
Myositis/Myasthenia after Pembrolizumab in a Bladder Cancer Patient with an Autoimmunity-Associated HLA: Immune–Biological Evaluation and Case Report

 , , and
, , and
Abstract
:1. Introduction
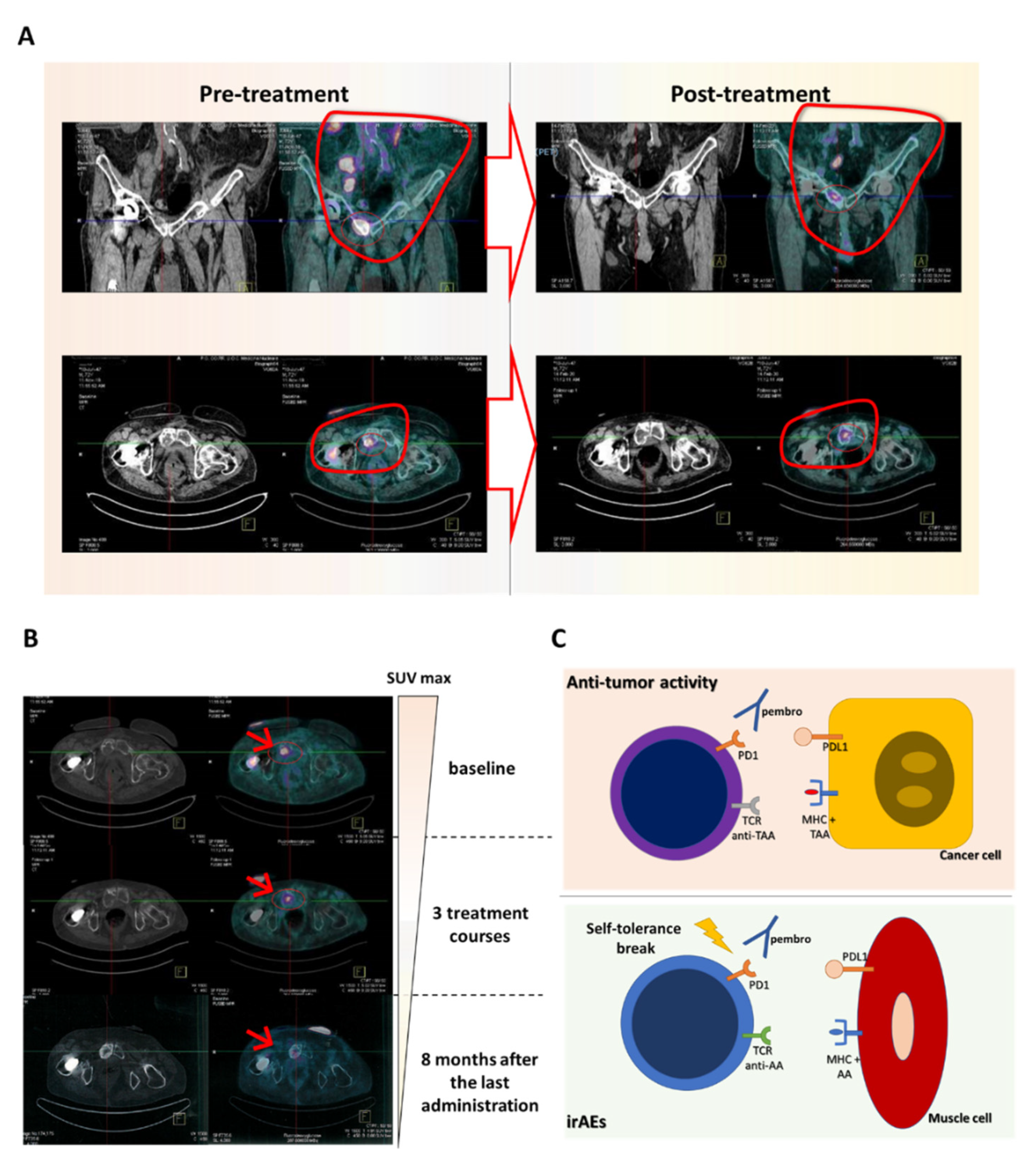
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pardoll, D.M. The blockade of immune checkpoints in cancer immunotherapy. Nat. Rev. Cancer 2012, 12, 252–264. [Google Scholar] [CrossRef] [Green Version]
- Xia, L.; Liu, Y.; Wang, Y. PD-1/PD-L1 Blockade Therapy in Advanced Non-Small-Cell Lung Cancer: Current Status and Future Directions. Oncologist 2019, 24, S31–S41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, F.; Liu, Z.; Liang, J.; Zhang, F.; Wu, K.; Zhou, C.; Lu, Y.; Wang, X. The efficacy and safety of immunotherapy targeting the PD-1 pathway for advanced urothelial carcinoma: A meta-analysis of published clinical trials. Clin. Transl. Oncol. 2020. [CrossRef]
- Day, D.; Hansen, A.R. Immune-Related Adverse Events Associated with Immune Checkpoint Inhibitors. BioDrugs 2016, 30, 571–584. [Google Scholar] [CrossRef] [PubMed]
- Correale, P.; Tagliaferri, P.; Fioravanti, A.; Del Vecchio, M.T.; Remondo, C.; Montagnani, F.; Rotundo, M.S.; Ginanneschi, C.; Martellucci, I.; Francini, E.; et al. Immunity feedback and clinical outcome in colon cancer patients undergoing chemoimmunotherapy with gemcitabine + FOLFOX followed by subcutaneous granulocyte macrophage colony-stimulating factor and aldesleukin (GOLFIG-1 Trial). Clin. Cancer Res. 2008, 14, 4192–4199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giannicola, R.; D’Arrigo, G.; Botta, C.; Agostino, R.; Del Medico, P.; Falzea, A.C.; Barbieri, V.; Staropoli, N.; Del Giudice, T.; Pastina, P.; et al. Early blood rise in auto-antibodies to nuclear and smooth muscle antigens is predictive of prolonged survival and autoimmunity in metastatic-non-small cell lung cancer patients treated with PD-1 immune-check point blockade by nivolumab. Mol. Clin. Oncol. 2019, 11, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Leonardi, G.C.; Candido, S.; Falzone, L.; Spandidos, D.A.; Libra, M. Cutaneous melanoma and the immunotherapy revolution (Review). Int. J. Oncol. 2020, 57, 609–618. [Google Scholar] [CrossRef]
- Rodriguez-Cerdeira, C.; Carnero Gregorio, M.; Lopez-Barcenas, A.; Sanchez-Blanco, E.; Sanchez-Blanco, B.; Fabbrocini, G.; Bardhi, B.; Sinani, A.; Guzman, R.A. Advances in Immunotherapy for Melanoma: A Comprehensive Review. Mediat. Inflamm. 2017, 2017, 3264217. [Google Scholar] [CrossRef] [Green Version]
- Maher, V.E.; Fernandes, L.L.; Weinstock, C.; Tang, S.; Agarwal, S.; Brave, M.; Ning, Y.M.; Singh, H.; Suzman, D.; Xu, J.; et al. Analysis of the Association Between Adverse Events and Outcome in Patients Receiving a Programmed Death Protein 1 or Programmed Death Ligand 1 Antibody. J. Clin. Oncol. 2019, 37, 2730–2737. [Google Scholar] [CrossRef]
- Mohn, N.; Beutel, G.; Gutzmer, R.; Ivanyi, P.; Satzger, I.; Skripuletz, T. Neurological Immune Related Adverse Events Associated with Nivolumab, Ipilimumab, and Pembrolizumab Therapy-Review of the Literature and Future Outlook. J. Clin. Med. 2019, 8, 1777. [Google Scholar] [CrossRef] [Green Version]
- Mohn, N.; Suhs, K.W.; Gingele, S.; Angela, Y.; Stangel, M.; Gutzmer, R.; Satzger, I.; Skripuletz, T. Acute progressive neuropathy-myositis-myasthenia-like syndrome associated with immune-checkpoint inhibitor therapy in patients with metastatic melanoma. Melanoma Res. 2019, 29, 435–440. [Google Scholar] [CrossRef]
- Cuzzubbo, S.; Javeri, F.; Tissier, M.; Roumi, A.; Barlog, C.; Doridam, J.; Lebbe, C.; Belin, C.; Ursu, R.; Carpentier, A.F. Neurological adverse events associated with immune checkpoint inhibitors: Review of the literature. Eur. J. Cancer 2017, 73, 1–8. [Google Scholar] [CrossRef]
- Wang, D.Y.; Salem, J.E.; Cohen, J.V.; Chandra, S.; Menzer, C.; Ye, F.; Zhao, S.; Das, S.; Beckermann, K.E.; Ha, L.; et al. Fatal Toxic Effects Associated With Immune Checkpoint Inhibitors: A Systematic Review and Meta-analysis. JAMA Oncol. 2018, 4, 1721–1728. [Google Scholar] [CrossRef] [Green Version]
- Correale, P.; Botta, C.; Martino, E.C.; Ulivieri, C.; Battaglia, G.; Carfagno, T.; Rossetti, M.G.; Fioravanti, A.; Guidelli, G.M.; Cheleschi, S.; et al. Phase Ib study of poly-epitope peptide vaccination to thymidylate synthase (TSPP) and GOLFIG chemo-immunotherapy for treatment of metastatic colorectal cancer patients. Oncoimmunology 2016, 5, e1101205. [Google Scholar] [CrossRef] [Green Version]
- Correale, P.; Saladino, R.E.; Giannarelli, D.; Sergi, A.; Mazzei, M.A.; Bianco, G.; Giannicola, R.; Iuliano, E.; Forte, I.M.; Calandruccio, N.D.; et al. HLA Expression Correlates to the Risk of Immune Checkpoint Inhibitor-Induced Pneumonitis. Cells 2020, 9, 1964. [Google Scholar] [CrossRef]
- Cusi, M.G.; Botta, C.; Pastina, P.; Rossetti, M.G.; Dreassi, E.; Guidelli, G.M.; Fioravanti, A.; Martino, E.C.; Gandolfo, C.; Pagliuchi, M.; et al. Phase I trial of thymidylate synthase poly-epitope peptide (TSPP) vaccine in advanced cancer patients. Cancer Immunol. Immunother. 2015, 64, 1159–1173. [Google Scholar] [CrossRef]
- Nardone, V.; Pastina, P.; Giannicola, R.; Agostino, R.; Croci, S.; Tini, P.; Pirtoli, L.; Giordano, A.; Tagliaferri, P.; Correale, P. How to Increase the Efficacy of Immunotherapy in NSCLC and HNSCC: Role of Radiation Therapy, Chemotherapy, and Other Strategies. Front. Immunol. 2018, 9, 2941. [Google Scholar] [CrossRef] [PubMed]
- Cappelli, L.C.; Gutierrez, A.K.; Bingham, C.O., 3rd; Shah, A.A. Rheumatic and Musculoskeletal Immune-Related Adverse Events Due to Immune Checkpoint Inhibitors: A Systematic Review of the Literature. Arthritis Care Res. (Hoboken) 2017, 69, 1751–1763. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, L.B.; Salama, A.K.S. A Review of Immune-Mediated Adverse Events in Melanoma. Oncol. Ther. 2019, 7, 101–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.H.; Zang, X.Y.; Wang, J.C.; Huang, S.S.; Xu, J.; Zhang, P. Diagnosis and Management of Immune Related Adverse Events (irAEs) in Cancer Immunotherapy. Biomed. Pharmacother. 2019, 120, 109437. [Google Scholar] [CrossRef] [PubMed]
- Simeone, E.; Grimaldi, A.M.; Festino, L.; Trojaniello, C.; Vitale, M.G.; Vanella, V.; Palla, M.; Ascierto, P.A. Immunotherapy in metastatic melanoma: A novel scenario of new toxicities and their management. Melanoma Manag. 2019, 6, MMT30. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Y.; Zeng, L.; Shen, Q.; Zhou, Z.; Mao, Z.; Wang, Q.; Zhang, X.; Li, Y.; Yao, W. Diagnosis and Treatment of Rheumatic Adverse Events Related to Immune Checkpoint Inhibitors. J. Immunol. Res. 2020, 2020, 2640273. [Google Scholar] [CrossRef]
- Zhong, H.; Zhou, J.; Xu, D.; Zeng, X. Rheumatic immune-related adverse events induced by immune checkpoint inhibitors. Asia Pac. J. Clin. Oncol. 2020. [CrossRef] [PubMed]
- Solimando, A.G.; Crudele, L.; Leone, P.; Argentiero, A.; Guarascio, M.; Silvestris, N.; Vacca, A.; Racanelli, V. Immune Checkpoint Inhibitor-Related Myositis: From Biology to Bedside. Int. J. Mol. Sci. 2020, 21, 3054. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Calle, N.; Rodriguez-Otero, P.; Villar, S.; Mejias, L.; Melero, I.; Prosper, F.; Marinello, P.; Paiva, B.; Idoate, M.; San-Miguel, J. Anti-PD1 associated fulminant myocarditis after a single pembrolizumab dose: The role of occult pre-existing autoimmunity. Haematologica 2018, 103, e318–e321. [Google Scholar] [CrossRef]
- Cuce, M.; Gallo Cantafio, M.E.; Siciliano, M.A.; Riillo, C.; Caracciolo, D.; Scionti, F.; Staropoli, N.; Zuccala, V.; Maltese, L.; Di Vito, A.; et al. Trabectedin triggers direct and NK-mediated cytotoxicity in multiple myeloma. J. Hematol. Oncol. 2019, 12, 32. [Google Scholar] [CrossRef]
- Botta, C.; Misso, G.; Martino, E.C.; Pirtoli, L.; Cusi, M.G.; Tassone, P.; Tagliaferri, P.; Caraglia, M.; Correale, P. The route to solve the interplay between inflammation, angiogenesis and anti-cancer immune response. Cell Death Dis. 2016, 7, e2299. [Google Scholar] [CrossRef] [Green Version]
- Botta, C.; Di Martino, M.T.; Ciliberto, D.; Cuce, M.; Correale, P.; Rossi, M.; Tagliaferri, P.; Tassone, P. A gene expression inflammatory signature specifically predicts multiple myeloma evolution and patients survival. Blood Cancer J. 2016, 6, e511. [Google Scholar] [CrossRef] [PubMed]
- Botta, C.; Cuce, M.; Caracciolo, D.; Fiorillo, L.; Tagliaferri, P.; Tassone, P. Immunomodulatory Activity of MicroRNAs: Potential Implications for Multiple Myeloma Treatment. Curr. Cancer Drug Targets 2017, 17, 819–838. [Google Scholar] [CrossRef] [PubMed]
- Botta, C.; Bestoso, E.; Apollinari, S.; Cusi, M.G.; Pastina, P.; Abbruzzese, A.; Sperlongano, P.; Misso, G.; Caraglia, M.; Tassone, P.; et al. Immune-modulating effects of the newest cetuximab-based chemoimmunotherapy regimen in advanced colorectal cancer patients. J. Immunother. 2012, 35, 440–447. [Google Scholar] [CrossRef]
- Botta, C.; Barbieri, V.; Ciliberto, D.; Rossi, A.; Rocco, D.; Addeo, R.; Staropoli, N.; Pastina, P.; Marvaso, G.; Martellucci, I.; et al. Systemic inflammatory status at baseline predicts bevacizumab benefit in advanced non-small cell lung cancer patients. Cancer Biol. Ther. 2013, 14, 469–475. [Google Scholar] [CrossRef] [Green Version]
- Botta, C.; Gulla, A.; Correale, P.; Tagliaferri, P.; Tassone, P. Myeloid-derived suppressor cells in multiple myeloma: Pre-clinical research and translational opportunities. Front. Oncol. 2014, 4, 348. [Google Scholar] [CrossRef] [PubMed]
- Perez, C.; Botta, C.; Zabaleta, A.; Puig, N.; Cedena, M.T.; Goicoechea, I.; Alameda, D.; San Jose-Eneriz, E.; Merino, J.; Rodriguez-Otero, P.; et al. Immunogenomic identification and characterization of granulocytic myeloid-derived suppressor cells in multiple myeloma. Blood 2020, 136, 199–209. [Google Scholar] [CrossRef]
- Sacco, A.; Battaglia, A.M.; Botta, C.; Aversa, I.; Mancuso, S.; Costanzo, F.; Biamonte, F. Iron Metabolism in the Tumor Microenvironment-Implications for Anti-Cancer Immune Response. Cells 2021, 10, 303. [Google Scholar] [CrossRef] [PubMed]
- Nerli, S.; Sgourakis, N.G. Structure-based modeling of SARS-CoV-2 peptide/HLA-A02 antigens. bioRxiv 2020. [CrossRef]
- Chinoy, H.; Payne, D.; Poulton, K.V.; Fertig, N.; Betteridge, Z.; Gunawardena, H.; Davidson, J.E.; Oddis, C.V.; McHugh, N.J.; Wedderburn, L.R.; et al. HLA-DPB1 associations differ between DRB1*03 positive anti-Jo-1 and anti-PM-Scl antibody positive idiopathic inflammatory myopathy. Rheumatology 2009, 48, 1213–1217. [Google Scholar] [CrossRef] [Green Version]
- Maniaol, A.H.; Elsais, A.; Lorentzen, A.R.; Owe, J.F.; Viken, M.K.; Saether, H.; Flam, S.T.; Brathen, G.; Kampman, M.T.; Midgard, R.; et al. Late onset myasthenia gravis is associated with HLA DRB1*15:01 in the Norwegian population. PLoS ONE 2012, 7, e36603. [Google Scholar] [CrossRef] [Green Version]
- Rothwell, S.; Chinoy, H.; Lamb, J.A.; Miller, F.W.; Rider, L.G.; Wedderburn, L.R.; McHugh, N.J.; Mammen, A.L.; Betteridge, Z.E.; Tansley, S.L.; et al. Focused HLA analysis in Caucasians with myositis identifies significant associations with autoantibody subgroups. Ann. Rheum. Dis. 2019, 78, 996–1002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carr, A.S.; Cardwell, C.R.; McCarron, P.O.; McConville, J. A systematic review of population based epidemiological studies in Myasthenia Gravis. BMC Neurol. 2010, 10, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osserman, K.E.; Genkins, G. Studies in myasthenia gravis: Review of a twenty-year experience in over 1200 patients. Mt. Sinai J. Med. 1971, 38, 497–537. [Google Scholar]
- Hoch, W.; McConville, J.; Helms, S.; Newsom-Davis, J.; Melms, A.; Vincent, A. Auto-antibodies to the receptor tyrosine kinase MuSK in patients with myasthenia gravis without acetylcholine receptor antibodies. Nat. Med. 2001, 7, 365–368. [Google Scholar] [CrossRef] [PubMed]
- Lindstrom, J.M.; Seybold, M.E.; Lennon, V.A.; Whittingham, S.; Duane, D.D. Antibody to acetylcholine receptor in myasthenia gravis. Prevalence, clinical correlates, and diagnostic value. Neurology 1976, 26, 1054–1059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larkin, J.; Chmielowski, B.; Lao, C.D.; Hodi, F.S.; Sharfman, W.; Weber, J.; Suijkerbuijk, K.P.M.; Azevedo, S.; Li, H.; Reshef, D.; et al. Neurologic Serious Adverse Events Associated with Nivolumab Plus Ipilimumab or Nivolumab Alone in Advanced Melanoma, Including a Case Series of Encephalitis. Oncologist 2017, 22, 709–718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Safa, H.; Johnson, D.H.; Trinh, V.A.; Rodgers, T.E.; Lin, H.; Suarez-Almazor, M.E.; Fa’ak, F.; Saberian, C.; Yee, C.; Davies, M.A.; et al. Immune checkpoint inhibitor related myasthenia gravis: Single center experience and systematic review of the literature. J. Immunother. Cancer 2019, 7, 319. [Google Scholar] [CrossRef]


{kind=link}
| Blood Tests | Baseline | Post-Treatment | Follow-Up |
|---|---|---|---|
| Inflammatory markers | |||
| CRP (mg/L) | 40.7 (#) | 15.5 (#) | 6.59 (#) |
| ESR (mm/h) | 104 (#) | 50 (#) | 24 (#) |
| Cell lysis enzymes | |||
| AST (U/L) | 35 | 445 (#) | 19 |
| ALT (U/L) | 15 | 109 (#) | 7 |
| LDH (U/L) | 154 | 4403 (#) | 177 |
| CK (U/L) | ND | 4403 (#) | 100 |
| CK MB(U/L) | ND | 189 (#) | 9 |
| Troponin I (ng/mL) | ND | 5.42 (#) | <0.012 |
| Auto-antibodies | |||
| ASMA | ND | negative | negative |
| ENA | ND | negative | negative |
| ANA | ND | 1/1280 (#) | 1/160 (#) |
| Anti-peroxidase (U/l) | ND | 94.64 (#) | 125.80 (#) |
| Anti-ChR-abs (U/mL) | ND | 2.8 (#) | 2.68 (#) |
| Anti-MuSK (U/mL) | ND | <0.4 | <0.4 |
| CD4+/CD8+ T cell ratio | 1.50 | 1.1 | ND |
| Activated T cells % (HLA-DR+) | 21 | 27 | ND |
| Activated T cells % (HLA-DR+) |
| Patient’s Characteristics | |
|---|---|
| Contrast-enhanced brain MRI | No CNS metastases |
| Single-fiber EMG and repetitive nerve stimulation test | Within normal ranges |
| Cerebrospinal fluid | Within normal ranges |
| hearth ultrasonography | Within normal ranges |
| HLA haplotype | HLA-A*02/*29 HLA-B*08/*35 HLA-C*04/*07 DRB1*03/*04 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Botta, C.; Agostino, R.M.; Dattola, V.; Cianci, V.; Calandruccio, N.D.; Bianco, G.; Mafodda, A.; Maisano, R.; Iuliano, E.; Orizzonte, G.; et al. Myositis/Myasthenia after Pembrolizumab in a Bladder Cancer Patient with an Autoimmunity-Associated HLA: Immune–Biological Evaluation and Case Report. Int. J. Mol. Sci. 2021, 22, 6246. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22126246
Botta C, Agostino RM, Dattola V, Cianci V, Calandruccio ND, Bianco G, Mafodda A, Maisano R, Iuliano E, Orizzonte G, et al. Myositis/Myasthenia after Pembrolizumab in a Bladder Cancer Patient with an Autoimmunity-Associated HLA: Immune–Biological Evaluation and Case Report. International Journal of Molecular Sciences. 2021; 22(12):6246. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22126246
Chicago/Turabian StyleBotta, Cirino, Rita Maria Agostino, Vincenzo Dattola, Vittoria Cianci, Natale Daniele Calandruccio, Giovanna Bianco, Antonino Mafodda, Roberto Maisano, Eleonora Iuliano, Giovanna Orizzonte, and et al. 2021. "Myositis/Myasthenia after Pembrolizumab in a Bladder Cancer Patient with an Autoimmunity-Associated HLA: Immune–Biological Evaluation and Case Report" International Journal of Molecular Sciences 22, no. 12: 6246. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22126246