN Study Group. Effect of raloxifene—A selective oestrogen receptor modulator—On kidney function in post-menopausal women with Type 2 diabetes: Results from a randomized, placebo-controlled pilot trial. Diabet Med. 2007, 24, 906–910. [Google Scholar] [CrossRef] [PubMed]
- Ramesh, S.; Mann, M.C.; Holroyd-Leduc, J.M.; Wilton, S.B.; James, M.T.; Seely, E.W.; Ahmed, S.B. Hormone therapy and clinical and surrogate cardiovascular endpoints in women with chronic kidney disease: A systematic review and meta-analysis. Menopause 2016, 23, 1028–1037. [Google Scholar] [CrossRef]
- Hu, X.; Liu, W.; Yan, Y.; Liu, H.; Huang, Q.; Xiao, Y.; Gong, Z.; Du, J. Vitamin D protects against diabetic nephropathy: Evidence-based effectiveness and mechanism. Eur. J. Pharmacol. 2019, 845, 91–98. [Google Scholar] [CrossRef]
- Cutolo, M.; Plebani, M.; Shoenfeld, Y.; Adorini, L.; Tincani, A. Vitamin D endocrine system and the immune response in rheumatic diseases. Vitam. Horm. 2011, 86, 327–351. [Google Scholar] [CrossRef]
- Gembillo, G.; Cernaro, V.; Siligato, R.; Curreri, F.; Catalano, A.; Santoro, D. Protective Role of Vitamin D in Renal Tubulopathies. Metabolites 2020, 10, 115. [Google Scholar] [CrossRef] [Green Version]
- Gembillo, G.; Siligato, R.; Amatruda, M.; Conti, G.; Santoro, D. Vitamin D and Glomerulonephritis. Medicina 2021, 57, 186. [Google Scholar] [CrossRef]
- Gembillo, G.; Cernaro, V.; Salvo, A.; Siligato, R.; Laudani, A.; Buemi, M.; Santoro, D. Role of Vitamin D Status in Diabetic Patients with Renal Disease. Medicina 2019, 55, 273. [Google Scholar] [CrossRef] [Green Version]
- Fondjo, L.A.; Sakyi, S.A.; Owiredu, W.K.B.A.; Laing, E.F.; Owiredu, E.W.; Awusi, E.K.; Ephraim, R.K.D.; Kantanka, O.S. Evaluating Vitamin D Status in Pre- and Postmenopausal Type 2 Diabetics and Its Association with Glucose Homeostasis. Biomed. Res. Int. 2018, 2018, 9369282. [Google Scholar] [CrossRef] [Green Version]
- Agmon-Levin, N.; Theodor, E.; Segal, R.M. Vitamin D in systemic and organ-specific autoimmune diseases. Clin. Rev. Allergy Immunol. 2013, 45, 256–266. [Google Scholar] [CrossRef]
- Cutolo, M.; Paolino, S.; Sulli, A.; Smith, V.; Pizzorni, C.; Seriolo, B. Vitamin D, steroid hormones, and autoimmunity. Ann. N. Y. Acad. Sci. 2014, 1317, 39–46. [Google Scholar] [CrossRef]
- Santoro, D.; Gembillo, G.; Andò, G. Glomerular Filtration Rate as a Predictor of Outcome in Acute Coronary Syndrome Complicated by Atrial Fibrillation. J. Clin. Med. 2020, 9, 1466. [Google Scholar] [CrossRef]
- Gangula, P.R.; Dong, Y.L.; Al-Hendy, A.; Richard-Davis, G.; Montgomery-Rice, V.; Haddad, G.; Millis, R.; Nicholas, S.B.; Moseberry, D. Protective cardiovascular and renal actions of vitamin D and estrogen. Front. Biosci. 2013, 5, 134–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meyer, M.R.; Clegg, D.J.; Prossnitz, E.R.; Barton, M. Obesity, insulin resistance and diabetes: Sex differences and role of oestrogen receptors. Acta Physiol. 2011, 203, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Dunlop, M. Aldose reductase and the role of the polyol pathway in diabetic nephropathy. Kidney Int. Suppl. 2000, 77, S3–S12. [Google Scholar] [CrossRef] [Green Version]
- Conti, G.; Caccamo, D.; Siligato, R.; Gembillo, G.; Satta, E.; Pazzano, D.; Carucci, N.; Carella, A.; Campo, G.D.; Salvo, A.; et al. Association of Higher Advanced Oxidation Protein Products (AOPPs) Levels in Patients with Diabetic and Hypertensive Nephropathy. Medicina 2019, 55, 675. [Google Scholar] [CrossRef] [Green Version]
- Semba, R.D.; Nicklett, E.; Ferrucci, L. Does accumulation of advanced glycation end products contribute to the aging phenotype? J. Gerontol. Ser. A Biomed. Sci. Med Sci. 2010, 65, 963–975. [Google Scholar] [CrossRef] [Green Version]
- Cai, W.; Ramdas, M.; Zhu, L.; Chen, X.; Striker, G.E.; Vlassara, H. Oral advanced glycation endproducts (AGEs) promote insulin resistance and diabetes by depleting the antioxidant defenses AGE receptor-1 and sirtuin 1. Proc. Natl. Acad. Sci. USA 2012, 109, 15888–15893. [Google Scholar] [CrossRef] [Green Version]
- Uribarri, J.; Cai, W.; Ramdas, M.; Goodman, S.; Pyzik, R.; Chen, X.; Zhu, L.; Striker, G.E.; Vlassara, H. Restriction of advanced glycation end products improves insulin resistance in human type 2 diabetes: Potential role of AGER1 and SIRT1. Diabetes Care 2011, 34, 1610–1616. [Google Scholar] [CrossRef] [Green Version]
- Elliot, S.J.; Karl, M.; Berho, M.; Xia, X.; Pereria-Simon, S.; Espinosa-Heidmann, D.; Striker, G.E. Smoking induces glomerulosclerosis in aging estrogen-deficient mice through cross-talk between TGF-beta1 and IGF-I signaling pathways. J. Am. Soc. Nephrol. 2006, 17, 3315–3324. [Google Scholar] [CrossRef] [Green Version]
- Blush, J.; Lei, J.; Ju, W.; Silbiger, S.; Pullman, J.; Neugarten, J. Estradiol reverses renal injury in Alb/TGF-beta1 transgenic mice. Kidney Int. 2004, 66, 2148–2154. [Google Scholar] [CrossRef] [Green Version]
- Gross, M.-L.; Adamczak, M.; Rabe, T.; Harbi, N.A.; Krtil, J.; Koch, A.; Ritz, E. Beneficial effects of estrogens on indices of renal damage in uninephrectomized SHRsp rats. J. Am. Soc. Nephrol. 2004, 15, 348–358. [Google Scholar] [CrossRef] [Green Version]
- Dean, S.A.; Tan, J.; O’Brien, E.R.; Leenen, F.H. 17beta-estradiol downregulates tissue angiotensin-converting enzyme and ANG II type 1 receptor in female rats. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2005, 288, R759–R766. [Google Scholar] [CrossRef]
- Negulescu, O.; Bognar, I.; Lei, J.; Devarajan, P.; Silbiger, S.; Neugarten, J. Estradiol reverses TGF-β1–induced mesangial cell apoptosis by a casein kinase 2-dependent mechanism. Kidney Int. 2002, 62, 1989–1998. [Google Scholar] [CrossRef] [Green Version]
- Xiao, S.; Gillespie, D.G.; Baylis, C.; Jackson, E.K.; Dubey, R.K. Effects of estradiol and its metabolites on glomerular endothelial nitric oxide synthesis and mesangial cell growth. Hypertension 2001, 37, 645–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pereira-Simon, S.; Rubio, G.A.; Xia, X.; Cai, W.; Choi, R.; Striker, G.E.; Elliot, S.J. Inhibition of Advanced Glycation End Products (AGEs) Accumulation by Pyridoxamine Modulates Glomerular and Mesangial Cell Estrogen Receptor α Expression in Aged Female Mice. PLoS ONE 2016, 11, e0159666. [Google Scholar] [CrossRef]
- Nakamura, T.; Miller, D.; Ruoslahti, E.; Border, W.A. Production of extracellular matrix by glomerular epithelial cells is regulated by transforming growth factor-beta 1. Kidney Int. 1992, 41, 1213–1221. [Google Scholar] [CrossRef] [Green Version]
- Miner, J.H. Renal basement membrane components. Kidney Int. 1999, 56, 2016–2024. [Google Scholar] [CrossRef] [Green Version]
- Patek, C.E.; Fleming, S.; Miles, C.G.; Bellamy, C.O.; Ladomery, M.; Spraggon, L.; Mullins, J.; Hastie, N.D.; Hooper, M.L. Murine Denys-Drash syndrome: Evidence of podocyte de-differentiation and systemic mediation of glomerulosclerosis. Hum. Mol. Genet. 2003, 12, 2379–2394. [Google Scholar] [CrossRef]
- Lee, H.S.; Song, C.Y. Differential role of mesangial cells and podocytes in TGF-ß-induced mesangial matrix synthesis in chronic glomerular disease. Histol. Histopathol. 2009, 24, 901–908. [Google Scholar] [CrossRef]
- Lee, H.S. Pathogenic role of TGF-ß in the progression of podocyte diseases. Histol. Histopathol. 2011, 26, 107–116. [Google Scholar] [CrossRef]
- Lin, Y.; Nakachi, K.; Ito, Y.; Kikuchi, S.; Tamakoshi, A.; Yagyu, K.; Watanabe, Y.; Inaba, Y.; Tajima, K.; Jacc Study Group. Variations in serum transforming growth factor-beta1 levels with gender, age and lifestyle factors of healthy Japanese adults. Dis. Markers 2009, 27, 23–28. [Google Scholar] [CrossRef]
- Ito, I.; Hanyu, A.; Wayama, M.; Goto, N.; Katsuno, Y.; Kawasaki, S.; Nakajima, Y.; Kajiro, M.; Komatsu, Y.; Fujimura, A.; et al. Estrogen inhibits transforming growth factor beta signaling by promoting Smad2/3 degradation. J. Biol. Chem. 2010, 285, 14747–14755. [Google Scholar] [CrossRef] [Green Version]
- Zdunek, M.; Silbiger, S.; Lei, J.; Neugarten, J. Protein kinase CK2 mediates TGF-β; 1-stimulated type IV collagen gene transcription and its reversal by estradiol. Kidney Int. 2001, 60, 2097–2108. [Google Scholar] [CrossRef] [Green Version]
- Ruggenenti, P.; Cravedi, P.; Remuzzi, G. The RAAS in the pathogenesis and treatment of diabetic nephropathy. Nat. Rev. Nephrol. 2010, 6, 319. [Google Scholar] [CrossRef]
- Yanes, L.L.; Sartori-Valinotti, J.C.; Reckelhoff, J.F. Sex steroids and renal disease: Lessons from animal studies. Hypertension 2008, 51, 976–981. [Google Scholar] [CrossRef]
- Bumke-Vogt, C.; Bähr, V.; Diederich, S.; Herrmann, S.M.; Anagnostopoulos, I.; Oelkers, W.; Quinkler, M. Expression of the progesterone receptor and progesterone- metabolising enzymes in the female and male human kidney. J. Endocrinol. 2002, 175, 349–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nielsen, C.B.; Flyvbjerg, A.; Bruun, J.M.; Forman, A.; Wogensen, L.; Thomsen, K. Decreases in renal functional reserve and proximal tubular fluid output in conscious oophorectomized rats: Normalization with sex hormone substitution. J. Am. Soc. Nephrol. 2003, 14, 3102–3110. [Google Scholar] [CrossRef] [Green Version]
- Sandhi, J.; Singh, J.P.; Kaur, T.; Ghuman, S.S.; Singh, A.P. Involvement of progesterone receptors in ascorbic acid-mediated protection against ischemia-reperfusion-induced acute kidney injury. J. Surg. Res. 2014, 187, 278–288. [Google Scholar] [CrossRef] [PubMed]
- Al-Trad, B.; Ashankyty, I.M.; Alaraj, M. Progesterone ameliorates diabetic nephropathy in streptozotocin-induced diabetic Rats. Diabetol. Metab. Syndr. 2015, 7, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kashtan, C. (2017). Alport syndrome: Facts and opinions. F1000Research 2017, 6, 50. [Google Scholar] [CrossRef]
- Temme, J.; Kramer, A.; Jager, K.J.; Lange, K.; Peters, F.; Müller, G.-A.; Kramar, R.; Heaf, J.G.; Finne, P.; Palsson, R.; et al. Outcomes of male patients with alport syndrome undergoing renal replacement therapy. Clin. J. Am. Soc. Nephrol. 2012, 7, 1969–1976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savige, J.; Colville, D.; Rheault, M.; Gear, S.; Lennon, R.; Lagas, S. Special feature alport syndrome in women and girls. Clin. J. Am. Soc. Nephrol. 2016, 11, 1713–1720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Seaghdha, C.M.; Fox, C.S. Genome-wide association studies of chronic kidney disease: What have we learned? Nat. Rev. Nephrol. 2011, 8, 89–99. [Google Scholar] [CrossRef] [Green Version]
- Regele, F.; Jelencsics, K.; Shiffman, D.; Paré, G.; McQueen, M.J.; Mann, J.F. Genome-wide studies to identify risk factors for kidney disease with a focus on patients with diabetes. Nephrol. Dial. Transplant. 2015, 30 (Suppl. S4), iv26–iv34. [Google Scholar] [CrossRef] [Green Version]
- Seaquist, E.R.; Goetz, F.C.; Rich, S.; Barbosa, J. Familial clustering of diabetic kidney disease. Evidence for genetic susceptibility to diabetic nephropathy. N. Engl. J. Med. 1989, 320, 1161–1165. [Google Scholar] [CrossRef]
- Quinn, M.; Angelico, M.C.; Warram, J.H.; Krolewski, A.S. Familial factors determine the development of diabetic nephropathy in patients with IDDM. Diabetologia 1996, 39, 940–945. [Google Scholar] [CrossRef]
- Vijay, V.; Snehalatha, C.; Shina, K.; Lalitha, S.; Ramachandran, A. Familial aggregation of diabetic kidney disease in Type 2 diabetes in south India. Diabetes Res. Clin. Pract. 1999, 43, 167–171. [Google Scholar] [CrossRef]
- Pettitt, D.J.; Saad, M.F.; Bennett, P.H.; Nelson, R.G.; Knowler, W.C. Familial predisposition to renal disease in two generations of Pima Indians with type 2 (noninsulin- dependent) diabetes mellitus. Diabetologia 1990, 33, 438–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freedman, B.I.; Spray, B.J.; Tuttle, A.B.; Buckalew, V.M., Jr. The familial risk of endstage renal disease in African Americans. Am. J. Kidney Dis. 1993, 21, 387–393. [Google Scholar] [CrossRef]
- Gu, H.F. Genetic and Epigenetic Studies in Diabetic Kidney Disease. Front. Genet. 2019, 10, 507. [Google Scholar] [CrossRef]
- Prudente, S.; Di Paola, R.; Copetti, M.; Lucchesi, D.; Lamacchia, O.; Pezzilli, S. The rs12917707 polymorphism at the UMOD locus and glomerular filtration rate in individuals with type 2 diabetes: Evidence of heterogeneity across two different European populations. Nephrol. Dial. Transplant. 2017, 32, 1718–1722. [Google Scholar] [CrossRef] [PubMed]
- Mooyaart, A.L.; Valk, E.J.J.; Van Es, L.A.; Bruijn, J.A.; De Heer, E.; Freedman, B.I.; Dekkers, O.M.; Baelde, H.J. Genetic associations in diabetic nephropathy: A meta-analysis. Diabetologia 2011, 54, 544–553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandholm, N.; Van Zuydam, N.; Ahlqvist, E.; Juliusdottir, T.; Deshmukh, H.A.; Rayner, N.W.; Di Camillo, B.; Forsblom, C.; Fadista, J.; Ziemek, D.; et al. The genetic landscape of renal complications in type 1 diabetes. J. Am. Soc. Nephrol. 2017, 28, 557–574. [Google Scholar] [CrossRef] [Green Version]
- Teumer, A.; Tin, A.; Sorice, R.; Gorski, M.; Yeo, N.C.; Chu, A.Y.; Li, M.; Li, Y.; Mijatovic, V.; Ko, Y.A.; et al. Genome-wide Association Studies Identify Genetic Loci Associated With Albuminuria in Diabetes. Diabetes 2016, 65, 803–817. [Google Scholar] [CrossRef] [Green Version]
- van Zuydam, N.R.; Ahlqvist, E.; Sandholm, N.; Deshmukh, H.; Rayner, N.W.; Abdalla, M.; Ladenvall, C.; Ziemek, D.; Fauman, E.; Robertson, N.R.; et al. A Genome-Wide Association Study of Diabetic Kidney Disease in Subjects With Type 2 Diabetes. Diabetes 2018, 67, 1414–1427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salem, R.M.; Todd, J.N.; Sandholm, N.; Cole, J.B.; Chen, W.-M.; Andrews, D.; Pezzolesi, M.G.; McKeigue, P.M.; Hiraki, L.T.; Qiu, C.; et al. Genome-Wide Association Study of Diabetic Kidney Disease Highlights Biology Involved in Glomerular Basement Membrane Collagen. J. Am. Soc. Nephrol. 2019, 30, 2000–2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mori, R.C.; Santos-Bezerra, D.P.; Pelaes, T.S.; Admoni, S.N.; Perez, R.V.; Monteiro, M.B.; Machado, C.G.; Queiroz, M.S.; Machado, U.F.; Correa-Giannella, M.L. Variants in HSD11B1 gene modulate susceptibility to diabetes kidney disease and to insulin resistance in type 1 diabetes. Diabetes Metab. Res. Rev. 2021, 37, e3352. [Google Scholar] [CrossRef]
- Kato, M.; Natarajan, R. Diabetic nephropathy–emerging epigenetic mechanisms. Nat. Rev. Nephrol. 2014, 10, 517–530. [Google Scholar] [CrossRef]
- Allis, C.D.; Jenuwein, T. The molecular hallmarks of epigenetic control. Nat. Rev. Genet. 2016, 17, 487–500. [Google Scholar] [CrossRef]
- Vujkovic, M.; Keaton, J.M.; Lynch, J.A.; Miller, D.R.; Zhou, J.; Tcheandjieu, C.; Huffman, J.E.; Assimes, T.L.; Lorenz, K.; Zhu, X.; et al. Discovery of 318 new risk loci for type 2 diabetes and related vascular outcomes among 1.4 million participants in a multi-ancestry meta-analysis. Nat. Genet. 2020, 52, 680–691. [Google Scholar] [CrossRef] [PubMed]
- Freire, M.B.; Ji, L.; Onuma, T.; Orban, T.; Warram, J.H.; Krolewski, A.S. Gender-specific association of M235T polymorphism in angiotensinogen gene and diabetic nephropathy in NIDDM. Hypertension 1998, 31, 896–899. [Google Scholar] [CrossRef] [Green Version]
- Lin, J.; Hu, F.B.; Qi, L.; Curhan, G.C. Genetic polymorphisms of angiotensin-2 type 1 receptor and angiotensinogen and risk of renal dysfunction and coronary heart disease in type 2 diabetes mellitus. BMC Nephrol. 2009, 10, 9. [Google Scholar] [CrossRef]
- Möllsten, A.; Vionnet, N.; Forsblom, C.; Parkkonen, M.; Tarnow, L.; Hadjadj, S.; Marre, M.; Parving, H.H.; Groop, P.H. A polymorphism in the angiotensin II type 1 receptor gene has different effects on the risk of diabetic nephropathy in men and women. Mol. Genet. Metab. 2011, 103, 66–70. [Google Scholar] [CrossRef] [PubMed]
- Ahluwalia, T.S.; Lindholm, E.; Groop, L.C. Common variants in CNDP1 and CNDP2, and risk of nephropathy in type 2 diabetes. Diabetologia 2011, 54, 2295–2302. [Google Scholar] [CrossRef] [Green Version]
- Alkhalaf, A.; Landman, G.W.; van Hateren, K.J.; Groenier, K.H.; Mooyaart, A.L.; De Heer, E.; Gans, R.O.; Navis, G.J.; Bakker, S.J.; Kleefstra, N.; et al. Sex specific association between carnosinase gene CNDP1 and cardiovascular mortality in patients with type 2 diabetes (ZODIAC-22). J Nephrol. 2015, 28, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Kurashige, M.; Imamura, M.; Araki, S.; Suzuki, D.; Babazono, T.; Uzu, T.; Umezono, T.; Toyoda, M.; Kawai, K.; Imanishi, M.; et al. The influence of a single nucleotide polymorphism within CNDP1 on susceptibility to diabetic nephropathy in Japanese women with type 2 diabetes. PLoS ONE 2013, 8, e54064. [Google Scholar] [CrossRef] [PubMed]
- Crook, E.D.; Genous, L.; Oliver, B. Angiotensin-converting enzyme genotype in blacks with diabetic nephropathy: Effects on risk of diabetes and its complications. J. Investig Med. 2003, 51, 360–365. [Google Scholar] [CrossRef]
- Sakka, Y.; Babazono, T.; Sato, A.; Ujihara, N.; Iwamoto, Y. ACE gene polymorphism, left ventricular geometry, and mortality in diabetic patients with end-stage renal disease. Diabetes Res. Clin. Pract. 2004, 64, 41–49. [Google Scholar] [CrossRef]
- Tien, K.J.; Hsiao, J.Y.; Hsu, S.C.; Liang, H.T.; Lin, S.R.; Chen, H.C.; Hsieh, M.C. Gender-dependent effect of ACE I/D and AGT M235T polymorphisms on the progression of urinary albumin excretion in Taiwanese with type 2 diabetes. Am. J. Nephrol. 2009, 29, 299–308. [Google Scholar] [CrossRef]
- Zambrano-Galván, G.; Reyes-Romero, M.A.; Lazalde, B.; Rodríguez-Morán, M.; Guerrero-Romero, F. Risk of microalbuminuria in relatives of subjects with diabetic nephropathy: A predictive model based on multivariable dimensionality reduction approach. Clin. Nephrol. 2015, 83, 86–92. [Google Scholar] [CrossRef]
- Gu, H.F.; Alvarsson, A.; Efendic, S.; Brismar, K. SOX2 has gender-specific genetic effects on diabetic nephropathy in samples from patients with type 1 diabetes mellitus in the GoKinD study. Gend Med. 2009, 6, 555–564. [Google Scholar] [CrossRef]
- Monteiro, M.B.; Patente, T.A.; Mohammedi, K.; Queiroz, M.S.; Azevedo, M.J.; Canani, L.H.; Parisi, M.C.; Marre, M.; Velho, G.; Corrêa-Giannella, M.L. Sex-specific associations of variants in regulatory regions of NADPH oxidase-2 (CYBB) and glutathione peroxidase 4 (GPX4) genes with kidney disease in type 1 diabetes. Free Radic. Res. 2013, 47, 804–810. [Google Scholar] [CrossRef]
- Mlynarski, W.M.; Placha, G.P.; Wolkow, P.P.; Bochenski, J.P.; Warram, J.H.; Krolewski, A.S. Risk of diabetic nephropathy in type 1 diabetes is associated with functional polymorphisms in RANTES receptor gene (CCR5): A sex-specific effect. Diabetes. 2005, 54, 3331–3335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandholm, N.; McKnight, A.J.; Salem, R.M.; Brennan, E.P.; Forsblom, C.; Harjutsalo, V.; Mäkinen, V.P.; McKay, G.J.; Sadlier, D.M.; Williams, W.W.; et al. Chromosome 2q31.1 associates with ESRD in women with type 1 diabetes. J. Am. Soc. Nephrol. 2013, 24, 1537–1543. [Google Scholar] [CrossRef] [Green Version]
- Gu, T.; Horová, E.; Möllsten, A.; Seman, N.A.; Falhammar, H.; Prázný, M.; Brismar, K.; Gu, H.F. IGF2BP2 and IGF2 genetic effects in diabetes and diabetic nephropathy. J. Diabetes Complicat. 2012, 26, 393–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mantovani, A.; Zusi, C.; Sani, E.; Colecchia, A.; Lippi, G.; Zaza, G.L.; Valenti, L.; Byrne, C.D.; Maffeis, C.; Bonora, E.; et al. Association between PNPLA3rs738409 polymorphism decreased kidney function in postmenopausal type 2 diabetic women with or without non-alcoholic fatty liver disease. Diabetes Metab. 2019, 45, 480–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russo, G.T.; Giandalia, A.; Romeo, E.L.; Muscianisi, M.; Ruffo, M.C.; Alibrandi, A.; Bitto, A.; Forte, F.; Grillone, A.; Asztalos, B.; et al. HDL subclasses and the common CETP TaqIB variant predict the incidence of microangiopatic complications in type 2 diabetic women: A 9years follow-up study. Diabetes Res. Clin. Pract. 2017, 132, 108–117. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.-C.; Chen, S.-Y.; Liu, S.-P.; Lin, J.-M.; Lin, H.-J.; Lei, Y.-J.; Chung, Y.-C.; Chen, Y.-C.; Wang, Y.-H.; Liao, W.-L.; et al. Cholesteryl Ester Transfer Protein Genetic Variants Associated with Risk for Type 2 Diabetes and Diabetic Kidney Disease in Taiwanese Population Genes. Genes (Basel) 2019, 10, 782. [Google Scholar] [CrossRef] [Green Version]
- Bartáková, V.; Kuricová, K.; Pácal, L.; Nová, Z.; Dvořáková, V.; Švrčková, M.; Malúšková, D.; Svobodová, I.; Řehořová, J.; Svojanovský, J.; et al. Hyperuricemia contributes to the faster progression of diabetic kidney disease in type 2 diabetes mellitus. J. Diabetes Complicat. 2016, 30, 1300–1307. [Google Scholar] [CrossRef]
- Fox, C.S.; Matsushita, K.; Woodward, M.; Bilo, H.J.; Chalmers, J.; Heerspink, H.J.; Lee, B.J.; Perkins, R.M.; Rossing, P.; Sairenchi, T.; et al. Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and without diabetes: A meta-analysis. Lancet 2012, 380, 1662–1673. [Google Scholar] [CrossRef] [Green Version]
- Huxley, R.; Barzi, F. Woodward. Excess risk of fatal coronary heart disease associated with diabetes in men and women: Meta-analysis of 37 prospective cohort studies. BMJ 2006, Russo GT, Baggio G, Rossi MC, Kautzky-Willer, A. Type 2diabetes and cardiovascular risk in women. Int. J. Endocrinol. 2015, 2015, 832484. [Google Scholar] [CrossRef]
- Huebschmann, A.G.; Huxley, R.R.; Kohrt, W.M.; Zeitler, P.; Regensteiner, J.G.; Reusch, J.E.B. Sex differences in the burden of type 2 diabetes and cardiovascular risk across the life course. Diabetologia 2019, 62, 1761–1772. [Google Scholar] [CrossRef] [Green Version]
- Ballotari, P.; Ranieri, S.C.; Luberto, F.; Caroli, S.; Greci, M.; Rossi, P.G.; Manicardi, V. Sex differences in cardiovascular mortality in diabetics and nondiabetic subjects: A population-based study (Italy). Int. J. Endocrinol. 2015, 2015, 914057. [Google Scholar] [CrossRef] [PubMed]
- Rospective Studies Collaboration and Asia Pacific Cohort Studies Collaboration. Sex-specific relevance of diabetes to occlusive vascular and other mortality: A collaborative meta-analysis of individual data from 980 793 adults from 68 prospective studies. Lancet Diabetes Endocrinol. 2018, 6, 538–546. [Google Scholar] [CrossRef]
- Kalyani, R.R.; Lazo, M.; Ouyang, P.; Turkbey, E.; Chevalier, K.; Brancati, F.; Becker, D.; Vaidya, D. Sex differences in diabetes and risk of incident coronary artery disease in healthy young and middle-aged adults. Diabetes Care 2014, 37, 830–838. [Google Scholar] [CrossRef] [Green Version]
- Millett, E.R.C.; Peters, S.A.E.; Woodward, M. Sex differences in risk factors for myocardial infarction: Cohort study of UK Biobank participants. BMJ 2018, 363, k4247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wright, A.K.; Kontopantelis, E.; Emsley, R.; Buchan, I.; Mamas, M.A.; Sattar, N.; Ashcroft, D.; Rutter, M.K. Cardiovascular risk and risk factormanagement in type 2 diabetes:a population-based cohort study assessing sex disparities. Circulation 2019, 139, 2742–2753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avogaro, A.; Giorda, C.; Maggini, M.; Mannucci, E.; Raschetti, R.; Lombardo, F.; Spila-Alegiani, S.; Turco, S.; Velussi, M.; Ferrannini, E. Incidence of coronary heart disease in type 2 diabetic men and women: Impact of microvascular complications, treatment, and geographic location. Diabetes Care 2007, 30, 1241–1247. [Google Scholar] [CrossRef] [Green Version]
- Ferrara, A.; Mangione, C.M.; Kim, C.; Marrero, D.G.; Curb, D.; Stevens, M.; Selby, J.V.; Translating Research Into Action for Diabetes Study Group. Sex disparities in control and treatment of modifiable cardiovascular disease risk factors among patients with diabetes: Translating Research Into Action for Diabetes (TRIAD) Study. Diabetes Care 2008, 31, 69–74. [Google Scholar] [CrossRef] [Green Version]
- Russo, G.; Pintaudi, B.; Giorda, C.; Lucisano, G.; Nicolucci, A.; Cristofaro, M.R.; Suraci, C.; Mulas, M.F.; Napoli, A.; Rossi, M.C.; et al. Age- and Gender-Related Differences in LDL-Cholesterol Management in Outpatients with Type 2 Diabetes Mellitus. Int. J. Endocrinol. 2015, 2015, 957105. [Google Scholar] [CrossRef]
- Russo, G.; Piscitelli, P.; Giandalia, A.; Viazzi, F.; Pontremoli, R.; Fioretto, P.; De Cosmo, S. Atherogenic dyslipidemia and diabetic nephropathy. J. Nephrol. 2020, 33, 1001–1008. [Google Scholar] [CrossRef]
- Russo, G.T.; De Cosmo, S.; Viazzi, F.; Pacilli, A.; Ceriello, A.; Genovese, S.; Guida, P.; Giorda, C.; Cucinotta, D.; Pontremoli, R.; et al. Plasma Triglycerides and HDL-C Levels Predict the Development of Diabetic Kidney Disease in Subjects With Type 2 Diabetes: The AMD Annals Initiative. Diabetes Care 2016, 39, 2278–2287. [Google Scholar] [CrossRef] [Green Version]
- Hanai, K.; Babazono, T.; Yoshida, N.; Nyumura, I.; Toya, K.; Hayashi, T.; Bouchi, R.; Tanaka, N.; Ishii, A.; Iwamoto, Y. Gender differences in the association between HDL cholesterol and the progression of diabetic kidney disease in type 2 diabetic patients. Nephrol. Dial. Transplant. 2012, 27, 1070–1075. [Google Scholar] [CrossRef] [Green Version]
- Wan, H.; Wang, Y.; Chen, Y.; Fang, S.; Zhang, W.; Xia, F.; Wang, N.; Lu, Y. Different associations between serum urate and diabetic complications in men and postmenopausal women. Diabetes Res. Clin. Pract. 2020, 160, 108005. [Google Scholar] [CrossRef] [PubMed]
- Pisano, A.; Cernaro, V.; Gembillo, G.; D’Arrigo, G.; Buemi, M.; Bolignano, D. Xanthine Oxidase Inhibitors for Improving Renal Function in Chronic Kidney Disease Patients: An Updated Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2017, 18, 2283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Cosmo, S.; Viazzi, F.; Pacilli, A.; Giorda, C.; Ceriello, A.; Gentile, S.; Russo, G.; Rossi, M.C.; Nicolucci, A.; Guida, P.; et al. (2015). Serum Uric Acid and Risk of CKD in Type 2 Diabetes. Clin. J. Am. Soc. Nephrol. CJASN 2015, 10, 1921–1929. [Google Scholar] [CrossRef] [PubMed]
- Guo, M.; Niu, J.Y.; Li, S.R.; Ye, X.W.; Fang, H.; Zhao, Y.P.; Gu, Y. Gender differences in the association between hyperuricemia and diabetic kidney disease in community elderly patients. J. Diabetes Complicat. 2015, 29, 1042–1049. [Google Scholar] [CrossRef]
- Chung, W.K.; Erion, K.; Florez, J.C.; Hattersley, A.T.; Hivert, M.F.; Lee, C.G.; McCarthy, M.I.; Nolan, J.J.; Norris, J.M.; Pearson, E.R.; et al. Precision Medicine in Diabetes: A Consensus Report From the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2020, 43, 1617–1635. [Google Scholar] [CrossRef]
- Kautzky-Willer, A.; Harreiter, J.; Pacini, G. Sex and Gender Differences in Risk, Pathophysiology and Complications of Type 2 Diabetes Mellitus. Endocr. Rev. 2016, 37, 278–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ueda, P.; Svanström, H.; Melbye, M.; Eliasson, B.; Svensson, A.M.; Franzén, S.; Gudbjörnsdottir, S.; Hveem, K.; Jonasson, C.; Pasternak, B. Sodium glucose cotransporter 2 inhibitors and risk of serious adverse events: Nationwide register based cohort study. BMJ 2018, 363, k4365. [Google Scholar] [CrossRef] [Green Version]
- Pasternak, B.; Wintzell, V.; Melbye, M.; Eliasson, B.; Svensson, A.M.; Franzén, S.; Gudbjörnsdottir, S.; Hveem, K.; Jonasson, C.; Svanström, H.; et al. Use of sodium-glucose co-transporter 2 inhibitors and risk of serious renal events: Scandinavian cohort study. BMJ 2020, 369, m1186. [Google Scholar] [CrossRef] [PubMed]
- Zinman, B.; Wanner, C.; Lachin, J.M.; Fitchett, D.; Bluhmki, E.; Hantel, S.; Mattheus, M.; Devins, T.; Johansen, O.E.; Woerle, H.J.; et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N. Engl. J. Med. 2015, 373, 2117–2128. [Google Scholar] [CrossRef]
- Perkovic, V.; Jardine, M.J.; Neal, B.; Bompoint, S.; Heerspink, H.J.L.; Charytan, D.M.; Edwards, R.; Agarwal, R.; Bakris, G.; Bull, S.; et al. Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy. N. Engl. J. Med. 2019, 380, 2295–2306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heerspink, H.J.L.; Stefánsson, B.V.; Correa-Rotter, R.; Chertow, G.M.; Greene, T.; Hou, F.F.; Mann, J.F.E.; McMurray, J.J.V.; Lindberg, M.; Rossing, P.; et al. Dapagliflozin in Patients with Chronic Kidney Disease. N. Engl. J. Med. 2020, 383, 1436–1446. [Google Scholar] [CrossRef] [PubMed]
- Carrero, J.J.; de Mutsert, R.; Axelsson, J.; Dekkers, O.M.; Jager, K.J.; Boeschoten, E.W.; Krediet, R.T.; Dekker, F.W.; NECOSAD Study Group. Sex differences in the impact of diabetes on mortality in chronic dialysis patients. Nephrol. Dial. Transplant. 2011, 26, 270–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Reference | Ethnic Group | Study Design | Sex Specific Association | MAU | Low eGFR | ESRD |
|---|---|---|---|---|---|---|
| Studies on T2DM subjects | ||||||
| Gall, 1997 [20] | Denmark | Prospective | Male | Higher risk | NR | NR |
| Lewis J, 2001 [21] | Multi-ethnic | Intervention study | Female | Higher risk | NR | NR |
| Keane WF, 2003 [22] | Multi-ethnic | Intervention study | Female | Higher risk | Higher risk | Higher risk |
| Rossing K, 2004 [23] | Denmark | Prospective | Both sexes | NR | Higher risk | Higher risk |
| Retkaran, 2006 [24] | UK | Prospective | Male/Female | Higher risk male | Higher risk female | NR |
| Penno, 2011 [25] | Italy | Cross-sectional | Male/Female | Higher risk male | Higher risk female | NR |
| Yu M, 2012 [26] | USA | Cross-sectional | Male/Female | Higher risk male | Higher risk male | Higher risk female |
| Jardine, 2012 [27] | UK | Intervention study | Male | NR | NR | Higher risk |
| Zoppini, 2012 [28] | Italy | Prospective | Both sexes | NR | Higher risk | NR |
| Altemtan,2012 [29] | UK | Retrospective | Both sexes | NR | Higher risk | NR |
| Elley, 2013 [30] | New Zealand | Nationwide cohort | Female | NR | NR | Higher risk |
| de Hautecloque 2014 [31] | France | Prospective | Male | NR | Higher risk | Higher risk |
| Kaiwara 2016 [32] | Japan | Prospective | Female | NR | Higher risk | NR |
| Studies on T1DM subjects | ||||||
| Orchard, 1990 [33] | US | Prospective | Male | Higher risk | NR | NR |
| Lovshin, 1990 [34] | US | Cross-sectional | Male | Higher risk | NR | NR |
| Holl, 1999 [35] | Germany | Retrospective | Female | Higher risk | NR | NR |
| Jacobsen, 1999 [36] | Denmark | Prospective | Male | NR | Higher risk | NR |
| Rossing, 2002 [37] | Denmark | Prospective | Both sexes | Higher risk | NR | NR |
| Zhang, 2003 [38] | US | Prospective | Male | Higher risk | NR | NR |
| Hovind, 2004 [39] | Denmark | Prospective | Male | Higher risk | NR | NR |
| Finne, 2005 [40] | Finland | Register | Male | NR | NR | Higher risk |
| Sibley, 2006 [41] | US | Prospective | Male | Higher risk | NR | NR |
| RAile, 2007 [42] | Germany | Prospective | Male | Higher risk | NR | NR |
| Monti, 2007 [43] | US | Cross-sectional | Both sexes | Higher risk | Higher risk | NR |
| Mollsten, 2010 [44] | Sweden | Population | Male | NR | NR | Higher risk |
| Costacou, 2011 [45] | US | Prospective | Male 1950-1964 | Higher risk | NR | Higher risk |
| Costacou, 2011 [45] | US | Prospective | Female1965-1980 | Higher risk | NR | Higher risk |
| Harjutsalo, 2011 [46] | Finland | Prospective | Male | NR | NR | Higher risk |
| Kautzy-Willer 2013 [47] | Austria | Cross-sectional | both sexes | Higher risk | Higher risk | NR |
| Skupien, 2019 [48] | Multi-ethnic | Prospective | Male | NR | NR | Higher risk |
| Studies including T1DM/T2DM subjects | ||||||
| Dick, 1994 [49] | Canada | Prospective | Female | NR | NR | Higher risk |
| Xue, 2007 [51] | USA | Prospective | Female | NR | NR | Higher risk |
| Yamagotha, 2007 [52] | Japan | Prospective | Male | Higher risk | Both sexes | NR |
| Hippsley-Cox,2010 [53] | UK | Registrative data | Female | NR | Both sexes | Higher risk |
| Hoffman F, 2011 [54] | Germany | Claims data | Female | NR | NR | Higher risk |
| Johnson, 2011 [55] | USA | Retrospective | Male | NR | NR | Higher risk |
| Tohidi, 2012 [56] | Iran | Prospective | Female | NR | Higher risk | NR |
| Kei, 2013 [57] | Japan | Prospective | Both sexes | Higher risk | NR | NR |
| van Blijderveen, 2014 [58] | Netherlands | Retrospective | Male/Female | Higher risk Male | Both sexes | Higher risk Female |
| Haroun, 2003 [50] | USA | Prospective | Female | NR | NR | Higher risk F |
| Ricardo,2018 [13] | USA | Prospective | Male | Higher risk Male | Both sexes | Higher risk Male |
| T1DM | |||
| Prevalence | Incidence 5 years | 4 years Progression eGFR<60 mL/min or >30% reduction | |
| Male Sex | DKD 1.01 (0.91–1.11) p = 0.901 Low eGFR 0.64 (0.55–0.74) p < 0.001 MAU 1.26 (1.14–1.40) p < 0.001 | DKD 1.01 (0.81–1.27) p = 0.913 Low eGFR 0.96 (0.59–1.56) p = 0.873 MAU 1.04 (0.82–1.32) p = 0.760 | 0.59 (0.46–0.76) p < 0.001 |
| Age | By 10 year DKD 1.15 (1.10–1.19) p < 0.001 Low eGFR 1.85 (1.74–1.96) p < 0.001 MAU 0.93 (0.89–0.87) p < 0.001 | By 10 year DKD 1.07 (0.96–1.18) p = 0.203 Low eGFR 1.95 (1.57–2.43) p < 0.001 MAU 0.93 (0.84–1.04) p = 0.227 | By 10 year 1.46 (1.30–1.63) p < 0.001 |
| T2DM | |||
| Prevalence | Incidence 5 years | 4 years Progression eGFR <60 mL/min or >30% reduction | |
| Male Sex | Low eGFR 0.69 (0.64–0.73) MAU 1.89 (1.81–1.98) Both 1.52 (1.42–1.63) | Low eGFR 1.373 (1.326–1.422) p < 0.001 MAU 1.075 (1.033–1.118) p < 0.001 Both 1.381 (1.306–1.460) p < 0.001 | In subjects with DM and hypertension 0.78 (0.72–0.86) p < 0.001 |
| Age | By 1 year Low eGFR 1.12 (1.11–1.12) MAU 1.01 (1.01–1.01) Both 1.12 (1.12–1.13) | By 10 year Low eGFR 0.767 (0.681–0.864) p < 0.001 MAU 1.355 (1.220–1.504) p < 0.001 Both 1.090 (0.926–1.283) p = 0.30 | By 10 year 1.49 (1.41–1.58) p < 0.001 |
| Reference | Ethnic Group | Locus | Study Design | Sex Specific Association * | MAU | Low eGFR | DKD |
|---|---|---|---|---|---|---|---|
| Studies on T2DM subjects | |||||||
| Lin, 2009 [191] | US | AGT1R (1166) | cohort study | Male/Female | Not significant | Higher risk | Higher risk |
| Tien, 2009 [198] | Taiwan | ACE D/I | Prospective | Female | Higher risk | Higher risk | Higher risk |
| Mooyaart, 2011 [181] | Multi-ethnic | 24 gene variants: ACE, AKR1B1 (two variants), APOC1, APOE, EPO,NOS3 (two variants), HSPG2, VEGFA, FRMD3 (two variants), CARS (two variants), UNC13B, CPVL and CHN2, and GREM1, plus 3 variants not near genes. | GWAS | NR | Higher risk | Higher risk | Higher risk |
| Ahluwalia, 2011 [193] | Sweden | CNDP1 (rs2346061) | Case–control | Male/Female | Higher risk | Not significant | Higher risk |
| Ahluwalia, 2011 [193] | Sweden | CNDP2 (rs7577) | Case–control | Female | Higher risk | Not significant | Higher risk |
| Kurashige, 2013 [195] | Japan | CNDP1 (rs12604675) | Case–control | Female | Higher risk | Not significant | Higher risk |
| Alkhalaf, 2015 [194] | Netherlands | CNDP1 (5L-5L) | prospective | Male/Female | Not significant | Not significant | Not significant |
| Teumer, 2015 [183] | European | RAB38/CTSC (rs649529), HS6ST1 (rs13427836), CUBN (rs10795433) | GWAS | NR | NR | NR | NR |
| Prudente, 2017 [180] | Italy | UMOD (rs12917707) | Cross-sectional | NR | NR | NR | NR |
| Russo, 2017 [206] | Italy | CETP Taq1B | cohort | Female | Not significant | Not significant | Not significant |
| van Zuydam, 2018 [184] | European | GABRR1 (rs9942471) | GWAS | NR | Higher risk | Not significant | Higher risk |
| Huang, 2019 [207] | Taiwan | CETP rs1800775 | Cross-sectional | NR | Higher risk | Higher risk | Higher risk |
| Mantovani, 2019 [205] | Italy | PNPLA3 rs738409 | Cross-sectional | Female | NR | Higher risk | Higher risk |
| Vujkovic, 2020 [189] | Multi-ethnic | UMOD | GWAS | Not significant | Not significant | Higher risk | Higher risk |
| Studies on T1DM subjects | |||||||
| Freire, 1998 [190] | US | AGT (M235T) | case–control | Male | Higher risk | Not significant | Higher risk |
| Miynarski, 2005 [202] | US | CCR5 (A59029G) | Case–control | Male | Higher risk | Higher risk | Higher risk |
| Miynarski, 2005 [202] | US | CCR5 (32bp deletion) | Case–control | Male | Higher risk | Higher risk | Higher risk |
| Mollsten, 2011 [192] | Denmark, Finland, France and Sweden | AGTR1 (rs5186) | case–control | Male | Higher risk | Not significant | Higher risk |
| Gu/Horova, 2012 [204] | European | IGF2 (rs10770125) | Case–control | Male | Higher risk | Higher risk | Higher risk |
| Gu/Horova, 2012 [204] | European | IGF2BP2(rs4402960) | Case–control | Male | Higher risk | Higher risk | Higher risk |
| Montero, 2013 [201] | Brazil/France/Belgium | CYBB (rs6610650) | Cross-sectional | Female | Higher risk | Higher risk | Higher risk |
| Montero, 2013 [201] | Brazil/France/Belgium | GPX4 (rs713041) | Cross -sectional | Male | Higher risk | Higher risk | Higher risk |
| Saldholm, 2013 [203] | Finland | Chr2q31.1 (rs4972593) | GWAS | Female | NR | Higher risk | Higher risk |
| Sanholm, 2017 [182] | European | AFF3, CNTNAP2, NRG3, and PTPN13, ELMO1, 13q, and SIK1 | GWAS | NR | Higher risk | Higher risk | Higher risk |
| Gu, 2019 [200] | Sweden | SOX2 (rs11915160) | Case–control | Female | Higher risk | Higher risk | Higher risk |
| Salem, 2019 [185] | European | COL4A3 (rs55703767) | GWAS | Male | Higher risk | Higher risk | Higher risk |
| Mori, 2020 [186] | Brazil | HSD11B1 (rs17389016) | cohort | NR | Not significant | Higher risk | Higher risk |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giandalia, A.; Giuffrida, A.E.; Gembillo, G.; Cucinotta, D.; Squadrito, G.; Santoro, D.; Russo, G.T. Gender Differences in Diabetic Kidney Disease: Focus on Hormonal, Genetic and Clinical Factors. Int. J. Mol. Sci. 2021, 22, 5808. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22115808
Giandalia A, Giuffrida AE, Gembillo G, Cucinotta D, Squadrito G, Santoro D, Russo GT. Gender Differences in Diabetic Kidney Disease: Focus on Hormonal, Genetic and Clinical Factors. International Journal of Molecular Sciences. 2021; 22(11):5808. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22115808
Chicago/Turabian StyleGiandalia, Annalisa, Alfio Edoardo Giuffrida, Guido Gembillo, Domenico Cucinotta, Giovanni Squadrito, Domenico Santoro, and Giuseppina T. Russo. 2021. "Gender Differences in Diabetic Kidney Disease: Focus on Hormonal, Genetic and Clinical Factors" International Journal of Molecular Sciences 22, no. 11: 5808. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22115808