
2021 Update on Diagnostic Markers and Translocation in Salivary Gland Tumors


Abstract
:1. Introduction
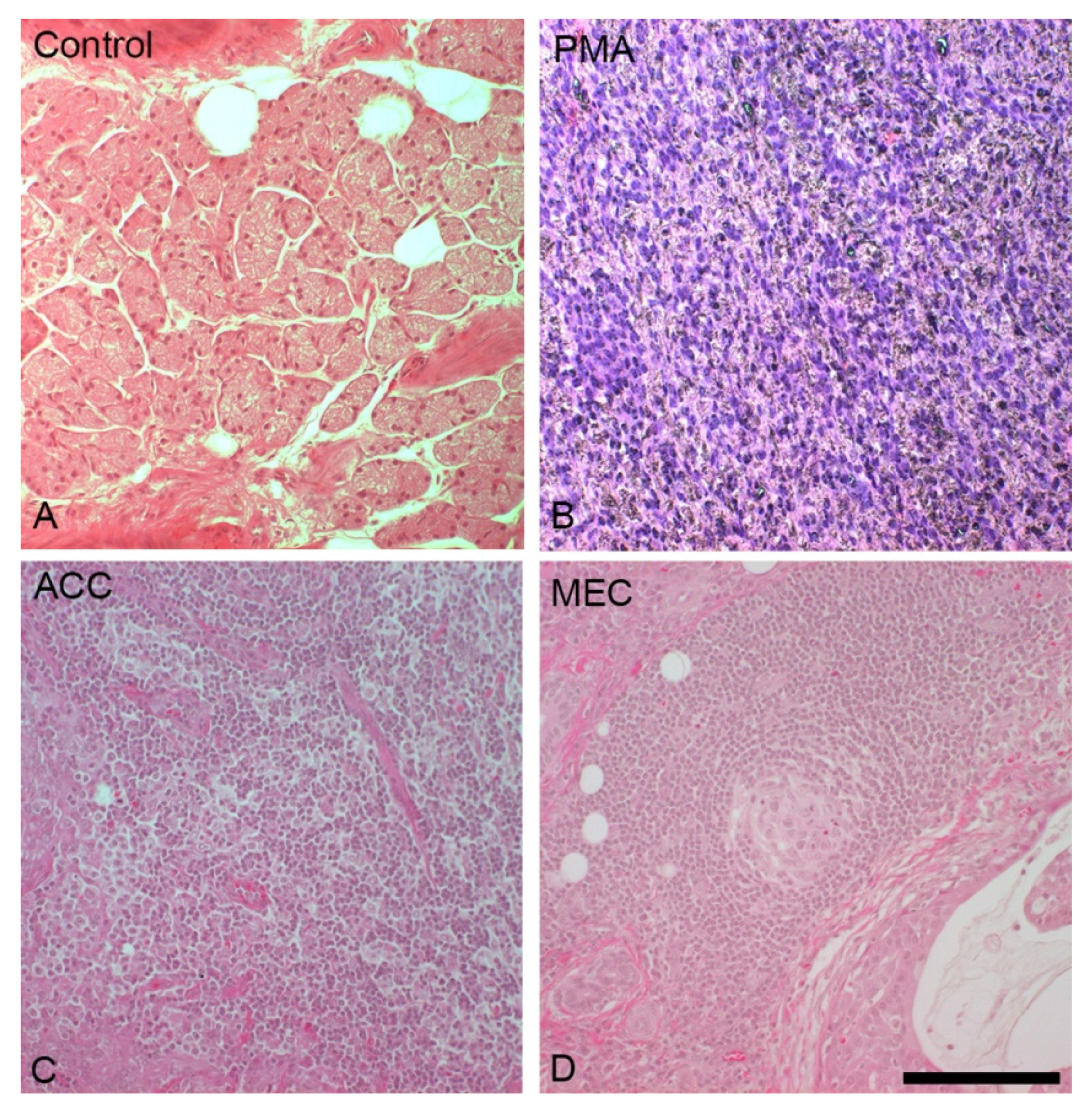
1.1. Histology of the Healthy Salivary Gland
1.2. Current Status of Salivary Gland Tumors and Markers
1.2.1. Acinar and Adenoid Cell Carcinomas

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Sample Size ACC | Marker | Reaction | in % |
|---|---|---|---|---|
| [30] | Six | Alpha-1-Antitrypsin | 3 of 6 | 50% |
| [31] | Three of parotid origin | Amylase | 0 of 3 | 0% |
| [11] | Four of parotid origin | Apocrine | 1 of 4 | 25% |
| [11] | Four of parotid origin | Caldesmon | 0 of 4 | 0% |
| [11,12] | Eight of salivary gland and head and neck origin; four of parotid origin | Calponin | 0 of 8; 0 of 4 | 0% |
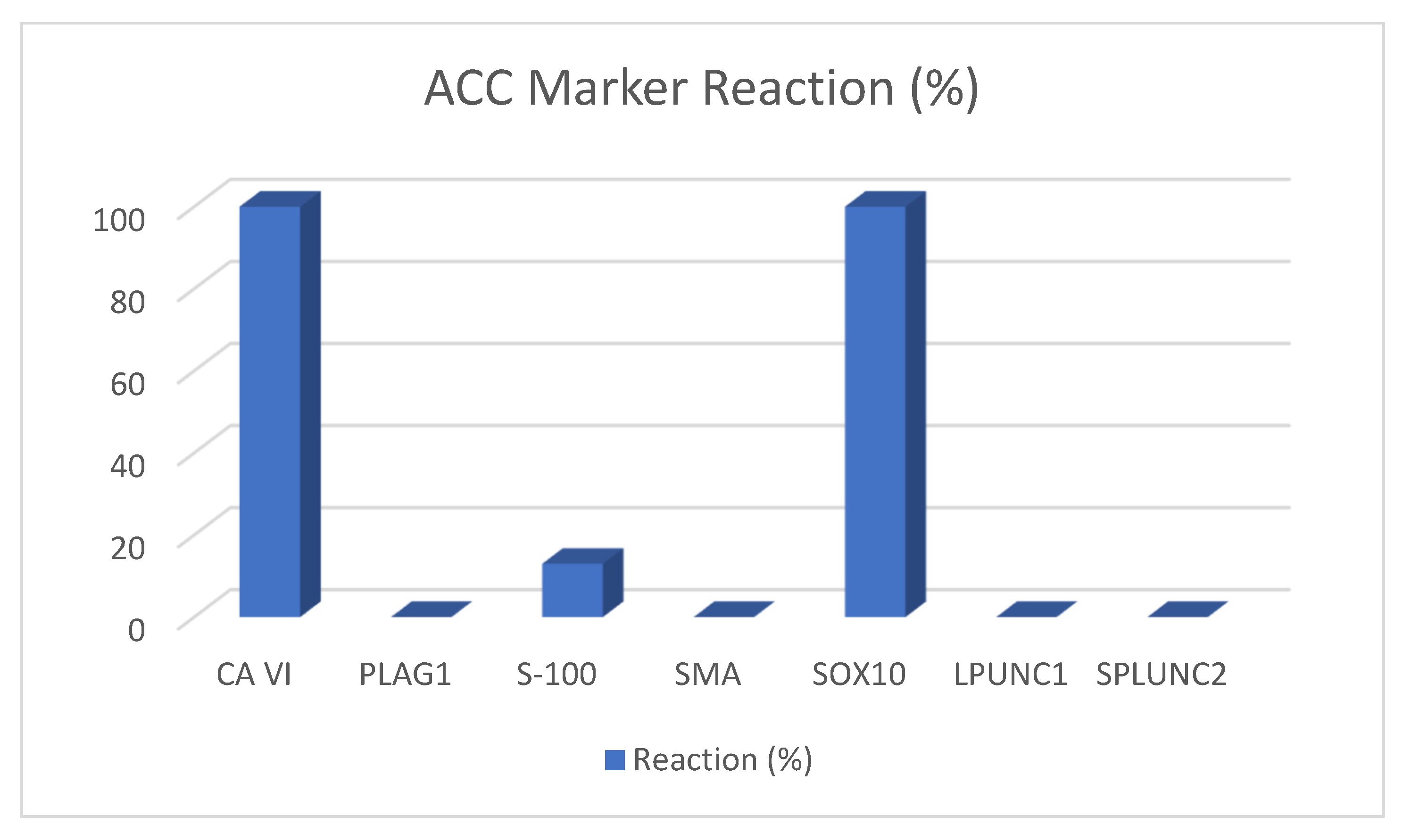
| [14] | 28 of salivary gland origin | Carbonic anhydrase VI (CA6) | 28 of 28 | 100% |
| [30] | Six | Chromogranin | 0 of 6 | 0% |
| [30] | Six | Chymotrypsin | 4 of 6 | 67% |
| [11] | Four of parotid gland origin | CK7 | 4 of 4 | 100% |
| [11] | Four of parotid origin | CK 8 | 4 of 4 | 100% |
| [11] | Four of parotid origin | CK14 | 0 of 4 | 0%//+ |
| [11] | Four of parotid origin | CK 17 | 0 of 4 | 0%//+ |
| [11] | Four of parotid origin | CK19 | 4 of 4 | 100% |
| [11] | Four of parotid origin | CK20 | 0 of 4 | 0% |
| [14,18] | 28 of salivary gland origin; 28 of salivary gland origin | DOG-1 | 28 of 28; 28 of 28 | 100%; 100% |
| [12] | Eight of salivary gland and head and neck origin | GFAP | 0 of 8 | 0% |
| [19] | One of salivary gland origin or potential mimickers | HMGA-2 | 0 of 1 | 0% |
| [21] | Seven of upper aerodigestive tract origin | KIT (CD117) | 6 of 7 | 86% |
| [22] | Nine of salivary gland origin | LPLUNC1 | 0 of 9 | 0% |
| [23,24] | Five of salivary gland origin; eleven of salivary gland origin | Maspin | 5 of 5; 0 of 11 | 100%; 0% |
| [23] | Five of salivary gland origin | MCM2 | 5 of 5 | 100% |
| [11] | Four of parotid origin | Mit | 1 of 4 | 25% |
| [21] | Seven of upper aerodigestive tract origin | MYB | 0 of 7 | 0% |
| [13] | Five | p53 | 2 of 5 | 40% |
| [12,27] | Eight of salivary gland and head and neck origin; eight | p63 | 0 of 8; 0 of 8 | 0%; 0% |
| [27] | Eight | p73 | 5 of 8 | 63% |
| [19] | One of salivary gland origin or potential mimickers | PLAG1 | 0 of 1 | 0% |
| [12,14] | Eight of salivary gland and head and neck origin; 28 of salivary gland origin | S-100 | 1 of 8; 2 of 28 | 13%; 7.1% |
| [11,12] | Eight of salivary gland and head and neck origin; four of parotid origin | SMA | 0 of 8; 0 of 4 | 0% |
| [11] | Four of parotid origin | SMM | 0 of 4 | 0% |
| [22] | Nine of salivary gland origin | SPLUNC1 | 0 of 9 | 0% |
| [22] | Nine of salivary gland origin | SPLUNC2 | 0 of 9 | 0% |
| [12] | Eight of salivary gland and head and neck origin | SOX10 | 8 of 8 | 100% |
| [30] | Six | Synaptophysin | 4 of 6 | 67% |
| [14] | 28 of salivary gland origin | Vimentin | 23 of 28 | 82% |
1.2.2. Mucoepidermoid Carcinomas
1.2.3. Polymorphous Adenocarcinomas
1.2.4. Salivary Duct Carcinomas
1.2.5. Pleomorphic Adenomas
2. State-of-the-Art Methods in Pre-Operative Diagnosis of Salivary Gland Tumors
3. Fine Needle Aspiration of Salivary Gland Tumors
4. Translocations
4.1. Translocations in Pleomorphic Adenomas (PAs)
4.2. Translocations in Mucoepidermoid Carcinomas (MECs)
4.3. Translocations in Adenoid Cystic Carcinomas (ACCs)
5. Analysis of Markers
6. Future Directives
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Bradley, P.J.; McGurk, M. Incidence of Salivary Gland Neoplasms in a Defined UK Population. Br. J. Oral Maxillofac. Surg. 2013, 51, 399–403. [Google Scholar] [CrossRef]
- Del Signore, A.G.; Megwalu, U.C. The Rising Incidence of Major Salivary Gland Cancer in the United States. Ear Nose Throat J. 2017, 96, E13–E16. [Google Scholar] [CrossRef]
- Rousseau, A.; Badoual, C. Head and Neck: Salivary Gland Tumors: An Overview. Atlas Genet. Cytogenet. Oncol. Haematol. 2011, 15. [Google Scholar] [CrossRef]
- Cunha, J.L.S.; Coimbra, A.C.P.; Silva, J.V.R.; Nascimento, I.S.; Andrade, M.E.; Oliveira, C.R.; Almeida, O.; Soares, C.; Sousa, S.F.; Albuquerque-Júnior, R.L. Epidemiologic Analysis of Salivary Gland Tumors over a 10-Years Period Diagnosed in a Northeast Brazilian Population. Med. Oral Patol. Oral Cirugia Bucal 2020, 25, e516–e522. [Google Scholar] [CrossRef]
- Speight, P.M.; Barrett, A.W. Salivary Gland Tumours: Diagnostic Challenges and an Update on the Latest WHO Classification. Diagn. Histopathol. 2020, 26, 147–158. [Google Scholar] [CrossRef]
- Hellquist, H.; Skalova, A. Histopathology of the Salivary Glands; Springer: Berlin/Heidelberg, Germany, 2014; ISBN 978-3-540-46912-4. [Google Scholar]
- Nagao, T.; Sato, E.; Inoue, R.; Oshiro, H.; Takahashi, R.H.; Nagai, T.; Yoshida, M.; Suzuki, F.; Obikane, H.; Yamashina, M.; et al. Immunohistochemical Analysis of Salivary Gland Tumors: Application for Surgical Pathology Practice. ACTA Histochem. Cytochem. 2012, 45, 269–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curran, A.E.; Allen, C.M.; Beck, F.M.; Damm, D.D.; Murrah, V.A. Distinctive Pattern of Glial Fibrillary Acidic Protein Immunoreactivity Useful in Distinguishing Fragmented Pleomorphic Adenoma, Canalicular Adenoma and Polymorphous Low Grade Adenocarcinoma of Minor Salivary Glands. Head Neck Pathol. 2007, 1, 27–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eveson, J.W.; Cawson, R.A. Salivary gland tumours. A review of 2410 cases with particular reference to histological types, site, age and sex distribution. J. Pathol. 1985, 146, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Schneider, S.; Kloimstein, P.; Pammer, J.; Brannath, W.; Grasl, M.C.; Erovic, B.M. New Diagnostic Markers in Salivary Gland Tumors. Eur. Arch. Otorhinolaryngol. 2014, 271, 1999–2007. [Google Scholar] [CrossRef]
- Foschini, M.P.; Marucci, G.; Eusebi, V. Low-grade mucoepidermoid carcinoma of salivary glands: Characteristic immunohistochemical profile and evidence of striated duct differentiation. Virchows Arch. 2002, 440, 536–542. [Google Scholar] [CrossRef]
- Ohtomo, R.; Mori, T.; Shibata, S.; Tsuta, K.; Maeshima, A.M.; Akazawa, C.; Watabe, Y.; Honda, K.; Yamada, T.; Yoshimoto, S.; et al. SOX10 is a novel marker of acinus and intercalated duct differentiation in salivary gland tumors: A clue to the histogenesis for tumor diagnosis. Mod. Pathol. 2013, 26, 1041–1050. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsubochi, H.; Suzuki, T.; Suzuki, S.; Ohashi, Y.; Ishibashi, S.; Moriya, T.; Fujimura, S.; Sasano, H. Immunohistochemical study of basaloid squamous cell carcinoma, adenoid cystic and mucoepidermoid carcinoma in the upper aerodigestive tract. Anticancer Res. 2000, 20, 1205–1211. [Google Scholar]
- Hsieh, M.S.; Jeng, Y.M.; Jhuang, Y.L.; Chou, Y.H.; Lin, C.Y. Carbonic anhydrase VI: A novel marker for salivary serous acinar differentiation and its application to discriminate acinic cell carcinoma from mammary analogue secretory carcinoma of the salivary gland. Histopathology 2016, 68, 641–647. [Google Scholar] [CrossRef]
- Sakamoto, K.; Nakamura, Y.; Nakashima, T. Immunohistochemical distribution of CD9 in parotid gland tumors. Auris Nasus Larynx 2004, 31, 49–55. [Google Scholar] [CrossRef]
- Woo, V.L.; Bhuiya, T.; Kelsch, R. Assessment of CD43 expression in adenoid cystic carcinomas, polymorphous low-grade adenocarcinomas, and monomorphic adenomas. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 102, 495–500. [Google Scholar] [CrossRef] [PubMed]
- Edwards, P.C.; Bhuiya, T.; Kelsch, R.D. C-kit expression in the salivary gland neoplasms adenoid cystic carcinoma, polymorphous low-grade adenocarcinoma, and monomorphic adenoma. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2003, 95, 586–593. [Google Scholar] [CrossRef] [Green Version]
- Chenevert, J.; Duvvuri, U.; Chiosea, S.; Dacic, S.; Cieply, K.; Kim, J.; Shiwarsk, D.; Seethala, R.R. DOG1: A novel marker of salivary acinar and intercalated duct differentiation. Mod. Pathol. 2012, 25, 919–929. [Google Scholar] [CrossRef]
- Foo, W.C.; Jo, V.Y.; Krane, J.F. Usefulness of translocation-associated immunohistochemical stains in the fine-needle aspiration diagnosis of salivary gland neoplasms. Cancer Cytopathol. 2016, 124, 397–405. [Google Scholar] [CrossRef]
- Mino, M.; Pilch, B.Z.; Faquin, W.C. Expression of KIT (CD117) in neoplasms of the head and neck: An ancillary marker for adenoid cystic carcinoma. Mod. Pathol. 2003, 16, 1224–1231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- West, R.B.; Kong, C.; Clarke, N.; Gilks, T.; Lipsick, J.; Cao, H.; Kwok, S.; Montgomery, K.D.; Varma, S.; Le, Q.T. MYB expression and translocation in adenoid cystic carcinomas and other salivary gland tumors with clinicopathologic correlation. Am. J. Surg. Pathol. 2011, 35, 92–99. [Google Scholar] [CrossRef] [Green Version]
- Vargas, P.A.; Speight, P.M.; Bingle, C.D.; Barrett, A.W.; Bingle, L. Expression of PLUNC family members in benign and malignant salivary gland tumours. Oral Dis. 2008, 14, 613–619. [Google Scholar] [CrossRef] [Green Version]
- Ghazy, S.E.; Helmy, I.M.; Baghdadi, H.M. Maspin and MCM2 Immunoprofiling in Salivary Gland Carcinomas. Diagn. Pathol. 2011, 6, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Schwarz, S.; Ettl, T.; Kleinsasser, N.; Hartmann, A.; Reichert, T.-E.; Driemel, O. Loss of Maspin Expression Is a Negative Prognostic Factor in Common Salivary Gland Tumors. Oral Oncol. 2008, 44, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Heiduschka, G.; Erovic, B.M.; Pammer, J.; Kotowski, U.; Kaider, A.; Ch. Grasl, M.; Thurnher, D. Mcl-1 expression is up-regulated in malignancies of the parotid gland. Dis. Markers 2011, 30, 229–233. [Google Scholar] [CrossRef]
- do Nascimento, K.C.; de Faria, P.R.; Dib, L.L.; Ferreira de Aguiar, M.C.; Cardoso, S.V.; Chen, J.; Loyola, A.M. Immunohistochemical Localization of the NM23 Protein in Salivary Gland Neoplasms with Distinct Biological Behavior. Virchows Arch. 2006, 449, 660–666. [Google Scholar] [CrossRef]
- Seethala, R.R.; LiVolsi, V.A.; Zhang, P.J.; Pasha, T.L.; Baloch, Z.W. Comparison of P63 and P73 Expression in Benign and Malignant Salivary Gland Lesions. Head Neck 2005, 27, 696–702. [Google Scholar] [CrossRef]
- Pramoonjago, P.; Baras, A.S.; Moskaluk, C.A. Knockdown of Sox4 Expression by RNAi Induces Apoptosis in ACC3 Cells. Oncogene 2006, 25, 5626–5639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, A.K.; Bland, K.I.; McGinnis, L.S.; Morrow, M.; Eyre, H.J. Clinical highlights from the National Cancer Data Base, 2000. CA: A Cancer J. Clin. 2000, 50, 171–183. [Google Scholar] [CrossRef] [PubMed]
- Skacel, M.; Ormsby, A.H.; Petras, R.E.; McMahon, J.T.; Henricks, W.H. Immunohistochemistry in the Differential Diagnosis of Acinar and Endocrine Pancreatic Neoplasms. Appl. Immunohistochem. Mol. Morphol. 2000, 8, 203–209. [Google Scholar] [CrossRef]
- Morely, D.J.; Hodes, M.E. Amylase Expression in Human Parotid Neoplasms: Evidence by In Situ Hybridization for Lack of Transcription of the Amylase Gene. J. Histochem. Cytochem. 1988, 36, 487–491. [Google Scholar] [CrossRef]
- Kokemueller, H.; Brueggemann, N.; Swennen, G.; Eckardt, A. Mucoepidermoid carcinoma of the salivary glands--clinical review of 42 cases. Oral Oncol. 2005, 41, 3–10. [Google Scholar] [CrossRef]
- Capodiferro, S.; Ingravallo, G.; Limongelli, L.; Mastropasqua, M.G.; Tempesta, A.; Favia, G.; Maiorano, E. Intra-Cystic (In Situ) Mucoepidermoid Carcinoma: A Clinico-Pathological Study of 14 Cases. J. Clin. Med. 2020, 9, 1157. [Google Scholar] [CrossRef] [Green Version]
- Butler, R.T.; Spector, M.E.; Thomas, D.; McDaniel, A.S.; McHugh, J.B. An immunohistochemical panel for reliable differentiation of salivary duct carcinoma and mucoepidermoid carcinoma. Head Neck Pathol. 2014, 8, 133–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pires, F.R.; De Almeida, O.P.; De Araujo, V.C.; Kowalski, L.P. Prognostic factors in head and neck mucoepidermoid carcinoma. Arch. Otolaryngol. Head Neck Surg. 2004, 130, 174–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zyada, M.M.; Grawish, M.E.; Elsabaa, H.M. Predictive value of cyclooxygenase 2 and Bcl-2 for cervical lymph node metastasis in mucoepidermoid carcinoma. Ann. Diagn. Pathol. 2009, 13, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Alos, L.; Lujan, B.; Castillo, M.; Nadal, A.; Carreras, M.; Caballero, M.; de Bolos, C.; Cardesa, A. Expression of Membrane-Bound Mucins (MUC1 and MUC4) and Secreted Mucins (MUC2, MUC5AC, MUC5B, MUC6 and MUC7) in Mucoepidermoid Carcinomas of Salivary Glands. Am. J. Surg. Pathol. 2005, 29, 806–813. [Google Scholar] [CrossRef]
- Zhu, S.; Schuerch, C.; Hunt, J. Review and Updates of Immunohistochemistry in Selected Salivary Gland and Head and Neck Tumors. Arch. Pathol. Lab. Med. 2015, 139, 55–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Subhashraj, K. Salivary Gland Tumors: A Single Institution Experience in India. Br. J. Oral Maxillofac. Surg. 2008, 46, 635–638. [Google Scholar] [CrossRef]
- Seifert, G.; Langrock, I.; Donath, K. A pathological classification of pleomorphic adenoma of the salivary glands (author’s transl). Hno 1976, 24, 415–426. [Google Scholar]
- Seethala, R.R.; Stenman, G. Update from the 4th Edition of the World Health Organization Classification of Head and Neck Tumours: Tumors of the Salivary Gland. Head Neck Pathol. 2017, 11, 55–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bradley, P.J. Metastasizing pleomorphic salivary adenoma’ should now be considered a low-grade malignancy with a lethal potential. Curr. Opin. Otolaryngol. Head Neck Surg. 2005, 13, 123–126. [Google Scholar] [CrossRef]
- Matsuyama, A.; Hisaoka, M.; Nagao, Y.; Hashimoto, H. Aberrant PLAG1 expression in pleomorphic adenomas of the salivary gland: A molecular genetic and immunohistochemical study. Virchows Arch. 2011, 458, 583–592. [Google Scholar] [CrossRef]
- Abdel Razek, A.A.K.; Mukherji, S.K. State-of-the-Art Imaging of Salivary Gland Tumors. Neuroimaging Clin. N. Am. 2018, 28, 303–317. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, R.L.; Hall, B.J.; Wilson, A.R.; Layfield, L.J. A systematic review and meta-analysis of the diagnostic accuracy of fine-needle aspiration cytology for parotid gland lesions. Am. J. Clin. Pathol. 2011, 136, 45–59. [Google Scholar] [CrossRef] [Green Version]
- Layfield, L.J.; Gopez, E.; Hirschowitz, S. Cost efficiency analysis for fine-needle aspiration in the workup of parotid and submandibular gland nodules. Diagn. Cytopathol. 2006, 34, 734–738. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, R.L.; Hunt, J.P.; Hall, B.J.; Wilson, A.R.; Layfield, L.J. A systematic review and meta-analysis of the diagnostic accuracy of frozen section for parotid gland lesions. Am. J. Clin. Pathol. 2011, 136, 729–738. [Google Scholar] [CrossRef] [PubMed]
- Griffith, C.C.; Pai, R.K.; Schneider, F.; Duvvuri, U.; Ferris, R.L.; Johnson, J.T.; Seethala, R.R. Salivary gland tumor fine-needle aspiration cytology: A proposal for a risk stratification classification. Am. J. Clin. Pathol. 2015, 143, 839–853. [Google Scholar] [CrossRef] [Green Version]
- Vasudevan, G.; Bishnu, A.; Singh, B.M.K.; Singh, V.K. Mucoepidermoid Carcinoma of Salivary Gland: Limitations and Pitfalls on FNA. J. Clin. Diagn. Res. 2017, 11, ER04–ER06. [Google Scholar] [CrossRef]
- Bansal, A.; Kaur, M.; Dalal, V.; Siraj, F. Papillary Pattern in Acinic Cell Carcinoma of Parotid Gland: A Potential Diagnostic Pitfall on FNAC. J. Cytol. 2018, 35, 57–59. [Google Scholar] [CrossRef]
- Weinreb, I. Translocation-Associated Salivary Gland Tumors: A Review and Update. Adv. Anat. Pathol. 2013, 20, 367–377. [Google Scholar] [CrossRef]
- Seethala, R.R.; Dacic, S.; Cieply, K.; Kelly, L.M.; Nikiforova, M.N. A Reappraisal of the MECT1/MAML2 Translocation in Salivary Mucoepidermoid Carcinomas. Am. J. Surg. Pathol. 2010, 34, 1106–1121. [Google Scholar] [CrossRef] [PubMed]
- Krishnamurthy, S. Salivary Gland Disorders: A Comprehensive Review. World J. Stomatol. 2015, 4, 56–71. [Google Scholar] [CrossRef]





| Normal Salivary Gland | Marker | Reaction |
|---|---|---|
| General | Androgen receptor | Negative |
| EBER in situ hybridization | Negative | |
| Ki-67 (MIB-1) | Few cells positive | |
| General | Melan A | Negative |
| P53 | Negative | |
| General | Renal cell carcinoma/CD10 | Negative |
| General | S-100 | Variable |
| General | CEA | Positive |
| Acinar cells | CK14 | Positive |
| Abluminal cells | P63 | Positive |
| Abluminal cells | CK, AE1/AE3 | Positive |
| Myoepithelial cells | Calponin | Positive |
| Myoepithelial cells | GFAP | Positive (variable) |
| Myoepithelial cells | MSA | Positive |
| Myoepithelial cells | SMA | Positive |
| Myoepithelial cells | Vimentin | Positive |
| Luminal cells | EMA | Positive |
| Gross cystic disease fluid protein | Positive | |
| CK, AE1/AE3 | Positive | |
| HER2 | Negative to weakly positive | |
| Striated duct cells | Mitochondrial | Positive |
| Alpha-amylase | Positive |
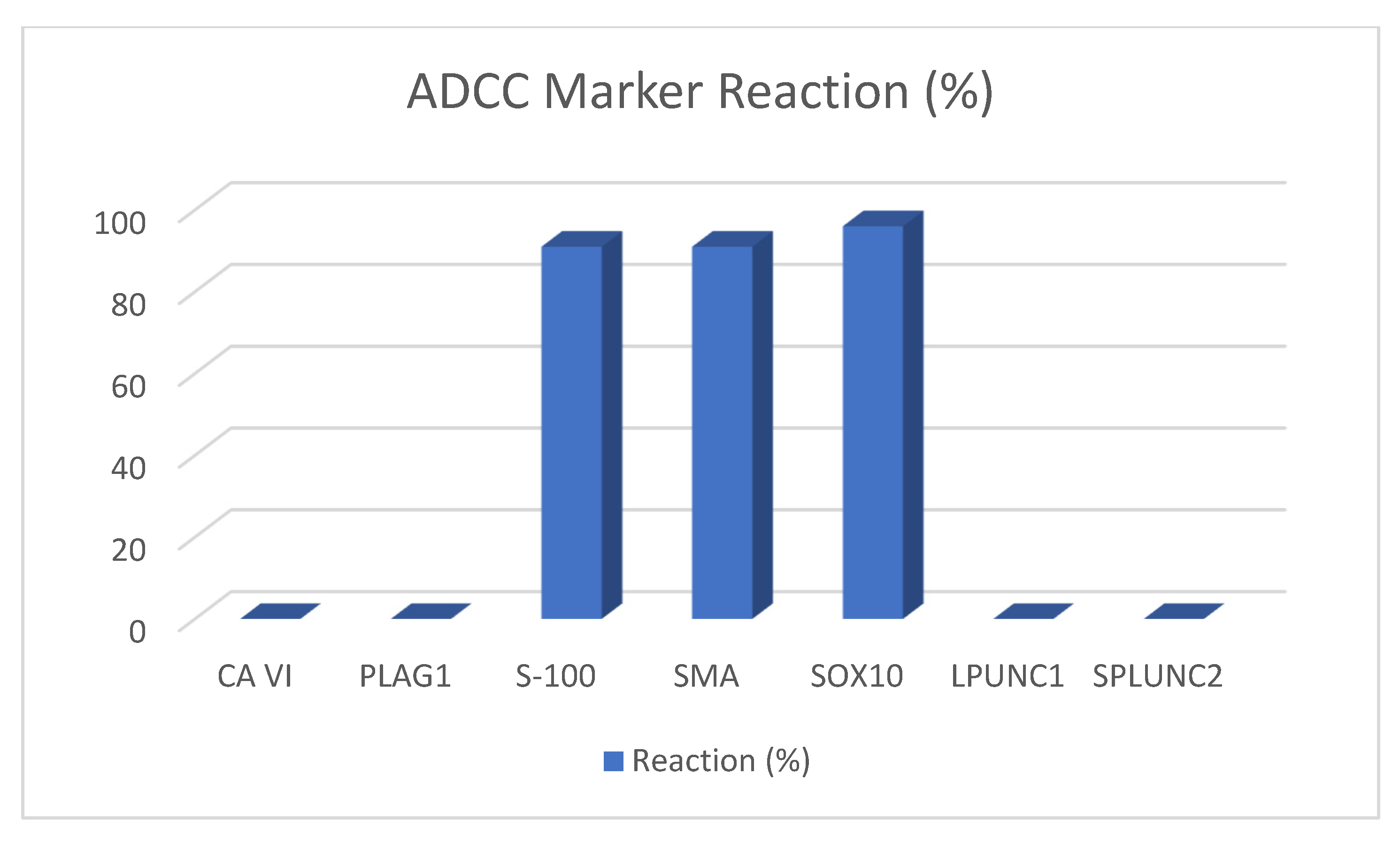
| Study | Sample Size ADCC | Marker | Reaction | in % |
|---|---|---|---|---|
| [11] | Three of upper aerodigestive tract origin | Apocrine | 0 of 3 | 0% |
| [11] | Three of upper aerodigestive tract origin | Caldesmon | 1 of 3 | 33% |
| [11,12] | 23 of salivary gland and head and neck origin; three of upper aerodigestive tract origin | Calponin | 18 of 23; 3 of 3 | 78%; 100% |
| [13] | Five | Carbohydrate Ag 19-9 | 0 of 5 | 0% |
| [14] | Six of salivary gland origin | Carbonic anhydrase VI (CA6) | 0 of 6 | 0% |
| [13] | Five | CEA | 0 of 5 | 0% |
| [15] | Three of parotid gland origin | CD9 | 0 of 3 | 0% |
| [16] | Four of parotid origin | CD43 | 4 of 4 | 100% |
| [13] | Five | CEA | 0 of 5 | 0% |
| [11] | Three of upper aerodigestive tract origin | CK7 | 3 of 3 | 100% |
| [11] | Three of upper aerodigestive tract origin | CK8 | 3 of 3 | 100% |
| [11] | Three of upper aerodigestive tract origin | CK14 | 3 of 3 | 100% |
| [11] | Three of upper aerodigestive tract origin | CK17 | 3 of 3 | 100% |
| [11] | Three of upper aerodigestive tract origin | CK19 | 3 of 3 | 100% |
| [11] | Three of upper aerodigestive tract origin | CK20 | 0 of 3 | 0% |
| [17] | 15 of salivary gland origin | C-Kit | 15 of 15 | 100% |
| [18] | 24 of salivary gland origin | DOG-1 | 17 of 24 | 70% |
| [12] | 23 of salivary gland and head and neck origin | GFAP | 5 of 23 | 21% |
| [19] | Nine of salivary gland origin or potential mimickers | HMGA-2 | 0 of 9 | 0% |
| [19,20,21] | 11 of salivary gland origin or potential mimickers; 66 of the head and neck area and breast; 37 of salivary gland origin | KIT | 4 of 11; 62 of 66 (H300 (54 of 66)/A4502 (58 of 66)); 37 of 37 | 36%; 94%; 100% |
| [22] | 13 of salivary gland origin | LPLUNC1 | 0 of 13 | 0% |
| [23,24] | 14 of salivary gland origin; 25 of salivary gland origin | Maspin | 12 of 14; 19 of 25 | 86%; 76% |
| [25] | 13 of parotid origin | Mcl-1 | 12 of 13 | 92% |
| [23] | 14 of salivary gland origin | MCM2 | 12 of 14 | 86% |
| [11] | Three of upper aerodigestive tract origin | Mit | 2 of 3 | 66% |
| [19,21] | Nine; 37 of salivary gland origin | MYB | 4 of 11; 24 of 37 | 36%; 65% |
| [26] | Six of upper aerodigestive tract and lung origin, 14 of salivary gland origin, one of maxilla origin | NM23 | 68,70% | |
| [12,27] | 23 of salivary gland and head and neck origin; 16 of salivary gland | p63 | 21 of 23; 16 of 16 | 91%; 100% |
| [27] | 16 of salivary gland | p73 | 16 of 16 | 100% |
| [19] | Eleven of salivary gland origin or potential mimickers | PLAG1 | 0 of 11 | 0% |
| [12] | 23 of salivary gland and head and neck origin | S-100 | 21 of 23 | 91% |
| [11,12] | 23 of salivary gland and head and neck origin; three of upper aerodigestive tract origin | SMA | 21 of 23; 3 of 3 | 91%; 100% |
| [11] | Three of upper aerodigestive tract origin | SMM | 2 of 3 | 66% |
| [22] | 13 of salivary gland origin | SPLUNC1 | 0 of 13 | 0% |
| [22] | 13 of salivary gland origin | SPLUNC2 | 0 of 13 | 0% |
| [28] | 28 | SOX4 | 28 of 28 | 100% |
| [12] | 23 of salivary gland and head and neck origin | SOX10 | 22 of 23 | 96% |
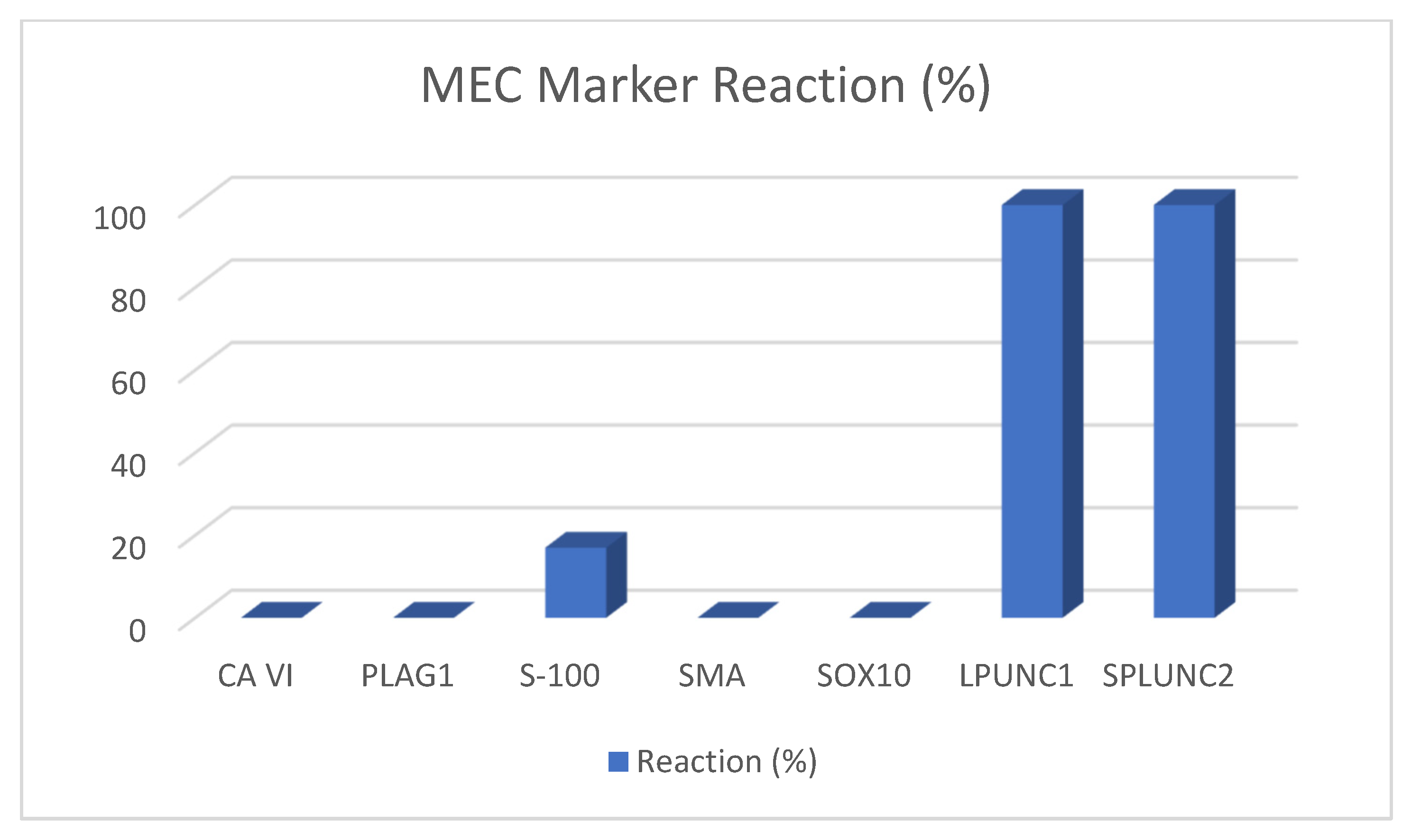
| Study | Sample Size MEC | Marker | Reaction | in % |
|---|---|---|---|---|
| [31] | Five of parotid origin | Amylase | 0 of 5 | 0% |
| [34] | 59 of upper aerodigestive tract origin | Androgen receptor | 0 of 59 | 0% |
| [11] | 10 of upper aerodigestive tract origin | Apocrine | 0 of 10 | 0% |
| [35] | 173 of upper aerodigestive tract origin | Bcl-2 | 63% | |
| [11] | 10 of upper aerodigestive tract origin | Caldesmon | 0 of 10 | 0% |
| [11,12] | Six; 10 of salivary gland and head and neck origin | Calponin | 0 of 6; 1 of 10 | 0%; 10% |
| [13] | Seven | Carbohydrate Ag 19-9 | 4 of 7 | 57.10% |
| [14] | Five of salivary gland origin | Carbonic anhydrase VI (CA6) | 0 of 5 | 0% |
| [13,35] | 173 of upper aerodigestive tract origin | CEA | 2 of 7 | 28.57%; 68.6% |
| [35] | 173 of upper aerodigestive tract origin | C-erb-2 | 80% | |
| [15] | Six of parotid origin | CD9 | 5 of 6 | 83% |
| [34] | 59 of upper aerodigestive tract origin | CK5/6 | 60 of 64 | 93.75% |
| [11] | 10 of upper aerodigestive tract origin | CK7 | 10 of 10 | 100% |
| [11] | 10 of upper aerodigestive tract origin | CK 8 | 10 of 10 | 100% |
| [11] | 10 of upper aerodigestive tract origin | CK14 | 10 of 10 | 100% |
| [11] | 10 of upper aerodigestive tract origin | CK 17 | 10 of 10 | 100% |
| [11] | 10 of upper aerodigestive tract origin | CK19 | 10 of 10 | 100% |
| [11] | 10 of upper aerodigestive tract origin | CK20 | 1 of 10 | 10% |
| [36] | 11 of upper aerodigestive tract origin | Cox-2 | 11 of 11 | 100% |
| [18] | Eight of salivary gland origin | DOG-1 | 3 of 8 | 37.50% |
| [12] | Six of salivary gland and head and neck origin | GFAP | 2 of 6 | 33% |
| [34] | 71 of upper aerodigestive tract origin | Her2/neu | 26 of 71 | 37% |
| [19] | Three of salivary gland origin or potential mimickers | HMGA-2 | 0 of 3 | 0% |
| [20,21] | Nine of head and neck origin; 23 of upper aerodigestive tract origin | KIT (CD117) | H300 (1 of 9)/A4502 (0 of 9); 10 of 23 | 1%; 43% |
| [22] | 10 of salivary gland origin | LPLUNC1 | 10 of 10 | 100% |
| [23,24] | 15 of salivary gland origin; 15 of salivary gland origin | Maspin | 15 of 15; 13 of 15 | 100%; 86.7% |
| [25] | 12 of parotid origin | Mcl-2 | 11 of 12 | 92% |
| [23] | 15 of salivary gland origin | MCM2 | 15 of 15 | 100% |
| [11] | 10 of upper aerodigestive tract origin | Mit | 10 of 10 | 100% |
| [37] | 40 of salivary gland origin | MUC1 | 40 of 40 | 100% |
| [37] | 40 of salivary gland origin | MUC2 | 2 of 40 | 5% |
| [37] | 40 of salivary gland origin | MUC4 | 38 of 40 | 95% |
| [37] | 40 of salivary gland origin | MUC5AC | 29 of 40 | 72% |
| [37] | 40 of salivary gland origin | MUC5B | 33 of 40 | 82% |
| [37] | 40 of salivary gland origin | MUC6 | 13 of 40 | 32% |
| [37] | 40 of salivary gland origin | MUC7 | 2 of 40 | 5% |
| [19,21] | 23 of the upper aerodigestive tract; three of salivary gland origin or potential mimickers | MYB | 1 of 23; 1 of 3 | 4%; 33% |
| [26] | Seven of upper aerodigestive tract, nine of salivary gland origin, one of maxilla, and two of mandibula origin | NM23 | 18 of 19 | 92.80% |
| [13,35] | Seven; seven of upper aerodigestive tract origin | p53 | 4 of 7 | 57.1%; 16.4% |
| [12,27,34] | Six of salivary gland and head and neck origin; four; 65 of upper aerodigestive tract origin | p63 | 2 of 6; 4 of 4; 62 of 65 | 33%; 100%; 95.3% |
| [27] | Four | p73 | 4 of 4 | 100% |
| [35] | No sample size number available | PCNA | 92.9% | |
| [19] | Three of salivary gland origin or potential mimickers | PLAG1 | 0 of 3 | 0% |
| [12] | Six of salivary gland and head and neck origin | S-100 | 1 of 6 | 17% |
| [11,12] | 10 of upper aerodigestive tract origin; six of salivary gland and head and neck origin | SMA | 0 of 10; 0/6 | 0% |
| [11] | 10 of upper aerodigestive tract origin | SMM | 0 of 10 | 0% |
| [22] | 10 of salivary gland origin | SPLUNC1 | 0 of 10 | 0% |
| [22] | 10 of salivary gland origin | SPLUNC2 | 10 of 10 | 100% |
| [12] | Six of salivary gland and head and neck origin | SOX10 | 0 of 6 | 0% |
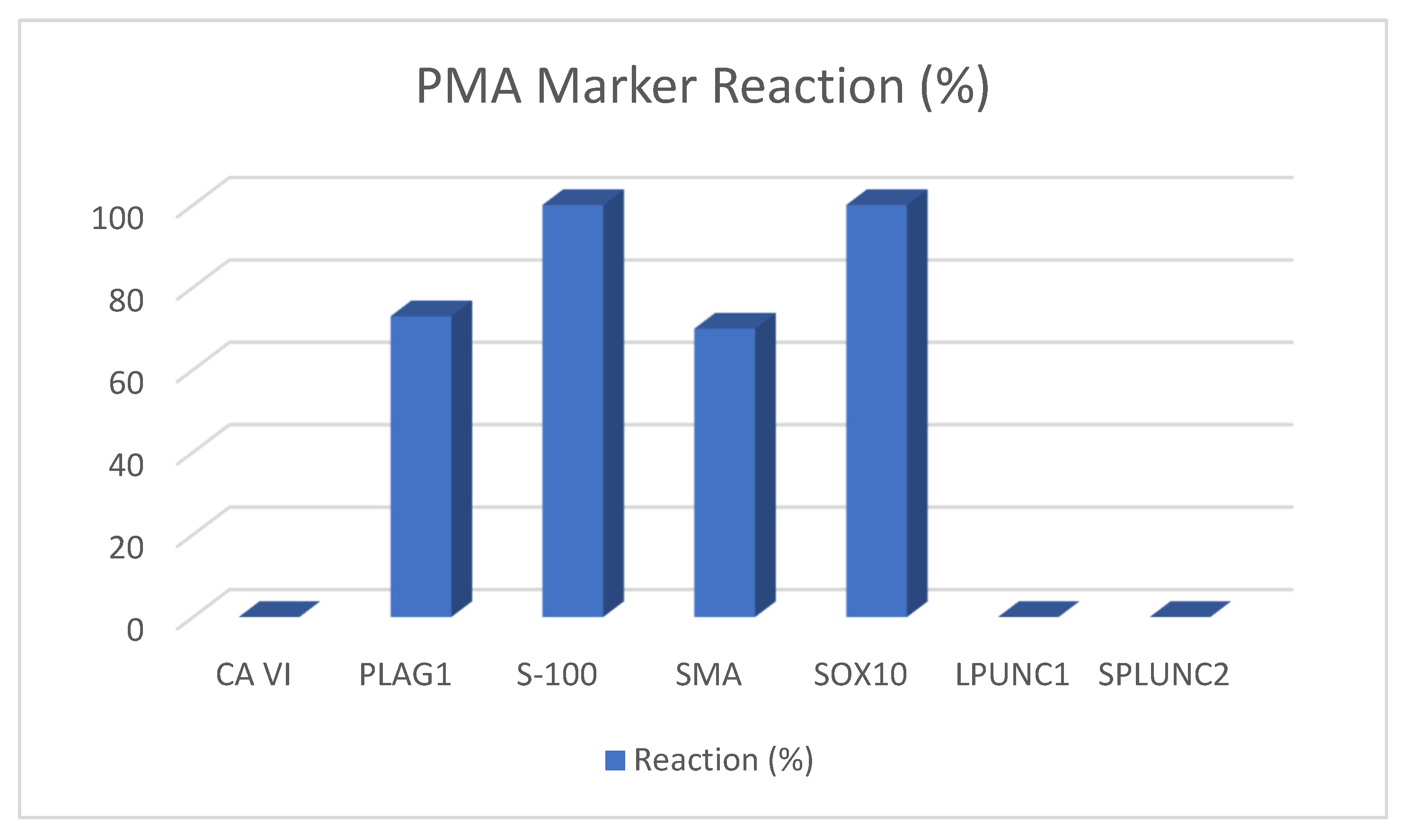
| Study | Sample Size PMA | Marker | Reaction |
|---|---|---|---|
| [31] | 10 of parotid origin | Amylase | 10% (1 of 10) |
| [12] | 10 (thereof four carcinomas) | Calponin | 70% (7 of 10) |
| [19,20,21] | 30; 16; 16 of salivary gland origin | KIT | 10%; 19%; 44% |
| [14] | Five of salivary gland origin | Carbonic anhydrate VI | Zero (0 of 5) |
| [15] | 16 of parotid origin | CD9 | 68.75% (11 of 16) |
| [18] | 14 of salivary gland origin | DOG1 | 7% (1 of 14) |
| [22] | 10 of salivary gland origin | SPLUNC1 | 0% (0 of 10) |
| [22] | 10 of salivary gland origin | SPLUNC2 | 0% (0 of 10) |
| [22] | 10 of salivary gland origin | LPLUNC1 | 0% (0 of 10) |
| [12] | 10 of salivary gland and head and neck origin (thereof four carcinomas) | GFAP | 90% (9 of 10) |
| [26] | 16 | NM23 | 75% |
| [12] | 10 of salivary gland and head and neck origin (thereof four carcinomas) | P63 | 80% (8 of 10) |
| [25] | 30 of parotid origin | Mcl-2 | 73% (22 of 30) |
| [12] | 10 of salivary gland and head and neck origin (thereof four carcinomas) | S100 | 100% (10 of 10) |
| [12] | 10 of salivary gland and head and neck origin (thereof four carcinomas) | SMA | 70% (7 of 10) |
| [19,21] | 29 of salivary gland origin or potential mimickers; 16 of salivary gland origin | MYB | 4% (1 of 4); 6% (1 of 16) |
| [19,43] | 30 of salivary gland origin or potential mimickers; 45 of salivary gland origin | PLAG1 | 73% (22 of 30); 100% (45 of 45) |
| Tumor | Gene | Chromosomal Rearrangement | Prevalence |
|---|---|---|---|
| PMA | PLAG1 fusions | 8q12 translocations | >50% |
| HMGA2 fusions | 12q13–15 translocations | ~15% | |
| MEC | CRTC1-MAML2 | t (11; 19) (q21; p13) | 40–80% |
| CRTC3-MAML2 | t (11; 15) (q21; q26) | ~5% | |
| CDKN2A deletion | 9p21.3 | ~35% | |
| ADCC | MYB fusion/activation | 6q22–23 translocations | ~80% |
| MYBL1 fusion/activation | 8q13 translocations | ~10% | |
| NOTCH1 mutation | - | 5–10% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meyer, M.T.; Watermann, C.; Dreyer, T.; Ergün, S.; Karnati, S. 2021 Update on Diagnostic Markers and Translocation in Salivary Gland Tumors. Int. J. Mol. Sci. 2021, 22, 6771. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22136771
Meyer MT, Watermann C, Dreyer T, Ergün S, Karnati S. 2021 Update on Diagnostic Markers and Translocation in Salivary Gland Tumors. International Journal of Molecular Sciences. 2021; 22(13):6771. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22136771
Chicago/Turabian StyleMeyer, Malin Tordis, Christoph Watermann, Thomas Dreyer, Süleyman Ergün, and Srikanth Karnati. 2021. "2021 Update on Diagnostic Markers and Translocation in Salivary Gland Tumors" International Journal of Molecular Sciences 22, no. 13: 6771. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22136771